
Abstract
Background
Each year, an estimated 15 million babies are born preterm. Micronutrient deficiencies, including vitamin D deficiency (VDD), are common in many low- and middle-income countries (LMICs), and these conditions are often associated with adverse pregnancy outcomes. Bangladesh experiences a high prevalence of VDD. The country also has a high preterm birth (PTB) rate. Using data from a population-based pregnancy cohort, we estimated the burden of VDD during pregnancy and its association with PTB.
Methods
Pregnant women (N = 3,000) were enrolled after ultrasound confirmation of gestational age at 8–19 weeks of gestation. Trained health workers prospectively collected phenotypic and epidemiological data at scheduled home visits. Trained phlebotomists collected maternal blood samples at enrollment and 24 -28 weeks of gestation. Aliquots of serum were stored at -800 C. We conducted a nested case–control study with all PTB (n = 262) and a random sample of term births (n = 668). The outcome, PTB, was defined as live births < 37 weeks of gestation, based on ultrasound. The main exposure was vitamin D concentrations of 24–28 weeks maternal blood samples. The analysis was adjusted for other PTB risk factors. Women were categorized as VDD (lowest quartile of 25(OH)D; < = 30.25 nmol/L) or not deficient (upper-three quartiles of 25(OH)D; > 30.25 nmol/L). We used logistic regression to determine the association of VDD with PTB, adjusting for potential confounders.
Results
The median and interquartile range of serum 25(OH)D was 38.0 nmol/L; 30.18 to 48.52 (nmol/L). After adjusting for co-variates, VDD was significantly associated with PTB [adjusted odds ratio (aOR) = 1.53, 95% confidence interval (CI) = 1.10 – 2.12]. The risk of PTB was also higher among women who were shorter (aOR = 1.81, 95% CI: 1.27–2.57), primiparous (aOR = 1.55, 95% CI = 1.12 – 2.12), passive smokers (aOR = 1.60, 95% CI = 1.09 – 2.34), and those who received iron supplementation during pregnancy (aOR = 1.66, 95% CI: 1.17, 2.37).
Conclusion
VDD is common in Bangladeshi pregnant women and is associated with an increased risk of PTB.
Similar content being viewed by others


Background
Globally, an estimated 15 million babies are born preterm each year, which is increasing. Preterm birth (born before 37 completed weeks of gestation) and its complications are the leading cause of neonatal deaths [1, 2] and deaths among children under the age of 5 years, accounting for approximately one million child deaths each year [3, 4]. Many surviving preterm babies experience a lifetime disability, including learning disabilities and visual and hearing problems [5]. Low- and middle-income countries (LMICs), such as those in Southeast Asia and Sub-Saharan Africa, have a significantly higher burden of preterm birth (PTB) [6] National-level data on PTB in Bangladesh is unavailable. Based on modeling, Chawanpaiboon S. et al., estimated that the preterm birth rate in Bangladesh is 19.1% [7].
The ability to find markers that correlate with PTB can aid in decreasing child morbidity and mortality rates. PTB is of multifactorial origin, partially associated with immunologic, genetic, nutritional, and environmental factors [8,9,10]. The other factors include infection or inflammation, pregnancy complications, including uteroplacental ischemia or hemorrhage, previous preterm birth, periodontal disease, uterine overdistension, stress, and other immunologically mediated processes [11, 12]. Figure 1 shows the factors associated with preterm birth and the possible pathways. The attribution of these factors has not yet been well elucidated.

Conceptual framework: factors associated with preterm birth and the possible pathways
Micronutrient deficiencies, including vitamin D deficiency (VDD), are common in many LMICs, and these deficiencies are often associated with adverse pregnancy outcomes [13, 14]. Pregnant women have a higher demand for micronutrients, and complications can arise from maternal micronutrient deficiency [15]. Vitamin D is an important micronutrient that regulates calcium and phosphate metabolism; it is essential for building bones. It is also a necessary part of the innate immune system as it aids in producing antimicrobial peptides [16]. Inadequate dietary intake, conditions that prevent the skin from producing enough vitamin D, and other factors that interfere with vitamin D metabolism or absorption can all contribute to VDD [17]. The current literature examining the association of VDD and PTB is conflicting. Some studies observed that low maternal vitamin D concentration was correlated with adverse outcomes in pregnancy, including PTB, low birth weight, gestational diabetes, and pre-eclampsia [18,19,20,21,22,23]. However, other studies did not show such association [24, 25].
VDD is highly prevalent in Bangladesh, with 66% to 94.2% adult women in their childbearing age experiencing the deficiency [26]. Bangladesh also experiences one of the highest PTB rates [7]. According to a systematic review published in Lancet Global Health, Bangladesh is one of the top five countries that experience the largest number of PTB [7]. India, China, Nigeria, Bangladesh, and Indonesia accounted for 57.9 million (41.4%) of 139·9 million live births and 6.6 million (44.6%) of 14.8 million PTB globally in 2014 [7, 27, 28]. The high burden of VDD as well as PTB in Bangladesh, makes the country a suitable place to further investigate if a correlation exists between the two. In this study, we aimed to investigate the relationship between Serum 25(OH)D concentrations and PTB among pregnant women in a rural area of Bangladesh.
Methods
Study design, setting, and data
This is a nested case–control study that uses data from a population-based cohort of pregnant women and their children; the study is known as the Alliance for Maternal and Newborn Health Improvement (AMANHI). As part of AMANHI, we established a biorepository and enrolled 3,000 pregnant women between 2014 and 2018 in two sub-districts of Sylhet district in northeast Bangladesh and followed them until day 42–60 postpartum. The details of the study methodology were published earlier [29]. Trained community health workers (CHWs) with a minimum of ten-grade education collected data after obtaining written informed consent. Pregnancies were identified through 2-monthly home visits and confirmed by strip–based pregnancy tests administered by CHWs and dated through ultrasound scans carried out by trained ultrasonologists between 8 and 19 weeks of gestation. CHWs made three antenatal home visits (at 8–19 weeks, 24–28 weeks, and 32–36 weeks of gestation) and two postnatal home visits (< 7 days and at 42–60 days). During these visits, the CHWs collected detailed phenotypic, socio-demographic, and epidemiological data from the pregnant women.
Sample collection
Maternal blood samples were collected twice during pregnancy (8–19 weeks and 24–28 weeks or 32–36 weeks of gestation) and once during the postpartum period (42–60 days postpartum). The second pregnancy sample was collected from about three-fourths of the randomly selected women. The third sample was collected from women who were not selected for the second blood sample. The blood samples were collected by trained phlebotomists at the study clinic, and serum samples were separated by centrifugation, aliquoted, and stored at -80 ℃ using standard procedures [30].
Population, cases and controls
For this study, we considered all women who had the second antenatal blood drawn (n = 2,287), had at least one antenatal and one postnatal visit and the pregnancy outcome data (n = 2,075), and had a live-born baby (n = 2,014). In this nested case–control study, all women who had a PTB (between 24 and < 37 weeks of gestation) were included as cases (n = 263) and a random sample of term births were included as controls (n = 671). Vitamin D was measured from cases and controls only. Vitamin D measurement was missing in one case and three control mothers; these mothers were excluded from the analysis. Thus, 262 cases and 668 controls were included in the analysis (Fig. 2).

Study flow chart
Vitamin D assay
The frozen serum samples were transferred to the Immunobiology, Nutrition and Toxicology laboratory of the international center for diarrhoeal disease research Bangladesh (icddr,b) for analysis. Serum 25(OH)D concentrations were measured by electrochemiluminescence immunoassay (ECLIA) with Roche automated immunoassay analyzers Cobas e601 using a commercial kit (Roche Diagnostics, GmbH, 68305 Mannheim, Germany) according to the manufacturer’s instruction. The method for vitamin D was standardized against LC MS/MS which in turn was standardized to the NIST standard. The measuring range for 25(OH)D was 7.50‑175 nmol/L. Commercial control based on human serum in two concentration ranges was run in each lot/day to monitor the accuracy and precision of this assay.
Measurements
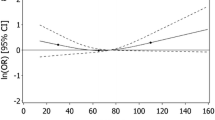
The outcome, PTB, was defined as live births < 37 weeks of gestation, based on ultrasound. The main exposure was vitamin D concentrations of 24–28 weeks maternal blood samples. Using Serum 25(OH)D concentrations, we categorized women into quartiles [lowest quartile (≤ 30.25 nmol/L), 3rd quartile (30.25–37.99 nmol/L), 2nd quartile (38.0–48.52 nmol/L), and highest quartile (≥ 48.53 nmol/L)]. Table 1 showed that about 75% of women had an insufficient vitamin D level (< 48.53 nmol). We then examined the association of vitamin D concentrations with the primary outcome, PTB and observed that compared to the highest quartile of vitamin D, all other quartiles had a higher risk of PTB, but the risks were only marginally higher in the second and 3rd quartiles. The lowest quartile had a 67% significantly higher risk of PTB. We then combined the upper three quartiles of vitamin D as ‘not deficient’ [25(OH)D ≥ 30.25 to ≥ 48.53 nmol/L] and the lowest quartile as vitamin D ‘deficient’ [25(OH)D ≤ 30.25 nmol/L]. We used these two categories in all subsequent analysis (Table 1).
Maternal age was categorized into < 30 and ≥ 30 years. Parity was categorized as 0/primiparous, 1–3, and ≥ 4 children. Maternal and paternal education was categorized into 0–5 years and > 5 years of schooling. Maternal height was categorized into height < 145 cm and > = 145 cm. Household crowding index was created by dividing the number of persons by number of sleeping rooms. We then categorized the household crowding into < = 2 and > 2. Using principal component analysis, we calculated scores for household wealth based on housing materials and household contents. The households were divided into tertiles using the wealth scores.
Sample size and statistical analysis
Since the number of cases were fixed, using Kelsey et al. [31] formula for sample size calculation for unmatched case–control study, we calculated the number of controls required per case to detect an Odd Ratio of 1.5 with the following parameters: proportion of controls with exposure = 20%; proportion of cases with exposure = 30%; two-sided confidence interval = 95%, and power = 80%. The number of controls required per case was 2.5. Accordingly, we selected 671 controls for 262 cases.
We conducted two sets of bi-variate analyses using Pearson’s chi-squared test for independence. First, we examined the association of vitamin D concentrations (deficient vs not deficient) with the mother’s age, education, occupation, maternal height, tobacco consumption, husband’s education, husband’s occupation, household crowding, and household wealth index. In the second set of bivariate analysis, we examined the association of infant’s preterm or term status with vitamin D concentrations and selected socioeconomic, demographic, and care-seeking characteristics of mothers. Multivariable logistic regression was used to calculate unadjusted and adjusted odds ratios (aORs) and 95% confidence intervals (CIs) to identify factors significantly associated with PTB. Variables with a p-value of < 0.2 in the bivariate analyses with PTB were included in the multivariable logistic regression model. We used Stata V.17 to analyze the data (StataCorp 2017).
Results
The association of maternal serum vitamin D concentrations with selected characteristics of mothers and households is presented in Table 2. The mother’s age, education, and household crowding were significantly associated with vitamin D concentrations. Younger mothers, age < 30 years and those with education > 5 years were more likely to have vitamin D deficiency (Table 2).
In bivariate analysis, the mother’s serum vitamin D concentrations, mother’s height, parity, iron supplementation during pregnancy, and passive smoking were associated with the infant’s term and preterm birth status (Table 3).
In the unadjusted logistic regression analysis examining the factors associated with PTB, mothers with VDD (OR, 95% CI: 1.49, 1.08–2.05), mother’s height (OR, 95% CI: 1.81, (1.29–2.54), primiparity (OR, 95% CI: 1.53, 1.12–2.10), mothers with history of passive smoking during pregnancy (OR, 95% CI: 1.47, 1.02–2.13), and mothers who received iron supplements (OR, 95%CI: 1.70 (1.20–2.40) showed a higher risk of PTB (Table 4). The risk of PTB associated with VDD remained similar after adjusting for other covariates that were significant in the bivariate analysis. Maternal serum VDD was associated with about 1.5 times higher risk of PTB (aOR, 95% CI: 1.53, 1.10 to 2.12). The risk of PTB was about 2 times higher among mothers with height < 145 cm (aOR, 95% CI: 1.81, 1.27–2.57) compared mothers with height > = 145 cm (Table 4). Compared to mothers with 1–3 children, primiparous mothers had about 1.5 times higher risk of PTB (aOR, 95% CI: 1.55, 1.12 -2.12) (Table 4). Mothers who consumed iron during pregnancy showed a 66% higher risk of PTB (aOR, 95% CI: 1.66, 1.17- 2.37) compared to mothers who did not (Table 4). In comparison to mothers who did not report passive smoking, those who did report it had 1.60 times (aOR, 95% CI: 1.60, 1.09–2.34) increased risk of PTB (Table 4).
Discussion
In a population-based cohort study of pregnant women followed through the early post-partum period in rural Bangladesh, we documented a high prevalence of serum 25(OH)D deficiency during the second trimester of pregnancy. A vitamin D concentration of < 50 nmol/L or 20 ng/ml is considered deficient and associated with unfavorable outcomes [32]. In the present study, about 3 out of 4 Bangladeshi pregnant women had a vitamin D concentration of < 50 nmol/L. For this analysis, we considered women in the lowest vitamin D quartile with a level of < 30.25 nmol/L as deficient and the remaining women as not deficient although women in the second and third vitamin D quartiles also had a trend towards a higher risk of PTB compared to women in the highest vitamin D quartile. Thus, this analysis showing about a fifty percent higher risk of preterm birth (aOR 1.53 95% CI; 1.10 to 2.12) in VDD women compared to those who were considered not deficient is conservative.
In addition to VDD, maternal short stature, primiparity, passive smoking, and iron supplementation during pregnancy were also significantly associated with higher risks of PTB. The significantly higher risk of PTB among women who consumed iron during pregnancy is counter-intuitive. An earlier study conducted in the same population found a similar result [33]. The benefits of iron supplementation during pregnancy in iron-deficient population are well-established [34]. Results from a systematic review which included 48 randomized trials and 44 cohort studies, revealed a significant effect of prenatal iron consumption on reducing the risk of low birth weight (RR: 0.81; 95% CI: 0.71, 0.93), but the effect on preterm birth was not significant (RR: 0.84; 95% CI: 0.68, 1.03) [34]. There is also evidence to suggest that increasing iron intake is not always beneficial. Iron availability may influence the severity and chronicity of maternal infections and thus might lead to negative pregnancy outcomes, including preterm birth [35], particularly in populations where the prevalence of maternal infections is high.
Our study showed that there was increased risk of PTB among women who had VDD. However, the current literature on vitamin D concentrations and PTB is conflicting. Some studies showed an association while others did not. In a study conducted in South Carolina, USA, using two datasets from National Institute of Child Health and Human Development (n = 333) and Thrasher Research Fund (n = 154), Wagner et al., 2015 found an increased risk of PTB in women with lower vitamin D concentrations [36]. Women who had vitamin D concentrations < 20 ng/mL in their third trimester had 3.3 times the odds of PTB compared to those who had concentrations > 40 ng/mL [36].
In a retrospective cohort study, also conducted in South Carolina, USA, McDonnell et al., (2017) found that pregnant women who had vitamin D concentrations > 40 ng/mL had 62% lower odds of having PTB when compared to women who had vitamin D concentrations < 20 ng/mL [37]. A Meta-analysis of observational studies conducted in 10,098 women also showed an increased risk of PTB in those who had vitamin D concentrations < 20 ng/mL (OR 1.29, 95% CI: 1.16,1.45) [38].
However, several other studies did not show an association between VDD and PTB. A prospective cohort study by Wang S et al., (2021) in 3,465 pregnant women in Zhoushan Maternal and Child Health Hospital, Zhejiang, China did not show a significant association between maternal VDD and risk for PTB [39]. A retrospective study of 1,1641 women in southern China also did not find an association [40].
Randomized clinical trials (RCT) conducted to assess whether vitamin D supplementation to those who are deficient can improve the rate of PTB has also been inconclusive. Sablok et al., (2015) performed a RCT in 180 pregnant women in Delhi, India and found an 8.3% PTB rate among women who received Vitamin D compared to a rate of 21.1% among those who did not [41]. Rostami et al., (2018) conducted a stratified randomized trial among 2,500 Iranian women and showed a 40% (95% CI, 0.40 to 0.80) lower rate of PTB in women who were supplemented with vitamin D [42]. However, another randomized control trial conducted by Hossain et. al., 2014 at the university hospital in Karachi, Pakistan, did not show an effect. In this study of 207 pregnant women, one group received ferrous sulfate and calcium while the other group received 4,000 IU of Vitamin D3. Though vitamin D concentrations increased in both mother and baby with supplementation, there was no significant difference in PTB rate [43]. Mojibian et al., (2015) conducted a randomized clinical trial in 500 pregnant women (12–16 weeks) with vitamin D deficiency and did not see a significant difference in the PTB rate among those that were given 400 IU of vitamin D daily versus 50,000 IU of vitamin D every 2 weeks [44]. The reason for this conflicting results in different studies are likely multifactorial, including different experimental designs, difference in the timing of measurement of vitamin D level, prevalence of vitamin D deficiency and PTB in the population studied, and different geographical locations and racial backgrounds. The RCTs that showed no benefit in terms of reduction of PTB with supplementation had relatively small sample size. Further RCTs with a larger number of pregnant women in vitamin D deficient population may help delineate whether supplementing mothers can help reduce PTB rate.
The mechanism of maternal vitamin D deficiency and PTB has not been fully elucidated. However, recent studies suggested several pathways including oxidative stress, imbalance in the regulation of the inflammatory response, and compromise of placental function during pregnancy [45, 46]. Yamada et al., (2020) hypothesized that women with VDD may experience increased risk of PTB due to deregulation of immune response [47]. Improved maternal vitamin D status may act through reducing the risk of infections, including bacterial vaginosis that has been implicated in the causation of preterm labor [48].
The strength of the study is its population-based prospective design. The main outcome variable, PTB, was based on gestational age dating by early pregnancy ultrasound conducted by trained ultrasonologists. Thus, the term/preterm classification was accurate compared to classification based on reported date of last menstrual period. The study also has several limitations. This is a case–control study, which can be subject to bias and confounding [49]. Since we collected data prospectively from the entire cohort using the same methods, the bias, if any, should be minimum [50]. Another limitation is that we did not have data on all possible risk factors for PTB.
Conclusion
The study showed a high prevalence of VDD in Bangladeshi pregnant women, and that these women had an increased risk of PTB. This findings from a case–control study should be cautiously interpreted to infer causality. Additional research is warranted, both observational to further explore the associations between VDD and the risk of PTB and randomized trials to examine if the supplementation is beneficial.
Availability of data and materials
The dataset used and analyzed for this manuscript will be available from the corresponding author on request.
Abbreviations
- LMICs:
-
Low- and middle-income countries
- PTB:
-
Preterm birth
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- AMANHI:
-
Alliance for Maternal and Newborn Health Improvement
- CHWs:
-
Community health workers
- icddr,b:
-
International center for diarrhoeal disease research Bangladesh
- ECLIA:
-
Electrochemiluminescence immunoassay
- GA:
-
Gestational age
- BMI:
-
Body mass index
- AOR:
-
Adjusted odds ratio
- NICHD:
-
National Institute of Child Health and Human Development
- RCT:
-
Randomized clinical trials
References
Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966):430–40.
Harrison MS, Goldenberg RL. Global burden of prematurity. Semin Fetal Neonatal Med. 2016;21(2):74–9.
Dimes Mo, PMNCH, Children St, WHO. Born too soon: the global action report on preterm birth. Geneva: World Health Organization; 2020. https://www.marchofdimes.org/materials/born-too-soon-the-global-action-report-on-preterm-.pdf.
Perin J, Mulick A, Yeung D, Villavicencio F, Lopez G, Strong KL, et al. Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc Health. 2022;6(2):106–15.
Blencowe H, Cousens S, Chou D, Oestergaard M, Say L, Moller AB, et al. Born too soon: the global epidemiology of 15 million preterm births. Reprod Health. 2013;10 Suppl 1(Suppl 1):S2.
Walani SR. Global burden of preterm birth. Int J Gynaecol Obstet. 2020;150(1):31–3.
Chawanpaiboon S, Vogel JP, Moller AB, Lumbiganon P, Petzold M, Hogan D, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health. 2019;7(1):e37–46.
Romero R, Espinoza J, Kusanovic JP, Gotsch F, Hassan S, Erez O, et al. The preterm parturition syndrome. BJOG. 2006;113 Suppl 3(Suppl 3):17–42.
Beck S, Wojdyla D, Say L, Betran AP, Merialdi M, Requejo JH, et al. The worldwide incidence of preterm birth: a systematic review of maternal mortality and morbidity. Bull World Health Organ. 2010;88(1):31–8.
Institute of Medicine Committee on Understanding Premature B, Assuring Healthy O. The National Academies Collection: Reports funded by National Institutes of Health. In: Behrman RE, Butler AS, editors. Preterm Birth: Causes, Consequences, and Prevention. Washington (DC): National Academies Press (US); 2007. Copyright © 2007, National Academy of Sciences.
Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. The Lancet. 2008;371(9606):75–84.
Zhang G, Jacobsson B, Muglia LJ. Genetic Associations with Spontaneous Preterm Birth. N Engl J Med. 2017;377(24):2401–2.
Darnton-Hill I, Mkparu UC. Micronutrients in pregnancy in low- and middle-income countries. Nutrients. 2015;7(3):1744–68.
Gernand AD, Schulze KJ, Stewart CP, West KP Jr, Christian P. Micronutrient deficiencies in pregnancy worldwide: health effects and prevention. Nat Rev Endocrinol. 2016;12(5):274–89.
Kanasaki K, Kumagai A. The impact of micronutrient deficiency on pregnancy complications and development origin of health and disease. J Obstet Gynaecol Res. 2021;47(6):1965–72.
Bartley J. Vitamin D: emerging roles in infection and immunity. Expert Rev Anti Infect Ther. 2010;8(12):1359–69.
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–81.
Palaniswamy S, Williams D, Järvelin MR, Sebert S. Vitamin D and the promotion of long-term metabolic health from a programming perspective. Nutr Metab Insights. 2015;8(Suppl 1):11–21.
Chen YH, Fu L, Hao JH, Wang H, Zhang C, Tao FB, et al. Influent factors of gestational vitamin D deficiency and its relation to an increased risk of preterm delivery in Chinese population. Sci Rep. 2018;8(1):3608.
Baczyńska-Strzecha M, Kalinka J. Assessment of correlation between vitamin D level and prevalence of preterm births in the population of pregnant women in Poland. Int J Occup Med Environ Health. 2017;30(6):933–41.
Kalinjuma AV, Darling AM, Sudfeld CR, Mugusi F, Wright J, Abioye AI, et al. Vitamin D Concentration during Early Pregnancy and Adverse Outcomes among HIV-Negative Women in Dar-es-Salaam, Tanzania: A Case-Control Study. Nutrients. 2019;11(12):2906.
Miliku K, Vinkhuyzen A, Blanken LM, McGrath JJ, Eyles DW, Burne TH, et al. Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes. Am J Clin Nutr. 2016;103(6):1514–22.
Amegah AK, Klevor MK, Wagner CL. Maternal vitamin D insufficiency and risk of adverse pregnancy and birth outcomes: a systematic review and meta-analysis of longitudinal studies. PLoS One. 2017;12(3):e0173605.
Yang L, Pan S, Zhou Y, Wang X, Qin A, Huang Y, et al. The correlation between serum vitamin D deficiency and preterm birth. Med Sci Monit. 2016;22:4401–5.
Agarwal S, Kovilam O, Agrawal DK. Vitamin D and its impact on maternal-fetal outcomes in pregnancy: a critical review. Crit Rev Food Sci Nutr. 2018;58(5):755–69.
Islam MZ, Bhuiyan NH, Akhtaruzzaman M, Allardt CL, Fogelholm M. Vitamin D deficiency in Bangladesh: a review of prevalence, causes and recommendations for mitigation. Asia Pac J Clin Nutr. 2022;31(2):167–80.
Purisch SE, Gyamfi-Bannerman C. Epidemiology of preterm birth. Semin Perinatol. 2017;41(7):387–91.
Vogel JP, Chawanpaiboon S, Moller AB, Watananirun K, Bonet M, Lumbiganon P. The global epidemiology of preterm birth. Best Pract Res Clin Obstet Gynaecol. 2018;52:3–12.
Baqui AH, Khanam R, Rahman MS, Ahmed A, Rahman HH, Moin MI, et al. Understanding biological mechanisms underlying adverse birth outcomes in developing countries: protocol for a prospective cohort (AMANHI bio-banking) study. J Glob Health. 2017;7(2):021202.
Aftab F, Ahmed S, Ali SM, Ame SM, Bahl R, Baqui AH, et al. Cohort Profile: The Alliance for Maternal and Newborn Health Improvement (AMANHI) biobanking study. Int J Epidemiol. 2022;50(6):1780–1.
Jennifer KL, Alice WS, Alfred ES, Douglas TW. Methods in Observational Epidemiology 2nd Edition, Table 12–15. New York Oxford: Oxford University Press; 1996.
Amrein K, Scherkl M, Hoffmann M, Neuwersch-Sommeregger S, Köstenberger M, TmavaBerisha A, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74(11):1498–513.
Shah R, Mullany LC, Darmstadt GL, Mannan I, Rahman SM, Talukder RR, et al. Incidence and risk factors of preterm birth in a rural Bangladeshi cohort. BMC Pediatr. 2014;14:112.
Haider BA, Olofin I, Wang M, Spiegelman D, Ezzati M, Fawzi WW. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2013;346:f3443.
Brabin L, Brabin BJ, Gies S. Influence of iron status on risk of maternal or neonatal infection and on neonatal mortality with an emphasis on developing countries. Nutr Rev. 2013;71(8):528–40.
Wagner CL, Baggerly C, McDonnell SL, Baggerly L, Hamilton SA, Winkler J, et al. Post-hoc comparison of vitamin D status at three timepoints during pregnancy demonstrates lower risk of preterm birth with higher vitamin D closer to delivery. J Steroid Biochem Mol Biol. 2015;148:256–60.
McDonnell SL, Baggerly KA, Baggerly CA, Aliano JL, French CB, Baggerly LL, et al. Maternal 25(OH)D concentrations ≥40 ng/mL associated with 60% lower preterm birth risk among general obstetrical patients at an urban medical center. PLoS One. 2017;12(7):e0180483.
Qin LL, Lu FG, Yang SH, Xu HL, Luo BA. Does maternal vitamin D deficiency increase the risk of preterm birth: a meta-analysis of observational studies. Nutrients. 2016;8(5):301.
Wang S, Xin X, Luo W, Mo M, Si S, Shao B, et al. Association of vitamin D and gene variants in the vitamin D metabolic pathway with preterm birth. Nutrition. 2021;89:111349.
Yu L, Guo Y, Ke HJ, He YS, Che D, Wu JL. Vitamin D status in pregnant women in Southern China and risk of preterm birth: a large-scale retrospective cohort study. Med Sci Monit. 2019;25:7755–62.
Sablok A, Batra A, Thariani K, Batra A, Bharti R, Aggarwal AR, et al. Supplementation of vitamin D in pregnancy and its correlation with feto-maternal outcome. Clin Endocrinol (Oxf). 2015;83(4):536–41.
Rostami M, Tehrani FR, Simbar M, BidhendiYarandi R, Minooee S, Hollis BW, et al. Effectiveness of prenatal vitamin D deficiency screening and treatment program: a stratified randomized field trial. J Clin Endocrinol Metab. 2018;103(8):2936–48.
Hossain N, Kanani FH, Ramzan S, Kausar R, Ayaz S, Khanani R, et al. Obstetric and neonatal outcomes of maternal vitamin D supplementation: results of an open-label, randomized controlled trial of antenatal vitamin D supplementation in Pakistani women. J Clin Endocrinol Metab. 2014;99(7):2448–55.
Mojibian M, Soheilykhah S, FallahZadeh MA, Jannati MM. The effects of vitamin D supplementation on maternal and neonatal outcome: a randomized clinical trial. Iran J Reprod Med. 2015;13(11):687–96.
Jha RK, Kanyal D, Dhok DA, Butola LK. Need of vitamin d beyond bone: a consise review. Eur J Mol Clin Med. 2021;8(3):1096–109.
Sultana Z, Maiti K, Aitken J, Morris J, Dedman L, Smith R. Oxidative stress, placental ageing-related pathologies and adverse pregnancy outcomes. Am J Reprod Immunol. 2017;77:e12653. https://doi.org/10.1111/aji.12653.
Yadama AP, Mirzakhani H, McElrath TF, Litonjua AA, Weiss ST. Transcriptome analysis of early pregnancy vitamin D status and spontaneous preterm birth. PLoS One. 2020;15(1):e0227193.
Manns-James L. Bacterial vaginosis and preterm birth. J Midwifery Womens Health. 2011;56(6):575–83.
Verani JR, Baqui AH, Broome CV, Cherian T, Cohen C, Farrar JL, et al. Case-control vaccine effectiveness studies: preparation, design, and enrollment of cases and controls. Vaccine. 2017;35(25):3295–302.
Verani JR, Baqui AH, Broome CV, Cherian T, Cohen C, Farrar JL, et al. Case-control vaccine effectiveness studies: data collection, analysis and reporting results. Vaccine. 2017;35(25):3303–8.
Acknowledgements
We acknowledge the study participants for their participation in the study, time, samples, and data. We also thank the dedicated field and data teams for implementing the study.
Funding
The AMANHI study was funded by the Bill & Melinda Gates Foundation (Award No: OPP1054163, INV-005276). The funders had no role in the study design, data collection, data analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
TT and RK share joint first authorship. AB, TT, and RK conceptualized the study, reviewed the literature, planned the analysis, and wrote the first draft. NHC did data curation and basic analyses. AB and RK conducted the analysis separately to avoid any computational errors. SR, SA, TH, and RR engaged in study supervision: AKR, MBH, and RR conducted lab analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We obtained approval for the study from the ethics committees of the International Centre for Diarrhoeal Disease Research, Bangladesh (PR 12073), the Johns Hopkins Bloomberg School of Public Health (IRB No: 00004508), and the World Health Organization (RPC 532). Informed consent was obtained from all subjects and/or their legal guardian(s). All experiments were performed in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tahsin, T., Khanam, R., Chowdhury, N.H. et al. Vitamin D deficiency in pregnancy and the risk of preterm birth: a nested case–control study. BMC Pregnancy Childbirth 23, 322 (2023). https://doi.org/10.1186/s12884-023-05636-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-05636-z