
Abstract
Background
Cervical dystonia is a movement disorder typically characterized by a patterned and twisting movement of sustained or intermittent muscle contractions. Recently, new clinical trials are emerging, highlighting the potential benefit of physiotherapy (PT) on disease outcomes. Thus, the objective of this review is to update the effectiveness of PT on cervical dystonia disease outcomes and subsequently perform a meta-analysis.
Methods
Interventional studies published in English with adult patients with isolated cervical dystonia following a physiotherapy program were included. Relevant articles were searched in PubMed (MEDLINE), Web of Science, and Scopus. Cochrane and Joanna Briggs Institute risk of bias checklists were used for quality reporting. Meta-analysis was done using Review Manager 5.3 statistical software and a pooled mean difference for pain was presented.
Results
Fourteen articles were included in the review and two articles were included in the meta-analysis. The meta-analysis revealed that PT intervention had a significant effect on pain reduction scale (-5.00, 95% CI -6.26, -3.74) when used as an additional therapy with botulinum toxin (BoNT) injection. Additionally, findings indicate a possible positive effect of PT disease severity, disability, and quality of life.
Conclusions
Physiotherapy in addition to BoNT is recommended to decrease pain. The findings suggest a reduction of disease severity, disability, and improvement in quality of life. The variety in the type and duration of PT interventions did not allow a clear recommendation of a specific type of PT.
Similar content being viewed by others

Introduction
Cervical dystonia (CD) is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive movements, postures, or both. It is typically patterned, twisting, and may be tremulous [1]. Isolated cervical dystonia is the most common form of dystonia with a prevalence estimate of 20 − 4,100 cases/million [2, 3]. Although CD does not affect patients’ life expectancy, the disease is disabling and markedly affects patients’ quality of life [4] by causing severe functional and psychosocial impairment [5].
Functional limitations in different domains have been reported in most patients with CD [6] with impact on mobility-related activities (such as walking, driving, crossing the street, and parking) [7, 8], reduced productivity and job loss [9]. Quality of life (QoL) is also significantly affected by the presence of physical and mental health problems including mood disorders, anxiety, depression, low self-esteem, low self-confidence and pain [10].
The first treatment of choice are intramuscular injections of botulinum toxin (BoNT) [11], repeated every three to four months [12]. Other neurosurgical [13,14,15] and pharmacological [16] interventions are available but have various drawbacks. Additional to BoNT injection, paramedical interventions such as physiotherapy (PT) are advised. In 2014, we published a systematic review on the effect of PT [17]. Since then, multiple studies have been published, warranting a new overview of the effectiveness.
Therefore, the aim of this review is first to update the knowledge on the effect of PT on patients’ functioning, pain, disease severity, and quality of life. Secondly, to evaluate the effect of PT as add-on to BoNT by conducting a meta-analysis.
Methods
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA 2020) was followed [18]. The protocol was registered in PROSPERO with the number CRD42022376433 on 07/12/2022.
Eligibility criteria
Included studies are those reporting the effect of a physical therapy program (I) in patients with isolated cervical dystonia (P) on patients’ functioning including pain, disease severity, disability, and quality of life (O). In the review published in 2014 by De Pauw J et al. [17], case reports were included. For this updated literature review, the aim was to include only interventional studies. Therefore, observational studies, case reports, and conference papers were excluded.
For the meta-analysis, studies comparing PT and BoNT with BoNT alone were considered when reporting disease severity by standardized measures such as the visual analogue scale (VAS) for pain, Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS), and standardized QoL outcome measures.
Information sources
Three databases, PubMed (MEDLINE), Web of Science, and Scopus were searched for potentially relevant studies. The source was last searched on August 22, 2023.
Search strategy
The search strategy was developed following the PICO framework: population (P): adult patients with isolated cervical dystonia, intervention (I): physical therapy alone or adjuvant to BoNT injections, comparator (C): was not specified to include all available studies and the outcome(s) of interest (O) was: pain, disease severity, disability, or quality of life but was not specified to include all available studies. Accordingly, the following keywords are used: cervical dystonia or spasmodic torticollis combined with keywords related to physical therapy such as rehabilitation, physiotherapy, relaxation therapy, neuromotor rehabilitation, exercise therapy. The search strategy for each database is presented in (Table 1).
Selection process
Following removal of duplicates, all titles and abstracts of identified articles were independently screened for eligibility by two authors (JDP and SG) on the Rayyan platform [19]. The full texts of potentially relevant studies were then independently assessed to determine eligibility based on the predetermined inclusion and exclusion criteria. In case of discrepancies, a consensus meeting was held.
Data collection process
Prior to the data collection, a data extraction instrument was designed according to the Cochrane handbook for systematic reviews of interventions [20]. Key data concerning study design, study participants (sample size, sex, mean age), information regarding the disease and medical treatment if provided (duration of cervical dystonia, severity of the symptoms, duration of treatment, medication or BoNT injections), information regarding the intervention (physical therapy modalities, duration and frequency of sessions), and intervention outcomes (pain, disease severity, disability and QoL) from each of the selected studies were extracted independently by two reviewers (JDP and SG). A consensus meeting was held in case of discrepancies.
Study risk of bias assessment
Risk of bias was independently assessed by two reviewers (JDP and SG) using the Cochrane Risk of Bias checklist for randomized controlled trials [21] and the Joanna Briggs Institute (JBI) checklist for non-randomized experimental studies and case series [22]. A consensus meeting was held in case of disagreement.
Effect measures and synthesis methods
For the meta-analysis, statistical software Review Manager 5.3 was used. We aimed to estimate the change in the mean score of cervical dystonia symptoms (TWSTRS total score, pain, severity, and disability score) following a physical therapy intervention consisting of multiple treatment modalities. Studies reporting only one treatment option such as tape were not included. The pooled mean difference was presented for the outcome. The Cochrane Q-test and I2 statistics were used to evaluate heterogeneity between included studies. The I2 value is interpreted as follows: 0–40% (not important); 30–60% (moderate heterogeneity); 50–90% (substantial heterogeneity); and 75–100% (considerable heterogeneity) [23].
Results
Study selection
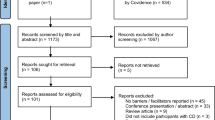
A total of 466 articles were initially identified. Before screening, duplicates were removed, resulting in 462 reports. In the first screening phase of title and abstract, 488 were excluded. The full texts of 14 potentially eligible reports were retrieved and included as they all met the inclusion criteria. Since the previous review in 2014 by De Pauw et al. [17], 8 new studies have been published and included in this review. Contrary to the review of 2014, case-reports were now excluded. Two of the 14 articles [24, 25] reported the effect of PT intervention on pain and were selected for meta-analysis. The detailed selection process is depicted in the PRISMA flow chart (Fig. 1).

PRISMA flow chart - updated systematic literature review
Study characteristics
Of the 14 included studies, 8 were RCTs [24, 26,27,28,29,30,31,32], 3 case-control studies [25, 33, 34], and 3 case-series [35,36,37]. A total of 414 patients with CD participated in the included studies. The mean reported duration of cervical dystonia ranged from 21.2 months to 27.8 years. Study participants in the intervention group received various physical therapy interventions modalities such as stretching, exercise therapy (posture, coordination, proprioception, strengthening underactive muscles, motor learning, relaxation, sensorimotor exercises with feedback), aquatic relaxation therapy, home exercise program, active and passive mobilizations of the neck, taping, biofeedback and Transcutaneous Electrical Neural Stimulation (TENS). Twelve out of 14 studies [24,25,26,27,28, 30, 31, 33,34,35,36,37] applied various physical therapy modality interventions whereas 2 studies [29, 32] used taping as the sole intervention.
The duration of the physical therapy intervention ranged from two weeks to 12 months. In 11 of the 14 included articles, the physical therapy intervention was additional to BoNT injections. In two studies, none of the participants received BoNT [33, 35]. In one study, about one-third of participants received BoNT during the length of the study [26]. Two studies compared a specialized physiotherapy program to standard physiotherapy care additional to BoNT [27, 31] (Table 2).
Risk of bias in studies
The overall risk bias was found to be ‘low’ for almost all RCTs [24, 26, 27, 29, 31, 32]; two RCTs [28, 30] had ‘some concerns’ about their quality. The methodological qualities of all case-control studies [25, 33, 34] were found to be good. The three case-series [35,36,37] have good quality (Tables 3, 4 and 5).
Result of individual studies
Effect of physical therapy on pain
The effect of PT on pain was investigated in all of the 14 studies [24,25,26,27,28,29,30,31,32,33,34,35,36,37]; four studies reported the VAS scale [28, 29, 35, 36]; 10 studies [24,25,26,27,28, 30,31,32, 34, 37] reported pain by the pain subscale of the TWSTRS; one study [33] reported both. All included studies reported a reduction of pain after physical therapy intervention which was 30% [28, 36], 40% [34], and up to 50% [24] larger in the PT group compared to the control group. When 2 types of PT intervention are compared, both types resulted in reduction of pain, no differences between the interventions were found for pain [27, 31].
Effect of physical on Disease severity
The effect of PT on disease severity was investigated in 7 studies by the TWSTRS [25, 26, 28, 30,31,32, 34]. Van den Dool et al. found an improvement of dystonic postures in the intervention group after they received specialized PT which emphasized motor training [31]. Similarly, other studies reported statistically significant improvement in severity scores in the PT group [28, 32].
Effect of physical therapy on disability
The effect of PT on disability was investigated in seven studies [25, 26, 28, 30,31,32, 34] by the TWSTRS and reported significant improvements. Tassorelli et al. also reported a marked reduction in disability score by 4.5 in activities of daily living as compared to BoNT therapy alone [24]. When 2 types of PT intervention are compared, both types resulted in reduction of disability of 1.7 points on the TWSTRS subscale [31]. However, no differences between the interventions were found [27, 31].
Effect of physical therapy on QoL
The effect of PT on patient QoL was investigated in 10 studies [25,26,27,28, 31,32,33,34, 36, 37]. It was measured by the Short Form Health Survey (SF-36) in four studies [25, 28, 33, 34], three studies [26, 32, 36] used the Craniocervical Dystonia Questionnaire (CDQ-24), two studies [27, 37] used the EuroQol group quality questionnaire (EQ-5D), and one study used both the SF-36 and CDQ-24 [31]. Data on QoL were not always clearly reported. There is conflicting evidence on the different domains of the SF-36. General health perceptions improved after PT intervention in two studies [31, 34], mental health improved in three studies [25, 33, 34] but one study found no effect [28].
Meta – analysis: effect of PT additional to BoNT
Two studies with low risk of bias reporting on the effect of PT additional to BoNT compared to BoNT alone were selected [24, 25]. A fixed effect model was used, and the mean difference was reported. Regarding study heterogeneity, there was no evidence of clinical, methodological, or statistical heterogeneity for outcome analysis of pain. For the other outcome measures of disease severity, disability, and QoL, there was significant heterogeneity observed among the studies. The I2 statistics were greater than 50% and the p-value of test of the overall effect of Z was found to be > 0.05 in all those parameters. So a meta-analysis could only be done for the outcome parameter of pain. Pooling the data of the two studies revealed that PT intervention for CD patients as an add-on therapy had a significant positive effect on pain measured by the TWSTR pain scale (-5.00, 95% CI -6.26, -3.74) (Fig. 2).

Forest plot of meta-analysis of the effect of physiotherapy on TWSTRS pain score
Discussion
Given the progress in the field since the previous literature review in 2014, new emerging evidence on the effectiveness of PT for cervical dystonia has been published. An update of the knowledge was therefore warranted. Of the 14 articles included, 8 were RCTs. The literature shows that PT has a beneficial effect on different outcomes such as pain, disability, and disease severity. The effect on QoL is conflicting.
The finding of the meta-analysis revealed a positive effect of PT for reducing pain. BoNT in itself is beneficial on different outcomes such as pain and disease severity [11]. However, when PT is added to BoNT interventions, the pooled findings of two studies [24, 25] showed a reduction in pain (-5.00, 95% CI -6.26, -3.74) in groups receiving multimodal PT intervention with BoNT compared to BoNT alone. Pain reduction was reported in all included studies so we recommend physical therapy additional to BoNT for pain reduction in patients with CD. A 6 week PT intervention results in decreased pain and disease severity which correlated to enhanced sensorimotor plasticity. This was reported in the study of Hu et al. [28] in CD and previously in patients with writers’ cramp [38]. The central changes following physical therapy may account for the improvement in motor function and reduction of pain [39]. But the working mechanism need to be further explored.
Regarding the effect of physical therapy on disease severity and disability and quality of life, improvements are reported in 7 studies [24, 25, 30, 31, 34,35,36]. However, the heterogeneity between the studies was too high to pool the data so no firm recommendations can be made. Nevertheless, clinicians and patients might expect improvements in disease severity and disability following a physical therapy program.
A broad variety of PT intervention modalities were used in the included studies. Two studies used active exercises exclusively with relaxation therapy and motor relearning exercises [26, 33], 2 studies solely applied kinesiotape [29, 32], and 10 used combined modalities [24, 25, 27, 28, 30, 31, 34,35,36,37]. The PT program used by Tassorelli et al., included passive myofascial elongation manoeuvres, deep massage of cervical muscle, biofeedback training, and active stretching of muscles, tendons, and ligaments [24]. The main PT techniques by Werner et al. consisted of passive and active mobilization of the cervical spine and shoulder girdle, feedback exercises, perception and coordination training, posture training, and relaxation [25]. In one RCT of Hu et al., subjects were trained to perform a 6 week home exercise program after one supervised PT session [28]. These home exercises resulted in a 30% reduction of the TWSTRS score, indicating the benefits of exercising at home, or the possible use of telemedicine in CD. In the studies by Counsell et al. and Van den Dool et al., standard PT interventions were compared to a specialized PT program [27, 31] with no clear favorable outcome for the specialized interventions. Despite the large variability in intervention modalities in the intervention group, patients receiving PT were positively favoured over the control group. In line with this, existing evidence highlighted the modulating effect of exercise on abnormal movement patterns in healthy adults and neurological disorders [39, 40]. However, there is a lack of insight in dystonia.
Two RCTs reported pain reduction after applying KinesioTape [29, 32]. This effect was studied on short term (2–4 weeks) and may be attributed to changes in somatosensory temporal discrimination [29]. Applying tape did not have an impact on disease severity so it seems that active exercises are necessary to obtain these changes.
The findings of this literature review are in line with the previous review of 2014 but with higher quality studies included, enabling a meta-analysis. The findings are also in line with the review of Loudovici-Krug [41], which included 6 RCTs of 2 databases. The current review is a more comprehensive review including 8 RCTs with a more comprehensive overview of the effect of PT on several disease outcomes such as pain, disability, severity, and quality of life.
Based on the findings in this review, we cannot state the difference in effect size of PT alone compared to BoNT alone. BoNT alone has beneficial effects on pain and disease severity [11]. When combined with PT, the reduction in pain, disease severity and disability is even larger, based on our results. But to our knowledge, no research is available comparing the effect of BoNT alone to PT alone as BoNT is the first treatment of choice.
Implications for future research
The diverse nature of the comparison groups in the care they were receiving did not allow the reviewers to quantify the impact of PT on the outcomes such as TWSTRS total, disability, severity, and QoL. Thus, there is a need for further high-quality RCTs with a large study population that considers the comparison of PT with BoNT and BoNT alone. Up to now, it is unclear how long PT interventions should last before reaching optimal effect on neuroplasticity and lead to optimal treatment outcome for patients. Further fundamental research might address the underlying mechanisms in the sensorimotor network.
Implications for clinical practice
Various PT intervention modalities with different duration and frequencies were used in included studies. All studies showed a decrease in pain intensity. A clear recommendation of a specific type of PT as a favourable therapeutic intervention in the clinical setup cannot be made but multimodal interventions show effect on multiple outcome parameters.
Strengths and limitations of the review
As strength, the methodological quality of included articles was assessed independently by two reviewers. Furthermore, a meta-analysis was done with strict inclusion criteria.
As a review limitation, we searched articles published in the English language from three databases only. Three articles reported the outcome parameter of interest in a different way and were excluded in some of the outcome analysis. Furthermore, the limited number of primary studies with heterogeneous findings did not allow to perform meta-analysis for all outcome measures.
Conclusions
We recommend physical therapy interventions additional to BoNT for improving pain in patients with cervical dystonia. Patients might expect improvements in disease severity, disability and QoL.
Overall, the current review findings indicate beneficial effects of PT in reducing disease severity, disability, pain, and improving patient QoL. The meta-analysis also showed the statistically significant positive effect of PT in reducing TWSTRS pain scores. However, there is a lack of evidence to recommend the preferred type of PT, its duration, and frequency.
Given the variety of PT modalities used, no clear recommendation can be formulated on the best possible practice. Thus, there is a need to conduct additional RCTs before making a clear recommendation on the content of the therapy.
Protocol registration
This review protocol was registered in PROSPERO with the number CRD42022376433.
Data availability
All data generated and analyzed during this review are included in this manuscript.
References
Albanese A, et al. Phenomenology and classification of dystonia: a consensus update. Mov Disord. 2013;28(7):863–73.
Defazio G. The epidemiology of primary dystonia: current evidence and perspectives. Eur J Neurol. 2010;17(Suppl 1):9–14.
Defazio G, et al. Descriptive epidemiology of cervical dystonia. Tremor and Other Hyperkinetic Movements; 2013. p. 3.
Tomic S, et al. Cervical dystonia and quality of life. Acta Neurol Belgica. 2016;116(4):589–92.
Page D, Butler A, Jahanshahi M. Quality of life in focal, segmental, and generalized dystonia. Mov Disorders: Official J Mov Disorder Soc. 2007;22(3):341–7.
De Pauw J, et al. Measuring disability in patients with cervical dystonia according to the international classification of functioning, disability and health. OTJR: Occupation Participation and Health. 2017;37(3):132–40.
Amlang CJ, et al. Contributions of visual and motor signals in cervical dystonia. Brain. 2017;140(1):e4–e4.
Bradnam L, et al. Reduced vision-related quality of life in people living with dystonia. Disabil Rehabil. 2020;42(11):1556–60.
Molho ES, et al. Effect of cervical dystonia on employment: a retrospective analysis of the ability of treatment to restore premorbid employment status. Mov Disorders: Official J Mov Disorder Soc. 2009;24(9):1384–7.
Queiroz MR, Chien HF, Barbosa ER. Quality of life in individuals with cervical dystonia before botulinum toxin injection in a Brazilian tertiary care hospital. Arq Neuropsiquiatr. 2011;69:900–4.
Castelao M et al. Botulinum toxin type A therapy for cervical dystonia. Cochrane Database of Systematic Reviews, 2017(12).
Burbaud P, et al. Botulinum toxin treatment in neurological practice: how much does it really cost? A prospective cost-effectiveness study. J Neurol. 2011;258(9):1670–5.
Albanese A, et al. A systematic review on the diagnosis and treatment of primary (idiopathic) dystonia and dystonia plus syndromes: report of an EFNS/MDS-ES Task Force. Eur J Neurol. 2006;13(5):433–44.
Cacciola F, et al. Bilateral deep brain stimulation for cervical dystonia: long-term outcome in a series of 10 patients. Neurosurgery. 2010;67(4):957–63.
Skogseid I, et al. Good long-term efficacy of pallidal stimulation in cervical dystonia: a prospective, observer‐blinded study. Eur J Neurol. 2012;19(4):610–5.
Albanese A, et al. EFNS guidelines on diagnosis and treatment of primary dystonias. Eur J Neurol. 2011;18(1):5–18.
De Pauw J, et al. The effectiveness of physiotherapy for cervical dystonia: a systematic literature review. J Neurol. 2014;261(10):1857–65.
Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Reviews. 2021;10(1):1–11.
Ouzzani M, et al. Rayyan—a web and mobile app for systematic reviews. Syst Reviews. 2016;5:1–10.
Higgins JP, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2019.
Higgins JP et al. Assessing risk of bias in a randomized trial Cochrane handbook for systematic reviews of interventions, 2019: p. 205–228.
Institute JB. Critical Appraisal tools for use in JBI systematic reviews. Adelaide (AU): JBI; 2017.
Higgins JP, Green S, Scholten R. Maintaining reviews: updates, amendments and feedback Cochrane handbook for systematic reviews of interventions, 2008: p. 31.
Tassorelli C, et al. Botulinum toxin and neuromotor rehabilitation: an integrated approach to idiopathic cervical dystonia. Mov Disorders: Official J Mov Disorder Soc. 2006;21(12):2240–3.
Werner C, et al. Effects of a 3-month physiotherapy intervention in stable cervical dystonia as add-on to botulinum toxin therapy. Phys Medizin Rehabilitationsmedizin Kurortmedizin. 2019;29(01):53–7.
Boyce MJ, et al. Active exercise for individuals with cervical dystonia: a pilot randomized controlled trial. Clin Rehabil. 2013;27(3):226–35.
Counsell C, et al. A randomized trial of specialized versus standard neck physiotherapy in cervical dystonia. Parkinsonism Relat Disord. 2016;23:72–9.
Hu W, et al. A randomized study of botulinum toxin versus botulinum toxin plus physical therapy for treatment of cervical dystonia. Parkinsonism Relat Disord. 2019;63:195–8.
Pelosin E, et al. Kinesiotaping reduces pain and modulates sensory function in patients with focal dystonia: a randomized crossover pilot study. Neurorehabilit Neural Repair. 2013;27(8):722–31.
Stanković I, et al. The effect of physical therapy in the treatment of patients with cervical dystonia with or without concomitant use of botulinum toxin. Vojnosanit Pregl. 2018;75(10):1035–40.
van den Dool J et al. Long-term Specialized Physical Therapy in Cervical Dystonia. 2019.
Dec-Ćwiek M, et al. KinesioTaping after botulinum toxin type A for cervical dystonia in adult patients. Brain and Behavior. 2022;12(4):e2541.
Isabel Useros-Olmo A, Martínez-Pernía D, Huepe D. The effects of a relaxation program featuring aquatic therapy and autogenic training among people with cervical dystonia (a pilot study) Physiotherapy theory and practice, 2020. 36(4): p. 488–497.
Queiroz MAR, et al. Physical therapy program for cervical dystonia: a study of 20 cases. Funct Neurol. 2012;27(3):187.
Smania N, et al. The effect of two different rehabilitation treatments in cervical dystonia: preliminary results in four patients. Funct Neurol. 2003;18(4):219–26.
Zetterberg L, et al. Physiotherapy in cervical dystonia: six experimental single-case studies. Physiother Theory Pract. 2008;24(4):275–90.
Castagna A, et al. Sensorimotor Perceptive Rehabilitation Integrated (SPRInt) program: exercises with augmented movement feedback associated to botulinum neurotoxin in idiopathic cervical dystonia—an observational study. Neurol Sci. 2020;41:131–8.
Bleton JP, et al. Somatosensory cortical remodelling after rehabilitation and clinical benefit of in writer’s cramp. J Neurol Neurosurg Psychiatry. 2011;82(5):574–7.
Jensen JL, Marstrand PC, Nielsen JB. Motor skill training and strength training are associated with different plastic changes in the central nervous system. J Appl Physiol. 2005;99(4):1558–68.
Tajiri N, et al. Exercise exerts neuroprotective effects on Parkinson’s Disease model of rats. Brain Res. 2010;1310:200–7.
Loudovici-Krug D, et al. Physiotherapy for cervical dystonia: a systematic review of Randomised controlled trials. Toxins. 2022;14(11):784.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
SG and JDP did the literature search, study quality assessment, and data extraction. SG performed the statistical analysis, SG and JDP drafted the tables and figures. SG wrote the first draft of this analysis; JDP, WDH, CD, and EKG revised the manuscript. JDP helped to finish the final version. All authors approved the conclusions of our study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The author(s) declared no potential competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kassaye, S.G., De Hertogh, W., Crosiers, D. et al. The effectiveness of physiotherapy for patients with isolated cervical dystonia: an updated systematic review and meta-analysis. BMC Neurol 24, 53 (2024). https://doi.org/10.1186/s12883-023-03473-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03473-3