
Abstract
Objective
Fibrinogen, essential in primary hemostasis, platelet aggregation, and leukocyte-endothelial interactions, is also associated with a heightened risk of acute ischemic stroke (AIS). However, its influence on AIS patient outcomes is unclear. This study examines the correlation between fibrinogen levels and the risk of unfavorable outcomes three months post-AIS.
Methods
This is a secondary analysis of a prospective cohort study conducted in Korea. The sample consisted of 1851 AIS patients who received treatment at a Korean hospital between January 2010 and December 2016. Statistical models were established to understand the relationship between fibrinogen levels(mg/dL) and unfavorable outcomes(mRs ≥ 3), including logistic regression models, Generalized Additive Models (GAM), and smooth curve fitting (penalized splines). The log-likelihood ratio test has been utilized to evaluate the best fit. To ensure the robustness of the results, sensitivity analyses were conducted by reanalyzing the relationship after excluding participants with TG > 200 mg/dl and BMI > 25 kg/m2. Subgroup analyses were also performed to assess whether influencing factors modify the association between fibrinogen levels and unfavorable outcomes.
Results
After adjusting for multiple covariates including age, BMI, sex, LDL-c, TG, HGB, HDL-c, BUN, FPG, ALB, PLT, AF, hypertension, smoking, DM, mRs score at admission, the binary logistic regression model demonstrated revealed a significant positive association between fibrinogen levels and the risk of unfavorable outcomes in AIS patients (OR = 1.215, 95% CI: 1.032–1.429, p = 0.019). Sensitivity analyses supported these findings, with similar ORs observed in subsets of patients with TG < 200 mg/dL (OR = 1.221, 95% CI: 1.036–1.440) and BMI < 25 kg/m2 (OR = 1.259, 95% CI: 1.051–1.509). Additionally, the relationship between fibrinogen levels and outcomes was nonlinear, with a critical threshold of 2.74 g/L. Below the inflection point, the OR for unfavorable outcomes was 0.666 ((95% CI: 0.360, 1.233, p = 0.196), whereas above it, the OR increased to 1.374 (95% CI: 1.138, 1.659).
Conclusions
This study has provided evidence of a positive and nonlinear correlation between fibrinogen levels and 3-month poor functional outcomes in patients with AIS. When fibrinogen levels exceeded 2.74 g/L, a significant and positive association was observed with the risk of poor outcomes. This study provides a further reference for optimizing rehabilitation exercises and facilitating clinical counseling in patients with acute ischemic stroke.
Similar content being viewed by others


Introduction
Acute Ischemic Stroke (AIS) often leads to death or disability in patients [1,2,3]. Accurately predicting the prognosis of AIS patients is crucial for developing personalized treatment plans and improving patient outcomes [4]. Age, cardiac disease, diabetes, etiology of stroke, and hypertension have been identified as major prognostic factors for stroke [5,6,7]. Indeed, biomarkers play a key role in the management and prognostic assessment of AIS. Some biomarkers not only aid in diagnosis but can also predict disease progression and outcomes, providing clinicians with objective, quantifiable indicators to assist in clinical decision-making [8, 9].
Fibrinogen is an acute-phase protein that plays a crucial role in platelet activation, coagulation, and inflammatory responses [10,11,12]. In the general population, higher levels of fibrinogen have been identified as a risk factor for cardiovascular events, including ischemic stroke [13,14,15]. Research has confirmed that inflammatory responses and a hypercoagulable state are associated with poor prognosis following a stroke [16]. However, few studies have explored the relationship between fibrinogen levels and functional prognosis after AIS, with inconsistent findings reported. One study confirmed that hyperfibrinogenemia (> 4.0 g/L) is associated with a 1.76-fold increase in the risk of in-hospital mortality (hazard ratio, HR = 1.76; 95% confidence interval [CI]: 1.10–2.81), but found no significant association with poor prognosis at discharge (mRS > 3) [17]. A study from India demonstrated through regression analysis that fibrinogen levels (mg/dl) were positively correlated with early neurological deterioration (OR = 1.004, 95% CI 1.000-1.007, P = 0.038) [18]. Another study showed that after adjusting for potential confounders, the relationship between fibrinogen levels and poor outcomes after AIS (mRS > 3) was not significant (OR = 1.05, 95% CI: 0.90–1.21) [19]. However, it is well known that high levels of fibrinogen are considered a risk factor for ischemic stroke. Therefore, we propose a hypothesis that elevated fibrinogen may still be positively correlated with adverse outcomes in AIS patients. Additionally, considering the inconsistency of these results (based on linear regression), which may be influenced by non-linear associations and variations in the distribution range of fibrinogen, there may exist a non-linear relationship between fibrinogen levels and adverse outcomes in AIS patients. The objective of this study was to investigate the relationship, both linear and nonlinear, between fibrinogen levels and unfavorable outcomes in AIS patients, utilizing data from a Korean cohort study.
Methods
Study design
This is a secondary analysis based on a prospective cohort study in South Korea [20]. The original researchers utilized prospective single-center registry data to collect information on patients diagnosed with AIS admitted within one week of symptom onset, covering January 2010 to December 2016 [20]. Upon admission, professional nurses measured patients’ height and weight using an automatic weighing scale (Model GL-150, G-Tech International, Hwaseong-si, Gyeonggi-do, South Korea). For severely affected stroke patients who could not stand independently, weight was measured using a bed scale and height with a tape measure. Laboratory data, including Scr, TG, and fibrinogen were extracted from electronic medical records. A modified Rankin Scale (mRs) score was also conducted upon admission to assess the initial neurological condition [20].
Data source and study population
This second analysis employed data and information from the article “Geriatric Nutritional Risk Index Predicts Poor Outcomes in Patients with Acute Ischemic Stroke - Automated Undernutrition Screen Tooll” by Kang MK, et al., published under the Creative Commons Attribution License allowing unlimited use with proper attribution [20]. Originally approved by Seoul National University Hospital’s IRB (IRB number 1009-062-332) with a patient consent waiver, no additional ethical approval was needed for this second analysis [20].
The initial study initially included 2,084 patients diagnosed with acute AIS. However, 72 patients lacking dysphagia testing or laboratory information within 24 h of admission, along with 106 individuals without a three-month modified Rankin Scale (mRS) score after discharge, were subsequently excluded. As a result, the final sample size for the original study amounted to 1,906 participants. For the current study, an additional exclusion criterion was applied, resulting in the exclusion of participants with fibrinogen deficiency (n = 22) as well as those with fibrinogen abnormalities and extreme values (greater than or less than three standard deviations from the mean) (n = 33).
Variables
Fibrinogen
Fibrinogen, measured in g/L, is considered a continuous variable for patients with AIS within 24 h of admission [20]. Fibrinogen was transformed into a categorical variable based on quartiles: Q1 (< 2.80), Q2 (2.80–3.19), Q3 (3.19–3.67), and Q4 (≥ 3.67).
Neurological recovery status of acute ischemic stroke patients at three months
The neurological recovery status of AIS patients at three months was evaluated using the mRS score [21]. Data was collected through telephone interviews or structured outpatient interviews [20]. An unfavorable outcome was defined as an mRS score of 3 or higher [20, 21].
Covariates
In our study, we selected covariates based on previous research and our clinical expertise [20, 22,23,24]. The following variables were utilized as covariates: (i) Categorical variables: sex, diabetes mellitus (DM), age, atrial fibrillation (AF), smoking, and hypertension; (ii) continuous variables: hemoglobin concentration (HGB), serum high-density lipoprotein cholesterol (HDL-c), body mass index (BMI), total serum cholesterol (TC), geriatric nutritional index(NRI), fasting blood glucose (FBG), blood Urea Nitrogen (BUN), serum low-density lipoproteins cholesterol (LDL-c), platelet (PLT), mRs score at admission, serum triglyceride (TG), international normalized ratio(INR), serum albumin (ALB), activated partial thromboplastin time(APTT).
Missing data processing
In our study, a total of 1 (0.05%), 1 (0.05%), 67 (3.62%), 91 (4.92%), 99 (5.35%), and 130 (7.02%) participants had missing data for WBC, TC, LDL-c, HDL-c, TG, and FBG, respectively. To address this issue and minimize potential bias in the modeling phase, we employed multiple imputation techniques to estimate the missing values [25, 26]. Age, LDL-c, HGB, sex, TG, ALB, PLT, BUN, FBG, hypertension, DM, AF, smoking, and mRs scores at admission were included in the estimation model (number of iterations was 10, and regression type was linear regression). The missing data analysis process used the missing at random (MAR) assumption [25].
Statistical analysis
Mean and standard deviation are reported for normally distributed continuous variables, while medians (quartiles) are reported for skewed distributions, and frequencies with percentages are reported for categorical variables. Differences among different fibrinogen quartile groups were tested using the χ2 test, one-way ANOVA test, or Kruskal-Wallis H test, depending on the type of variable.
Two different models were constructed using univariate and multivariate binary logistic regression (binary dependent variable: mRS < 3; mRS ≥ 3) and linear regression analysis (mRS as a continuous variable) to investigate the association between fibrinogen and the risk of unfavorable outcomes after AIS. The variables adjusted in the multivariable logistic regression model include sex, HDL-c, age, BMI, LDL-c, HGB, PLT, TG, ALB, BUN, hypertension, DM, smoking, atrial fibrillation, and mRS score at admission. Odds ratios (OR) and their corresponding 95% confidence intervals (95% CI) were calculated and reported. Adjustment for confounding variables was based on clinical knowledge, existing literature, and results from univariate analyses. The multivariate regression equation adjusted for variables excluding TC because of its covariance with other factors (Supplementary Table S1). Besides, the decision to adjust for covariates is also guided by the following principle: when a covariate is added to the model, the matched odds ratio changes by at least 10% (Supplementary Table S2) [27].
The nonlinear relationship between fibrinogen and adverse outcomes was further investigated through generalized additive modeling (GAM) and smooth curve fitting using penalized splines. When nonlinearity was observed, an iterative algorithm was employed to compute inflection points, which were subsequently used to construct binary logistic regression models on each side of the inflection point. A log-likelihood ratio test was utilized to determine the most appropriate model for describing the relationship between fibrinogen levels and unfavorable prognosis in AIS patients.
A set of sensitivity analyses were performed to assess the robustness of the findings. Fibrinogen was transformed into a categorical variable using quartiles, and P values for trends were computed to evaluate the impact of fibrinogen as a continuous variable and to investigate potential nonlinearity. Given the significant correlation between obesity, hypertriglyceridemia, and unfavorable prognosis in patients with AIS [25, 28]. As a result, we excluded patients with TG > 200 mg/dL and BMI ≥ 25 kg/m2 from other sensitivity analyses to investigate the association between fibrinogen and unfavorable outcomes in AIS patients [29, 30]. Besides, participants were divided into high fibrinogen and non-high fibrinogen groups based on the clinical cutoff value (4.0 g/L) for propensity score(PS) matching analysis [31]. Fibrinogen was used as the independent variable, and all baseline parameters listed in Supplementary Table S3 were used as variables in the non-fitted multivariate logistic regression model to calculate PS. Variables used for matching included sex, DM, age, AF, smoking, hypertension, HDL-c, BMI, TC, FPG, BUN, LDL-c, PLT, INR, mRs score at admission, TG, ALB, GLB, and APTT, using a 1:1 matching scheme without replacement (greedy matching algorithm) with a caliper width of 0.05. Additionally, potential unobserved confounders between fibrinogen and poor outcome were investigated by calculating E-value [32]. Furthermore, we used generalized additive modeling (GAM) to incorporate continuous covariates as curves in the equations to ensure the robustness of the results.
Besides, subgroup analyses on various subgroups, including sex, age, hypertensive disease, diabetes, and smoking status, using stratified binary logistic regression models. Age was categorized into < 60, 60–70, 70–80, and ≥ 80 years [7]. Adjustments were made for each stratification factor, such as sex, age, HDL-c, BMI, LDL-c, HGB, PLT, TG, ALB, BUN, hypertension, DM, smoking, AF, and mRs scores at admission. Moreover, likelihood ratio tests were performed to compare models with and without interaction terms.
The STROBE statement was adhered to when documenting all findings [27]. Statistical analysis was performed using the R software (http://www.R-project.org, The R Foundation) and the EmpowerStats software (http://www.empowerstats.com, X&Y Solutions, Inc, Boston, MA). Statistical significance was determined by considering two-sided P values less than 0.05.
Results
A total of 1851 participants were included in this second analysis, consisting of 1,134 males and 717 females. Figure 1 depicted the participant selection process. The number of participants aged < 60, 60–70, 70–80, and ≥ 80 years were 426, 487, 651, and 287, respectively. The prevalence of hypertension, DM, and AF was 63.1%, 31.87%, and 21.56%, respectively. Fibrinogen levels are normally distributed, ranging from 1.25 to 5.85 g/L, with a mean (standard deviation) of 3.282 ± 0.782 g/L (Supplementary Figure S1). Table 1 listed the demographic and clinical characteristics of the study participants. The participants were divided into subgroups based on fibrinogen quartiles(< 2.80, 2.8–3.19, 3.19–3.67, ≥ 3.67 g/L). Compared to the first quartile group (fibrinogen < 2.8 g/L), patients in the fourth quartile had higher levels of PLT, LDL-c, BUN, Scr, APTT, and mRS scores at admission and lower levels of NRI and HDL-c. Additionally, participants in the fourth quartile had a higher percentage of females, hypertension, DM, and were ≥ 80 years of age compared to those in the first quartile.

Flowchart of study participants
Incidence of unfavorable prognosis three months after acute ischemic stroke
Table 2 presented data indicating that a total of 526 participants exhibited an unfavorable prognosis. The overall incidence rate of adverse outcomes was 28.42%. Specifically, the incidence rates of unfavorable prognosis among participants in the first to fourth quartiles of fibrinogen were 24.18%, 24.35%, 27.89%, and 37.00%, respectively. When stratified by age groups (< 60, 60 to < 70, 70 to < 80, and ≥ 80), the incidence of unfavorable outcomes in individuals with AIS was higher in females compared to males, regardless of age category. Additionally, the incidence of unfavorable outcomes was observed to increase with age in both males and females (Supplementary Figure S2).
Results of univariate analysis using binary logistic regression models
The results of the univariate analysis indicate significant associations between certain factors and the risk of unfavorable outcomes in AIS patients. Specifically, BMI、HGB、TG、ALB, NRI, and LDL-c are negatively correlated with the risk. Conversely, BUN, mRs score at admission, fibrinogen, and FBG positively correlate with unfavorable outcome risks. Additionally, individuals aged 80 years or older, females, patients with hypertension, and those with DM are more likely to experience unfavorable outcomes (all P < 0.05). (Supplementary Table S4).
Results of the multivariate analysis using binary logistic regression and linear regression models
Firstly, when treating the dependent variable as a binary outcome (unfavorable outcome versus non-unfavorable outcome), multivariate logistic regression analysis revealed that each 1 g/L increase in fibrinogen was associated with a 22.9% increase in the incidence of unfavorable outcomes in AIS patients (OR = 1.229, 95% CI: 1.054, 1.434; p = 0.008). The variables adjusted for included sex, HDL-c, age, BMI, LDL-c, HGB, PLT, TG, ALB, Scr, hypertension, DM, smoking, AF, and mRS score at admission (Table 3 Model I). When fibrinogen was analyzed categorically, the test for trend in effect size (OR values) was statistically significant (P for trend < 0.05). These results indicate that the trend in effect size between groups when fibrinogen levels are transformed into categorical variables is consistent with the results when fibrinogen is treated as a continuous variable (Table 3 Model I).
Besides, when using the 3-month post-AIS mRS score as the outcome variable, multivariate logistic regression analysis(adjusted for sex, HDL-c, age, BMI, LDL-c, HGB, PLT, TG, ALB, BUN, hypertension, DM, smoking, AF, and the mRS score at admission) showed that each 1 g/L increase in fibrinogen is associated with an increase of 0.163 points in the 3-month post-AIS mRs score (β = 0.163, 95% CI: 0.058, 0.268; P = 0.002) (Supplementary Table S5). When fibrinogen levels were categorized, the trend in effect size(OR value) between groups remained consistent with the results when fibrinogen was treated as a continuous variable.
Sensitivity analyses
A series of sensitivity analyses were conducted to verify the reliability of the results. Firstly, a GAM was used to include continuous covariates as curves in the equation; the results from Model II in Table 3 are consistent with those from the fully adjusted Model I. Additionally, an E-value was calculated to assess the susceptibility of the study results to unmeasured confounding factors. Additionally, an E-value of 1.44, surpassing the relative risk of 1.32 for unmeasured confounders, suggests minimal impact from unmeasured or unknown confounders on the fibrinogen-unfavorable outcome relationship. Besides, other sensitivity analyses that excluded participants with a BMI ≥ 25 kg/m2 and TG ≥ 200 mg/dL also yielded similar results, showing a positive correlation between fibrinogen levels and the risk of unfavorable outcomes at 3 months in AIS patients. (Supplementary Table S6).
Additionally, a propensity score matching analysis involved one-to-one matching of 262 AIS patients with high fibrinogen levels to 262 AIS patients with non-high fibrinogen levels. After matching, there were no significant differences in baseline characteristics between the high and non-high fibrinogen groups (Supplementary Table S3). Further logistic regression analysis indicated that AIS patients with high fibrinogen levels had a 68.1% higher risk of unfavorable outcomes than those with lower fibrinogen levels (Supplementary Table S7).
Generalized additive models address the nonlinear relationship between fibrinogen and unfavorable outcomes
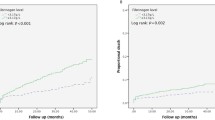
Using GAM and smooth curve fitting while adjusting for various covariates, including sex, age, HDL-c, BMI, LDL-c, HGB, PLT, TG, ALB, BUN, hypertension, DM, smoking, AF, and mRs scores at admission, we observed a nonlinear association between fibrinogen levels in patients with AIS and the risk of unfavorable outcomes(P for log-likelihood ratio test = 0.047) (Fig. 2). The inflection point of fibrinogen level (2.74 g/L) was determined using a recursive method. Subsequently, a two-piece logistic regression model was employed to estimate the OR and CI for both sides of the inflection point. The OR for the left side of the inflection point was 0.666 (95% CI: 0.360, 1.233, P = 0.196), indicating no statistically significant difference. In contrast, the OR for the right side of the inflection point was 1.374(95% CI: 0.360, 1.233, p < 0.001) (Table 4).

The nonlinear relationship between fibrinogen and the risk of unfavorable outcomes in patients with acute ischemic stroke. A nonlinear relationship was detected after adjusting for age, sex, BMI, LDL-c, HGB, TG, HDL-c, BUN, FPG, ALB, PLT, AF, hypertension, smoking, DM, and mRs score at admission
Results of subgroup analyses
In all prespecified or exploratory subgroup assessments (Supplementary Table S8), age, sex, smoking status, DM, and hypertension did not significantly interact with fibrinogen. These influences did not modify or alter the relationship between fibrinogen and unfavorable outcomes in patients with AIS.
Discussion
The objective of this study was to examine the correlation between fibrinogen and the neurological status of patients with AIS over a period of three months. The findings revealed a positive association between fibrinogen and the risk of unfavorable outcomes after AIS. Furthermore, a threshold effect curve with an inflection point for fibrinogen of 2.74 g/L was observed. Distinct relationships between fibrinogen and unfavorable outcomes were observed on either side of this inflection point.
Fibrinogen plays a crucial role in primary hemostasis, platelet aggregation, and leukocyte-endothelial cell interactions. Additionally, it serves as a significant determinant of blood viscosity and functions as an acute-phase protein [33]. Previous research has consistently demonstrated a strong association between fibrinogen and an elevated risk of ischemic stroke [13, 14, 34,35,36]. Therefore, we hypothesize that fibrinogen may also be associated with an increased risk of poor prognosis in ischemic stroke. Nevertheless, there is a paucity of research on the impact of fibrinogen on the prognosis of patients with AIS, and the conclusions are inconsistent. Several studies with limited sample sizes have indicated that elevated fibrinogen levels are linked to higher mortality rates among individuals experiencing acute stroke [37,38,39]. One study found that elevated fibrinogen levels at 24 h after rt-PA treatment were associated with an approximately 40% increase in mortality at 90 days [40]. A study using data from China’s National Stroke Registry III, which included 10,518 patients with AIS within seven days of onset (baseline), showed that high baseline fibrinogen levels were associated with poor functional prognosis (mRs > 2) (OR = 1.63; 95%=CI:1.35–1.97) [41]. Similar results were obtained in a small-sample study from India, where baseline fibrinogen (per 1 mg/dL) was positively associated with poor functional prognosis (OR = 1.011, 95% CI 1.006–1.015, P < 0.001) [18]. However, some studies have yielded inconsistent results. A previous study showed that fibrinogen levels were associated with poor functional prognosis after adjustment for simple risk factors, but this association disappeared after further adjustment for underlying factors [19]. In another earlier study, which included 83 patients treated with intravenous alteplase, fibrinogen levels at admission were not associated with prognosis (mRS > 2) at 3 months [42]. There are several possible reasons for the inconsistency of the findings. First, there were differences in the populations and sample sizes of these studies. Second, the outcome variables were different. Third, the adjusted variables were different. The results of our study are consistent with previous findings that fibrinogen levels are positively associated with poor outcomes in AIS. Besides, we also found that baseline fibrinogen levels are positively correlated with the mRS scores at 3 months post-AIS. In addition, this study explored the relationship between fibrinogen and adverse outcomes by using fibrinogen as both a categorical and continuous variable, thereby minimizing information loss and quantifying the relationship. The sensitivity analyses also focused on participants with BMI < 25 kg/m2 or TG < 200 mg/dL, and the results further confirmed the existence of the relationship in this group of participants, validating the stability of the results. In conclusion, these results suggest that fibrinogen may be a useful marker for predicting the prognosis of acute ischemic stroke, providing a reference for optimizing the rehabilitation of stroke patients and facilitating doctor-patient communication.
The underlying mechanisms by which fibrinogen levels play a role in prognosis have not been well elucidated. Blood fibrinogen levels reflect inflammatory states and coagulation disorders. Both inflammatory response and hypercoagulability are associated with poor prognosis [16, 43].
Additionally, our study is the first to observe a nonlinear relationship between fibrinogen levels and the risk of unfavorable outcomes in AIS patients. When fibrinogen levels exceed 2.74 g/L, there is a significant positive association with the incidence of unfavorable outcomes three months after AIS. This provides a reference for optimizing the rehabilitation of AIS patients in clinical settings. When a patient’s fibrinogen level exceeds 2.74 g/L, it indicates a potentially poorer prognosis, with higher levels correlating with worse outcomes. These patients may require better rehabilitation and care to minimize the risk of unfavorable outcomes.
Our study possesses several strengths. Firstly, we utilized both quartiles of fibrinogen as a categorical variable and fibrinogen as a continuous variable to examine its association with unfavorable outcomes in AIS patients. This approach reduces information loss and quantifies the relationship effectively. Secondly, addressing the nonlinear relationship represents a significant advancement compared to prior research. Thirdly, we employed the multiple imputation method to handle missing data, enhancing statistical power and mitigating potential bias resulting from missing covariate information. Moreover, to ensure the reliability of our findings, we conducted a series of sensitivity analyses. These included transforming the independent variable, calculating E-values to explore the possibility of unmeasured confounders, and reanalyzing the association between fibrinogen and unfavorable outcomes in AIS after excluding participants with a BMI ≥ 25 kg/m2 and TG ≥ 200 mg/dl. Additionally, a propensity-matched analysis was conducted to assess the relationship between high fibrinogen levels(≥ 4.0 g/L) and unfavorable outcomes in AIS patients.
It is important to acknowledge potential limitations in our study. Firstly, our study focused on Korean subjects, and further validation is necessary to assess the generalizability of these results to other racial groups. Secondly, fibrinogen measurements were conducted solely at the time of admission and were not repeated subsequently. Consequently, we lack information on whether fibrinogen levels changed within the first 24 h after admission, which warrants further investigation. Thirdly, this study’s outcome measure, the mRS score at three months post-AIS, lacks inclusion of the Glasgow Outcome Scale-Extended (GOSE) or assessments of long-term functional outcomes. While the mRS is widely used for evaluating post-stroke function, it does not fully capture all aspects of patient recovery. Future research should extend follow-up durations and include broader assessment tools like the GOSE to more thoroughly evaluate patient outcomes. Fourthly, some variables had incomplete data. For instance, the original study database provided age-stratification information in terms of ten intervals rather than the specific ages of patients, potentially resulting in incomplete data on certain variables. Future study designs may benefit from collecting more detailed variable information. Fifth, as with all observational studies, the presence of uncontrolled or unmeasured confounding factors remains a possibility, even when known potential confounders have been accounted for. Additionally, this study relied on secondary analysis of published data, which limited adjustments for variables not included in the dataset, such as information on intravenous thrombolysis or endovascular thrombectomy, antihyperglycemic medications, onset-to-door time (ODT), and timing of head CT scans. Although we calculated E-values to quantify the potential effects of unmeasured confounders, they are not a complete substitute for the effects of these confounders. Moving forward, we will initiate new study to collect more variable information.
Conclusion
This study revealed a positive and nonlinear relationship between fibrinogen levels and unfavorable functional outcomes in patients with AIS. When fibrinogen was ≥ 2.74 g/L, it was significantly and positively associated with poor function in patients with acute ischemic stroke. When the patient’s fibrinogen was greater than 2.74 g/L, it suggested that the patient’s prognosis might be poor, and this group of patients needed to enhance rehabilitation and nursing care to minimize the risk of poor prognosis, which provided a reference for clinical optimization of rehabilitation for patients with AIS.
Data availability
Users can download data from the “PLos one” database, which can be reached at https://journals.plos.org/plosone/.
Abbreviations
- AIS:
-
Acute ischemic stroke
- ALB:
-
Serum albumin
- BMI:
-
Body mass index
- BUN:
-
Blood urea nitrogen
- CI:
-
Confidence interval
- DM:
-
Diabetes mellitus
- FBG:
-
Fasting blood glucose
- FIB:
-
Fibrinogen
- GAM:
-
Generalized additive models
- HDL-c:
-
High-density lipoprotein cholesterol
- HGB:
-
Hemoglobin concentration
- LDL-c:
-
Low-density lipoproteins cholesterol
- mRS:
-
Modified Rankin Scale
- OR:
-
Odds ratio
- PLT:
-
Platelet
- Scr:
-
Serum creatinine
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
References
Prabhakaran S, Ruff I, Bernstein RA. Acute stroke intervention: a systematic review. Jama-J Am Med Assoc. 2015;313(14):1451–62.
Global regional. National burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. 2021;20(10):795–820.
Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120(3):439–48.
Harvey RL. Predictors of functional outcome following stroke. Phys Med Reh Clin N. 2015;26(4):583–98.
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418.
Jacob L, Tanislav C, Kostev K. Long-term risk of stroke and its predictors in transient ischaemic attack patients in Germany. Eur J Neurol. 2020;27(4):723–8.
Han Y, Huang Z, Zhou J, Wang Z, Li Q, Hu H, Liu D. Association between triglyceride-to-high density lipoprotein cholesterol ratio and three-month outcome in patients with acute ischemic stroke: a second analysis based on a prospective cohort study. BMC Neurol. 2022;22(1):263.
Dimaras T, Merkouris E, Tsiptsios D, Christidi F, Sousanidou A, Orgianelis I, Polatidou E, Kamenidis I, Karatzetzou S, Gkantzios A, et al. Leukoaraiosis as a promising biomarker of stroke recurrence among stroke survivors: a systematic review. Neurol Int. 2023;15(3):994–1013.
Jickling GC, Russo TL. Predicting stroke outcome: role of a biomarker panel. Neurology. 2019;92(4):157–8.
Bennett JS. Platelet-fibrinogen interactions. Ann Ny Acad Sci. 2001;936:340–54.
Heemskerk JW, Bevers EM, Lindhout T. Platelet activation and blood coagulation. Thromb Haemostasis. 2002;88(2):186–93.
Chen Y, Zhong H, Zhao Y, Luo X, Gao W. Role of platelet biomarkers in inflammatory response. Biomark Res. 2020;8:28.
Peycheva M, Deneva T, Zahariev Z. The role of fibrinogen in acute ischaemic stroke. Neurol Neurochir Pol. 2021;55(1):74–80.
Danesh J, Lewington S, Thompson SG, Lowe GD, Collins R, Kostis JB, Wilson AC, Folsom AR, Wu K, Benderly M, et al. Plasma fibrinogen level and the risk of major cardiovascular diseases and nonvascular mortality: an individual participant meta-analysis. JAMA-J AM MED ASSOC. 2005;294(14):1799–809.
Wilhelmsen L, Svärdsudd K, Korsan-Bengtsen K, Larsson B, Welin L, Tibblin G. Fibrinogen as a risk factor for stroke and myocardial infarction. New Engl J Med. 1984;311(8):501–5.
Bao Q, Zhang J, Wu X, Zhao K, Guo Y, Yang M, Du X. Clinical significance of plasma D-Dimer and fibrinogen in outcomes after stroke: a systematic review and meta-analysis. Cerebrovasc Dis. 2023;52(3):318–43.
You S, Yin X, Liu H, Zheng D, Zhong C, Du H, Zhang Y, Zhao H, Qiu C, Fan L, et al. Hyperfibrinogenemia is significantly associated with an increased risk of in-hospital mortality in acute ischemic stroke patients. Curr Neurovasc Res. 2017;14(3):242–9.
Mehta V, Sharma A, Jyoti D, Prabhakar R, Kumar R, Guria RT, Sharma CB. Fibrinogen as a predictor of early neurological deterioration in acute ischemic stroke - evidence from the Indian population. J Cent Nerv Syst Dis. 2023;15:1605283715.
Whiteley W, Jackson C, Lewis S, Lowe G, Rumley A, Sandercock P, Wardlaw J, Dennis M, Sudlow C. Inflammatory markers and poor outcome after stroke: a prospective cohort study and systematic review of interleukin-6. Plos Med. 2009;6(9):e1000145.
Kang MK, Kim TJ, Kim Y, Nam KW, Jeong HY, Kim SK, Lee JS, Ko SB, Yoon BW. Geriatric nutritional risk index predicts poor outcomes in patients with acute ischemic stroke - automated undernutrition screen tool. Plos One. 2020;15(2):e228738.
Haggag H, Hodgson C. Clinimetrics: modified Rankin scale (mRS). J Physiother. 2022;68(4):281.
Zan Y, Xiong W, Zhang X, Han Y, Cao C, Hu H, Wang Y, Ou H. Body mass index has a non-linear association with three-month outcomes in men with acute ischemic stroke: an analysis based on data from a prospective cohort study. Front Endocrinol. 2022;13:1041379.
Wang J, Tang H, Wang X, Wu J, Gao J, Diao S, Wu Y. Association of triglyceride-glucose index with early neurological deterioration events in patients with acute ischemic stroke. Diabetol Metab Syndr. 2023;15(1):112.
Wang C, Cui T, Li S, Wang T, Cui J, Zhong L, Jiang S, Zhu Q, Chen M, Yang Y et al. The change in fibrinogen is associated with outcome in patients with acute ischemic stroke treated with endovascular thrombectomy. Neurocrit Care. 2023.
Groenwold RH, White IR, Donders AR, Carpenter JR, Altman DG, Moons KG. Missing covariate data in clinical research: when and when not to use the missing-indicator method for analysis. Can Med Assoc J. 2012;184(11):1265–9.
White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30(4):377–99.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–9.
Weir CJ, Sattar N, Walters MR, Lees KR. Low triglyceride, not low cholesterol concentration, independently predicts poor outcome following acute stroke. Cerebrovasc Dis. 2003;16(1):76–82.
Appropriate body-mass. Index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–63.
Yayan J. Association of traditional risk factors with coronary artery disease in nonagenarians: the primary role of hypertension. Clin Interv Aging. 2014;9:2003–12.
Yao C, Zhang G, Zhang N, Li R, Sun S, Zhang L, Xia Y, Chen S, Sun J, Chen M. Fibrinogen Is Associated with prognosis of critically ill patients with sepsis: a study based on Cox regression and propensity score matching. Mediat Inflamm. 2023;2023:7312822.
Haneuse S, VanderWeele TJ, Arterburn D. Using the E-value to assess the potential effect of unmeasured confounding in observational studies. Jama-J Am Med Assoc. 2019;321(6):602–3.
Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, Larrue V, Lees KR, Medeghri Z, Machnig T, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. New Engl J Med. 2008;359(13):1317–29.
Eidelman RS, Hennekens CH. Fibrinogen: a predictor of stroke and marker of atherosclerosis. Eur Heart J. 2003;24(6):499–500.
Sato S, Iso H, Noda H, Kitamura A, Imano H, Kiyama M, Ohira T, Okada T, Yao M, Tanigawa T et al. Plasma fibrinogen concentrations and risk of stroke and its subtypes among Japanese men and women. Stroke. 2006;37(10):2488–2492.
Tanne D, Benderly M, Goldbourt U, Boyko V, Brunner D, Graff E, Reicher-Reiss H, Shotan A, Mandelzweig L, Behar S. A prospective study of plasma fibrinogen levels and the risk of stroke among participants in the bezafibrate infarction prevention study. Am J Med. 2001;111(6):457–63.
Swarowska M, Polczak A, Pera J, Klimkowicz-Mrowiec A, Slowik A, Dziedzic T. Hyperfibrinogenemia predicts long-term risk of death after ischemic stroke. J Thromb Thrombolys. 2014;38(4):517–21.
Frøyshov HM, Bjørnerem Å, Engstad T, Halvorsen DS. Elevated inflammatory markers predict mortality in long-term ischemic stroke-survivors: a population-based prospective study. Aging Clin Exp Res. 2017;29(3):379–85.
Turaj W, Słowik A, Dziedzic T, Pułyk R, Adamski M, Strojny J, Szczudlik A. Increased plasma fibrinogen predicts one-year mortality in patients with acute ischemic stroke. J Neurol Sci. 2006;246(1–2):13–9.
Li D, Xing C, Li Y, Zhu X. Elevated plasma fibrinogen indicates short-term poor outcome in patients with acute ischemic stroke after intravenous thrombolysis. J Stroke Cerebrovasc. 2020;29(8):104991.
Hou HQ, Xiang XL, Pan YS, Zhang QH, Li H, Meng X, Wang YJ. Baseline or 90-day fibrinogen levels and long-term outcomes after ischemic stroke or TIA: results from the China national stroke registry III. Atherosclerosis. 2021;337:35–41.
Martí-Fàbregas J, Borrell M, Cocho D, Belvís R, Castellanos M, Montaner J, Pagonabarraga J, Aleu A, Molina-Porcel L, Díaz-Manera J, et al. Hemostatic markers of recanalization in patients with ischemic stroke treated with rt-PA. Neurology. 2005;65(3):366–70.
Xu J, Sun Y, Gong D, Fan Y. Utility of fibrinogen levels for predicting survival and functional outcomes in patients with acute ischemic stroke: a meta-analysis. Curr Med Chem. 2023;30(4):481–91.
Acknowledgements
Since this is a secondary analysis, the primary sources of the data and method explanation are as follows: Kim TJ, Kim Y, Kim SK, Jeong H-Y, Nam K-W, Kim MK, et al. (2020) An automated undernutrition screen tool based on the geriatric nutritional risk score indicates that patients with acute ischemic stroke will not fare well. 15(2) PLoS ONE: e0228738. Doi: 10.1371/journal.pone.0228738. We express our gratitude to each and every research author of the original study.
Funding
This study was supported by the Shenzhen Science and Technology Program (JCYJ20180228163014668) and the Key Clinical Research Project of Shenzhen Second People’s Hospital (Grant No.20243357011).
Author information
Authors and Affiliations
Contributions
The study was designed by Feng Chen, Haofei Hu, and yuying Guo, who also carried out the statistical analysis and wrote the report. Yong Han and Dehong Liu took part in the design of the study and the revision of the paper. The final draft of the work has been reviewed and approved by all authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board of Seoul National University Hospital examined and authorized the studies involving human subjects. Furthermore, informed consent was not required, according to the Institutional Review Board (IRB No. 1009-062-332).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, F., Han, Y., Hu, H. et al. Nonlinear association of fibrinogen levels with functional prognosis in patients with acute ischemic stroke: a prospective cohort study. BMC Neurol 24, 163 (2024). https://doi.org/10.1186/s12883-024-03674-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-024-03674-4