
Abstract
Background
Husbands’ knowledge and awareness of pregnancy complications have a positive impact on their wives’ utilization of maternal health care services. In this study, we examined whether husbands’ knowledge and awareness of pregnancy complications can serve as determinants of maternal health service utilization among wives from the tribal population.
Methods
This cross-sectional study was conducted in the rural Gadchrioli district of Maharashtra, India, during November 2014–March 2015. This study included a representative population-based sample of 385 men whose wives had given birth in last 2 years at the age of 15–49 years. A multistage sampling strategy was adopted to select the respondents. Univariate, bivariate, and binary logistic regression analyses were applied to examine the association between men’s knowledge and maternal health service utilization.
Results
The result revealed that an increase in husbands’ education level increased the wives’ utilization of antenatal (ANC) care services. The type of tribe also contributed to significant differences in ANC utilization (OR: 2.64; 95% CI: 0.847–8.24). Regarding standard of living, husbands who were poor were 22% less likely than husbands in the rich category to report the utilization of ANC by their wives. Men with partial or complete knowledge of pregnancy, childbirth, and postpartum complications were more likely to utilize all maternal health services by their wives.
Conclusions
The wives are of men who aware of complications during pregnancy and childbirth are more likely to use maternal health services. Therefore, educating and empowering men about pregnancy complications will contribute to the reduction in maternal and neonatal deaths.
Similar content being viewed by others


Background
Every day in 2015, approximately 830 women died due to complications during pregnancy and childbirth. Almost all of these deaths occurred in low-resource settings, and most could have been prevented [1]. The risk of a woman in a developing country dying from maternal-related causes during her lifetime is approximately 33 times higher than a woman in a developed country. Many determinants account for safe motherhood. The utilization of maternal health services such as complete antenatal care, institutional delivery services, and postnatal care services is associated with multiple factors that influence, directly or indirectly, the health of the mother and infant. In developing countries, maternal health service utilization is poor compared with that in developed countries. In India, maternal health service utilization is lower among tribal communities than among other social groups [2,3,4,5]. The reasons for the underutilization of maternal health services differ from place to place in the country. The major reasons are the distance from a health facility, unavailability, cultural barriers, educational level of women, economic inequalities, household status, and other demographic factors [6, 7]. The reproductive and child health programs of India exclusively focus on women to increase maternal health service utilization.
To improve maternal health, reproductive and child health programs began to focus on the male partner in 1990, and reproductive health concerns have gained continual importance. Many studies have reported the positive benefits of male knowledge of pregnancy complications for women health in developed and developing countries; these benefits include the following: the increased use of antenatal services, institutional delivery services, and postnatal care [8,9,10]. Male participation and support for women during pregnancy also discourage unhealthy practices such as smoking and tobacco use among women [11, 12].
In India, maternal mortality declined from 240 maternal deaths for 100,000 live births in 2004 to 176 maternal deaths for 100,000 live births in 2016. However, the desired level of decline has not been achieved, and the decline is not uniform across states and social groups. Scheduled caste (SC) and scheduled tribal (ST) communities have higher maternal mortality and morbidity than other social groups in India [13, 14]. The tribal population has far worst health indicators due to the underdevelopment, remote living conditions, lack of availability and accessibility maternal health services.
Husbands with knowledge of complications during pregnancy and delivery are more likely to promote wives for seeking antenatal care services, institutional deliveries, and postnatal services. Further, knowledgeable husbands will contribute to the birth preparedness [15,16,17]. In countries such as India, the majority of decisions related to pregnancy and childbirth, including the place of delivery, are taken by a male member of the household or the husband; therefore, well-informed men will make positive decisions for women [18, 19]. Several studies have provided sufficient evidence of positive childbirth outcomes for male involvement in maternal health. However, husbands’ knowledge of pregnancy complications and its association with maternal health service utilization have not been specifically documented in the Indian literature on maternal health. Furthermore, tribal men’s level of knowledge of pregnancy complications has been rarely studied. Therefore, in this study, we examined the men’s knowledge and awareness of pregnancy complications and maternal health service utilization among the Gond and Madiya tribal communities in Maharashtra, India.
Methods
Data source
This study was conducted in the Gadchiroli district of Maharashtra, India, from November 2014 to March 2015. The estimated population of Gadchiroli district is 1,072,942, with the male population being 541,328 and the female population being 531,614 as per the 2011national census. In 2011, the literacy rate among men was 82.31%. Paddy is the main agricultural produce in the district. The other agricultural produces in the district are jwar, linseed, tur, and wheat. The district has comprises 12 administrative blocks. The district as 1 civil hospital, 13 rural hospitals, 45 primary health centers, and 36 primary health units.
Study design and sampling
This study was designed as a cross-sectional descriptive community survey. A multistage sampling procedure was employed to select the participants of the study. In the first stage, the district was selected purposively. In the second stage, the block was selected on the basis of the highest tribal population. In the third stage, 19 villages were selected using the probability proportional to size sampling method. From these villages, a list of women who delivered in the last 2 years was collected from local health care providers. In total, 385 men were interviewed those wives have given birth in last 2 years. The study excluded the men those wives died during childbirth or postpartum period. The response rate for this study was 95%.
Variable description
Face to face interviews were conducted to collect the data. Before data collection pretest was conducted on 10% sample of study in the same areas were study carried out. The questionnaire included questions related to socio-demographic characteristics such as age, education level, standard of living of household, and sanitation facilities. To capture the men’s awareness and knowledge about pregnancy complication we have adopted the safe motherhood questionnaire developed by the Maternal and Neonatal Program of JHPIEGO, an affiliate of John Hopkins University was used with some modifications with local context [20]. (See Additional file 1) This tool is widely used in the low resource setting to assess the pregnancy complications knowledge among both men and women [21, 22]. The participants’ awareness and knowledge of complications during pregnancy, during delivery, and after delivery were determined. Possible complications during pregnancy included vaginal bleeding, convulsions, prolonged labor, fever for 3 days, hypertension, no movement of the fetus, and urinary problems. Possible complications during delivery included excessive vaginal bleeding, ruptured uterus, premature labor, prolonged labor, breech presentation, and weakness. Possible complications in the postpartum period were excessive vaginal bleeding, convulsions, high fever, lower abdominal pain, vaginal discharge, painful urination, depression, severe headache, and weakness.
Outcome variables
Antenatal Care: Any antenatal care taken by women during pregnancy.
Place of delivery: The study reported institutional delivery or home delivery.
Post Natal Care: Any postnatal care taken by women after delivery.
All three variables were used as outcome variables, which are presented as dichotomous variables.
Independent variables
Men’s knowledge and awareness were assessed in three areas: complications during pregnancy, during childbirth, and in the postnatal period. The questionnaire contained multiple choice questions for each area. Each answer was coded as yes or no. Using these multiple choice questions, we created an index of three categories: no knowledge, partial knowledge, and complete knowledge of complications during pregnancy, during delivery, and after delivery. Those who reported that they did not know of any complication were coded as no knowledge, those who reported that they know of two complications were coded as partial knowledge, and those who reported that they know of more three complications and more were coded as complete knowledge. This categorization was made based on previous studies [23,24,25]. The psychometric properties for the above questions calculated based on Cronbach’s alpha value.
Other variables
In this study, the other key variables were the respondents’ age, current occupation, type of marriage (arranged or love), type of tribe (Gond or Madiya), education level (illiterate, primary, secondary, or graduation and above), type of family (joint or family), media exposure (high, moderate, or low), wealth index (low, medium, or high).
Statistical analysis
Data collected were coded and entered into CSPro software and were exported to SPSS, version 22, for analysis. Frequency, percentage, and descriptive summaries were used to describe the study variable by using univariate analysis. Logistic regression was performed to identify the association of knowledge of pregnancy complications with maternal health service utilization. These results are expressed as odds ratio (OR) and 95% confidence interval (CI). P value 0.05 denoted a significant association between outcome and explanatory variables.
Ethical concerns
The Institutional Review Board of the International Institute of Population Sciences, Mumbai, India, reviewed the study and granted ethical approval. Permission to conduct this study was granted by the local leaders of Gond and Madiya tribes and village heads. Respondents were provided an explanation of the study objectives and rationale; they were informed of their right to stop the interview at any time if they wished, without giving any reason. They were also told that their names would not be revealed anywhere. Information collected from individuals and the community was used for only academic research purposes.
Results
Socio-demographic characteristics of respondents
Table 1 presents the socio-demographic profile of the respondents. Nearly 41% of respondents belonged to the age group of 18–25 years, 43% to the 26–30 years age groups, 12% were aged 31–35 years. Around 28 of the respondents were illiterate. About 18%had completed primary schooling, 38% had studied up to secondary level education.
Agriculture is the dominant occupation with 57% of the respondents being engaged in it followed by agriculture labourer (24%) and employment in the government and private sector (14% of the sample). Around 60% of the families were nuclear with the remaining being joint. There were only two tribal groups living in the study area, the Gonds and Madiyas who comprised of 36 and 67%. Nearly 23.4% of the men had opted for love marriages. More than 75% respondents had an arranged marriage.
Men’s knowledge pregnancy complications
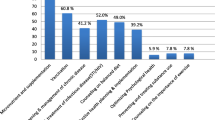
Table 2 shows knowledge about complications during pregnancy, delivery and after childbirth. Nearly 40% of the respondents reported that they did not know of any complications during pregnancy, childbirth and postpartum. Most of the men (58%) reported that they were aware of convulsions during pregnancy, prolonged labour (42%) fever (31%) and vaginal bleeding (24%). Regarding complications during pregnancy, less than one third of the respondents reported awareness of excessive bleeding, premature labour and prolonged labour. About 27% men reported that they knew about ruptured uterus and weakness. Only half of the respondents said that they had knowledge about complications during delivery. From the Table 2, it is seen that 47.8% of the men had no knowledge about the possible complications after delivery. Most of them (51%) said that women experience weakness after childbirth, and 42% said that the women have lower abdominal pain. About 28% of the men also said that women have high fever and 15% said that they were aware of depression.
Respondents’ socio-demographic characteristics and maternal health care service utilization
Socio-demographic characteristics and maternal health service utilization are presented in Table 3.Men aged 18–25 years reported higher utilization of ANC, institutional delivery, and PNC services. With the increasing age of respondents, the use of all three-maternal health services decreased. From the table, it is evident that the increasing education level of men contributed to the increased use of all three maternal health care services, and their education level was positively associated with health care service utilization. Regarding the occupation of men, men employed in salaried jobs reported higher utilization of maternal health services for their wives. Husbands’ type of job was statistically significantly associated with the utilization of all maternal health services. However, the type of family was not significantly associated with maternal health service utilization. Regarding the type of marriage, men who had a love marriage to their wives showed higher utilization of all three domains of maternal health services. Men in the rich category of the wealth index showed high utilization of all three domains of maternal health services for their wives.
Regression results of men’s knowledge of complications during pregnancy and maternal health service utilization
Table 4 shows logistic regression models that were used to examine the association between men’s knowledge and maternal health service utilization. Model 1 showed the association between socio-demographic variables and ANC utilization, model 2 examined the association between husbands’ levels of knowledge of pregnancy complications and maternal ANC service utilization. Model 3 showed the association between both socio demographic variables and pregnancy complication knowledge of husbands and utilization of ANC services for their wives.
In Model 1, husband-related characteristics were considered; in Model 2, husband’s knowledge of pregnancy complications was added; in Model 3, two sets of variables were considered. The results indicated a statistically significant association between husbands’ socio-demographic characteristics and wives’ utilization of ANC services. The result revealed that an increase in husbands’ education level increased the wives ‘utilization of ANC care services (OR: 5.75; 95% CI: 2.590–12.800). The type of tribe also contributed to significant differences in ANC utilization (OR: 2.64; 95% CI: 0.847–8.24). Regarding standard of living, husbands who were poor were 0.22 times less likely than husbands in the rich category to report the utilization of ANC by their wives.
In Model 2, husbands ‘knowledge of pregnancy was included. In this model, it was found that husbands with partial knowledge of pregnancy complications reported higher utilization of ANC by their wives than husbands having no knowledge (OR: 7.09; 95% CI: 0.76–65.65). Thus, husbands’ partial knowledge of complications during delivery was associated with their wives utilization of ANC services. By contrast, husbands with partial knowledge of complications after delivery were 3 times more likely to report the utilization of ANC by their wives than husbands having no knowledge of complications after delivery (OR: 3.88; 95% CI: 0.812–18.503). In Model 3, husbands’ characteristics and their knowledge of pregnancy were considered. It was found that husbands’ education level, Madiya type of tribe, husbands in the poor category, and complete knowledge of complications during delivery in Model 3 had same significance as those in Model 1 and Model 2.
Regression analysis was applied to understand the adjusted effect of all selected variables on the place of delivery. In Table 5, model 1 was adjusted for the socio-demographic characteristics of husbands. It was found that the education level, occupation, and wealth index were statistically significant determinants of the place of delivery for their wives. Moreover, husbands with primary education, secondary education, and high school education and more were 2.29, 3.86, and 5.75 times, respectively, more likely to report wives’ institutional delivery than husbands who were illiterate. Husbands engaging in other occupations were more likely to report their wives’ institutional delivery (OR: 2.38; 95% CI: 0.914–6.226) than their counterpart. According to the wealth index, husbands in the middle and poor categories were 0.32 and 0.52 times, respectively, less likely to report their wives’ institutional delivery. In Model 2, all background variables were excluded, and only husbands’ knowledge of pregnancy was included. After adjusting for husbands’ knowledge of pregnancy, their knowledge of complications after delivery was statistically significantly associated with the place of delivery. Husbands ‘with partial knowledge and those with complete knowledge were 1.65 (95% CI: 0.962–2.85) and 3.66 (95% CI: 1.83–7.32) times, respectively, more likely to report wives’ institutional delivery than those having no knowledge. Furthermore, the results for Model 3 were similar to this for Model 1 and Model 2; specifically, husbands’ education level, occupation, wealth index, and knowledge of complications after delivery significantly determined their wives’ institutional delivery.
The results of regressions analysis of PNC service utilization are presented in Table 6. Model 1 was adjusted for husbands’ background characteristics such as age, education level, occupation, type of family, type of tribe, and wealth index. In this model, four factors statistically significantly determined the utilization of postnatal care by respondents’ wives. For example, husbands with secondary education and high school education and more were 3 and 10 times, respectively, more likely to report wives’ postnatal utilization than those in the reference category. According to the type of family, husbands living in a joint family were less likely to utilize postnatal care (OR: .63; 95% CI: 0.395–1.013) than those living in a nuclear family. Husbands with a love marriage were 1.8 times more likely to report wives’ postnatal utilization than those with an arranged marriage. According to the wealth index, husbands in the middle and poor categories (OR: .580; 95% CI: 0.328–1.025 and OR: 0.608; 95% CI: 0.338–1.095, respectively) were less likely to report their wives’ postnatal utilization than those in the rich category.
The results indicated a statistically significant association between wives’ PNC utilization and husbands’ knowledge of pregnancy complications in Model 2. Husbands with partial knowledge and complete knowledge of complications after delivery (OR: 4.843; 95% CI: 2.731–8.587 and OR: 10.17; 95% CI: 4.403–23.50, respectively) were more likely to report wives’ PNC utilization than their counterpart. The results for Model 3, which included both husbands ‘characteristics and knowledge of pregnancy, husbands’ education level and knowledge of complications after delivery were similar to Model 1 and Model 2. In addition, husbands aged 25–29 years were 1.81 times more likely to report their wives’ postnatal check than in those in reference category.
Discussion
In this study, Gond and Madiya tribal men’s level of knowledge and awareness of complications during pregnancy, during childbirth, and in the postnatal period were found to be poor. A large proportion of men were not aware of at least one pregnancy complication. Furthermore, illiterate men were less likely to possess knowledge of complications during pregnancy, during childbirth, and in the postpartum period. Awareness of the complications of vomiting, abdominal pain, and convulsions was high among the study participants. Nearly half of the tribal men were unaware of any pregnancy complication during pregnancy. This finding is consistent with the findings of previous studies conducted in South Asia and India [26]. Tribal people in India live in remote areas. They are not exposed to development; thus, overall development is extremely poor.
The major results of this study are the association found between husbands’ knowledge of pregnancy complications and maternal health care service utilization. Husbands with complete knowledge of pregnancy complications were more likely to report antenatal care, delivery, and postnatal care utilization by their wives than husbands having no knowledge. To the best of our knowledge, this is the first study to examine the relationship between men’s knowledge of pregnancy complications and maternal health care utilization among tribal communities in India. Studies have identified a wide range of factors responsible for maternal health service utilization in India. These factors include the limited availability of health care within an area, lack of health care human resources, poor road connectivity, poor level of awareness of institutional delivery services, and lack of transportation [27,28,29,30]. National and sub national studies have reported that the knowledge of pregnancy complications among men or husbands have positive health outcomes for women in the general population. Male support and involvement in the matters of reproductive health of women also have positive outcomes for women health, specifically for maternal health care service utilization [19, 31,32,33,34]. Moreover, men with higher levels of awareness related to pregnancy complications are more likely to participate in maternal health.
Most studies have been conducted in women to evaluate the knowledge of pregnancy complications; however, to the best of our knowledge, this study is the first to examine husbands’ knowledge of pregnancy complications and its association with maternal health care service utilization by wives. The main study rationale was that men are the primary decision makers regarding health and health care in the family and also regarding reproductive health concerns. Therefore, educating the male population about concerns and problems of maternal health in general and pregnancy complications in particular is an important strategy to achieve the higher utilization of maternal health services.
The study results are significantly useful for policy makers, program managers, and health care workers in addressing maternal health concerns, specifically those in underserved populations such as tribal communities in India. Increasing the education levels of the tribal population is an urgent requirement. Utilizing information, education and communication (IEC) material to demonstrate the causes and symptoms of pregnancy complications to communities may be an effective strategy for increasing the education levels. Further, educating men about pregnancy complications could be important component of any intervention to address the maternal health.
Study limitations
This study has several limitations. First, the study sample is smaller than that of other national studies. This study was conducted in two specific tribal groups, namely Gond and Madiya, in the tribal-dominated district of Gadchiroli, Maharashtra, India. Therefore, the results of this study may not by generalizable to the general population or other tribal groups. This study examined men’s knowledge of complications during pregnancy, during childbirth, and in the postpartum period and its association with maternal health service utilization; however, other factors may play an important role in maternal health service utilization; this is a major limitation of this study. This study was conducted in men whose wives had given birth in last 2 years; occasionally, another person in the family may be aware of pregnancy complications, eventually leading to the use of maternal health services. While conducting interviews with men, researchers provided the possible answers in options so that they could immediately match their awareness to particular options; therefore, it is possible that respondents provided socially acceptable answers.
Since the use of maternal services occurs before the survey of men, that use may influence the men’s knowledge of complications, especially if the wives of had any complications. The does not received any specific education from any health care workers. The men’s knowledge of complications entirely dependent on the men’s interest to learn from local health workers such as ASHAs and Multipurpose workers.
Conclusion
Despite these limitations, the findings of the study are useful for program managers and health care providers. Engaging and informing husbands about pregnancy and pregnancy complications and the importance of maternal health service use comprise a useful strategy to reduce maternal mortality and morbidity in the tribal population. Community health care workers play an important role in informing husbands about pregnancy-related matters; this represents an important strategy that can lead to safer deliveries.
Abbreviations
- ANC:
-
Antenatal care
- ASHA:
-
Accredited Social Health Activist
- PNC:
-
Postnatal care
References
Trends in maternal mortality. 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization; 2015.
Adamson PC, Krupp K, Niranjankumar B, Freeman AH, Khan M, Madhivanan P. Are marginalized women being left behind? A population-based study of institutional deliveries in Karnataka, India. BMC Public Health. 2012;12(1):30.
Jungari S, Bomble P. Caste-based social exclusion and health deprivation in India. J Exclusion Stud. 2013;3(2):84–91.
Jungari S, Chauhan BG. Caste, wealth and regional inequalities in health status of women and children in India. Contemp Voice Dalit. 2017;9(1):87–100.
Saxena D, Vangani R, Mavalankar D, Thomsen S. Inequity in maternal health care service utilization in Gujarat: analyses of district-level health survey data. Glob Health Action. 2013;6(1):19652.
Singh L, Rai RK, Singh PK. Assessing the utilization of maternal and child health care among married adolescent women: evidence from India. J Biosoc Sci. 2012;44(1):1–26.
Singh A, Padmadas SS, Mishra US, Pallikadavath S, Johnson FA, Matthews Z. Socio-economic inequalities in the use of postnatal care in India. PLoS One. 2012;7(5):e37037.
Ramchandani PG, Domoney J, Sethna V, Psychogiou L, Vlachos H, Murray L. Do early father–infant interactions predict the onset of externalising behaviours in young children? Findings from a longitudinal cohort study. J Child Psychol Psychiatry. 2013;54(1):56–64.
Redshaw M, Henderson J. Fathers’ engagement in pregnancy and childbirth: evidence from a national survey. BMC Pregnancy Childbirth. 2013;13(1):70.
Starrs AM. Safe motherhood initiative: 20 years and counting. Lancet. 2006;368(9542):1130–2.
Martin LT, McNamara MJ, Milot AS, Halle T, Hair EC. The effects of father involvement during pregnancy on receipt of prenatal care and maternal smoking. Matern Child Health J. 2007;11(6):595–602.
Schaffer MA, Lia-Hoagberg B. Effects of social support on prenatal care and health behaviors of low-income women. J Obstet Gynecol Neonatal Nurs. 1997;26(4):433–40.
Nayar KR. Social exclusion, caste & health: a review based on the social determinants framework. Indian J Med Res. 2007;126(4):355.
Baru R, Acharya A, Acharya S, Kumar AS, Nagaraj K. Inequities in access to health services in India: caste, class and region. Econ Pol Wkly. 2010;18:49–58.
Mullany BC, Becker S, Hindin MJ. The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal: results from a randomized controlled trial. Health Educ Res. 2006;22(2):166–76.
Tweheyo R, Konde-Lule J, Tumwesigye NM, Sekandi JN. Male partner attendance of skilled antenatal care in peri-urban Gulu district, Northern Uganda. BMC Pregnancy Childbirth. 2010;10(1):53.
Iliyasu Z, Abubakar IS, Galadanci HS, Aliyu MH. Birth preparedness, complication readiness and fathers’ participation in maternity care in a Northern Nigerian community. Afr J Reprod Health. 2010;14:21–32.
Char A, Saavala M, Kulmala T. Influence of mothers-in-law on young couples’ family planning decisions in rural India. Reprod Health Matters. 2010;18(35):154–62.
Chattopadhyay A. Men in maternal care: evidence from India. J Biosoc Sci. 2012;44(2):129–53.
JHPIEGO. Maternal and Neonatal Health Pro-gram. Birth Preparedness and Complication Readiness: A Matrix of Shared Responsibilities. Maryland: JHPIEGO; 2004.
Bintabara D, Mpembeni RN, Mohamed AA. Knowledge of obstetric danger signs among recently-delivered women in Chamwino district, Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2017;17(1):276.
Smeele P, Kalisa R, van Elteren M, van Roosmalen J, van den Akker T. Birth preparedness and complication readiness among pregnant women admitted in a rural hospital in Rwanda. BMC Pregnancy Childbirth. 2018;18(1):190.
Hailu D, Berhe H. Knowledge about obstetric danger signs and associated factors among mothers in Tsegedie district, Tigray region, Ethiopia 2013: community based cross-sectional study. PLoS One. 2014;9(2):e83459.
Hibstu DT, Siyoum YD. Knowledge of obstetric danger signs and associated factors among pregnant women attending antenatal care at health facilities of Yirgacheffe town, Gedeo zone, southern Ethiopia. Arch Public Health. 2017;75(1):35.
Mwilike B, Nalwadda G, Kagawa M, Malima K, Mselle L, Horiuchi S. Knowledge of danger signs during pregnancy and subsequent healthcare seeking actions among women in urban Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2018;18(1):4.
Bloom SS, Tsui AO, Plotkin M, Bassett S. What husbands in northern India know about reproductive health: correlates of knowledge about pregnancy and maternal and sexual health. J Biosoc Sci. 2000;32(2):237–51.
Griffiths P, Stephenson R. Understanding users’perspectives of barriers to maternal health care use in Maharashtra, India. J Biosoc Sci. 2001;33(3):339–59.
Jat TR, Ng N, San Sebastian M. Factors affecting the use of maternal health services in Madhya Pradesh state of India: a multilevel analysis. Int J Equity Health. 2011;10(1):59.
Navaneetham K, Dharmalingam A. Utilization of maternal health care services in southern India. Soc Sci Med. 2002;55(10):1849–69.
Pillai RK, Williams SV, Glick HA, Polsky D, Berlin JA, Lowe RA. Factors affecting decisions to seek treatment for sick children in Kerala, India. Soc Sci Med. 2003;57(5):783–90.
August F, Pembe AB, Mpembeni R, Axemo P, Darj E. Men’s knowledge of obstetric danger signs, birth preparedness and complication readiness in rural Tanzania. PLoS One. 2015;10(5):e0125978.
Barua A, Pande RP, MacQuarrie K, Walia S. Caring men? Husbands' involvement in maternal care of young wives. Econ Polit Wkly. 2004;39:5661–8.
Bhalerao VR, Galwankar MM, Kowli SS, Kumar RR, Chaturvedi RM. Contribution of the education of the prospective fathers to the success of maternal health care programme. J Postgrad Med. 1984;30(1):10.
Narang H, Singhal S. Men as partners in maternal health: an analysis of male awareness and attitude. Int J Reprod Contracept Obstetrics Gynecol. 2016;2(3):388–92.
Acknowledgements
The authors would like to thanks field work team and health care providers in the study area for providing the details of participants. We also thank the participants for their active participation.
Funding
Not received any funding.
Availability of data and materials
The anonymized data generated or analyzed during this study are available from the first author on reasonable requests.
Author information
Authors and Affiliations
Contributions
SJ conceived research idea, collected the data, analysis and written manuscript. BP guided and supervised the data collection and edited the manuscript. Both authors were involved in the design of the study and interpretation of the data. Both authors have approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance to conduct the study was obtained from the International Institute for Population Sciences, Mumbai, India. Individual written consent was obtained from participants for conducting the survey.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
The questionnaire used for this study to assess the men’s knowledge of pregnancy complications and utilization of maternal health care services by their wives. Brief description of the data: Questionnaire examining the men’s knowledge of pregnancy complications and utilization of maternal health care services by their wives. (DOCX 25 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Jungari, S., Paswan, B. What he knows about her and how it affects her? Husband’s knowledge of pregnancy complications and maternal health care utilization among tribal population in Maharashtra, India. BMC Pregnancy Childbirth 19, 70 (2019). https://doi.org/10.1186/s12884-019-2214-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-019-2214-x