
Abstract
Background
Preeclampsia (PE) is a serious complication of pregnancy and one of the main causes of maternal and neonatal mortality and morbidity in the world. Finding a biomarker with high sensitivity and specificity could lead to prediction and early diagnosis of the disease and reduces its complications. In this study, we evaluated diagnostic accuracy of Soluble fms-like tyrosine kinase-1 (sFlt-1) to Placental growth factor (PlGF) ratio for diagnosis of PE.
Methods
The cases included 23 mild, 15 severe preeclamptic patients, and 20 normal term pregnant women as control referred to GYN ward of the Persian Gulf Hospital in Bandar Abbas from 2014 to 2016. Levels of sFlt-1 and PlGF were measured. Receiver Operating Characteristic (ROC) curve analysis was applied to calculate diagnostic accuracy of sFlt-1/PlGF ratio.
Results
The mean Level of sFlt-1/PlGF in PE patients (91.33 ng/ml) was significantly higher than control women (17.62) (P<0.001). ROC curve analysis showed sFlt-1/PlGF ratio diagnostic accuracy in preeclamptic patients with Area Under Curve (AUC) of 0.90, the best cut-off value of 24.96, sensitivity and specificity of 84.2 and 85.0%, respectively.
Conclusions
Our data showed sFlt-1/PlGF ratio has higher accuracy for differentiating PE patients from non-PEs in comparison with its power for differentiating severe or early onset forms of the disease.
Similar content being viewed by others


Background
Preeclampsia (PE) is diagnosed after 20 weeks of gestation [1]. This multisystem disorder affects 2–7% of pregnant women [2]. PE has serious complications including liver and kidney dysfunction, seizure and even death. PE is one of the major causes of maternal death, neonatal mortality and premature deliveries [3, 4]. As long as the placenta is present, PE is likely to happen and the recovery process starts post-delivery following the removal of placenta [5]. PE is divided into early-onset and late-onset according to the time of onset. Early-onset PE develops before 34 weeks of gestation, while late-onset PE develops at or after 34 weeks of gestation. The etiology of early-onset form of PE is related to incomplete trophoblast invasion and failure of normal spiral artery remodeling. Late-onset PE is associated with increased maternal vascular susceptibility to the normal inflammatory state of pregnancy or atherosis of a placenta grown initially normal [6]. Diagnostic criteria for PE include hypertension after 20 weeks of gestation and the coexistence of one or more of the following new-onset conditions: proteinuria, maternal organ dysfunction, and uteroplacental dysfunction [7]. Definite pathogenesis of PE is not completely clear, but the imbalance between angiogenic factors like vascular endothelial growth factor or placental growth factor (PlGF) and anti-angiogenic factors like soluble fms-like tyrosine kinase 1 (sFlt-1) are known to be related to the disease pathogenesis [8, 9].
In normal pregnancies, the level of sFLT-1 starts to rise after 30–32 weeks of gestation and PlGF level starts to decrease after 30 weeks of gestation. Actually cellular stress in the syncytiotrophoblast, which occurs during the last 8–10 weeks of a pregnancy leads to biochemical changes in levels of sFlt-1 and PlGF in normal pregnancies [10]. Circulating levels of sFlt-1 and PlGF alter in PE patients. This alteration begins before the disease onset and stays during the course of the disease [11]. In women with PE sFlt-1 rises approximately 5 weeks prior to disease onset [12] while the level of PlGF decreases before the rising of sFlt-1 [12, 13]. Hence, to improve the quality of PE diagnosis, some studies suggest sFlt1/PlGF Ratio as a better marker compared to measuring sFlt1 or PlGF separately for diagnosis of PE [11]. The aim of this study was to evaluate the diagnostic accuracy of sFlt-1: PlGF ratio, and the simplified best cut-off values for sFlt-1:PlGF ratio in assessing the diagnosis of PE.
Methods
This research was a case-control study. Subjects were chosen from pregnant women referred to the Persian Gulf hospital located in Bandar Abbas in the south of Iran from 2014 to 2016. There were 38 PE patients and 20 normal term pregnant women as controls in the study. Informed written consent was obtained from all participants according to the protocols approved by the Ethical Committee of Hormozgan University of Medical Sciences (No. 1-HEC-93-7-8). Patients were sub-grouped as mild (23 women) and sever (15 women). Patients were classified into early-onset (9 women) and late-onset (29 women). Patients with diabetes, renal disease, collagen vascular diseases, and chronic hypertension were excluded from the study. PE was defined as gestational hypertension (systolic pressure > 140 mmHg or diastolic blood pressure > 90 mmHg on two or more occasions after gestational week 20) with proteinuria (> 0.3 g/day). The disease was defined severe if, more than one of the following criteria were met: (i) severe gestational hypertension; that is, systolic pressure > 160 mmHg or diastolic blood pressure > 110 mmHg on two or more occasions after gestational week 20, (ii) severe proteinuria; that is, protein ≥5 g in a 24-h urine specimen, (iii) oliguria, (iv) cerebral or visual disturbances, (v) pulmonary edema or cyanosis, (vi) epigastric or right upper quadrant pain, (vii) impaired liver function, (viii) thrombocytopenia or (ix) fetal growth restriction [1]. PE was defined early-onset (< 34 weeks of gestation) and late-onset (≥34 weeks) [14]. The whole blood samples were obtained from participants and centrifuged at 3000 g for 20 min and separated serum samples stored at − 80 °C for ELISA. Levels ofsFlt-1 and PlGF were measured using (ELISA, R&D System, Human VEGF R1/Flt-1Immunoassay, Catalog Number DVR100B and Human PlGF Immunoassay, Catalog NumberDPG00) according to the procedure provided by the manufacturer.
Statistical analysis
One-way ANOVA/Kruskal-Wallis test with Bonferroni correction was applied for comparison of data between multiple groups and Mann-Whitney test / unpaired t-test was used for comparison between two groups based on the normality of data. Data were shown as number (%), mean (±SD). The Receiver Operating Characteristics (ROC) curve analysis was applied to calculate the Area Under the Curve (AUC) and to find the best cut-off point, Positive Predictive Values (PPVs), Negative Predictive Values (NPVs), diagnostic accuracy, sensitivity, specificity and likelihood ratios.
Results
We did not observe any significant difference in maternal age (P = 0.546) and BMI before pregnancy (P = 0.355) between case and control groups. This showed that case and control groups were matched. Clinical characteristics are displayed in Table 1. The number of nulliparous women in both groups was almost similar (40% in the control group and 44.7% in the case group). Recurrent PE was observed in 15.8% of women in the case group.
Mean Level of sFlt-1/PlGF was 91.33 ng/ml in PE patients and 17.62 in controls which were increased significantly (P<0.001). In comparison between mild, severe and controls the mean level of sFlt-1/PlGF was 130.97 in severe PE patients which was significantly increased compared to controls (P<0.001). Also, it was 65.48 in mild PE patients which was increased significantly compared to controls (P<0.001). Although the level of sFlt-1/PlGF was higher in severe PE patients compared to mild women, there was no significant difference between these two groups (P = 0.389). Also in the comparison between early-onset, late-onset and controls the mean level of sFlt-1/PlGF was 153.44 in the early-onset PE patients and 72.06 in late-onset PE patients. There was a significant difference between early-onset group and controls (P<0.001), and also between late-onset PE patients and controls (P<0.001), but there was no significant difference between early and late onset PE patients (0.503) (Fig. 1).

a Comparison of sFlt-1/PlGFratio between PE patients and controls; b mild and sever PE patients with controls; c early and late onset PE patients with controls, which shows significant increase in all PE groups in comparison with the normal women. The 10th and 90th centiles are represented by lower and upper bars. The horizontal line in the box shows median
ROC-curve analysis
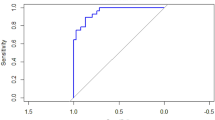
The ROC curve analysis was applied to differentiate PE patients from normal controls and also for differentiating severe and early-onset forms of PE using sFlt-1/PlGF ratio. The results for differentiation of PE patients from normal pregnancies showed an AUC of 0.90 (95% CI =0.83–0.98). The best cut-off value was 24.96 ng/ml with sensitivity of 84.2% (95% CI =68.7–94) and specificity 85% (95% CI =62.1–96.8). Table 2 and Fig. 2 provide results related to LR, PPV, and NPV. Moreover, ROC curve analysis was also applied to differentiate early onset PE from controls using sFlt-1/PlGF ratio (Table 2 and Fig. 2).

ROC curve analysis of sFlt-1/PlGF ratio in preeclampsia, which shows the ability of maternal serum sFlt-1/PlGF ratio to (a) differentiate preeclampsia from normal pregnancies; (b) severe PE patients; (c) early-onset PE patients. sFlt-1 has the highest AUC for the diagnosis of PE patients from normal pregnant women
Discussion
Anti-angiogenic factors like sFlt-1 are released by the placenta in the circulation of women affected to PE and are known as the cause of endothelial dysfunction observed in this disease. This anti-angiogenic protein inhibits the activity of VEGF and PlGF and results in hypertension and proteinuria as main symptoms of PE [11]. Recombinant sFlt-1 could block development of endothelial tubes and inhibit vasodilatory effects of VEGF and PlGF in vasculature [15]. In women with PE, the levels of sFlt-1 rise 5 weeks prior to clinical presentations, and stay elevated till the onset of the disease [12, 16] while the serum PlGF decreases before clinical presentation [12]. So these two markers could be used for prediction and diagnosis of PE, but recent studies showed that sFlt1/PlGF ratio is a better marker with more accuracy for screening PE rather than sFlt-1 or PlGF alone [17].
According to our knowledge, this is the first study which investigates the diagnostic accuracy of sFlt1/PlGF ratio in Iranian women with PE. Results of our study showed sFlt1/PlGF ratio has the highest accuracy for differentiating PE patients from normal pregnant women. In our study the best cut-off for the highest sensitivity (84.2%) and specificity (85%) was 24.96 ng/ml with LR+ 5.61, LR− 0.186 for differentiating PE from healthy women. So because of high sensitivity, specificity, positive and negative LR of sFlt1/PlGF ratio, it could help in diagnosing high-risk women for developing PE and decreasing costs related to serious maternal and neonatal complications by precise observation and early medical interventions. Also, we evaluated the accuracy of sFlt1/PlGF ratio in diagnosing severe and early-onset PE which more likely lead to preterm delivery.
Based on our ROC curve analysis for sFlt1/PlGF ratio, the best cut-off for diagnosing severe PE patients is 40.9 ng/ml with 80% sensitivity and 72.09% specificity, and the best cut-off for diagnosing early-onset PE is 39.7 ng/ml with sensitivity of 88.89% and specificity of 65.31%. In this study, sFlt1/PlGF ratio showed the highest sensitivity and specificity in differentiating PE patients from normal pregnant women. Our results are in agreement with findings of other studies which reported association of sFlt1/PlGF ratio with clinical diagnosis of PE [4, 8, 12, 18, 19].
Lim et al. reported higher levels of sFlt-1/PlGF in women with preeclampsia compared to normal controls. Like our study, they reported sFlt-1/PlGF ratio was not significantly different between mild and severe PE patients. Also, the cut-off value of sFlt-1/PlGF was 20.5 with AUC of 0.85 for the prediction of preeclampsia [8]. DE VIVO et al. applied ROC curve analysis for the second-trimester marker values in PE patients. They showed the best diagnostic profile for sFlt-1/PlGF ratio with AUC of 0.92 and the best cut-off of 38.47. They found this marker with the best prediction power for pre-eclampsia with a specificity, a sensitivity, a diagnostic accuracy, a PPV and a NPV of 88.5%, a positive likelihood ratio of 7.7 and a negative likelihood ratio of 0.13 [20]. KUSANOVIC et al. reported the best predictive performance for sFlt1/PlGF ratio with a sensitivity of 100%, specificity of 98–99%, and likelihood ratios for a positive test of 57.6, 55.6 and 89.6, respectively, for predicting early-onset preeclampsia [21].
Rana et. al. reported sFlt1/PlGF ratio of more than 85 had an association with harmful pregnancy complications and termination of pregnancy in 2 weeks. Moreover, they reported sFlt1/PlGF ratio along with systolic blood pressure (SBP) and proteinuria were a better predictive tool rather than SBP, proteinuria, and uric acid levels [3]. Ohkuchi et al. showed the best diagnostic power of sFlt1/PlGF ratio for both early and late onset PE. They reported a cut-off value of 45 with 97 and 95% sensitivity and specificity respectively for diagnosis of all preeclampsia and for diagnosis of early-onset PE (100 and 95%) [22].
Meanwhile, sFlt1/PlGF ratio could be a useful marker for the differential diagnosis of PE [3]. Hypertension and proteinuria are hallmark symptoms of both preeclampsia and chronic kidney disease (CKD). It is important to differentiate PE from CKD and manage PE efficiently. Rolfo et al. found that serum levels of sFlt1/PlGF ratio significantly increase in PE compared with CKD and controls [23]. Our results support previous studies about the association of high sFlt-1/PlGF ratio with the diagnosis of PE and also severe and early-onset forms of the disease. This marker has the highest sensitivity and specificity for distinguishing PE from normal pregnancies in comparison to severe and early-onset forms of the disease. Using angiogenic biomarkers might lead to screening and faster diagnosis of PE patients and also to preventing them from serious complications. One of the limitations of this study was the sample size. More studies in larger populations and among other ethnicities are required to determine the cost-effectiveness of sFlt-1/PlGF ratio as a biomarker for PE diagnosis. Another limitation was that it was not possible to carry out sampling prior to the patients’ diagnosis and samples were taken after PE diagnosis.
Conclusions
Our data showed that sFlt-1/PlGF ratio has the highest accuracy for the diagnosis of PE patients from normal pregnant women in comparison to its power for the diagnosis of severe or early-onset forms of the disease.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PE:
-
Preeclampsia
- PlGF:
-
Placental growth factor
- ROC curve:
-
Receiver operating characteristic curve
- sFlt-1:
-
Soluble fms-like tyrosine kinase-1
References
Practice ACO. Practice bulletin# 33: diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99(1):159–67.
Louwen F, Muschol-Steinmetz C, Reinhard J, Reitter A, Yuan J. A lesson for cancer research: placental microarray gene analysis in preeclampsia. Oncotarget. 2012;3(8):759–73.
Rana S, Powe CE, Salahuddin S, Verlohren S, Perschel FH, Levine RJ, et al. Angiogenic factors and the risk of adverse outcomes in women with suspected preeclampsia. Circulation. 2012;125(7):911–9.
Verlohren S, Galindo A, Schlembach D, Zeisler H, Herraiz I, Moertl MG, et al. An automated method for the determination of the sFlt-1/PIGF ratio in the assessment of preeclampsia. Am J Obstet Gynecol. 2010;202(2):161. e1–e11.
Sitras V, Paulssen R, Grønaas H, Leirvik J, Hanssen T, Vårtun Å, et al. Differential placental gene expression in severe preeclampsia. Placenta. 2009;30(5):424–33.
Park HJ, Kim SH, Jung YW, Shim SS, Kim JY, Cho YK, Farina A, Zanello M, Lee KJ, Cha DH. Screening models using multiple markers for early detection of late-onset preeclampsia in low-risk pregnancy. BMC Pregnancy Childbirth. 2014;14(1):35.
Tranquilli A, Dekker G, Magee L, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: a revised statement from the ISSHP. Pregnancy Hypertens. 2014;4:97–104.
Lim JH, Kim SY, Park SY, Yang JH, Kim MY, Ryu HM. Effective prediction of preeclampsia by a combined ratio of angiogenesis-related factors. Obstet Gynecol. 2008;111(6):1403–9.
Stepan H, Unversucht A, Wessel N, Faber R. Predictive value of maternal angiogenic factors in second trimester pregnancies with abnormal uterine perfusion. Hypertension. 2007;49(4):818–24.
Huhn EA, Kreienbuehl A, Hoffmann I, Schoetzau A, Lange S, de Tejada BM, Hund M, Hoesli I, Lapaire O. Diagnostic accuracy of different soluble fms-like tyrosine kinase 1 and placental growth factor cut-off values in the assessment of preterm and term preeclampsia: a gestational age matched case-control study. Front Med. 2018;5:325.
Powe CE, Levine RJ, Karumanchi SA. Preeclampsia, a disease of the maternal endothelium the role of antiangiogenic factors and implications for later cardiovascular disease. Circulation. 2011;123(24):2856–69.
Levine RJ, Maynard SE, Qian C, Lim K-H, England LJ, Yu KF, et al. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004;350(7):672–83.
Thadhani R, Mutter WP, Wolf M, Levine RJ, Taylor RN, Sukhatme VP, et al. First trimester placental growth factor and soluble fms-like tyrosine kinase 1 and risk for preeclampsia. J Clin Endocrinol Metab. 2004;89(2):770–5.
Schaarschmidt W, Rana S, Stepan H. The course of angiogenic factors in early-vs. late-onset preeclampsia and HELLP syndrome. J Perinat Med. 2013;41(5):511–6.
Kendall RL, Thomas KA. Inhibition of vascular endothelial cell growth factor activity by an endogenously encoded soluble receptor. Proc Natl Acad Sci. 1993;90(22):10705–9.
Hertig A, Berkane N, Lefevre G, Toumi K, Marti H-P, Capeau J, et al. Maternal serum sFlt1 concentration is an early and reliable predictive marker of preeclampsia. Clin Chem. 2004;50(9):1702–3.
Andraweera P, Dekker G, Roberts C. The vascular endothelial growth factor family in adverse pregnancy outcomes. Hum Reprod Update. 2012;18(4):436–57.
Romero R, Nien JK, Espinoza J, Todem D, Fu W, Chung H, et al. A longitudinal study of angiogenic (placental growth factor) and anti-angiogenic (soluble endoglin and soluble vascular endothelial growth factor receptor-1) factors in normal pregnancy and patients destined to develop preeclampsia and deliver a small for gestational age neonate. J Matern Fetal Neonatal Med. 2008;21(1):9–23.
Sunderji S, Gaziano E, Wothe D, Rogers LC, Sibai B, Karumanchi SA, et al. Automated assays for sVEGF R1 and PlGF as an aid in the diagnosis of preterm preeclampsia: a prospective clinical study. Am J Obstet Gynecol. 2010;202(1):40. e1–7.
De Vivo A, Baviera G, Giordano D, Todarello G, Corrado F, D'anna R. Endoglin, PlGF and sFlt-1 as markers for predicting pre-eclampsia. Acta Obstet Gynecol Scand. 2009;87:837–42.
Kusanovic JP, Romero R, Chaiworapongsa T, Erez O, Mittal P, Vaisbuch E, et al. A prospective cohort study of the value of maternal plasma concentrations of angiogenic and anti-angiogenic factors in early pregnancy and midtrimester in the identification of patients destined to develop preeclampsia. J Matern Fetal Neonatal Med. 2009;22(11):1021–38.
Ohkuchi A, Hirashima C, Suzuki H, Takahashi K, Yoshida M, Matsubara S, et al. Evaluation of a new and automated electrochemiluminescence immunoassay for plasma sFlt-1 and PlGF levels in women with preeclampsia. Hypertens Res. 2010;33(5):422–7.
Rolfo A, Attini R, Nuzzo AM, Piazzese A, Parisi S, Ferraresi M, et al. Chronic kidney disease may be differentially diagnosed from preeclampsia by serum biomarkers. Kidney Int. 2013;83(1):177–81.
Acknowledgements
This work was financially supported by Research Vice-Chancellor of Hormozgan University.
For Medical Science (HUMS) gratefully acknowledged.
Funding
The study was funded by a grant from Hormozgan University of Medical Sciences (No. 1-HEC-93-7-8) which allowed all steps of the study to be conducted. These steps were study design, data gathering, analysis and interpretation of data, and the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
PN and MR contributed to the study design, initial drafting, and data extraction, developed the search strategy and revised the manuscript. NR, FP and FM critically revised the manuscript. SH and MA provided important intellectual input. All authors approved the final version of the manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed written consent was obtained from all participants under the protocols approved by.
the Ethical Committee of Hormozgan University of Medical Sciences, Iran. (No. 1-HEC-93-7-8).
Consent for Publication.
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Nikuei, P., Rajaei, M., Roozbeh, N. et al. Diagnostic accuracy of sFlt1/PlGF ratio as a marker for preeclampsia. BMC Pregnancy Childbirth 20, 80 (2020). https://doi.org/10.1186/s12884-020-2744-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-020-2744-2