
Abstract
Background
Prenatal corticosteroid administration is known to be an effective strategy in improving fetal pulmonary maturity. This study aimed to evaluate the impact of maternal betamethasone administration on fetal pulmonary and other arteries Doppler velocity and the correlation between RDS development and Doppler indices results.
Methods
Fifty one singleton pregnancies between 26 and 34 gestational weeks with a diagnosis of preterm labor were included in the exposed group and received betamethasone. Fifty one uncomplicated pregnancies were included in the non-exposed group. Fetal pulmonary, umbilical and middle cerebral arteries Doppler parameters were evaluated before and 24 to 48 h after steroid administration in the exposed group and two times at same intervals in the non-exposed group. Maternal records were matched to neonatal charts if delivery happened, and demographic and outcome data were abstracted.
Results
When compared with the nonexposed group, fetuses treated with corticosteroids demonstrated significantly decreased umbilical artery Pulsatility index (PI) and significantly increased the middle cerebral artery PI, pulmonary artery Acceleration time (AT) and pulmonary artery AT/ET (Ejection time), while all other indices remained similar. We found significantly decreased pulmonary artery AT in the fetuses with respiratory distress syndrome (RDS) compared to those that did not.
Conclusions
The results of our study showed that maternal antenatal betamethasone administration caused significant changes in the fetus blood velocity waveforms and also affected the blood flow in the pulmonary artery which led to an increase in the pulmonary artery AT and AT/ET. Among those fetuses with RDS, we found a significant decrease in the pulmonary artery AT, but we did not observe any pulmonary artery AT/ET differences.
Similar content being viewed by others

Introduction
Preterm birth, described by the world health organization (WHO) as delivery before 37 weeks of gestation, is a leading cause of neonatal morbidity and mortality [1].
Preterm birth is a risk factor in over 50 % of all neonatal deaths. In addition, preterm birth can result in a range of problems and long-term loss of human potential among survivors. Respiratory distress syndrome due to immaturity of fetal lungs, is one of the major complications for the fetus in preterm labor [1, 2].
The past few decades have seen significant development in outcomes for preterm infants due to the introduction of sophisticated neonatal ventilation, the use of exogenous surfactant, and the administration of antenatal steroid. When used appropriately, antenatal steroid administration is one of the most important and beneficial treatments used in perinatal medicine today. The two glucocorticoids in most common clinical use are dexamethasone and betamethasone [2, 3]. There are two different courses of standard corticosteroid therapy to accelerate fetal lung maturation: 1. Administration of betamethasone 12 mg intramuscularly and repetition of the same dose 24 h later 2. Dexamethasone 6 mg intravenously and its repetition every 12 h for up to 4 doses [4, 5]. The mechanism by which corticosteroids improve the respiratory status is unclear.
Antenatal administration of corticosteroids accelerate lung maturation. The normal thinning of the double capillary loops, to form the thin gas exchanging walls of alveoli, is accelerated, resulting in fast alveolisation. The maturation of surfactant producing type II pneumocytes is also speeded up. Although the alveolisation occurs rapidly as a result of the corticosteroids [2, 6].
Pulmonary surfactant is produced by type II pneumocyte. Surfactant phospholipids have surface tension reducing properties, while the surfactant proteins are important in regulating surfactant function, and may also have an immunomodulatory role [6, 7].
Evaluation of fetal lung maturity is one of the critical issues in managing pregnant patients at risk of preterm delivery. Diagnosis of fetal lung maturity is traditionally based on amniocentesis and measurement of the lecithin to sphingomyelin ratio, phosphatidylglycerol, fluorescence polarization test, foam or shake test, and counting the number of lamellar bodies in the amniotic fluid. Nevertheless, amniocentesis is an invasive procedure that must be performed according to its indications [8,9,10].
For these reasons, the use of noninvasive methods such as ultrasound to assess the fetal lung maturity has been considered in various cases. So far, efforts to predict fetal lung maturity based on ultrasound examination of lung volume, epiphysis centers, placental grading, and estimated fetal weight have been performed but has not been very successful in the clinical application [11,12,13,14].
During pregnancy, as the fetal lung develops, the vascular structure of the lungs changes, the amount of the smooth muscle tissue increases, and the level of pulmonary vascular resistance decreases, leading to a gradual increase in pulmonary blood flow. Doppler velocimetry can be a noninvasive method for assessing the fetal lung blood flow [15, 16].
Prenatal corticosteroid administration may increase the production of surfactant in the fetal lungs, which may increase the pulmonary artery blood flow probably due to accelerated lung maturation and its effect on the vascular structure [15, 17, 18] .
Although effects of betamethasone on fetal hemodynamics have been documented in some studies, the possible mechanisms underlying these alterations are still unclear. One of the possible theories to explain modifications in the fetal circulation associated with reduced placental resistance is based on an increased secretion of placental corticotropin-releasing hormone (CRH) after exogenous administration of corticosteroids, which consecutively causes nitric oxide-mediated vasodilatation [19, 20].
Another possibility is associated with increased fetal blood pressure. Experimental studies have shown that administration of betamethasone to fetal sheep causes an increase in blood pressure [21]. Furthermore, antenatal corticosteroid administration has been found to increase blood pressure levels in preterm newborns during the first days of life [22] .
This study aimed to evaluate the effect of maternal betamethasone administration on fetal pulmonary, umbilical and middle cerebral arteries Doppler indices and to investigate their relationship with the incidence of neonatal respiratory distress syndrome.
Materials and methods
We conducted a prospective cohort study between October 2019 and August 2020. This study was approved by the ethics committee of Shiraz University of Medical Sciences (ethics code: IR.SUMS.REC.1399.351) and written informed consent was obtained from all participants in the study. In the exposed group, singleton pregnancies between 26 and 34 gestational weeks with a diagnosis of preterm labor (evidence of cervical dilatation or uterine contraction in nonstress test) who were candidates for corticosteroid administration for lung maturity and had the inclusion criteria were included. In the nonexposed group, uncomplicated singleton pregnancies in the same gestational age range, which had the inclusion criteria, were included.
The inclusion criteria in this study were: existence of appropriate evidence to determine the gestational age, gestational age between 26 and 34 weeks, no consumption of corticosteroids during pregnancy, estimated fetal weight between 10 and 90 percentile, average amniotic fluid volume. Also, lack of evidence of preeclampsia, diabetes, hypertension, peripheral vascular disease, underlying disease requiring corticosteroids, preterm premature rupture of membrane, and vaginal bleeding in the mother.
Exclusion criteria in this study included the existence of chromosomal or structural abnormality in the fetus and occurrence of labor before the second ultrasonography Doppler evaluation.
After reviewing the inclusion criteria, 63 patients with the diagnosis of preterm birth and indication for corticosteroid administration in the exposure group were included in the study. Besides, 54 healthy pregnant women without preterm labor symptoms referred for routine pregnancy care with similar demographic characteristics to the exposed group were included in the study as a nonexposed group by observing other inclusion criteria.
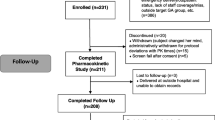
However, during the study, 12 subjects from the exposure group and 3 from the non-exposure group were excluded. Finally, the information of 51 people in each group were completed and used for the final analysis. The study population Fig. 2 shows the number of cases included, repeated measurements and the cases excluded.
After entering the study, information about each participant including the maternal age, demographic characteristics, and gestational age were recorded in the form for each patient. Gestational age was determined based on the patient’s last menstrual information and matched with the first trimester ultrasound.
This study was performed using a GE Voluson E6 (GE Healthcare) ultrasound machine equipped with a 2-5 MHz convex transducer by the trans-abdominal method. Ultrasound was performed in the supine position of the mother. When examining Doppler parameters, all fetuses had sinus rhythm, and the Doppler examination was performed when the fetus was not breathing. The same examiner performed all measurements.
At the beginning of the study in the non-exposed group and before the administration of betamethasone in the exposed group, ultrasound and fetal examination were performed, EFW (Estimated Fetal weight) was measured, and a general sonographic examination of the fetal heart was performed for evidence of fetal heart abnormalities. Also, the following Doppler values were measured: Umbilical Pulsatility Index (UMB PI), Middle Cerebral Artery Pulsatility Index (MCA PI), Middle Cerebral Artery Peak Systolic Velocity (MCA PSV), Pulmonary Artery Pulsatility Index (PA PI), Pulmonary Artery Resistance Index (PA RI), Pulmonary Artery Acceleration Time (PA AT), Pulmonary Artery Ejection Time (PA ET), and Pulmonary Artery AT/ET.
Doppler examination of the umbilical artery was performed in a free segment of the umbilical cord. Doppler examination of the pulmonary artery was performed in a short-axis view when the pulmonary valve and bifurcation and the right and left pulmonary branches were seen. In this study, the pulse doppler sample gate was placed in the middle of the main pulmonary artery (MPA) between the pulmonary valve and the bifurcation site. Doppler examination of the middle cerebral artery (MCA) was performed in the transverse position of the fetal head and a suitable axial section. The MCA Doppler examination was performed in the proximal third portion of the artery.
In all cases of Doppler examination, after applying the image magnification as much as possible, a sample gate of 2 mm was used; also, the angle of insonation (between sound beam and direction of blood flow) was kept below 20 degrees. The blood flow waveform was then displayed with a velocity range of 100 cm/s and a sweep speed of 200 mm/s. The shortest time interval that could be measured was 1 ms.
After obtaining the appropriate Doppler waves, each parameter was measured 3 times and their average was recorded in the patient form. The values of the pulsatility index and resistance index were measured automatically by the ultrasound machine and the values of AT and ET were measured manually as below.
AT (Acceleration time): between the foot to the top of PSV (peak systolic velocity).
ET (Ejection time): from the beginning to the end of the ventricular systole. (Fig. 1).

Schematic presentation of a Doppler flow velocity waveform of main pulmonary artery. AT: acceleration time; ET: ejection time; T: one heart cycle [23]
In the exposure group, 24 to 48 h after receiving the corticosteroid course (two doses of 12 mg betamethasone intramuscularly 24 h apart), the patient underwent ultrasonography again and the above Doppler indices were measured again. In the non-exposed group, all Doppler indices were measured and re-recorded 48 to 72 h after the initial ultrasonographic evaluation.
Also, if the fetus was born within 7 days after the last ultrasound examination, the infant was evaluated for the occurrence of Respiratory Distress Syndrome (RDS). The diagnosis of RDS in this study was based on the presence of at least two of the following three criteria: 1. respiratory signs (tachypnea, retractions and nasal flaring) and persistent oxygen requirement for more than 24 h; 2. administration of surfactant; and 3. radiographic evidence of hyaline membrane disease.
Mean ± SD and frequency (relative frequency) were used to describe the quantitative and qualitative variables, respectively. Kolmogorov-Smirnov normality test, independent t test, paired t test, regression analysis and two way ANOVA test were used to analyze the data (non-parametric test was used when necessary). Statistical analysis was performed using SPSS. v. 22. Statistical significance was defined as P < 0.05.
Results
At the beginning of the study, 63 patients in the exposure group and 54 patients in the non-exposure group were included. However, later, 12 patients in the exposure group were excluded from the study, 4 cases due to delivery before completing the corticosteroid course, 6 cases due to delivery after receiving a corticosteroid course but before the second Doppler examination, and 2 cases due to inability to examine the pulmonary artery Doppler (due to fetal position). In the non-exposed group, three patients were excluded from the study due to refusal to return for a second Doppler examination (Fig. 2).

Flowchart of sample selection in the cohort of 51 exposed (betamethasone) and 51 non-exposed cases
Finally, information of 102 participants in two groups (51 participants in each group) were used in the final analysis. Demographic information about the mothers and fetuses participating in the study is shown in Table 1.
In this study, there was no significant difference between the two groups in terms of maternal age, maternal body mass index, mean gestational age, and estimated fetal weight.
The results of measuring different Doppler parameters (first and second time of examination) in the 2 groups are shown in Table 2. Two way ANOVA analysis of these parameters is shown in Table 3.
At the beginning of the study, there was no statistically significant difference in the values of Doppler indices between the two groups. In the following as presented in Table 2 and Table 3, fetuses from mothers treated with corticosteroid compared to nonexposed group demonstrated significantly decreased umbilical artery PI (0.898 ± 0.079 VS. 0.991 ± 0.093, P < 0.05) and significantly increased MCA PI (2.015 ± 0.239 VS. 1.881 ± 0.121, P < 0.05), pulmonary artery AT (0.063 ± 0.013 VS. 0.055 ± 0.092, P < 0.05) and pulmonary artery AT/ET (0.229 ± 0.043 VS. 0.214 ± 0.031, P < 0.05), while all other indices were similar. Out of 51 patients in the exposure group with diagnosis of preterm labor, 25 cases were delivered within 7 days after the last measurement of Doppler parameters. During this time, no case of labor was seen in the non-exposed group. Out of 25 neonates born due to preterm labor in the exposure group, 8 cases had neonatal respiratory distress syndrome, and 17 neonates did not have symptoms of this syndrome. The mean time interval between the last Doppler examination and the onset of labor was 3.31 ± 0.86 days.
The mean gestational age in the neonates with respiratory distress syndrome was 29.04 ± 0.79 weeks and in neonates without symptoms of respiratory distress syndrome it was 31.5 ± 0.81 (P < 0.05). Table 4 shows the comparison and regression analysis of different fetus parameters and Doppler indices of different vessels (in the last measurement) in infants born in the desired period (1 week from the last Doppler examination) with or without RDS. Pulmonary artery AT values were significantly lower in the neonates affected by RDS (P < 0.05). There were no statistically significant differences in another pulmonary artery Doppler indices results between fetuses who developed RDS and those who did not (Table 4).
In order to evaluate different values of pulmonary Doppler indices in different gestational ages, different parameters measured at the beginning of the study were examined in three different groups of gestational age and are presented in Table 5.
-
Group 1: Gestational age more than 28 weeks and less than 30 weeks
-
Group 2: Gestational age 30 ≤ and less than 32
-
Group 3: Gestational age ≤ 32 and less than 34 weeks (Table 5).
Distribution of fetuses by gestational age was as follows: 28–30 weeks: 28 (27.45%), 30–32 weeks: 37 (36.27%) and 32–34 weeks: 37 (36.27%). As shown in Table 5, pulmonary artery AT and pulmonary artery AT/ET values increased significantly with increasing gestational age.
Discussion
Neonatal Respiratory Distress Syndrome is a common cause of mortality and morbidity in premature infants. The prenatal administration of corticosteroids to improve fetal pulmonary maturity is a well-known treatment used to reduce the risk of neonatal respiratory distress syndrome. The most beneficial effect of prenatal corticosteroid administration is 24 h to 7 days after completing the administration [24].
Despite the pleasing effect of steroids in improving pulmonary maturity, the mechanism of this positive effect is still unclear. Some researchers believe that the effect of corticosteroids in reducing pulmonary vascular resistance is the cause of this positive effect, but there are still different opinions on this subject.
We found significant decreases in the umbilical PI values after betamethasone administration, a finding similar to that of other reports [25, 26]. Elwany et al. demonstrated that antenatal steroids administration rose the fetal uteroplacental blood flow and significantly decreased the umbilical PI [27]. Thuring et al., Gungor et al., and Nozaki et al. obtained similar results [20, 23, 25]. Muldee et al. reviewed the articles about short term impacts of antenatal corticosteroids on fetal circulation, showing that 6 of 17 studies reported a decrease in the umbilical artery PI after steroid administration [28]. Some researchers believe that the reason for this decrease in placental resistance and umbilical PI is the increase in corticotropin-releasing hormone (CRH) after exogenous corticosteroid administration [19]. On the other hand, animal studies have attributed these changes to changes in fetal blood pressure [21, 22]. In general, more studies are needed to determine the cause of these hemodynamic changes in the fetus following corticosteroid administration.
As presented in Tables 2 and 3, among those fetuses exposed to betamethasone we found a statistically significant increase in the middle cerebral artery PI after betamethasone administration. Our results differ from those published by Elwany et al. in which the values of the middle cerebral artery decreased after steroid administration [20]. Besides, Nozaki et al. found no significant changes in the fetal middle cerebral artery velocity waveforms after corticosteroid treatment [21].
As mentioned above, some researchers [21, 22] believe that antenatal corticosteroid administration increase fetal blood pressure. According to this hypothesis, we can justify increase in middle cerebral artery resistance (MCA PI) as an autoregulation mechanism (to stabilize cerebral perfusion). However, there is currently no strong evidence to support this hypothesis. In another study by Piazze et al., a positive correlation between a middle cerebral artery (MCA) PI and lamellar bodies (LBs) count was found in preterm pregnancies [29]. The inclusion criteria in these studies have been different, which may justify these contradictory results. Another possible explanation for the different findings might be variances in treatment strategies and definitions of fetal growth retardation between the studies.
In our study, MCA peak systolic velocity (PSV), pulmonary artery PI, pulmonary artery RI and Pulmonary artery ET did not show any significant influence of betamethasone therapy, but we found significant changes in the pulmonary artery AT and Pulmonary artery AT/ET after betamethasone administration. Similar to the results of our study, Gungor et al. found no significant differences in the pulmonary artery PI and pulmonary artery RI results before and after steroid administration [25].
Lindsley et al. demonstrated that the pulmonary artery PI, pulmonary artery RI, and pulmonary artery ET did not show any significant influence of betamethasone therapy, but pulmonary artery AT significantly decreased after betamethasone administration [26]. Contrary to Lindsley et al. findings, we found a significant increase in the pulmonary artery AT after betamethasone administration. A possible explanation for this contradiction was “characteristics of participants”. In Lindsley et al.’s study, the range of gestational age and the mean of estimated fetal weight in the steroid group were significantly lower.
Unlike the authors mentioned above and us, Ustunyurt et al. described significant decreases in the pulmonary artery PI and pulmonary artery RI at 24 and 48 h after administration of the first dose of steroid [30].
As shown in Table 4, 25 fetuses from the steroid group were born within 7 days of the last Doppler examination, of which 8 had fetal respiratory distress syndrome (RDS). There was a significant difference in gestational age and pulmonary AT values compared to fetuses with RDS and those without it.
As expected, a negative correlation between gestational age and developing of respiratory distress syndrome was found. Pulmonary artery AT was significantly lower in the neonates affected by RDS (P < 0.05). This means that fetuses that develop RDS have higher pulmonary vascular resistance and lower pulmonary blood flow compared with fetuses that do not develop RDS. According to the results of our study, betamethasone reduces pulmonary artery resistance, which manifests as an increase in pulmonary artery AT. In addition, increased pulmonary artery AT was associated with a reduced risk of RDS in infants.
Besides, as represented in Table 5, in the evaluation of the pulmonary artery in our study, the mean pulmonary AT and pulmonary AT/ET values increased significantly with increasing gestational age. However, with increasing gestational age, no significant changes were observed in the pulmonary artery PI, pulmonary artery RI, and pulmonary artery ET.
Schenone et al. found that the pulmonary artery AT/ET and the surfactant/albumin ratio (TDX-FLMװ) were positively correlated [31]. This is similar to the results of our study and the increase in pulmonary artery AT and AT/ET after betamethasone administration. Like our study, Chaoui et al., Moety et al. and Guan et al. demonstrated that the pulmonary artery AT and pulmonary artery AT/ET increased with gestational age. Also, they found that neonates with respiratory distress syndrome had lower AT/ET levels [5, 17, 31].
In our study, only pulmonary artery AT had a negative correlation with RDS in neonates; however, we had some limitations. There were few cases of neonates with RDS (only 8) to fully examine the relationship between pulmonary artery Doppler indices and RDS.
Contrary to our report, Fuke et al. described that the pulmonary artery AT/ET ratio was persistent throughout gestation (20–39 weeks), but they found that the pulmonary artery AT/ET significantly reduced in pulmonary hypoplasia [32]. Some researchers [31, 33, 34] believed that the reduction in pulmonary arterial vascular resistance was reflected by the increase in the pulmonary artery AT and AT/ET; also, they suggested that compromised lung maturation was found to result in decreased vascularization, increased muscularization, and resistance in the peripheral vessels.
The underlying mechanism responsible for the reduction of pulmonary artery resistance after betamethasone treatment is not clear. A possible explanation for this mechanism is nitric oxide-mediated vasodilatation. Glucocorticoids induce the synthesis and secretion of placental CRH, which induces nitric oxide synthase [19, 35].
Human magnetic resonance imaging data also showed that third-trimester fetuses demonstrate remarkable pulmonary blood flow variation from one pregnancy to another, representing all-around from 4 to 30% of the combined cardiac output [36]. This evidence can justify different results of the studies.
Finally and based on our results, we can introduce fetal pulmonary artery Doppler indices as possible noninvasive method for prediction of neonatal RDS. This method had potentiality to be applied clinically, thereby avoid several invasive amniocentesis for evaluation of lung maturation.
Conclusion
Taken together, these data recommend that maternal antenatal betamethasone administration causes significant changes in fetus blood velocity waveforms. Also, fetal main pulmonary artery Doppler indices can be measured throughout gestation and this technique is safe and reproducible for evaluation of pulmonary circulation. Although considering the disparate findings above, additional extensive studies are needed to better examine the relationship between betamethasone administration, blood velocity waveforms, Doppler indices, and neonatal outcomes.
Availability of data and materials
All respectable readers and researchers can request the data by directly contacting the primary author at fahim.kaveh@gmail.com
Abbreviations
- PI:
-
Pulsatility index
- AT:
-
Acceleration time
- RDS:
-
Respiratory distress syndrome
- EFW:
-
Estimated Fetal weight
- UMB PI:
-
Umbilical Pulsatility Index
- (MCA PI:
-
Middle Cerebral Artery Pulsatility Index
- MCA PSV:
-
Middle Cerebral Artery Peak Systolic Velocity
- PA PI:
-
Pulmonary Artery Pulsatility Index
- PA RI:
-
Pulmonary Artery Resistance Index
- PA AT:
-
Pulmonary Artery Acceleration Time
- PA ET:
-
Pulmonary Artery Ejection Time
- MPA:
-
Main pulmonary artery
- MCA:
-
Middle cerebral artery
- AT:
-
Acceleration time
- ET:
-
Ejection time
- LBs:
-
Lamellar bodies
- PSV:
-
Peak systolic velocity
References
Blencowe H, Cousens S, Chou D, Oestergaard M, Say L, Moller AB, Kinney M, Lawn J. Born too soon: the global epidemiology of 15 million preterm births. Reprod Health. 2013;10(Suppl 1):S2.
Kemp MW, Jobe AH, Usuda H, Nathanielsz PW, Li C, Kuo A, Huber HF, Clarke GD, Saito M, Newnham JP, et al. Efficacy and safety of antenatal steroids. Am J Physiol Regul Integr Comp Physiol. 2018;315(4):R825–r839.
Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, Hale EC, Newman NS, Schibler K, Carlo WA, et al. Neonatal outcomes of extremely preterm infants from the NICHD neonatal research network. Pediatrics. 2010;126(3):443–56.
ACOG. Practice Bulletin No. 97: Fetal lung maturity. Obstet Gynecol. 2008;112(3):717–26.
Guan Y, Li S, Luo G, Wang C, Norwitz ER, Fu Q, Tu X, Tian X, Zhu J. The role of doppler waveforms in the fetal main pulmonary artery in the prediction of neonatal respiratory distress syndrome. J Clin Ultrasound. 2015;43(6):375–83.
Vyas J, Kotecha S. Effects of antenatal and postnatal corticosteroids on the preterm lung. Arch Dis Child Fetal Neonatal Ed. 1997;77(2):F147–50.
Akella A, Deshpande SB. Pulmonary surfactants and their role in pathophysiology of lung disorders. Indian J Exp Biol. 2013;51(1):5–22.
Luo G, Norwitz ER. Revisiting amniocentesis for fetal lung maturity after 36 weeks' gestation. Rev Obstet Gynecol. 2008;1(2):61–8.
Spong CY, Mercer BM, D’Alton M, Kilpatrick S, Blackwell S, Saade G. Timing of indicated late-preterm and early-term birth. Obstet Gynecol. 2011;118(2 Pt 1):323–33.
Ventolini G, Neiger R, Hood D, Belcastro C. Update on assessment of fetal lung maturity. J Obstet Gynaecol. 2005;25(6):535–8.
Deter RL, Hadlock FP, Carollo BR. Ultrasonically determined menstrual age as an indicator of fetal lung maturity. J Clin Ultrasound. 1982;10(4):153–7.
Harman CR, Manning FA, Stearns E, Morrison I. The correlation of ultrasonic placental grading and fetal pulmonary maturation in five hundred sixty-three pregnancies. Am J Obstet Gynecol. 1982;143(8):941–3.
Osada H, Iitsuka Y, Masuda K, Sakamoto R, Kaku K, Seki K, Sekiya S. Application of lung volume measurement by three-dimensional ultrasonography for clinical assessment of fetal lung development. J Ultrasound Med. 2002;21(8):841–7.
Tabsh KM. Correlation of ultrasonic epiphyseal centers and the lecithin: sphingomyelin ratio. Obstet Gynecol. 1984;64(1):92–6.
Ekin A, Gezer C, Solmaz U, Taner CE, Ozeren M, Dogan A, Uyar I. Effect of antenatal betamethasone administration on Doppler velocimetry of fetal and uteroplacental vessels: a prospective study. J Perinat Med. 2016;44(2):243–8.
Laudy JA, Wladimiroff JW. The fetal lung. 1: developmental aspects. Ultrasound Obstet Gynecol. 2000;16(3):284–90.
Chaoui R, Taddei F, Rizzo G, Bast C, Lenz F, Bollmann R. Doppler echocardiography of the main stems of the pulmonary arteries in the normal human fetus. Ultrasound Obstet Gynecol. 1998;11(3):173–9.
Kim SM, Park JS, Norwitz ER, Hwang EJ, Kang HS, Park CW, Jun JK. Acceleration time-to-ejection time ratio in fetal pulmonary artery predicts the development of neonatal respiratory distress syndrome: a prospective cohort study. Am J Perinatol. 2013;30(10):805–12.
Korebrits C, Yu DH, Ramirez MM, Marinoni E, Bocking AD, Challis JR. Antenatal glucocorticoid administration increases corticotrophin-releasing hormone in maternal plasma. Br J Obstet Gynaecol. 1998;105(5):556–61.
Nozaki AM, Francisco RP, Fonseca ES, Miyadahira S, Zugaib M. Fetal hemodynamic changes following maternal betamethasone administration in pregnancies with fetal growth restriction and absent end-diastolic flow in the umbilical artery. Acta Obstet Gynecol Scand. 2009;88(3):350–4.
Derks JB, Giussani DA, Jenkins SL, Wentworth RA, Visser GH, Padbury JF, Nathanielsz PW. A comparative study of cardiovascular, endocrine and behavioural effects of betamethasone and dexamethasone administration to fetal sheep. J Physiol. 1997;499(Pt 1):217–26.
Schwab M, Coksaygan T, Nathanielsz PW. Betamethasone effects on ovine uterine and umbilical placental perfusion at the dose used to enhance fetal lung maturation. Am J Obstet Gynecol. 2006;194(2):572–9.
Thuring A, Malcus P, Maršál K. Effect of maternal betamethasone on fetal and uteroplacental blood flow velocity waveforms. Ultrasound Obstet Gynecol. 2011;37(6):668–72.
Costa S, Zecca E, De Luca D, De Carolis MP, Romagnoli C. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007;131(2):154–7.
Güngör ES, İlhan G, Gültekin H, Zebitay AG, Cömert S, Verit FF. Effect of betamethasone on fetal pulmonary and umbilical artery Doppler Velocimetry and relationship with respiratory distress syndrome development. J Ultrasound Med. 2017;36(12):2441–5.
Lindsley W, Hale R, Spear A, Adusumalli J, Singh J, DeStefano K, Haeri S. Does corticosteroid therapy impact fetal pulmonary artery blood flow in women at risk for preterm birth? Med Ultrason. 2015;17(3):280–3.
Elwany E, Omar S, Ahmed A, Heba G, Atef D. Antenatal dexamethasone effect on Doppler blood flow velocity in women at risk for preterm birth: prospective case series. Afr Health Sci. 2018;18(3):596–600.
Mulder EJ, de Heus R, Visser GH. Antenatal corticosteroid therapy: short-term effects on fetal behaviour and haemodynamics. Semin Fetal Neonatal Med. 2009;14(3):151–6.
Piazze JJ, Anceschi MM, Picone G, Cerekja A, La Torre R, Cosmi EV. Association between maternal-fetal Doppler velocimetry and fetal lung maturity. J Perinat Med. 2003;31(6):484–8.
Ustunyurt OB, Ustunyurt E, Korkmazer E, Altug N, Bilge U, Danisman N. The effect of maternal betamethasone administration on Doppler flow velocity parameters of the fetal branch pulmonary artery. Ultrasound Obstet Gynecol. 2014;34(6):489–91.
Moety GA, Gaafar HM, El Rifai NM. Can fetal pulmonary artery Doppler indices predict neonatal respiratory distress syndrome? J Perinatol. 2015;35(12):1015–9.
Fuke S, Kanzaki T, Mu J, Wasada K, Takemura M, Mitsuda N, Murata Y. Antenatal prediction of pulmonary hypoplasia by acceleration time/ejection time ratio of fetal pulmonary arteries by Doppler blood flow velocimetry. Am J Obstet Gynecol. 2003;188(1):228–33.
Barth PJ, Rüschoff J. Morphometric study on pulmonary arterial thickness in pulmonary hypoplasia. Pediatr Pathol. 1992;12(5):653–63.
Schenone MH, Samson JE, Jenkins L, Suhag A, Mari G. Predicting fetal lung maturity using the fetal pulmonary artery Doppler wave acceleration/ejection time ratio. Fetal Diagn Ther. 2014;36(3):208–14.
Clifton VL, Read MA, Leitch IM, Giles WB, Boura AL, Robinson PJ, Smith R. Corticotropin-releasing hormone-induced vasodilatation in the human fetal-placental circulation: involvement of the nitric oxide-cyclic guanosine 3′,5′-monophosphate-mediated pathway. J Clin Endocrinol Metab. 1995;80(10):2888–93.
Prsa M, Sun L, van Amerom J, Yoo SJ, Grosse-Wortmann L, Jaeggi E, Macgowan C, Seed M. Reference ranges of blood flow in the major vessels of the normal human fetal circulation at term by phase-contrast magnetic resonance imaging. Circul Cardiovasc Imaging. 2014;7(4):663–70.
Acknowledgements
The authors would like to thank Shiraz University of Medical Sciences, Shiraz, Iran and also Center for Development of Clinical Research of Nemazee Hospital and Dr. Nasrin Shokrpour for editorial assistance.
Classification
Diagnostic study.
Funding
The study was funded by Shiraz University of Medical Sciences (Grant #98–01–85-21732).
Author information
Authors and Affiliations
Contributions
H V, N A, F K aided in the conceptualization, design, and critical revision of the final manuscript.AF, F K, N A, M K, Sh R and HV aided in design, preparation of manuscript and critical revision of the final manuscript. M Z, Sh R and Kh B aided in data analysis and critical revision of the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of Shiraz University of Medical Sciences. All patients gave their written and informed. (ethics code: IR.SUMS.REC.1399.351) consent to enter the study.
Consent for publication
Not Applicable.
Declaration of Helsinki: All methods were performed in accordance with the relevant guidelines and regulations.
Competing interests
There is no conflict of interest to be declared regarding the manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Vafaei, H., Kaveh Baghbahadorani, F., Asadi, N. et al. The impact of betamethasone on fetal pulmonary, umbilical and middle cerebral artery Doppler velocimetry and its relationship with neonatal respiratory distress syndrome. BMC Pregnancy Childbirth 21, 188 (2021). https://doi.org/10.1186/s12884-021-03655-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-021-03655-2