
Abstract
Background
Miller Fisher syndrome (MFS) is a subtype of Guillain-Barré syndrome (GBS) which is characterized by the three components of ophthalmoplegia, ataxia, and areflexia. Some studies reported MFS as an adverse effect of the COVID-19 vaccination. We aimed to have a detailed evaluation on demographic, clinical, and para-clinical characteristics of subjects with MFS after receiving COVID-19 vaccines.
Materials and methods
A thorough search strategy was designed, and PubMed, Web of Science, and Embase were searched to find relevant articles. Each screening step was done by twice, and in case of disagreement, another author was consulted. Data on different characteristics of the patients and types of the vaccines were extracted. The risk of bias of the studies was assessed using Joanna Briggs Institute (JBI) tools.
Results
In this study, 15 patients were identified from 15 case studies. The median age of the patients was 64, ranging from 24 to 84 years. Ten patients (66.6%) were men and Pfizer made up 46.7% of the injected vaccines. The median time from vaccination to symptoms onset was 14 days and varied from 7 to 35 days. Furthermore,14 patients had ocular signs, and 78.3% (11/14) of ocular manifestations were bilateral. Among neurological conditions, other than MFS triad, facial weakness or facial nerve palsy was the most frequently reported side effect that was in seven (46.7%) subjects. Intravenous immunoglobulin (IVIg) was the most frequently used treatment (13/15, 86.7%). Six patients received 0.4 g/kg and the four had 2 g/kg. Patients stayed at the hospital from five to 51 days. No fatal outcomes were reported. Finally, 40.0% (4/15) of patients completely recovered, and the rest experienced improvement.
Conclusion
MFS after COVID-19 immunization has favorable outcomes and good prognosis. However, long interval from disease presentation to treatment in some studies indicates that more attention should be paid to MFS as the adverse effect of the vaccination. Due to the challenging diagnosis, MFS must be considered in list of the differential diagnosis in patients with a history of recent COVID-19 vaccination and any of the ocular complaints, ataxia, or loss of reflexes, specially for male patients in their 60s and 70s.
Similar content being viewed by others


Introduction
Miller-Fisher syndrome (MFS) is a variant of Guillain–Barré syndrome (GBS), which is presented as the clinical triad of ataxia, areflexia, and ophthalmoplegia [1]. About half of the patients might experience symptoms related to the cranial nerves involvement other than the oculomotor nerves [2]. Previous Campylobacter jejuni or Hemophilus influenza infections are reported to be associated with the MFS onset [3, 4]. MFS is previously reported to be a side effect of vaccine administration, which may occur from 5 to 21 days after immunization with pneumovax [5], influenza [6], and Diphtheria—Pertussis—Tetanus (DPT) vaccines [7]. The molecular mimicry of infective agents bearing the GQ1b epitope is a described pathogenic mechanism of the MFS [3]. Notably, foreign antigens are suggested to stimulate an abnormal immune response, which targets the gangliosides found in peripheral nerves [8].
By introducing COVID-19 vaccines in early 2021, mortality rates of the infection were significantly reduced [9]. However, some incidental neurological complications in subjects after receiving COVID-19 vaccines have been reported [10, 11]. Reactivation of herpes zoster, GBS, and acute disseminated encephalomyelitis are among the instances [12]. Importantly, the reporting rate of GBS after COVID-19 vaccination is shown to be significantly higher than the rates after other vaccinations [13].
Though several reports are available about patients experiencing MFS after COVID-19 immunization, the clinical and prognostic characteristics of the patients have not been systematically assessed. In the current study, we systematically investigated the literature reporting MFS manifestation after receiving the COVID-19 vaccines to provide detailed demographic, clinical, and para-clinical characteristics of these patients to aid healthcare providers in diagnosing MFS sooner and getting better outcomes.
Material and methods
Databases search
On January 14, 2023, we performed a thorough search using electronic medical subject headings (MeSH), Embase subject headings (Emtree), and free keywords in PubMed, Web of Science, and Embase to identify relevant studies. The three databases were searched using the following terms without language filter or publication date or type restrictions: "Miller Fisher syndrome", "Fisher syndrome", "Guillain-Barré Syndrome", "ophthalmoplegia", "oculomotor motility disorder", "ataxia", "areflexia", "cranial nerve diseases", "Acute Inflammatory Demyelinating Polyneuropathy", "COVID-19", "SARS-CoV-2", "COVID-19 vaccines", "ChAdOx1 nCoV-19", "2019-nCoV vaccine mRNA-1273", "Moderna vaccine", "BNT162 vaccine", "Pfizer and BioNTech vaccine", "Baiya SARS-CoV-2 VAX COVID-19 vaccine", "Sinovac COVID-19 vaccine", "Sinopharm", "AstraZeneca vaccine", and "Johnson and Johnson vaccine". The exact search strategy and the number of records are provided in a Supplemantary file. Furthermore, Google Scholar was searched manually on the same date to have a sensitive search. The reference lists of the selected articles were also systematically reviewed to further find the relevant articles.
The study was conducted according to PRISMA guidelines [14].
Final enrollment of studies
The titles and abstracts of the retrieved articles were curated twice by four researchers (D.A., F.A., A.S., and F.S.) independently. In case of disagreement, another author checked the articles. No automation tools were used to exclude or include the records in the process. For the final inclusion and exclusion, researchers independently screened the full texts of the articles that were included in the previous screening step twice. In case of disagreement, another author was consulted.
The following inclusion criteria applied to include the articles: having original data, reporting symptoms of MFS that appeared after a COVID-19 vaccine injection regardless of vaccine type, and providing adequate clinical details of the MFS diagnosis, disease manifestation and information about the patient that we could evaluate the syndrome from the article. Other types of literature (e.g., correspondence, reviews, letters to the editors, expert opinions), studies with original data that reported different subtypes of GBS, and studies with insufficient patient data were considered to be excluded from our study.
Full texts of final studies were thoroughly examined to assess the quality and the risk of bias, and extract the needed data. Three researchers independently extracted the data from the final eligible studies, with discrepancies checked by another researcher (D.A). No automation tools were used to obtain the information.
Data extraction and risk of bias assessment
We designed a data extraction form to collect the information related to the patients (e.g. age, gender, nationality, history of recent infection, history of COVID-19 infection, and history of non-infectious diseases), the injected vaccine details (e.g. the name of the vaccine and vaccine doses received before the symptom onset), the disease symptoms (e.g. signs and symptoms and abnormal laboratory or imaging findings), and the treatment (treatment regimen, time from symptom onset to treatment, duration of treatment, outcome, and duration from the onset to outcome or length of hospital stay). In the current study, we reported the outcome as two categories; complete recovery, if the researchers reported that the patient's symptoms were completely resolved at the time of the discharge or during follow-up; or improvement, if the researchers reported the patient as partially improved or stated improvement of the sign or symptoms with some remained adverse effects as the last provided information.
To assess the risk of bias and the quality of the included studies, we used the Joanna Briggs Institute (JBI) critical appraisal tools 2020 version for evaluating the included case reports [15] and the case series [16]. Detailed information about the tools and the institute can be sought elsewhere. In short, JBI is an organization providing assessment tools for different types of studies and aids in researching evidence-based medicine [17]. To include studies, case reports in this review had to fulfill at least six criteria out of 8, and the included case series fulfilled 8 out of 10 criteria.
Results
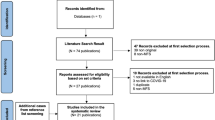
A total number of 4939 were retrieved. After removing 1551 duplicated records, titles and abstracts of 3388 articles were screened based on the criteria. After going through titles and abstracts, 190 records were sought for retrieval, and 169 records remained for the full-text assessment. Three studies reported a number of post-vaccination MFS cases. However, they were considered for exclusion due to the lack of information provided for patients. Other reasons for exclusion can be found in Fig. 1.

Flow chart of included studies with detailed exclusion reasons (PRISMA Flow Diagram)
In this study, after assessing the articles for eligibility, a total number of 15 subjects who developed MFS after receiving COVID-19 vaccines were included from 15 studies, including 14 case reports and one case series, each providing one patient with MFS [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. The median age of the patients was 64 years and ranging between 24 to 84 years. Both the oldest [26] and the youngest [18] patients were females (84 and 24-year-olds); however, most of the patients (66.6%) were men [19,20,21,22,23, 25, 27, 29, 31, 32]. Four cases (26.7%) were reported from Japan [20, 22, 29, 32] and four from the United States [21, 24, 25, 28]. Other cases were from Pakistan [31], South Korea [26], China [24], Australia [19], Croatia [18], Belgium [23], and Brazil [30]. The clinical and demographic characteristics of the patients are presented in Table 1 and the summary of provided data is shown in Table 2.
Most case reports fulfilled all 8 criteria, and most case series got 8 out of 10 questions. The details for each case report are provided in Table 3 and the case series are presented in Table 4.
Narrative synthesis
Pfizer made up 46.7% (7/15) of the injected vaccines [18, 20,21,22,23,24, 32]. The next most frequent vaccine received was Astra Zeneca, with 20.0% (3/15) patients [19, 26, 30]. Each of Sinovac [27, 31] and Johnson & Johnson injection [25, 28] were reported in two patients (13.3%), and in only one study with one patient Moderna was received [29]. Among the documented cases, eight patients had reported the syndrome onset after the first dose of vaccination (53.3%) [18, 19, 22, 23, 26, 28, 30, 31], and six patients with a second dose (40.0%) [20, 21, 24, 27, 29, 32]. The information was not provided in one case [25].
The median latency period from vaccination to symptoms onset was 14 days ranging from 7 to 35 days. More than half of the included studies (8/15, 53.3%) reported a duration between 11 and 20 days following the immunization to the onset of symptoms [18,19,20,21,22, 24, 25, 27]. While six of them (40.0%) reported less duration from vaccination to syndrome manifestation [26, 28,29,30,31,32], and only one study claimed it took 35 days [23].
Concerning the MFS triad assessment, only one study did not report any ocular complaint [30]. When evaluating the prevalence of different ocular manifestations of the syndrome, diplopia was the most frequent symptom, which affected 11 individuals (73.3%) [18,19,20,21, 23, 24, 26,27,28,29, 32]. Six studies (40.0%) reported restricted abduction or abducens nerve palsy [18, 23, 27,28,29, 31]. Ptosis was presented in four individuals (25%) [20, 22, 24, 26]. Three patients had abnormal pupil reflexes [20, 22, 24], and two patients reported being unable to completely close one or both eyes [27, 31]. Of these ocular signs, 78.3% (11/14) were bilateral [18, 19, 21, 22, 24,25,26,27,28,29, 32]. Moreover, 11 patients (73.3%) had ataxia [19, 21,22,23,24, 26, 27, 29,30,31,32], and reflexes were absent in nine (60.0%) [19, 21, 23, 26,27,28,29, 31, 32]. Eight patients (53.3%) had the complete triad of MFS [19, 21, 23, 26, 27, 29, 31, 32]. One or two features were absent in the rest.
Among other neurological conditions, facial weakness or facial nerve palsy was the most frequent complication that was reported in seven subjects [19, 25, 27,28,29,30,31]. Four patients had paresthesia [19, 21, 27, 31], and three had headaches [22, 27, 28]. Limb weakness [19, 30], nausea [24, 28], back pain [19, 28], and dizziness [27, 32] were each reported in two patients. One patient had dysarthria [25], and blood pressure fluctuation was diagnosed in one [24].
In terms of comorbidities and other medical conditions, four patients mentioned a medical history of hypertension (HTN) [24, 26, 29, 31], and three listed diabetes mellitus (DM) [20, 22, 23]. Importantly, one patient was admitted with flu [30], and one had positive testing for COVID-19 infection [21]. Other conditions were glaucoma and benign paroxysmal positional vertigo (BPPV) in one patient [20] and hyperuricemia and hyperlipidemia in another subject [29].
For paraclinical examinations, lumbar puncture (LP) was reported to be performed in all but one patient [30]. Albuminocytological dissociation was detected in 13 individuals [18,19,20,21,22,23,24,25,26,27,28, 30, 31], and one patient's LP analysis was normal [32]. Anti-Ganglioside Q1b (Anti-GQ1b) was positive in seven patients [18, 20, 24, 26, 27, 29, 32] and equivalent in one person [21]. The anti-GT1a [32], anti-GT1b [27], and anti-PCNA [18] were each positive in one patient.
Among the studies that reported the results of electromyography (EMG) or nerve conduction studies (NCS), abnormalities were reported in more than half (7/12, 58.3%) of studies [19, 24, 27,28,29,30,31]. In four cases (33.3%), abnormal F waves were observed [24, 28, 29, 31], that all were within the first ten days; at the time of admission [24], two [28], three [29], and ten days [31] after admission.
Thirteen patients underwent imaging, of which only four cases (30.7%) had modest abnormalities, including slight venous dilatation of the middle cerebral fossa in magnetic resonance imaging (MRI) [22], enhanced right oculomotor nerve [20], bilateral facial and oculomotor nerve in MRI [19], and Cauda equina enhancement [28].
Regarding the treatment, intravenous immunoglobulin (IVIg) was the most frequently used treatment (13/15) [18,19,20,21,22,23,24,25, 27,28,29,30, 32]. Six patients received 0.4 g/kg [20, 23, 24, 27, 30, 32], of five of them for five days (2g/kg as total dose) [20, 23, 24, 30, 32], and one patient for two days [27]. The four others had 2 g/kg [18, 19, 21, 28], three of them for five days (10g/kg as total dose) [18, 19, 21, 28], and one patient for two days [28]. Three studies did not report the dosage [22, 25, 29]. Besides IVIg, two patients also received steroids [18, 29] which were reported not to be effective in one patient [18]. Two patients had physiotherapy [30, 31], one received valacyclovir and mecobalamin [29], and one had daily acupuncture sessions [27]. One patient received pregabalin and physical therapy [29], whereas the other received no care [26]. Six patients completely benefited from the treatment, while the nine remaining only showed signs of improvement at the last session.
Hospital stays ranged in duration from 5 to 51 days, and the outcomes were assessed at the time of the discharge or during the follow-up, from the shortest three to 93 days after receiving the treatment, as the longest duration.
In terms of the prognosis, signs and symptoms of 40.0% (6/15) of patients were reported to be completely resolved at the last time of the follow-up. The rest (9/15, 60.0%) of patients improved and some of adverse effects were reported to be still present as the last record of the case. Although no fatal outcome was reported, it took some weeks [21, 27] and even one month [20, 22] for some patients to be diagnosed with MFS cases and get proper treatment.
Discussion
In this systematic review, we characterized 15 cases that developed MFS after receiving COVID-19 vaccination. The median age of patients was 64; most were male. East Asia made up the area with the most report. In most cases, the latency between receiving vaccines and symptoms onset was 11–20 days. Diplopia was the most frequent complaint, and ocular manifestations were bilateral rather than one-sided. IVIg was the most administered treatment regimen, with 0.4g/kg for five days. No fatal outcome was reported, and all subjects experienced improvement, with 40% being reported as having completely resolved signs and symptoms at the discharge or the last follow-up.
Importantly, in terms of the epidemiology, our results were consistent with the findings of the previous systematic review of post-COVID-19 infection MFS cases that most patients were middle-aged males [33]. Furthermore, in our study, the male:female ratio was 2:1, which is also in line with the previous works on MFS [2, 34].
In this review, Pfizer/BioNTech, an mRNA vaccine, was the most frequently reported vaccine, with seven out of 15 cases. Importantly, the rates of MFS after Pfizer, Johnson & Johnson, and Moderna in the United States are previously shown to be in the expected incidence range; therefore, there is a possibility that the type of vaccine does not make a significant difference [13]. However, it is noteworthy that vaccines of messenger RNA export spike proteins on the cell that provoke the production of antibodies and T-cell reactions [35]. Even though the current evidence is limited, it is suggested that these immunological changes may cause producing virus neutralizing as well as anti-GQ1b antibodies, therefore leading to neurological complications [20]. Importantly, the main suggested mechanisms by which COVID-19 vaccine triggers autoimmunity include molecular mimicry, the production of particular autoantibodies and the existence of certain vaccine adjuvants. The similarity between specific vaccine components and certain human proteins could trigger immune cross-reactivity and lead the immune system against pathogenic antigens to attack similar proteins in susceptible population [36]. In general, after mRNA vaccine injection, the ability to simultaneously activate the humoral and cellular immune systems may explain the side effects [37].
Among neurological signs and symptoms, other than the MFS triad, facial nerve palsy was the most common side effect, followed by dizziness, headache, myalgia, and paresthesia. Similar to our study, these signs and symptoms were reported as the most common neurologic side effects of the COVID-19 vaccines [12, 38]. GBS is also among the most common side effects of vaccines [39], which must be paid attention to when listing differential diagnoses in patients with neurological complaints and the history of a recent COVID-19 vaccination. Although GBS provides no absolute contraindication to receive COVID‐19 vaccines, it is suggested as an adverse event attributed to the vaccine, of which the likelihood of a causal link with vaccination should be determined through assessment along with getting detailed information about the complication and the severity of the condition [40].
MFS patients who present with limb weakness are considered MFS-GBS overlap syndromes [41,42,43]. Although no early predictors for progression from MFS to MFS-GBS overlap syndrome are provided, it is suggested that the transition occurs in the first week of the syndrome onset which warrants the need to carefully monitor MFS cases for at least the first week [43]. In our study, among 15 patients, two subjects reported limb weakness [19, 30]. Both improved and benefited from IVIg. Although the interval from symptom onset to the treatment of one patient was not provided [30], the other received treatment three days after the onset of the symptom [19]. Therefore, based on the current data of included studies and in line with previous reports, we support the benefit of early diagnosis and treatment of MFS to avoid further complications and progressive symptoms.
The cerebrospinal fluid (CSF) analysis is reported to be done in the MFS diagnosis, in which an increase in albuminocytological dissociation can be seen in 90% of patients [34]. However, this finding can not differentiate MFS from GBS [44]. In this study, and in line with previous studies [33, 34], 92.3% of patients showed albuminocytological dissociation in their CSF analysis, and only one study reported normal findings.
Treatment of MFS is generally supportive, using pain relievers and, if necessary, respiratory support. Alhough no randomized clinical trials have been performed for the MFS treatment, corticosteroids either orally or by injection have been reported not to be effective [33]. Similarly, in one patient of our study, before IVIg receiving, daily 500 mg of methylprednisolone showed no improvement, and subsequently, the patient went on IVIg therapy [18].
IVIg and plasmapheresis are effective treatments for severe MFS. No difference in the treatment outcomes is reported. However, the former is preferred for its convenience and fewer adverse effects [33]. In our review study, IVIg was administered to 86.6% of cases. All these patients experienced improvement mostly on the second day of the therapy. One patient did not receive treatment and exhibited improvement and a favorable outcome 30 days after the onset of the symptoms [26], and one had completely resolved symptoms only with pregabalin and physiotherapy [31].
Although among 15 patients, no death was reported, and all patients improved either partially or completely, the long duration from the onset to the treatment of some patients shows a challenging diagnosis. According to the current literature, the progressive nature of the syndrome and especially if the patient does not present with the classic triad, might make the diagnosis difficult and cause delay in receiving the proper treatment [34].
As mentioned earlier, simultaneous activation of the humoral and cellular immune systems following the injection of mRNA vaccines may cause MFS after vaccination [20, 35]. Another possible mechanism is the antibody cross-reaction [39]. Considering that COVID-19 vaccines induce immunization against the virus spike proteins, proteins might bind to sialic acid-containing glycoprotein and gangliosides on cell surfaces, which might explain a potential association [45]. Although MFS is reported that can be caused by COVID-19 infection [33], there is no solid evidence linking COVID-19 vaccination as a result of MFS exposure and demonstration. Furthermore, using case-centered and self-controlled case series analysis, Lee and colleagues rejected the proposed definitive and causal relationship between COVID-19 vaccination and the development of MFS [13]. One included study in this systematic review was a report of a COVID-19 vaccine clinical trial in which the side effects have also been observed in one subject of the placebo group [28]. Due to the design of the included studies, which are case reports and case series, we can not approve nor reject a potential casualty. However, regardless of the type of association, it is worth studying the characteristics of patients to provide better insight for clinicians and improve prognosis, as we did in this systematic review.
One of the limitations of our study is that several studies on patients with GBS did not address the subtype of the disease nor provide enough clinical features of GBS in each patient; therefore, we suggest that data on MFS cases are unavailable due to the lack of provided patients clinical characteristics. Furthermore, the currently available data on MFS cases after COVID-19 vaccination are reports of cases with no control group, and since the case–control studies are needed to get further information, In this review, we could not provide the incidence rate of the disease and compare it before and after COVID-19 vaccination.
To our knowledge, this review is the first systematic review studying demographic characteristics of patients with MFS after COVID-19 vaccination. Furthermore, we tried to provide details and clues based on current evidence to aid healthcare providers in the early diagnosis and treatment of patients with neurological manifestations and subsequently reduce its consequences and improve the quality of their lives.
Conclusion
According to our findings, MFS that occurred following SARS-Cov2 immunization is a neurological condition with a good prognosis and favorable outcomes. Male patients, especially in their 60s and 70s, who came with a history of previous COVID-19 vaccination and complaints of ophthalmoplegia, ataxia, and areflexia, should be better suspected for MFS. The MFS and its approach must be among the diseases at the top of the differential diagnosis list of a physician in order not to miss the opportunity to provide the patient with well-established treatment regimens, and to avoid the consequences of this disease progression. The exact cause of its occurrence has not been determined well, and underlying pathologies need to be further evaluated. However, based on up-to-date findings of other investigations it can be concluded that molecular mimicry and vaccine components and certain human proteins similarity might trigger this syndrome in susceptible population and the symptoms diminish following the reduction in anti-GQ1b antibody. Despite the above, vaccination should still be advocated because its risk–benefit ratio remains positive when compared to COVID-19 serious adverse events.
Availability of data and materials
Data could be available from the corresponding author upon reasonable reply.
Abbreviations
- MFS:
-
Miller-Fisher syndrome
- GBS:
-
Guillain–Barré syndrome
- DPT:
-
Diphtheria—Pertussis—Tetanus
- JBI:
-
Joanna Briggs Institute
- HTN:
-
Hypertension
- DM:
-
Diabetes mellitus
- LP:
-
Lumbar puncture
- EMG:
-
Electromyography
- NCS:
-
Nerve conduction studies
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- IVIg:
-
Intravenous immunoglobulin
- BPPV:
-
Benign paroxysmal positional vertigo
- IHD:
-
Ischemic heart disease
- MENA:
-
Middle East and North Africa
References
Fisher M. An unusual variant of acute idiopathic polyneuritis (syndrome of ophthalmoplegia, ataxia and areflexia). N Engl J Med. 1956;255(2):57–65.
Berlit P, Rakicky J. The Miller Fisher syndrome. Review of the literature. J Clin Neuro-ophthalmol. 1992;12(1):57–63.
Snyder LA, Rismondo V, Miller NR. The Fisher variant of Guillain-Barré syndrome (Fisher syndrome). J Neuroophthalmol. 2009;29(4):312–24.
Koga M, Yuki N, Tai T, Hirata K. Miller Fisher syndrome and Haemophilus influenzae infection. Neurology. 2001;57(4):686–91.
Thaler A. Miller Fisher syndrome in a 66-year-old female after flu and pneumovax vaccinations. J Am Med Dir Assoc. 2008;9(4):283–4.
Shoamanesh A, Chapman K, Traboulsee A. Postvaccination miller Fisher syndrome. Arch Neurol. 2011;68(10):1327–9.
Krämer HH, Niemöller U, Döring K, Fockenberg S, Kaps M, Nedelmann M. Postvaccination Miller Fisher syndrome after combined pertussis, diphtheria and tetanus toxoid vaccine. J Infect. 2013;66(5):460–1.
Yuki N, Hartung H-P. Guillain–barré syndrome. N Engl J Med. 2012;366(24):2294–304.
Jabłońska K, Aballéa S, Toumi M. The real-life impact of vaccination on COVID-19 mortality in Europe and Israel. Public Health. 2021;198:230–7.
Garg RA-O, Paliwal VA-O. Spectrum of neurological complications following COVID-19 vaccination. 2022;43(1):3–40. https://doi.org/10.1007/s10072-021-05662-9.
Patone M, Handunnetthi LA-O, Saatci D, Pan J, Katikireddi SA-O, Razvi SA-OX, et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. 2021;27(12):2144–53. https://doi.org/10.1038/s41591-021-01556-7.
Goss AL, Samudralwar RD, Das RR, Nath A. ANA Investigates: Neurological Complications of COVID-19 Vaccines. Ann Neurol. 2021;89(5):856–7.
Lee JR, Jaffry M, Mandava K, Rosario S, Elshourbagy T, Jaffry K, et al. Investigating the relationship of Miller Fisher Syndrome and COVID-19 Vaccination: A Vaccine Adverse Event Reporting (VAERS) Study (P4–9.001). Chicago: American Academy of Neurology; 2022.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Moola S MZ, Tufanaru C, Aromataris E, Sears K, Sfetcu R, Currie M, Qureshi R, Mattis P, Lisy K, Mu P-F. Systematic reviews of etiology and risk. In: Aromataris E MZ, editor. JBI Manual for Evidence Synthesis: JBI. Adelaide: Faculty of Health and Medical Sciences; 2020.
Munn Z BT, Moola S, Tufanaru C, Stern C, McArthur A, Stephenson M, Aromataris E. Methodological quality of case series studies. JBI Evidence Synthesis. 2020;18(10):2127–33. https://doi.org/10.11124/JBISRIR-D-19-00099
CRITICAL APPRAISAL TOOLS: Joanna Briggs Institute; [Available from: https://jbi.global/critical-appraisal-tools.
Abičić A, Adamec I, Habek M. Miller Fisher syndrome following Pfizer COVID-19 vaccine. Neurol Sci. 2022;43(3):1495-7. https://doi.org/10.1007/s10072-021-05776-0.
Dang YL, Bryson A. Miller-Fisher syndrome and Guillain-Barre syndrome overlap syndrome in a patient post Oxford-AstraZeneca SARS-CoV-2 vaccination. BMJ Case Reports CP. 2021;14(11):e246701.
Kubota T, Hasegawa T, Ikeda K, Aoki M. Case Report: Isolated, unilateral oculomotor palsy with anti-GQ1b antibody following COVID-19 vaccination. F1000Res. 2021;10:1142. https://doi.org/10.12688/f1000research.74299.2.
Michaelson NM, Lam T, Malhotra A, Schiff ND, MacGowan DJL. Miller Fisher syndrome presenting after a second dose of Pfizer-BioNTech vaccination in a patient with resolved COVID-19: a case report. J Clin Neuromuscul Dis. 2021;23(2):113–5.
Nishiguchi Y, Matsuyama H, Maeda K, Shindo A, Tomimoto H. Miller Fisher syndrome following BNT162b2 mRNA coronavirus 2019 vaccination. BMC Neurol. 2021;21:1–6.
Sansen PY, Calaras E, Weynants N, Glorieux P. Miller-Fisher Syndrome following the first dose of Comirnaty (Pfizer COVID-19 vaccination). J Med Case Rep Case Series. 2021;2:16.
Chen B, Lopez S, Eggenberger E. Miller Fisher syndrome after Pfizer BioNTech vaccine booster responsive to intravenous Ig treatment. BMJ Case Rep. 2022;15(11):e251361. https://doi.org/10.1136/bcr-2022-251361.
Kaur N, Mayo M, Torres M. 228: Miller-Fisher syndrome and Covid vaccination. Crit Care Med. 2022;50(1):99.
Kim JE, Min YG, Shin JY, Kwon YN, Bae JS, Sung JJ, Hong YH. Guillain-Barré Syndrome and Variants Following COVID-19 Vaccination: Report of 13 Cases. Front Neurol. 2022;12:820723. https://doi.org/10.3389/fneur.2021.820723.
Liang H, Cao Y, Zhong W, Ma Z, Liu J, Chen H. Miller-Fisher syndrome and Guillain-Barre syndrome overlap syndrome following inactivated COVID-19 vaccine: case report and scope review. Hum Vaccin Immunother. 2022;18(6):2125753.
Loza AMM, Holroyd KB, Johnson SA, Pilgrim DM, Amato AA. Guillain-Barré syndrome in the placebo and active arms of a COVID-19 vaccine clinical trial: temporal associations do not imply causality. Neurology. 2021;96(22):1052–4.
Nanatsue K, Takahashi M, Itaya S, Abe K, Inaba A. A case of Miller Fisher syndrome with delayed onset peripheral facial nerve palsy after COVID-19 vaccination: a case report. BMC Neurol. 2022;22(1):309.
Pirola FJC, Santos BAM, Sapienza GF, Cetrangolo LY, Geranutti CHWG, de Aguiar PHP. Miller-Fisher syndrome after first dose of Oxford/AstraZeneca coronavirus disease 2019 vaccine: a case report. J Med Case Reports. 2022;16(1):437.
Siddiqi AR, Khan T, Tahir MJ, Asghar MS, Islam MS, Yousaf Z. Miller Fisher syndrome after COVID-19 vaccination: case report and review of literature. Medicine. 2022;101(20):e29333.
Yamakawa M, Nakahara K, Nakanishi T, Nomura T, Ueda M. Miller Fisher syndrome following vaccination against SARS-CoV-2. Intern Med. 2022;61(7):1067–9.
Li Z, Li X, Shen J, Chan MTV, Wu WKK. Miller Fisher syndrome associated with COVID-19: an up-to-date systematic review. Environ Sci Pollut Res Int. 2021;28(17):20939–44.
Rocha Cabrero F ME. Miller Fisher Syndrome: Treasure Island (FL): StatPearls; Publishing; 2022 [Cited 10 Feb 2023]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507717/.
Sahin U, Muik A, Derhovanessian E, Vogler I, Kranz LM, Vormehr M, et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature. 2020;586(7830):594–9.
Chen Y, Xu Z, Wang P, Li XM, Shuai ZW, Ye DQ, et al. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology. 2022;165(4):386–401.
Sadarangani M, Marchant A, Kollmann TR. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat Rev Immunol. 2021;21(8):475–84.
Finsterer J, Scorza FA. Neurological Side Effects of SARS-CoV-2 Vaccinations are Not Uncommon but Frequently Ignored [Letter]. Neuropsychiatr Dis Treat. 2022;18:1273–5.
Finsterer J. Neurological side effects of SARS-CoV-2 vaccinations. Acta Neurol Scand. 2022;145(1):5–9.
COVID-19 vaccine contraindications and precautions: Autralian Government Department of Health and Aged Care; [Updated 1 Dec 2022. Available from: https://www.health.gov.au/our-work/covid-19-vaccines/advice-for-providers/clinical-guidance/contraindications-and-precautions.
Sekiguchi Y, Mori M, Misawa S, Sawai S, Yuki N, Beppu M, et al. How often and when Fisher syndrome is overlapped by Guillain-Barré syndrome or Bickerstaff brainstem encephalitis? Eur J Neurol. 2016;23(6):1058–63.
Funakoshi K, Kuwabara S, Odaka M, Hirata K, Yuki N. Clinical predictors of mechanical ventilation in Fisher/Guillain–Barré overlap syndrome. J Neurol Neurosurg Psychiatry. 2009;80(1):60–4.
Verboon C, van Berghem H, van Doorn PA, Ruts L, Jacobs BC. Prediction of disease progression in Miller Fisher and overlap syndromes. J Peripher Nerv Syst. 2017;22(4):446–50.
Arányi Z, Kovács T, Sipos I, Bereczki D. Miller Fisher syndrome: brief overview and update with a focus on electrophysiological findings. Eur J Neurol. 2012;19(1):15-e3.
Sun X-L. The role of cell surface sialic acids for SARS-CoV-2 infection. Glycobiology. 2021;31(10):1245–53.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
D.A., N.S., A.H.L. and N.R. conceptualized the study. D.A. and A.H.L.participated in the search strategy and the research design of the systematic review. D.A., A.S., F.A., and F.S. did the articles screening of title, abstract, and full text and data extraction. Any disagreements were resolved by consulting with a third reviewer (A.H.L., N.S., and N.R.). D.A., A.S., F.A., and F.S. drafted the manuscript. D.A., N.S., A.H.L., and N.R. critically revised the manuscript for important intellectual content, and approved the final version to be published. N.R. supervised the study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alijanzadeh, D., Soltani, A., Afra, F. et al. Clinical characteristics and prognosis of temporary miller fisher syndrome following COVID-19 vaccination: a systematic review of case studies. BMC Neurol 23, 332 (2023). https://doi.org/10.1186/s12883-023-03375-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03375-4