
Abstract
Background
Limited evidence exists on the correlation between the pre-pregnancy low-carbohydrate (LC) diet and maternal oral glucose tolerance test (OGTT) levels during pregnancy. Our aim was to compare the differences in maternal OGTT levels among women who had been diagnosed with gestational diabetes mellitus (GDM) during pregnancy and adopted different dietary patterns in the pre-pregnancy period.
Methods
A case–control study was conducted in 20 women with GDM who adhering to an LC diet (carbohydrate intake < 130 g/d) during pre-conception (LC/GDM,cases). Control subjects, who were matched in a 4:1 ratio, were 80 women with GDM and conventional diet (Con/GDM,control), and 80 women with conventional diet but without GDM (Con/Healthy,control). Women diagnosed with GDM using 75-g OGTT between 24 and 28 weeks of gestation. We used unadjusted raw data to compare the dietary composition data and biomarkers of the three study groups.
Results
The average pre-conception BMI in each group suggested a similar body size from the three study groups(19.12 ± 2.00 LC/GDM, 19.65 ± 2.32 Con/GDM, 19.53 ± 2.30 Con/Healthy; P = 0.647). Compared with the Con/GDM group, the OGTT-1 h and OGTT-2 h values in LC/GDM group were significantly higher (10.36 ± 1.28 mmol/L vs. 9.75 ± 0.98 mmol/L; 9.12 ± 0.98 mmol/L vs. 8.29 ± 1.06 mmol/L). Furthermore, the percentage of women who had more than one abnormal OGTT value (OGTT-1 h and OGTT-2 h) was 40% in the LC/GDM group, which was significantly higher than in the Con/GDM group (16.3%).
Conclusions
We observed a relationship between the pre-pregnancy LC diet and more detrimental OGTT values in patients with GDM. This finding warrants further studies to understand the effect of pre-pregnancy LC diet practice on maternal glucose tolerance.
Similar content being viewed by others


Introduction
Gestational diabetes mellitus (GDM), characterized by glucose intolerance first diagnosed during pregnancy, is one of the most common maternal complications [1]. In China, a recent systematic review and meta-analysis including 79,064 participants showed a total incidence of 14.8%, while the Shanghai Birth Cohort found 14.2% (585 women) with GDM [2, 3]. Epidemiologic data have shown that GDM is associated with both short- and long-term adverse health consequences for the mother and the offspring [4]. Risk factors of developing GDM include those with advanced maternal age, pre-pregnancy overweight/obesity, family history of diabetes, and excessive weight gain during pregnancy [5]. Poor dietary behaviors before and during pregnancy, such as excessive consumption of sugary drinks and higher intake of animal fat and cholesterol, were also associated with an increased risk of GDM [6].
Regarding the optimum diet for a gestational diabetic woman, Jovanovic-Peterson et al. suggested that the primary treatment strategy for pregnancies complicated by diabetes should be one which does not precipitate ketones of starvation, but restricts carbohydrates sufficiently to prevent postprandial hyperglycemia in 1990 [7, 8]. In 2014, Bao et al. found that, compared with the highest pre-pregnancy carbohydrate intake group, the lowest pre-pregnancy carbohydrate intake group had a 27% higher risk of GDM (relative risk [RR] = 1.27, 95% CI: 1.06, 1.51) [9]. The Australian Longitudinal Study on Women’s Health’s results also suggested that relatively low-carbohydrate (LC) diet and high fat intakes may increase the risk of GDM [10]. However, the above studies compared the differences between the lowest (lowest quintile of carbohydrate score) and highest (highest quintile of carbohydrate score) carbohydrate intake groups based on the LC diet scores rather than by absolute intakes of carbohydrate, fat, and protein; the lowest carbohydrate intakes were 178 g/d and 162 g/d, respectively; Low-carbohydrate diet, a dietary pattern with carbohydrate restriction, is a popular approach in weight loss and glucose control [11]. The dietary guidelines for Chinese residents (2022) recommends at least 130 g/d of carbohydrate intake during early pregnancy, while the Institute of Medicine (IOM) recommends at least 175 g/d of carbohydrate intake during pregnancy [12]. For the purposes of our study, we refer to diets with less than 130 g/day as a low-carbohydrate (LC) diet, consistant with the definition in recent reviews on safety of low carbohydrate diets [13, 14]. Despite the increasing popularity of strictly LC diets for weight loss in women of childbearing age, but it remains unknown whether the LC-diet is safe for maternal metabolic needs over longer period of time.
The purpose of this case–control study was to evaluate the differences in OGTT levels between women with GDM adhering to a LC diet (LC/GDM) and a conventional diet (Con/GDM) during pre-conception, and healthy pregnant women adhering to a conventional diet (Con/Healthy) during pre-conception for healthy control.
Methods
Study design and participants
This case–control study was conducted at Shanghai International Peace Maternity and Child Health Hospital (IPMCH) between January 2019 and January 2020. According to the routine medical procedures for pregnant women in Shanghai, a 75-g oral glucose tolerance test (OGTT) will be arranged between 24 and 28 weeks’ gestation to detect GDM. Women with a diagnosis of GDM will be referred to nutrition clinic for nutritional consultation and treatment. All participants were recruited after OGTT and dietary assessment between 24 and 28 weeks’ gestation.
-
The participants recruited in the “case” group (LC/GDM) were women with a diagnosis of GDM, and the women with GDM were further interviewed with trained dietitians to identify if she had adhering to an initiative limit-carbohydrate diet (carbohydrate intake < 130 g/d) for weight management for at least 12 months before pregnancy.
-
The participants recruited in the first “control” group (Con/GDM) were women with a diagnosis of GDM, and the women with GDM were further interview with trained dietitians to identify if she had adhering to an conventional diet (carbohydrate intake ≥ 130 g/d) before pregnancy.
-
The participants recruited in the second “control” group (Con/Healthy) were healthy women on a conventional diet (carbohydrate intake > 130 g/d) before pregnancy.
-
The two control groups (Con/GDM and Con/Healthy) were matched to the LC/GDM group by 1:4 for age, pre-pregnancy BMI (underweight, normal, overweight, obese), parity and family history of diabetes. A total of 180 pregnant women in 24-28 gestational weeks were included in this study (Fig. 1).

Patient workflow
Subjects with the following criteria were excluded: 1) those with religious dietary restrictions; 2) those diagnosed with type 2 diabetes mellitus (T2DM) before pregnancy;3) those with history of polycystic ovary syndrome, unexplained recurrent spontaneous abortion, and other digestive tract disease, liver disease, and kidney disease. Cut-off points of BMI were adopted based on the Chinese population standards [15].
Written informed consent was obtained from all participants. This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involing human subjects/patients were approved by the Institutional Review Board of the IPMCH affiliated with the School of Medicine, Shanghai Jiao Tong University (GKLW2018-35).
Dietary assessments
The women in the “case” group (LC/GDM) were healthy women before pregnancy, who followed a long-term (≧12 months) LC diet for weight management. During the nutritional interview, participants’ habitual dietary intake before pregnancy was varified through a 24-h dietary recall about the average intake of major foods or food groups by trained dietitians. The low-carbohydrate (LC) diet was defined as diets with less than 130 g/day, and a conventional diet (Con diet) was defined as diets with carbohydrate intake ≥ 130 g/d, and without special food restriction.
Participants were also invited to complete a 24-h dietary recalls on their current dietary intake (between 24 and 28 weeks of gestation). If a participant reported during a 24-h recall that she did not eat or drink normally the day before (e.g., because of fasting, illness, or other reasons), dietary data from that 24-h recall will be performed at another visit.
Trained dietitians administered the interview, using food models to access the food intake. The interviews were conducted between 24 and 28 weeks of gestation. The intakes of energy and macronutrients were calculated by nutrient calculation software ZHEN DIN 2.0.
OGTT value and diagnosis of GDM
Each OGTT value (fasting, 1 h, and 2 h) were compared among three groups. The type and number of abnormal OGTT values were also compared, such as the numbers (preportions) of women with an abnormal fasting value, abnormal 1-h value, or with an abnormal 2-h value. The “Higher-1 h-2 h” refer to women who had more than one abnormal OGTT value (OGTT-1 h and OGTT-2 h).
GDM was diagnosed by the International Association of the Diabetes and Pregnancy Study Groups (IADPSG) criteria between 24 and 28 weeks of gestation. A one-step approach using 75-g OGTT was performed after at least an 8-h fast (cutoff values: fasting ≥ 5.1 mmol/L; 1 h ≥ 10.0 mmol; 2 h ≥ 8.5 mmol/L). GDM was defined as one or more abnormal OGTT values [16].
Area under the curve (AUC) of OGTT were calculated according to the approximate trapezoidal area formula, AUC = (fasting blood glucose/2 + postprandial 1 h + postprandial 2 h/2) × 1 h[mmol/(L˙h)].
Clinical examinations
All participants underwent standard clinical care which included biomedical blood tests. Fasting blood glucose, serum glycated haemoglobin (HbA1c) and lipid profiles [total cholesterol (TC), triacylglycerol (TG), high density lipoprotein cholesterol (HDLC), low density lipoprotein cholesterol (LDLC)]were measured in the first trimester of pregnancy (10–12 weeks of gestation). Serum HbA1c, glycated albumin (GA) and levels of OGTT test were performed between 24–28 gestational weeks. All the blood samples were detected with Cobas 8000 modular analyzer series. The detection of ketones in the urine was performed through Sysmex UC-3500 urine chemistry analyzer.
Anthropometric measurements
The participants were weighed barefoot using a standardized digital height and weight scale calibrated to 0.1 kg (SECA-285). After resting for 5 min, an automated system (OMRON-HEM-1020) was used to measure the blood pressure once. Weighing and blood pressure measurements were performed during every routine check-up.
Statistical analysis
Given the exploratory nature of this study (the sample size of women with a strict LC diet was limited), we did not conduct a priori sample size estimation. We only used unadjusted data to compare the dietary composition data and biomarkers of the three study groups because we have matched the potential confounders in different groups. One-way analysis of variance was used to analyze difference in continuous variables, and pairwise comparisons between the three groups were performed using Tukey’s studentized range test. Continuous variables were showed as means and SD. Chi-square test was used to analyze difference in categorical variables, and pairwise comparisons were performed using Bonferroni test. Statistical analysis was performed using SPSS statistical software, version 23. P values < 0.05 was considered statistically significant.
Results
Characteristics of the participants
The main characteristics of the study groups participants were presented in Table 1. As expected, all study participants were comparable in terms of age, parity, educational level, pre-pregnancy BMI, and family history of diabetes. There was no significant difference between the weight gains during pregnancy in the three groups in the first trimester. In the second trimester, the LC/GDM group had the lowest weight gain (5.72 kg) followed by the Con/GDM group (7.01 kg); the Con/Healthy group gained the most weight (8.33 kg). There was no difference in weight gain among women in the LC/GDM and Con/GDM groups in the third trimester, while the gestational weight gain in GDM groups were significantly lower than that in the Con/Healthy group (P < 0.001). No other significant differences were observed, including infant birth weight and macrosomia rate.
Ditary intake
Figure 2 shows the dietary intake data of the study groups before pregnancy and at the second trimester of pregnancy. The total energy intake before pregnancy in the LC/GDM group was 1078.5 kcal/d, which was significantly lower than the 1585.5 kcal/d in the Con/GDM group (P < 0.001) and 1532.5 kcal/d (P < 0.001) in the Con/Healthy group. During the second trimester, the energy intakes were increased in all three groups, however, women in the LC/GDM group still consumed much less calories(1375.6 ± 192.9 kcal) compared to the Con/GDM (1826.9 ± 268.3 kcal) and Con/Healthy (1899.2 ± 364.0) groups (P < 0.001).

Changes in dietary intake pre-pregnancy and during the second trimester of pregnancy
The LC/GDM group had the lowest intake of carbohydrates (95.3 g/d; energy supply ratio, 33.4%) compared to the other two groups before pregnancy, with minimum and maximum intakes of 52.8 g/d and 126.6 g/d, respectively, which met the LC intake standard of < 130 g/d. All study groups showed increased carbohydrate intake during the second trimester. The intake in the LC/GDM and Con/GDM groups increased by an average of 64.4 g and 31.3 g, respectively. Although the LC/GDM group had the highest increase in carbohydrate intake, that in the second trimester was still lower than that in the other two groups (P < 0.001), and six (30%) participants in the LC/GDM group still followed an LC diet in the second trimester.
In the pre-pregnancy period, the protein intake level (58.1 g/d) of the LC/GDM group was lower than that of the Con/GDM group (69.9 g/d). The protein energy supply ratio of the LC/GDM group was 21%, which was higher than the 17.6% of the Con/GDM group in the pre-pregnancy period. There was no difference in the total fat intake among the three groups during the pre-pregnancy period (P = 0.729), but the fat energy supply ratio of the LC/GDM group was significantly higher than that of the Con/GDM and Con/Healthy groups (P < 0.001).
The dietary patterns of the Con/GDM and Con/Healthy groups were similar before and during pregnancy in terms of the energy and macronutrient intakes and ratio, which were consistent with the recommended range of the Chinese food pagoda [17]. Compared with the Con/GDM and Con/Healthy groups, the LC/GDM group followed a typical LC diet before pregnancy.
Fasting plasma glucose and OGTT
Compared with women in the Con/GDM group, those in the LC/GDM group had a lower HbA1c level in the first trimester (5.14% vs. 5.32%, P < 0.05). Compared with the first trimester, the fasting blood glucose level of the three groups in the second trimester showed a downward trend (Table 2).
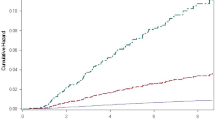
For comparing the blood glucose levels among the three groups at the three OGTT timepoints (OGTT-0 h, OGTT-1 h, and OGTT-2 h), the OGTT-0 h blood glucose levels in the LC/GDM and Con/GDM groups were not significantly different. However, those at OGTT-1 h and OGTT-2 h in the LC/GDM group were significantly higher than those in the Con/GDM group. The area under the blood glucose curve was also significantly higher than that of the Con/GDM group (P < 0.001) (Fig. 3). In addition, compared with the Con/GDM group, the ratio of abnormal values in both OGTT-1 h and OGTT-2 h in the LC/GDM group was significantly higher (LC/GDM: 40.0%; Con/Healthy: 16.3%). In the first and second trimesters, the HbA1c levels in the LC/GDM and Con/GDM groups were the lowest and highest, respectively, among the three groups. There was no significant difference in HbA1c levels between the LC/GDM and Con/GDM groups in the second trimester. However, in the second trimester, glycated albumin (GA) of the LC/GDM group was significantly lower than that of the Con/GDM group (P < 0.001).

The blood glucose levels of the two groups of participants diagnosed with GDM and the healthy controls at the three time points of the OGTT. LC, low carbohydrate diet; GDM, gestational diabetes; OGTT, oral glucose tolerance test. LC/GDM, patients with GDM on an low carbohydrate diet; Con/GDM, patients with GDM on a conventional diet; Con/Healthy, healthy women on a conventional diet
There was no significant difference in the rate of positive urine ketone bodies among the three groups in the first trimester. In the second trimester, the rate in the LC/GDM greatly increased, which was significantly higher than that in the Con/GDM and Con/Healthy groups (P < 0.001). In the third trimester, the positive rate of positive urine ketone bodies in LC/GDM group decreased to 5%.
Discussion
We found that compared with women with GDM who had a conventional diet before pregnancy, those who adhered to a long time LC diet before pregnancy had not only higher values in OGTT-1 h and OGTT-2 h but also higher rate of abnormal values both in OGTT-2 h and OGTT-2 h. This study is the first to explore the relationship between a strict LC diet before pregnancy and glucose tolerance during pregnancy. First, the daily carbohydrate intake of the LC/GDM group were less than 130 g, which belong to strict LC diet [13, 18]. Second, different from studies showing that LC diets were mostly for medical treatment, such as weight loss in obese people and therapy for patients with type 2 diabetes [19, 20], participants in this study were healthy women before pregnancy, who followed a long-term (≧12 months) LC diet to control body mass. To our best knowledge, both Bao’s study in 2014 and Looman’s study in 2018 had suggested that pre-pregnancy LC diet may increase the risk of GDM. The lowest quintile of carbohydrate intakes in these studies were 178 g/d and 162 g/d, respectively. Although the intake of 162 g of carbohydrate/day were taking in less than the recommended 175 g/d, it was higher than the carbohydrate intakes in the LC group in our study [9, 10].
Studies had suggested that the higher the OGTT glucose levels were, the more severe the imparied glucose tolerance [21]. While the GDM patients with a LC diet (LC/GDM) showed a more severe impaired glucose tolerance than the GDM with a conventional diet (Con/GDM), our study also indicated that long-term LC diet before pregnancy may be associated with impaired glucose tolerance during pregnancy. The possible explanation was that long-term LC diets make the body mobilize fat for energy, and lipolysis produces more free fatty acids (FFAs) which may lead to insulin resistance (or aggravates pregnant insulin resistance). Although effects of LC diet on maternal FFAs remain unclear [22], Hales’s study on healthy men showed a significant increase in OGTT glucose values and serum free fatty acids (FFAs) after 5 days of LC diet [23]. Hernandez’s study in 2014 show the concentration of FFAs in the LC diet group (carbohydrates 40%, fat 45%, protein 15%) was significantly higher than that of the high-carbohydrate diet group (carbohydrates 60%, fat 25%, protein 15%) [24]. Existing mechanistic studies also confirmed that the increase in serum FFAs can cause lipotoxicity through endoplasmic reticulum stress [25], reactive oxygen species [26], apoptosis, and inflammatory response [27], which leads to insulin resistance [28, 29]. Another possible explanation was degenerated function of pancreatic islet because of long-term low carbohydrate load in the LC group. Our study showed that HbA1c levels in the LC/GDM group were 5.14% (33 mmol/mol) and 4.90% (30 mmol/mol) in the first and the second trimesters, respectively, which were the lowest among the three groups. The HbA1c levels suggested that the participants in the LC/GDM group might had a long-term low carbohydrate load. Animal studies reported in 2014 showed that a reduction in β-cell mass was observed in mice on long-term LC diet (22 weeks) [30]. Our ongoing animal experiments also found that an LC diet for 4 weeks led to a decrease in the number of pancreatic islet β-cells in mice (to be reported separately).
To support the growth of the fetus in the second trimester, the intakes of total energy and carbohydrate in the LC/GDM group increased compared with those before pregnancy, but there were still six participants whose carbohydrate intakes less than 130 g/d. When carbohydrate intake is low, the body consumes its own adipose tissue as energy, which may produce ketone bodies.
Carbohydrate restriction may also promote maternal ketonemia promoting oxidation of FFA to betahydroxybutyrate and other ketones [22]. This could be the reason that the rate of positive urine ketone bodies in the LC/GDM group was 25% in the second trimester, which was significantly higher than that in the other two groups. According to the current GDM diagnosis and treatment guidelines in IPMCH [31], women dignosed with GDM were given medical nutritional care, the participants in the LC/GDM were advised to increase their carbohydrate intake appropriately, we observed the rate of positive urine ketone bodies was decreased to 5% in the third trimester.
Notably, the Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS) found the higher OGTT levels were associated with adverse outcome, such as macrosomia, cesarean delivery, neonatal hypoglycemia [32]. Furthermore, Hiersch et al. reported the more abnormal OGTT points during pregnancy, the higher the risk of type 2 diabetes after delivery [33]. Nishikawa et al. also found that the higher the level of OGTT-1 h, the higher the risk of impaired glucose tolerance after delivery [34]. Therefore, the abnormal glucose metabolism during pregnancy found in the LC/GDM population is particularly worthy of attention, and it provides a warning about the future risk of type 2 diabetes in the population with an LC diet. These findings highlight the urgent need for large-population, long time follow-up cohort studies on the long-term health effects of LC diets.
This study was designed to explore the relationship between a strict LC diet before pregnancy and glucose tolerance during pregnancy. Moreover, all the study participants were included during the similar time period, the food profiles were comparable among them. Different groups were matched by age, pre-pregnancy BMI, parity, conception, family history of diabetes and fasting blood glucose in first trimester of pregnancy to minimize the influence of confounding factors. However, there are several limitations to this study. First, the study sample size of the LC diet group was relatively small; however, given that the participants were a specific group of pregnant women, and based on the strict LC diet inclusion criteria, these inevitably limited the number of eligible women. Therefore, to fully compare the groups, we included a GDM conventional diet control group (Con/GDM group) and a healthy control group (Con/Healthy group) with good comparability. Second, assessment of diets is one of the most challenging behavioral assessments. Self-reporting and 24-h recall were combined to review the dietary patterns of the study participants before pregnancy. However, there may be recall bias.
Conclusion
In this study, we observed higher values in OGTT-1 h and OGTT-2 h and higher rate of abnormal values both in OGTT-2 h and OGTT-2 h in the LC/GDM group, compared with the Con/GDM group. The data suggested a relationship between the pre-pregnancy low-carbohydrate diet and imparied glucose tolerance during pregnancy. This finding suggests that it is questionable whether women of childbearing age should adopt a LC diet to control weight. It also warrants further studies to understand the effect of pre-pregnancy low-carbohydrate diet behavior on imparied glucose tolerance and its underlying pathophysiology.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- LC:
-
Low-carbohydrate
- OGTT:
-
Oral glucose tolerance test
- GDM:
-
Gestational diabetes mellitus
- LC/GDM:
-
GDM women with the low-carbohydrate diet
- Con/GDM:
-
GDM women with the conventional diet
- Con/Healthy:
-
Women with conventional diet but without GDM
- IPMCH:
-
The International Peace Maternity and Child Health Hospital
- IADPSG:
-
The International Association of the Diabetes and Pregnancy Study Groups
- HbA1c:
-
Glycated haemoglobin
- TC:
-
Total cholesterol
- TG:
-
Triacylglycerol
- HDLC:
-
High density lipoprotein cholesterol
- LDLC:
-
Low density lipoprotein cholesterol
- LGA:
-
Large-for gestational age
- SGA:
-
Small-for gestational age
- FBG:
-
Fasting blood glucose
- AUC:
-
Area under the blood glucose curve
- GA:
-
Glycated albumin
- SD:
-
Standard deviation
- FFAs:
-
Free fatty acids
References
Saravanan P, Diabetes in Pregnancy Working G, Maternal Medicine Clinical Study G, Royal College of O, Gynaecologists UK. Gestational diabetes: opportunities for improving maternal and child health. Lancet Diabetes Endocrinol. 2020;8(9):793–800.
Wang WJ, Zhang L, Zheng T, et al. Fetuin-A and fetal growth in gestational diabetes mellitus. BMJ Open Diabetes Res Care. 2020;8(1):e000864.
Gao C, Sun X, Lu L, Liu F, Yuan J. Prevalence of gestational diabetes mellitus in mainland China: A systematic review and meta-analysis. J Diabetes Investig. 2019;10(1):154–62.
Grunnet LG, Hansen S, Hjort L, et al. Adiposity, Dysmetabolic Traits, and Earlier Onset of Female Puberty in Adolescent Offspring of Women With Gestational Diabetes Mellitus: A Clinical Study Within the Danish National Birth Cohort. Diabetes Care. 2017;40(12):1746–55.
Gestational diabetes mellitus. Nat Rev Dis Primers. 2019;5(1):48.
Mijatovic-Vukas J, Capling L, Cheng S, et al. Associations of Diet and Physical Activity with Risk for Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients. 2018;10(6):698.
Jovanovicpeterson L, Peterson CM. Dietary Manipulation as a Primary-Treatment Strategy for Pregnancies Complicated by Diabetes. J Am Coll Nutr. 1990;9(4):320–5.
Bliss M. The discovery of insulin. 25th anniversary ed. Chicago: University of Chicago Press; 2007.
Bao W, Bowers K, Tobias DK, et al. Prepregnancy low-carbohydrate dietary pattern and risk of gestational diabetes mellitus: a prospective cohort study. Am J Clin Nutr. 2014;99(6):1378–84.
Looman M, Schoenaker D, Soedamah-Muthu SS, Geelen A, Feskens EJM, Mishra GD. Pre-pregnancy dietary carbohydrate quantity and quality, and risk of developing gestational diabetes: the Australian Longitudinal Study on Women’s Health. Br J Nutr. 2018;120(4):435–44.
Chawla S, Tessarolo Silva F, Amaral Medeiros S, Mekary RA, Radenkovic D. The Effect of Low-Fat and Low-Carbohydrate Diets on Weight Loss and Lipid Levels: A Systematic Review and Meta-Analysis. Nutrients. 2020;12(12):3774.
Medicine I, Board F, Macronutrients A, Intakes S, Intakes S. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients). 2005.
Goldenberg JZ, Day A, Brinkworth GD, et al. Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: systematic review and meta-analysis of published and unpublished randomized trial data. Bmj-Brit Med J. 2021;372:m4743.
Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition. 2015;31(1):1–13.
Zhou BF. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15(1):83–96.
Sacks DA, Hadden DR, Maresh M, et al. Frequency of gestational diabetes mellitus at collaborating centers based on IADPSG consensus panel-recommended criteria: the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. Diabetes Care. 2012;35(3):526–8.
Tian X, Huang Y, Wang H. Deviation of Chinese Adults’ Diet from the Chinese Food Pagoda 2016 and Its Association with Adiposity. Nutrients. 2017;9(9):995.
Sato J, Kanazawa A, Makita S, et al. A randomized controlled trial of 130 g/day low-carbohydrate diet in type 2 diabetes with poor glycemic control. Clin Nutr. 2017;36(4):992–1000.
Wang LL, Wang Q, Hong Y, et al. The Effect of Low-Carbohydrate Diet on Glycemic Control in Patients with Type 2 Diabetes Mellitus. Nutrients. 2018;10(6):661.
Nordmann AJ, Nordmann A, Briel M, et al. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Arch Intern Med. 2006;166(3):285–93.
Yerlikaya G, Falcone V, Stopp T, et al. To Predict the Requirement of Pharmacotherapy by OGTT Glucose Levels in Women with GDM Classified by the IADPSG Criteria. J Diabetes Res. 2018;2018:3243754.
Sweeting A, Mijatovic J, Brinkworth GD, et al. The Carbohydrate Threshold in Pregnancy and Gestational Diabetes: How Low Can We Go? Nutrients. 2021;13(8):2599.
Hales CN, Randle PJ. Effects of low-carbohydrate diet and diabetes mellitus on plasma concentrations of glucose, non-esterified fatty acid, and insulin during oral glucose-tolerance tests. Lancet. 1963;1(7285):790–4.
Hernandez TL, Van Pelt RE, Anderson MA, et al. A Higher- Complex Carbohydrate Diet in Gestational Diabetes Mellitus Achieves Glucose Targets and Lowers Postprandial Lipids: A Randomized Crossover Study. Diabetes Care. 2014;37(5):1254–62.
Legrand Poels S, Esser N, L’homme L, Scheen A, Paquot N, Piette J. Free fatty acids as modulators of the NLRP3 inflammasome in obesity/type 2 diabetes. Biochem Pharmacol. 2014;92(1):131–41.
Gao D, Nong SW, Huang XQ, et al. The Effects of Palmitate on Hepatic Insulin Resistance Are Mediated by NADPH Oxidase 3-derived Reactive Oxygen Species through JNK and p38(MAPK) Pathways. J Biol Chem. 2010;285(39):29965–73.
Sramek J, Nemcova-Furstova V, Kovar J. Kinase Signaling in Apoptosis Induced by Saturated Fatty Acids in Pancreatic beta-Cells. Int J Mol Sci. 2016;17(9):1400.
Boden G. Effects of free fatty acids (FFA) on glucose metabolism: Significance for insulin resistance and type 2 diabetes. Exp Clin Endocr Diab. 2003;111(3):121–4.
Kraegen EW, Cooney GJ. Free fatty acids and skeletal muscle insulin resistance. Curr Opin Lipidol. 2008;19(3):235–41.
Ellenbroek JH, van Dijck L, Tons HA, et al. Long-term ketogenic diet causes glucose intolerance and reduced beta- and alpha-cell mass but no weight loss in mice. Am J Physiol-Endoc M. 2014;306(5):E552–8.
Obstetrics Group of Chinese Medical Association. Guideline for Diagnosis and Treatment of Gestational Diabetes Mellitus (2014). Zhonghua Fu Chan Ke Za Zhi. 2014;49(8):561–71.
Lowe WL Jr, Scholtens DM, Kuang A, et al. Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS): Maternal Gestational Diabetes Mellitus and Childhood Glucose Metabolism. Diabetes Care. 2019;42(3):372–80.
Hiersch L, Shah BR, Berger H, et al. Oral Glucose Tolerance Test Results in Pregnancy Can Be Used to Individualize the Risk of Future Maternal Type 2 Diabetes Mellitus in Women With Gestational Diabetes Mellitus. Diabetes Care. 2021;44(8):1860–7.
Nishikawa T, Ono K, Hashimoto S, et al. One-hour oral glucose tolerance test plasma glucose at gestational diabetes diagnosis is a common predictor of the need for insulin therapy in pregnancy and postpartum impaired glucose tolerance. J Diabetes Investig. 2018;9(6):1370–7.
Acknowledgements
The authors would like to thank all the participants in the survey.
Funding
This work was supported by the Foundation of International Peace Maternity and Child Health Hospital for technical support (grant number CR2018SY04).
Author information
Authors and Affiliations
Contributions
WS obtained the funding. YH, LQ, and WS conceived and designed the study. YH, LQ, YG, LM, MG,YZ, YJ, QG, and YZ contributed to the data collection and analysis plans. YH and LQ drafted the manuscript. WS had primary responsibility for final content. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of the International Peace Maternal and Infant Hospital (IPMCH) of Shanghai (GKLW2018-35). Written informed consent was obtained from all participants. This study was conducted according to the guidelines laid down in the Declaration of Helsinki.
Consent for publication
Not applicable. Only anonymized data were used.
Competing interests
There is no any conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
STable 1. Recommended range of macronutrient intakes from Chinese Dietary Reference Intakes. STable 2. Carbohydrate intake habit of LC/GDM group
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hao, Y., Qu, L., Guo, Y. et al. Association of pre-pregnancy low-carbohydrate diet with maternal oral glucose tolerance test levels in gestational diabetes. BMC Pregnancy Childbirth 22, 734 (2022). https://doi.org/10.1186/s12884-022-05059-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-022-05059-2