
Abstract
Background
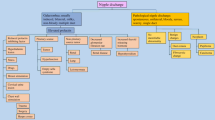
Painless bloody nipple discharge is often classified as pathological due to its association with malignant lesions. However, it can also be a completely harmless condition. Rusty pipe syndrome is a rare cause of benign, self-limiting bloody nipple discharge during late pregnancy and early lactation. Given that rusty pipe syndrome is not described in conventional textbooks, we thought it would be appropriate to bring this benign disease to the notice of readers.
Case presentation
A 31-year-old G1P1 female delivered an infant with a birth weight of 3000 g via cesarean section at 39 weeks of gestation. The baby was admitted to the pediatric intensive care unit for a suspected oblique inguinal hernia. The mother had bilateral painless bloody nipple discharge when she started to express milk. A physical examination uncovered no signs of inflammation, engorgement, palpable mass, tenderness, cracks or ulcers. A breast ultrasound and cytological analysis revealed no signs of a neoplasm. Without any medical intervention, the color of the rusty milk changed from dark brown to light brown during hospitalization and finally resolved six days postpartum.
Conclusion
Rusty pipe syndrome is a self-limiting benign condition that should be considered in the differential diagnosis of bloody nipple discharge. Awareness of this rare disease by medical professionals would be extremely beneficial for avoiding unneeded examinations and discontinuity of exclusive breastfeeding.
Similar content being viewed by others


Background
Human milk is considered the gold standard for infant feeding [1]. However, several problems can occur during the lactation period and compromise the breastfeeding rate. In clinical practice, a bloody nipple discharge during pregnancy or lactation is a rarely encountered symptom that results in significant patient worry and prompts medical evaluation and intervention [2]. Rusty pipe syndrome (RPS) is a benign physiological condition that occurs in primiparous women. RPS typically presents with brown or bloody milk mimicking flowing water from a rusty pipe; it is usually bilateral, painless, and self-limiting [3]. Most cases will clear within seven days without any medical treatment [4,5,6,7,8,9,10,11,12,13,14,15,16]. There are not many case reports on this topic, and its occurrence in China is quite rare. Due to the underrecognized and underdiagnosed condition of RPS, we conducted a review of blood-stained discharge of the breast and reported a case of RPS in a 31-year-old woman to achieve several objectives: first, to identify the clinical manifestation and lab characteristics of RPS; second, to discuss what doctors should do when faced with self-healable bloody nipple discharge when there are no masses in the breasts and what evidence is required before making a diagnosis.
Case report
A 31-year-old primipara delivered an infant with a birth weight of 3000 g via cesarean section at 39 weeks of gestation. After delivery, the infant was transferred to the neonatal intensive care unit after being diagnosed with an oblique inguinal hernia. Due to the separation of the mother and baby, the patient could only express milk and send it to the baby. The mother noticed a bilateral painless bloody nipple discharge when she expressed milk (Fig. 1). She told the doctor that this phenomenon occurred as early as 36 weeks of pregnancy. She denied experiencing any infection or trauma, and reported no suckling by the baby. The patient had no family history of any breast disease. She was in good health and denied having any alcohol or drug during pregnancy. A physical examination found no signs of inflammation, engorgement, palpable mass, or tenderness on either breast, and no cracks or ulcers on the nipples. Breast ultrasound imaging revealed lobular hyperplasia and mild ductal ectasia with no breast cyst, solid nodule, or enlarged lymph nodes. Cytological analysis of the milk showed large numbers of inflammatory cells, polynuclear macrophages, and a small number of epithelial cells with no signs of atypia (Fig. 2). A surgical consultation was obtained, and intraductal papilloma was ruled out as a cause because the blood-stained breastmilk was bilateral and emanated from multiple ducts. The patient was advised to express milk from her breasts every three hours to avoid breast engorgement and support continued breastfeeding. The rusty milk color changed from dark brown to light brown during hospitalization and finally resolved spontaneously six days after delivery, with no recurrence. Additional formula milk was given to the baby at first, but at discharge on the sixth day, the baby was exclusively breastfed. The mother-infant pair was followed up in the postpartum clinic for six months. Postpartum follow-up has revealed no evidence of neoplastic changes thus far. This case report follows the CARE Guidelines. Informed consent was obtained from the patient for publication.

Breast milk color of the patient with Rusty pipe syndrome (camera, HUAWEI P30pro)

Cytological smear of nipple discharge showing mammary epithelial cells and inflammatory cells (hematoxylin–eosin stain; microscope, LEICA DM2500/ × 40; software, NIS-Elements F 4.60.00 64-bit; camera, Nikon DS-Fi3;scale bars, 100 μm)
Discussion and conclusions
Bloody nipple discharge tends to coincide with symptomatic dysfunction of the ductal system and the potential presence of a subclinical malignancy in nonpregnant women [17]. Many authors have studied the relationship between bloody nipple discharge and breast carcinoma, observing that malignancy occurs in 8–30% of women with bloody discharge [18,19,20,21,22,23,24]. The occurrence of blood-stained nipple discharge is rare during pregnancy, and its prevalence is estimated to be approximately 0.1% [25]. It may cause great anxiety to the patient because of the perceived link with breast carcinoma in nonpregnant patients [26]. However, blood-stained milk may occur as a result of physiological changes during late pregnancy and the early lactation period. One such condition can be RPS, a self-limiting condition that presents as painless bloody or brown discharge in pregnant and postpartum women. Bloody nipple discharge correlates with proliferation of the duct epithelium. The capillary network around mammary ducts is fragile due to hormonal stimuli (estrogen, progesterone, oxytocin) and is easily traumatized, resulting in blood cells leaking into breast secretions [12, 16, 27].
To date, only 16 cases diagnosed with RPS have been reported (including one in this paper) [3,4,5,6,7,8,9,10,11,12,13,14,15,16]. A review of RPS cases including clinical manifestations and auxiliary examinations are summarized in Table 1. As shown in Table 1, the abnormal discharge was bilateral in all patients. Among those cases, 15 patients were primiparas, while one patient was a secundipara. For the secundipara described by Faridi [13], brown–red colored milk occurred both in her first and second pregnancies, while the other cases only had one occurrence. In the literature, RPS usually presents in the second or third trimester, or within the first few days of lactation: four mothers observed a bloody discharge several weeks before delivery (from the 26th to 36th week of gestation), while another 11 mothers started to have blood-stained milk within two days postnatally. The abnormal color of the milk faded away spontaneously in a progressive manner and completely disappeared in ten days. A follow-up of these patients ranging from six weeks to six months revealed no evidence of neoplastic changes on physical examination. Lactation was achieved successfully in all women who intended to breastfeed.
RPS can mimic more serious diseases, such as breast cancer. To minimize the rate of misdiagnosis, it is necessary to carefully assess and thoroughly understand the appearance of various benign and malignant breast lesions. A thorough physical examination may quickly differentiate conditions such as trauma, broken nipple, and mastitis. The most common cause of pathological nipple discharge is ductal papilloma, which accounts for 35–57% of cases, followed by duct ectasia (17–36%) and malignant lesions (4–21%) [28, 29]. Pregnancy-associated breast cancer (PABC) is defined as breast cancer diagnosed during pregnancy or in the first year of lactation. Most patients with PABC present with an asymptomatic mammary mass (not everyone does), and bloody nipple discharge, breast swelling, and pain are less frequent symptoms. King et al. reported on 63 cases of PABC, and three of them exhibited bloody nipple discharge [30]. Bloody nipple discharge and/or nipple retraction were reported in 8% of PABC patients in a study by Taskin et al. [31]. Wang et al. evaluated 142 patients with PABC, four of whom presented with papillary hemorrhagic discharge [32]. However, little information was available in the cases described by King, Taskin, and Wang. Disease status, time of onset, and discharge location were all lacking. Intraductal papilloma is often associated with unilateral, painless, bloody or serous nipple discharge in premenopausal women and is rarely observed in pregnant women. Cheah et al. described a patient presenting with a left breast mass (later identified as a benign papilloma) with bloody nipple discharge at 20 weeks of gestation [33]. Intraductal papilloma should be considered a differential diagnosis and excluded to diagnose RPS. Patients with mammary duct ectasia typically present with intermittent nipple discharge, swelling, and mild erythema near the areola [34]. Notwithstanding the extremely rare coexistence of pregnancy and the abovementioned diseases, such pathological conditions should be ruled out before RPS is diagnosed.
The first diagnosis of RPS is established by the history of the present illness and regular physical examination, followed by specific tests, such as cytological analysis of the bloody discharge and breast ultrasonography, if necessary. The available literature offers a mixed opinion on whether obtaining a cytological smear is strictly required. The diagnostic accuracy of nipple discharge fluid cytology for the detection of breast cancer is poor, while specificity and sensitivity data vary among published clinical studies. A meta-analysis from Jiwa et al. indicated that the sensitivity of nipple smear cytology was approximately 75% with a specificity of 87% [35]. Nipple discharge cytology is deemed difficult to diagnose given the presence of atypical cellular changes unrelated to a malignancy and the variability of interpretation by pathologists. Even though the clinical utility of cytology is limited, researchers discovered that the diagnostic accuracy of nipple smear cytology is similar to that of other available diagnostic methods, such as breast ultrasound and MRI [35]. Regarding imaging, the most suitable radiologic approach for assessing breast problems in pregnant and lactating women is ultrasound [27, 36]. The physiological changes of lactating breasts present as lobular hyperplasia and ductal ectasia, resulting in the sonographic appearance of large, hypoechoic ducts and lobules on a background of diffusely reduced breast echogenicity [37, 38]. Ultrasound images obtained from patients with RPS show similar physiological characteristics [6,7,8, 14, 16]. All masses discovered during pregnancy and breastfeeding should be thoroughly assessed, since nonrelevant or physiological masses caused by hormonal stimulation can only be diagnosed after a thorough radiologic examination [39]. Thus, patients presenting with unremitting bloody nipple discharge should urgently undergo a triple assessment (clinical, imaging, and pathological findings) due to the increased prevalence of breast cancer. Unless the lump is growing quickly or there is discordance in the triple assessment, a core needle biopsy or surgery is not recommended in pregnant or lactating women.
A variety of management approaches are reported in our review, ranging from reassurance only to temporarily discarding expressed breast milk and using formula instead. If the infant tolerates the milk, breast feeding is encouraged during this period. The prognosis of RPS is good; the blood-stained discharge should clear within seven days for most cases, and only one report showed bloody milk fully resolved by day ten [16]. The patients should be followed up regularly at least until the milk color is normal. If bloody milk continues for more than one week, further investigation, such as ultrasound and cytology analysis, should be carried out to rule out pathological causes. Long-term clinical follow-up appears normal on physical examination with no evidence of neoplastic alterations [5, 13, 14, 16]. The presence of RPS would not have a poor prognosis for neonates either. The results of the current follow-up show that breastfed babies are free from diseases such as growth retardation and breast milk intolerance [3, 5, 13]. Early diagnosis of this rare, self-limiting disease by obstetricians or neonatologists, followed by telling the mother that her infant would be unaffected by the small quantity of blood consumed, would be extremely beneficial in avoiding unneeded examinations and the discontinuation of exclusive breastfeeding.
Availability of data and materials
All data generated for this study are available on request to the corresponding author.
Abbreviations
- RPS:
-
Rusty pipe syndrome
- G1P1:
-
Gravida1 para1
- PABC:
-
Pregnancy-associated breast cancer
References
Bartick M, Hernandez-Aguilar MT, Wight N, Mitchell KB, Simon L, Hanley L, Meltzer-Brody S, Lawrence RM. ABM clinical protocol #35: supporting breastfeeding during maternal or child hospitalization. Breastfeed Med. 2021;16(9):664–74.
Lafreniere R. Bloody nipple discharge during pregnancy: a rationale for conservative treatment. J Surg Oncol. 1990;43(4):228–30.
Katarzyna W, Malgorzata P, Agata WP, Wioletta M, Jan M, Katarzyna R, Maciej W. Blood-stained colostrum: a rare phenomenon at an early lactation stage. Children (Basel). 2022;9(2):213.
Low JM, Amin Z, Ng YPM. Early recognition of rusty pipe syndrome to avoid disruption of breast feeding. Arch Dis Child Fetal Neonatal Ed. 2022;107(3):241.
Kural B, Sapmaz S. Rusty pipe syndrome and review of literature. Breastfeed Med. 2020;15(9):595–7.
Anil K, Sushma N, Murugesan A, Ravi T, Rimesh P. Rusty pipe syndrome: a benign cause of altered breast milk color in lactating mothers. Acad J Ped Neonatol. 2020;8(4):555800.
Mohamad N, Sulaiman Z, Tengku Ismail TA, Ahmad S. Bloody Nipple Discharge Post Delivery: A Case of "Rusty Pipe Syndrome". Korean J Fam Med. 2021;42(4):339–41.
Deboni FA, Moldenhauer M, do-Nascimento MBR. “Rusty pipe” syndrome: benign and rare cause of bloody nipple discharge during breastfeeding - case report. Residência Pediátrica. 2018;8(3):151–3.
Çintesun E, Gül A, Akar S, Ezveci H, Çelik Ç. Rusty pipe syndrome. Perinatal J. 2017;25(2):85–6.
Silva JR, Carvalho R, Maia C, Osorio M, Barbosa M. Rusty pipe syndrome, a cause of bloody nipple discharge: case report. Breastfeed Med. 2014;9(8):411–2.
Cizmeci MN, Kanburoglu MK, Akelma AZ, Tatli MM. Rusty-pipe syndrome: a rare cause of change in the color of breastmilk. Breastfeed Med. 2013;8(3):340–1.
Usharani Thota VMM, Jampana VR. Rusty pipe syndrome: a case report. Health. 2013;5:157–8.
Faridi MM, Dewan P, Batra P. Rusty pipe syndrome: counselling a key intervention. Breastfeed Rev. 2013;21(3):27–30.
Guèye M, Kane-Guèye SM, Mbaye M, Ndiaye-Guèye MD, Faye-Diémé ME, Diouf AA, Niang MM, Moreau JC. Rusty pipe syndrome in a 22-year-old primigravida at 26 weeks’ gestation. S Afr J Obstet Gynaecol. 2013;19(1):17–8.
Virdi VS, Goraya JS, Khadwal A. Rusty-pipe syndrome. Indian Pediatr. 2001;38(8):931–2.
Barco I, Vidal MC, Barco J, Badia A, Piqueras M, Garcia A, Pessarrodona A. Blood-stained colostrum and human milk during pregnancy and early lactation. J Hum Lact. 2014;30(4):413–5.
Chen L, Zhou WB, Zhao Y, Liu XA, Ding Q, Zha XM, Wang S. Bloody nipple discharge is a predictor of breast cancer risk: a meta-analysis. Breast Cancer Res Treat. 2012;132(1):9–14.
Dolan RT, Butler JS, Kell MR, Gorey TF, Stokes MA. Nipple discharge and the efficacy of duct cytology in evaluating breast cancer risk. Surgeon. 2010;8(5):252–8.
Montroni I, Santini D, Zucchini G, Fiacchi M, Zanotti S, Ugolini G, Manaresi A, Taffurelli M. Nipple discharge: is its significance as a risk factor for breast cancer fully understood? Observational study including 915 consecutive patients who underwent selective duct excision. Breast Cancer Res Treat. 2010;123(3):895–900.
Sanders LM, Daigle M. The rightful role of MRI after negative conventional imaging in the management of bloody nipple discharge. Breast J. 2016;22(2):209–12.
Wong Chung JE, Jeuriens-van de Ven SA, van Helmond N, Wauters CA, Duijm LE, Strobbe LJ. Does nipple discharge color predict (pre-) malignant breast pathology? Breast J. 2016;22(2):202–8.
Makita M, Akiyama F, Gomi N, Iwase T. Mammary ductoscopy and watchful follow-up substitute microdochectomy in patients with bloody nipple discharge. Breast Cancer. 2016;23(2):242–51.
Sauter ER, Schlatter L, Lininger J, Hewett JE. The association of bloody nipple discharge with breast pathology. Surgery. 2004;136(4):780–5.
Cabioglu N, Hunt KK, Singletary SE, Stephens TW, Marcy S, Meric F, Ross MI, Babiera GV, Ames FC, Kuerer HM. Surgical decision making and factors determining a diagnosis of breast carcinoma in women presenting with nipple discharge. J Am Coll Surg. 2003;196(3):354–64.
Merlob P, Aloni R, Prager H, Mor N, Litwin A. Blood-stained maternal milk: prevalence, characteristics and counselling. Eur J Obstet Gynecol Reprod Biol. 1990;35(2–3):153–7.
Ando N, Iwamitsu Y, Kuranami M, Okazaki S, Wada M, Yamamoto K, Todoroki K, Watanabe M, Miyaoka H. Psychological characteristics and subjective symptoms as determinants of psychological distress in patients prior to breast cancer diagnosis. Support Care Cancer. 2009;17(11):1361–70.
Sabate JM, Clotet M, Torrubia S, Gomez A, Guerrero R, de las Heras P, Lerma E. Radiologic evaluation of breast disorders related to pregnancy and lactation. Radiographics. 2007;27(Suppl 1):S101-124.
Nelson RS, Hoehn JL. Twenty-year outcome following central duct resection for bloody nipple discharge. Ann Surg. 2006;243(4):522–4.
Soleimani V, Jahanbin B. Breast Cytology and pathology in pregnancy and lactation. Adv Exp Med Biol. 2020;1252:27–32.
King RM, Welch JS, Martin JK Jr, Coulam CB. Carcinoma of the breast associated with pregnancy. Surg Gynecol Obstet. 1985;160(3):228–32.
Taskin F, Polat Y, Erdogdu IH, Soyder A. Pregnancy-associated breast cancer: a review of 47 women. Clin Imaging. 2019;58:182–6.
Wang B, Yang Y, Jiang Z, Zhao J, Mao Y, Liu J, Zhang J. Clinicopathological characteristics, diagnosis, and prognosis of pregnancy-associated breast cancer. Thorac Cancer. 2019;10(5):1060–8.
Cheah SD, Imi Sairi AH. Large breast lump with bloody nipple discharge: benign intraductal papilloma. BMJ Case Rep. 2020;13(11):e236818.
Hamwi MW, Winters R. Mammary Duct Ectasia. Treasure Island (FL): StatPearls; 2021.
Jiwa N, Kumar S, Gandhewar R, Chauhan H, Nagarajan V, Wright C, Hadjiminas D, Takats Z, Ashrafian H, Leff DR. Diagnostic accuracy of nipple discharge fluid cytology: a meta-analysis and systematic review of the literature. Ann Surg Oncol. 2022;29(3):1774–86.
Ahn BY, Kim HH, Moon WK, Pisano ED, Kim HS, Cha ES, Kim JS, Oh KK, Park SH. Pregnancy- and lactation-associated breast cancer: mammographic and sonographic findings. J Ultrasound Med. 2003;22(5):491–7 quiz 498-499.
Kieturakis AJ, Wahab RA, Vijapura C, Mahoney MC. Current recommendations for breast imaging of the pregnant and lactating patient. AJR Am J Roentgenol. 2021;216(6):1462–75.
Sharma R, Tzetzo S, Patel S, Zachariah M, Sharma S, Melendy T. BK virus in kidney transplant: current concepts, recent advances, and future directions. Exp Clin Transplant. 2016;14(4):377–84.
de Holanda AA, Goncalves AK, de Medeiros RD, de Oliveira AM, Maranhao TM. Ultrasound findings of the physiological changes and most common breast diseases during pregnancy and lactation. Radiol Bras. 2016;49(6):389–96.
Acknowledgements
Not applicable
Funding
Our work was supported by the National Key Research and Development Program of China (No.2018YFC1005003, 2021YFC2700601).
Author information
Authors and Affiliations
Contributions
All the authors have read and approved the manuscript. HT wrote the first draft. WZ and JC conducted the patient interviews and modified the manuscript. DZ contributed to the conception of the study and revised the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethnic Committee of the Women’s Hospital, School of Medicine, Zhejiang University (Number: IRB‐20220056‐R). All data were collected from the electronic medical record system in the hospital.
Consent for publication
A written informed consent was obtained from the patient for publication of this case report. A copy of the written consent is available for review by the editor of the journal.
Competing interests
The authors have no conflicts of interests to declare or competing financial interests regarding this report.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tang, H., Zhu, W., Chen, J. et al. Rusty pipe syndrome: a case report and review of the literature. BMC Pregnancy Childbirth 22, 770 (2022). https://doi.org/10.1186/s12884-022-05048-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-022-05048-5