
Abstract
Background
Our study aims to describe how obstetricians manage pregnant women infected with chronic hepatitis B in a region with a large high-risk population.
Methods
We performed a cross-sectional study among practicing obstetricians in Santa Clara County, California. All obstetricians practicing in Santa Clara County were invited to participate in the study. Obstetricians were recruited in person or by mail to complete a voluntary, multiple choice survey on hepatitis B (HBV). Survey questions assessed basic HBV knowledge and obstetricians’ self-reported clinical practices of the management of HBV-infected pregnant women. Pooled descriptive analyses were calculated for the cohort, as well as, correlation coefficients to evaluate the association between reported clinical practices and hepatitis B knowledge.
Results
Among 138 obstetricians who completed the survey, 94% reported routinely testing pregnant women for hepatitis B surface antigen (HBsAg) with each pregnancy. Only 60.9% routinely advised HBsAg-positive patients to seek specialist evaluation for antiviral treatment and monitoring and fewer than half (48.6%) routinely provided them with HBV information. While most respondents recognized the potential complications of chronic HBV (94.2%), only 21% were aware that chronic HBV carries a 25% risk of liver related death when left unmonitored and untreated, and only 25% were aware of the high prevalence of chronic HBV in the foreign-born Asian, Native Hawaiian and Pacific Islander population. Obstetricians aware of the high risk of perinatal HBV transmission were more likely to test pregnant women for HBV DNA or hepatitis B e-antigen in HBV-infected women (r = 0.18, p = 0.033). Obstetricians who demonstrated knowledge of the long-term consequences of untreated HBV infection were no more likely to refer HBV-infected women to specialists for care (r = 0.02, p = 0.831).
Conclusion
Our study identified clear gaps in the practice patterns of obstetricians that can be readily addressed to enhance the care they provide to HBV-infected pregnant women.
Similar content being viewed by others


Background
The elimination of mother-to-child transmission of hepatitis B virus (HBV) infection is a pillar of the United States (U.S.) national prevention strategy to combat viral hepatitis [1]. Infected newborns are particularly vulnerable to developing chronic HBV infection and carry a 25% risk of premature death from liver cancer and liver cirrhosis later in life [2, 3]. Risk of perinatal chronic HBV infection is as high as 90% if the mother is hepatitis B surface antigen (HBsAg) and hepatitis B e antigen (HBeAg) positive [4, 5]. A 2016 National Academy of Medicine report concluded that ending perinatal transmission of hepatitis B is highly feasible [6]. Administration of hepatitis immune globulin and HBV vaccination within 12 h of birth and completion of the HBV vaccine series is 85–95% effective in preventing chronic HBV in newborns of HBsAg-positive mothers [2]. Prophylactic antiviral therapy in the third trimester has also been demonstrated to further decrease perinatal chronic HBV transmission in highly viremic, HBeAg positive women [7].
Routine HBV screening of pregnant women has long been recommended by both the Advisory Committee on Immunization Practices (ACIP) and U.S. Preventive Services Task Force [8, 9]. The ACIP further recommends: antenatal reporting of HBsAg-positive pregnant women to public health departments, providing a laboratory copy of the HBsAg test result to the planned delivery hospital to prevent transcription errors, post-vaccination HBV testing (PVST) for infants born to infected mothers, and appropriate counseling and referral of HBsAg-positive pregnant women for medical management [2].
Despite these recommendations, only half of the estimated 25,000 HBsAg-positive women that give birth each year are referred for enrollment in the perinatal HBV prevention program for case management [10]. The percentage of infants born to HBsAg-positive women that received PVST has remained low and an estimated 800–1000 infants still become chronically infected each year [10].
In the U.S., 86% of women receive their prenatal care from obstetricians, providing the chance to prevent HBV transmission and optimize the health of the infected mothers [11]. In an effort to better understand the gaps and opportunities for improvement, we surveyed obstetricians’ HBV knowledge and preventative practices.
Methods
Design
The study conducted was a cross-sectional survey of HBV knowledge and existing practices among practicing obstetricians. The study protocol was approved by Stanford University Institutional Review Board and Institutional Review Boards of all participating hospitals. All study participants provided informed consent.
Sample selection
Participants were recruited via convenience sampling from the population of obstetricians (n = 311) practicing at eight major birthing hospitals in Santa Clara County, California between June 2008 and March 2010. Surveys were mailed to obstetricians of all eight hospitals up to three times to optimize recruitment and minimize sampling bias. Participants were also recruited in-person at hospital events.
Setting
Santa Clara County, California was selected because it has the second highest annual number of infants born to HBsAg-positive women in the state [12]. By CDC estimates, about 80% of HBsAg-positive women who give birth each year are foreign born and over 50% are Asians, Native Hawaiian and other Pacific islanders (AANHPI) [13]. Santa Clara County has both a large foreign born (39.5%) and AANHPI population (35.8%) [14].
Surveys
The multiple-choice survey assessed providers’ demographics, general HBV knowledge (i.e. transmission, prevalence, diagnostic testing, prevention, and treatment options), as well as, self-reported practice behavior. We have previously published extensively on our survey instrument [15,16,17,18,19,20,21,22].
Statistical analysis
The data collected were de-identified and pooled for analysis. Pooled descriptive analyses were calculated for the cohort and individual subjects were assigned knowledge scores based on the total number of correct responses for knowledge questions. We also calculated the Spearman correlation coefficient to evaluate the association between reported clinical practices and HBV knowledge. Statistical significance was defined as a two-sided p-value < 0.05. All statistical analyses were performed using SPSS version 13.
Results
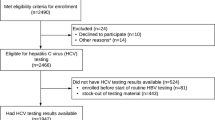
Of 278 obstetricians invited to participate in the study, the response rate was 64.7% (n = 180). Among the respondents, 76.7% (n = 138) were included in the study. Twenty-one respondents declined to participate in the study. An additional 21 respondents who completed less than 50% of the survey were excluded from analysis.
Demographics
The majority of participants were female (68.9%), averaged at least a decade of experience in their obstetric practice (range = 1–41 years, mean = 15 years), and predominantly non-Hispanic White (44.9%) or Asian (41.3%) (Table 1).
Survey responses
Most obstetricians (88.4%) reported they had cared for a pregnant patient who tested positive for HBsAg. The majority (94.2%) routinely tested all pregnant women for HBsAg with each pregnancy and almost 90% routinely informed HBsAg- positive pregnant women about the importance of immunoprophylaxis, including HBV immune globulin (89.9%) and the birth dose of the HBV vaccine (87.7%) within 12 h of birth. Less than half of the respondents (48.6%) routinely informed the HBsAg-positive women that their infants need to complete the three-dose HBV vaccine series, and only 20.3% routinely informed them about the need for PVST for infants. Only 76.1% informed HBsAg-positive women that their household and sexual contacts should be tested for HBV. Only 48.6% of obstetricians surveyed routinely provided educational information about HBV to their HBsAg-positive patients (Table 2).
Nearly one-fourth of the respondents (23.9%) did not know that California state ordinance requires physicians to report all positive HBsAg test results to the county health department, and only 64.5% routinely included a laboratory copy of the pregnant patient’s HBsAg test result in the medical record sent to the birth hospital prior to the expected delivery date. 63.8% of the respondents routinely order HBV DNA or HBeAg tests in HBsAg-positive pregnant women to further assess their infectivity risks, but only 77.5% monitor their liver enzymes during pregnancy. Only 60.9% routinely advised their HBsAg-positive patients to consult with a specialist for evaluation for antiviral therapy and management (Table 2).
The mean number of correct responses for the HBV knowledge questions was 3.7 out of 5 (Table 3). Most obstetricians recognized the complications of HBV infection (94.2%), but more than one fourth (26.1%) did not know that most infected individuals are asymptomatic. Just 22.5% of obstetricians correctly identified the high prevalence of chronic HBV infection in the foreign-born AANHPI population. One-third of obstetricians correctly responded that an infant has up to a 90% chance of developing chronic infection if infected at birth. Only one-fourth (25.4%) of obstetricians recognized the high mortality risk associated with chronic HBV infection.
Table 4 is a shows the correlation between the obstetricians’ HBV knowledge and clinical practice. The only positive correlation we found between knowledge and practice was obstetricians who knew the high risk of chronic infection when infected at birth were more likely to test their infected patients for HBV DNA and/or HBeAg in HBsAg-positive pregnant women. There was no correlation between knowing the sequelae of chronic HBV infection (Q14, Q18) and referral of HBsAg-positive pregnant women to specialists for further management.
Discussion
Our study found that while self-reported compliance with HBsAg testing of pregnant women was high among obstetricians surveyed, education of women who tested positive and subsequent referral to specialist care was low. Each year obstetricians provide care to an estimated 25,000 HBsAg-positive pregnant women in the U.S. [10]. Many asymptomatic women may not have previously known about their infection, HBV transmission routes, or the risk of liver cancer and cirrhosis [20, 23, 24]. Obstetricians can play an important role in protecting the entire family from HBV through education, ensuring that household or sexual contacts get tested and vaccinated, and by referring women to liver specialists.
Although most of the obstetricians surveyed reported having cared for HBsAg positive pregnant patient, less than half (46%) routinely provided their infected patients with HBV informational materials. Though alarming, this could readily be remedied. Targeted information and pamphlets in multiple languages for pregnant women with HBV are available from the CDC and the non-profit, HepBmoms.org websites [25, 26]. HepBmoms.org was founded as part of this CDC funded study to provide multilingual informational resources for infected mothers, as well as, for obstetrical clinics and delivery hospitals.
In our study, we found only 64.5% of obstetricians reported routinely provide the birth hospital a lab copy of the HBsAg test result, and 23.9% did not know they were required by law to report positive HBsAg tests. Obstetricians are the vital communication link between infected mothers and the healthcare system in preventing mother-to-child transmission. By providing birth hospitals with a lab copy of the HBV test result, obstetricians can reduce errors from transcription and ensure infected mothers are identified at the time of admission for delivery so their infants receive timely post-delivery immunoprophylaxis [2]. Among the 50 states, 32 states (including California) requires healthcare providers to report pregnant women HBsAg positive tests [27]. By promptly reporting antenatal tests positive for HBsAg to the county health department, obstetricians would enable the perinatal HBV prevention program coordinators to enroll these patients in case management.
Approximately three-quarter of obstetricians in this study reported routinely monitoring liver enzymes. Monitoring the liver enzymes of HBsAg positive pregnant women is important because HBV flare or reactivation is common during pregnancy and the post-partum period and can even lead to life threatening liver failure [28,29,30,31]. In addition, just over half of obstetricians surveyed reported referring infected mothers to their internists or liver specialists. Referral to liver specialists would help to identify women eligible for antiviral therapy to treat hepatitis flares or reduce the risk of perinatal transmission [7].
To our knowledge, this is the first study in the U.S. to assess obstetricians’ knowledge and practices regarding HBV-infected pregnant women. The gaps identified in this study is not unique to obstetricians, and is suggestive of a larger systematic problem in the way healthcare professionals are taught or trained about chronic HBV prevalence, risks and management. Surveys of family physicians in New Jersey [32], primary care providers in San Francisco, and physicians in training in Santa Clara County [33, 34] also showed inadequate chronic HBV knowledge and clinical management.
In another study of 518 perinatal nurses in eight birthing hospitals in Santa Clara County, we found less than a quarter recognized the high risk of developing chronic infection if infected at birth and the high risk of death from uncontrolled chronic HBV infection [35]. Although 80% reported having cared for HBsAg-positive pregnant women, only half reported educating these patients. After attending an in-service HBV seminar, all the nurses indicated they would provide their patients with educational information in the future. Lack of self-efficacy due to insufficient HBV training was attributed by obstetricians and perinatal nurses interviewed as a major barrier to counseling their patients about HBV [35].
There are some limitations of the study that should be considered. First, clinical practices were self-reported and data may have been inaccurate or biased due to over-reporting of compliance with recommended practices. In order to minimize this bias, future studies to evaluate clinical practice can be designed to include both self-reporting and concurrent review of medical records to evaluate for consistency in practice. Second, we were unable to compare respondents versus non-respondents to assess for non-response bias because we only had names and mailing addresses of non-respondents. Third, the survey was limited to multiple-choice responses which may carry inherent disadvantages (i.e. can suggest answers, does not comprehension of question, answer choices limit respondents’ response). As with all surveys, generalizability is limited and conclusions are based on associations of responses. Respondents were assumed to have answered truthfully and answers reflect actual practice. However, given that we surveyed obstetricians in an area with one of the highest rates of HBV in the U.S., it is unlikely that hepatitis-B-related knowledge or clinical practice is substantially better elsewhere in the country.
Conclusions
In summary, our survey of practicing obstetricians identified gaps in patient education, case reporting, referral for HBV treatment, and disease monitoring among HBV infected pregnant women. These gaps can have lifelong consequence for mother and child. Women identified as HBsAg-positive need to be evaluated for hepatitis flare during pregnancy and informed of the future risk of HBV related complications. In order to prevent transmission to their infants, infected women need counseling regarding timely immunoprophylaxis after delivery and PVST. Adherence to the 2015 CDC and American College of Obstetricians and Gynecologists endorsed algorithm for prenatal ALT, HBeAg and HBV DNA testing of HBsAg-positive women and specialist referral, along with, providing culturally and linguistically appropriate education are important steps towards optimizing the care of this patient population [36].
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AANHPI:
-
Asian Americans, Native Hawaiian and Pacific islanders
- ACIP:
-
Advisory Committee on Immunization Practices
- CDC:
-
Centers for Disease Control and Prevention
- HBeAg:
-
hepatitis B e-antigen
- HBsAg:
-
Hepatitis B surface antigen
- HBV:
-
Hepatitis B
- PSVT:
-
Post vaccination hepatitis B testing
References
Department of Health and Human Services. Action Plan for the Prevention, Care, & Treatment of Viral Hepatitis. 2014. https://www.hhs.gov/sites/default/files/viral-hepatitis-action-plan.pdf. Accessed 15 Feb 2018.
Mast EE, Margolis HS, Fiore AE, Brink EW, Goldstein ST, Wang SA, Moyer LA, Bell BP, Alter MJ. Advisory Committee on Immunization Practices (ACIP). A Comprehensive Immunization Strategy to Eliminate Transmission of Hepatitis B Virus Infection in the United States. Recommendations of the Advisory Committee on Immunization Practices (ACIP) Part 1: Immunization of Infants, Children, and Adolescents. MMWR. 2005;54(RR 16):1–23.
McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis. 1985;151:599–603.
Beasley RP, Trepo C, Stevens CE, Szmuness W. The e antigen and vertical transmission of hepatitis B surface antigen. Am J Epidemiol. 1977;105:94–8.
Okada K, Kamiyama I, Inomata M, Imai M, Miyakawa Y. E antigen and anti-e in the serum of asymptomatic carrier mothers as indicators of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med. 1976;294:746–9.
National Academy of Sciences, Engineering and Medicine. Eliminating the public health problem of hepatitis B and C in the United States: Phase one report. Washington, DC: The National Academies Press; 2016.
Pan CQ, Duan Z, Dai E, Zhang S, Han G, Wang Y, Zhang H, Zou H, Zhu B, Zhao W, Jiang H. China study Group for the Mother-to-Child Transmission of Hepatitis B. Tenofovir to prevent hepatitis B transmission in mothers with high viral load. N Engl J Med. 2016;374(24):2324–34.
CDC. Recommendation of the Immunization Practices Advisory Committee. Prevention of perinatal transmission of hepatitis B virus: prenatal screening of all pregnant women for hepatitis B surface antigen. MMWR. 1988;37:341–6,351.
US Preventive Services Task Force. Hepatitis B in pregnant women: screening; 1996. https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/hepatitis-b-virus-infection-pregnant-women-screeni. Accessed 17 Feb 2018.
Ko SC, Fan L, Smith EA, Fenlon N, Koneru AK, Murphy TV. Estimated annual perinatal hepatitis b virus infections in the United States, 2000–2009. J Pediatr Infect Dis Soc. 2014. https://doi.org/10.1093/jpids/piu115.
Uddin SG, Simon AE, Myrick K. Routine prenatal care visits by provider specialty in the United States, 2009–2010. NCHS Data Brief. 2014;(145):1-8.
U.S. Census Bureau (2010). Santa Clara County, California. https://factfinder.census.gov/faces/nav/jsf/pages/community_facts.xhtml?src=bkmk. Accessed 17 Feb 2018.
Din ES, Wasley A, Jacques-Carroll L, Sirotkin B, Wang S. Estimating the number of births to hepatitis B virus-infected women in 22 states, 2006. Pediatr Infect Dis J. 2011;30(7):575–9.
Center for Infectious Diseases. Vaccine-Preventable Diseases and Immunization Coverage in California, 2001–2006. California: Department of Public Health; 2008. p. 112.
Wang J, Feng Q, Tam A, Sun T, Zhou P, So S. Evaluation of the first open-access hepatitis B and safe injection online training course for health professionals in China. BMC Med Educ. 2016;16:81.
Chao SD, Wang BM, Chang ET, Ma L, So SK. Medical training fails to prepare providers to care for patients with chronic hepatitis B infection. World J Gastroenterol. 2015;21(22):6914–23.
Chao SD, Cheung CM, Yang EJ, So SK, Chang ET. Low levels of knowledge and preventive practices regarding vertical transmission among perinatal nurses. J Obstet Gynecol Neonatal Nurs. 2012;41:494–505.
Chang ET, Sue E, Zola J, So SK. 3 for life:a model pilot program to prevent hepatitis B virus infection and liver cancer in Asian and Pacific islander Americans. Am J Health Promot. 2009;23(3):176–81.
Chang ET, Nguyen BH, So SK. Attitudes toward hepatitis B and liver cancer prevention among Chinese Americans in the San Francisco Bay Area, California. Asian Pac J Cancer Prev. 2008;9(4):605–13.
Wu CA, et al. Hepatitis B and liver cancer knowledge and preventive practices among Asian Americans in the San Francisco Bay Area, California. Asian Pac J Cancer Prev. 2007;8(1):127–34.
Chao SD, et al. The jade ribbon campaign: a model program for community outreach and education to prevent liver cancer in Asian Americans. J Immigr Minor Health. 2007;11(4):281–90.
Bailey MB, Shiau R, Zola J, Fernyak SE, Fang T, So SK, Chang ET. San Francisco Hep B free: a grassroots community coalition to prevent hepatitis B and liver cancer. J Community Health. 2011;36(4):538–51.
Taylor VM, Jackson JC, Chan N, Kuniyuki A, Yasui Y. Hepatitis B knowledge and practices among Cambodian American women in Seattle, Washington. J Community Health. 2002;27(3):151–63.
Ma GX, Fang CY, Shive SE, Toubbeh J, Tan Y, Siu P. Risk perceptions and barriers to Hepatitis B screening and vaccination among Vietnamese immigrants. J Immigr Minor Health. 2007;9(3):213–20.
CDC. When a pregnant woman has hepatitis B. https://www.cdc.gov/hepatitis/hbv/perinatalxmtn.htm. Accessed 16 Mar 2017.
Chao SD. Hepatitis B and Moms-to-Be. http://www.hepbmoms.org/brochures. Accessed 16 Mar 2017.
Culp LA, Caucci L, Fenlon NE, Lindley MC, Nelson NP, Murphy TV. Assessment of state perinatal hepatitis B prevention laws. Am J Prev Med. 2016;51(6):e179–85.
Nguyen G, Garcia RT, Nguyen N, Trinh H, Keeffe EB, Nguyen MH. Clinical course of hepatitis B virus infection during pregnancy. Aliment Pharmacol Ther. 2009;29(7):755–64.
Yang YB, Li XM, Shi ZJ, Ma L. Pregnant woman with fulminant hepatic failure caused by hepatitis B virus infection: a case report. World J Gastroenterol. 2004;10(15):2305–6.
Giles M, Visvanathan K, Lewin S, Bowden S, Locarnini S, Spelman T, Sasadeusz J. Clinical and virologic predictors of hepatitis B flares in pregnant women with chronic hepatitis B. Gut. 2014;64(11):1810–5.
Elefsiniotis I, Vezali E, Vrachatis D, Hatzianastasiou S, Pappas S, Farmakidis G, Vrioni G, Tsakris A. Post-partum reactivation of chronic hepatitis B virus infection among hepatitis B e-antigen-negative women. World J Gastroenterol. 2015;21(4):1261–7.
Ferrante JM, et al. Family physicians’ knowledge and screening of chronic hepatitis and liver cancer. Fam Med. 2008;40(5):345–51.
Dulay M, Zola J, Hwang J, Baron A, Lai C. Are primary care clinicians knowledgeable about screening for chronic hepatitis B infection? Presented at the 30th annual meeting of the Society of General Internal Medicine (SGIM), Toronto, Canada. J Gen Intern Med. 2007;22(Suppl 1):100.
Lai CJ. Provider knowledge and practice regarding Hepatitis B screening in Chinese-speaking patients. J Cancer Educ. 2007;22(1):37–41.
Yang EJ, Cheung CM, So SKS, Chang ET, Chao D. Education and counseling of pregnant patients with chronic hepatitis B: perspectives from obstetricians and perinatal nurses in Santa Clara County, California. Asian Pac J Cancer Prev. 2013;14(3):1707–13.
CDC. Screening and referral algorithm for hepatitis B virus (HBV) infection among pregnant women; 2015. https://www.cdc.gov/hepatitis/hbv/pdfs/prenatalhbsagtesting.pdf. Accessed 16 Mar 2017.
Acknowledgements
The authors are most grateful to Professor Qimeng Feng for his assistance in statistical analysis, and Elizabeth Yang for her assistance in data collection.
STROBE statement
The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement.
Funding
This study was funded by a grant from the Centers for Disease Control and Prevention (CDC), grant #1R18PS000830. The CDC did not participate in study design, collection, data interpretation, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
SDC, CC, SS participated in study design. SDC and CC participated in data collection. SDC, CC, ETC, and SS participated in data analysis and interpretation. SDC, CC, AP, and SS were major contributors to manuscript preparation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All study participants provided written consent for participation. The study was reviewed and approved by the Stanford University Institutional Review Board (Protocol Number 11164).
Consent for publication
N/A.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chao, S.D., Cheung, C.M., Chang, E.T. et al. Management of hepatitis B infected pregnant women: a cross-sectional study of obstetricians. BMC Pregnancy Childbirth 19, 275 (2019). https://doi.org/10.1186/s12884-019-2421-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-019-2421-5