
Abstract
Background
Visual dysfunction have been well reported as one of the non-motor symptoms in Parkinson’s disease (PD). The aim of this study was to evaluate the functional and structural changes in the retina in patients with PD, and to correlate these changes with disease duration and motor dysfunction.
Methods
For this case–control study, we recruited patients fulfilling the diagnostic criteria for idiopathic PD according to British Brain Bank criteria, aged between 50 and 80 years. Age- and sex-matched healthy controls aged between 50 and 80 years were also recruited. Motor function for PD patients was assessed using Modified Hoehn and Yahr staging scale (H & Y staging) and Unified Parkinson’s Disease Rating Scale (UPDRS). Optical Coherence Tomography (OCT) and full field electroretinogram (ff-ERG) were done to all participants.
Results
Data from 50 patients and 50 healthy controls were included in the analysis. Patients with idiopathic Parkinson's had significantly reduced peripapillary retinal nerve fiber layer (RNFL) thickness and macular ganglion cell complex (GCC) thickness compared to healthy controls (P-value < 0.05 in all parameters). They also had significantly delayed latency and reduced amplitude in both dark-adapted rods and the light-adapted cone for both a & b waves compared to healthy controls (P-value < 0.001 in all parameters). There were statistically significant negative correlations between disease duration, and left superior, right inferior and right & left average RNFL thickness [(r) coef. = -0.327, -0.301, -0.275, and -0.285 respectively]. UPDRS total score was negatively correlated with the amplitude of light-adapted of both RT and LT a & b wave and with dark-adapted RT b-wave latency [(r) coef. = -0.311, -0.395, -0.362, -0.419, and -0.342].
Conclusion
The retinal structure and function were significantly affected in patients with PD in comparison to healthy controls. There was a significant impact of disease duration on retinal thickness, and there was a significant negative correlation between the degree of motor dysfunction in patients with PD and retinal function.
Similar content being viewed by others

Introduction
Parkinson’s disease (PD) is the second most common neurodegenerative disorder affecting middle-aged and elderly people in the developed world [1]. Idiopathic PD is diagnosed based on medical history and a neurologic examination using movement Disorder Society‐Unified Parkinson's Disease Rating Scale (MDS‐UPDRS) [2]. It can take several years to get a final conclusion due to heterogeneity of PD regarding the age of onset, clinical presentation, rate of progression [3]. As a result, the diagnosis process needs to be improved and expedited in the early stages of PD using new technologies [4]. The motor symptoms of PD, including bradykinesia, rigidity, resting tremor, and postural instability, are well-known. However, dopaminergic neuronal loss can also cause non-motor changes, such as anhedonia, dementia, and autonomic dysfunction [5]. In addition, a more diffuse pathology might be associated with the non-motor symptoms as well; the cholinergic glutamatergic, noradrenergic, and serotonergic systems [6].
One of the non-motor systems affected by PD is vision. Visual acuity, contrast sensitivity, ocular motility, and color perception are among the visual abnormalities associated with PD [7]. Such vision impairment in patients with PD seems to be caused by dysfunction of the intraretinal dopaminergic circuitry and final retinal output to the brain. The human retina has dopaminergic amacrine and interplexiform cells [8]. Through dopaminergic receptors, dopamine in the mammalian retina alters colour perception and contrast sensitivity (D1 and D2) [9]. Changes in signal dispersion, colour perception, and contrast sensitivity result from a complete loss of D1 and D2 receptor activation [9].
The retina is easily accessible for clinical examination and is a component of the central nervous system. Since the majority of the retinal ganglion cells (RGCs) axons are not myelinated, the retinal nerve fibre layer (RNFL) thickness measurements offer a relatively direct evaluation of the axons and axonal damage [10].
Optical coherence tomography (OCT) is a non-invasive imaging test that uses interference patterns created by low coherence light reflected from retinal tissues to obtain cross-sectional pictures of the retina and optic disc. This approach entails the creation of parameters that offer precise, impartial, and repeatable measurements of the various retinal layers [11]. Measures of specific layers, such the RGC layer, provide more precise information regarding axonal loss in neurodegenerative illnesses, according to recent study on segmentation and analysis of several retinal layers [11].
Electrophysiological studies such as visual evoked potential (VEP) can easily detect the subtle visual impairment that may develop in PD [12]. Electroretinogram (ERG) may also provide a simple tool to evaluate retinal dopaminergic mechanisms and contribute to the clinical assessment and monitoring of dopaminergic therapy [13].
As such, the aim of this study was to evaluate the functional and structural changes in the retina in patients with PD, and to see whether these changes correlate with disease duration and degree of motor dysfunction.
Methods
Study design
This case–control study was conducted on patients diagnosed with idiopathic PD and age- and sex-matched healthy controls. The patients were recruited from the Neurology outpatient clinic, Beni-Suef University Hospital, during the period from January 2021 to June 2022. Healthy controls were recruited from the patients’ relatives. The study was explained to all participants and written informed consent was obtained from them or their first-degree relatives before participation in the study. The study was ethically approved by Faculty of medicine, Beni Suef University Research Ethical Committee (FM-BSU REC). The approval number is FMBSUREC/06122020/ Mohammed. All methods were carried out in accordance with relevant guidelines and regulations.
Eligibility criteria
The study included patients fulfilling the criteria for diagnosis of Parkinson’s disease based on British Brain Bank criteria [14]. The age range was from 50–80.
Patients with the following conditions were excluded from this study: patients with secondary Parkinsonism (Drug-induced, post traumatic, or post infectious) or atypical Parkinsonism, patients having major neurocognitive disorder, patients with MRI brain showing structural lesion like multiple or extensive infarcts, severe white matter hyperintensity burden, intracerebral hemorrhage, subdural hematoma, tumors, encephalitis, or hydrocephalus, patients with significant refractive errors (> 5 diopters of spherical equivalent refraction or 3 diopters of astigmatism), intraocular pressure ≥ 21 mm Hg, media opacifications, ocular trauma, concomitant retinal or optic nerve pathology, and patient with any concomitant medical disorder known to affect the retina or optic nerve e.g. Hypertension (HTN), diabetes mellitus (DM) or autoimmune disorder.
Measures
Evaluation and staging of Parkinson’s disease using
Modified Hoehn and Yahr staging scale (H & Y staging) [15]
It provides an overall assessment of staging of Parkinson's disease based on clinical features and functional disability. Stage 0: no signs of disease, Stage 1.0: symptoms are very mild; unilateral involvement only, stage 1.5: unilateral and axial involvement, stage 2: bilateral involvement without impaired balance, stage 2.5: mild bilateral disease with recovery on pull test, stage 3: mild to moderate bilateral disease; some postural instability; physically independent, stage 4: severe disability; still able to walk or stand unassisted, and stage 5: wheelchair bound or bedridden unless aide.
Unified Parkinson’s Disease Rating Scale (UPDRS) [16]
It was used as a rating scale for assessment of PD patients included in our study (on medications). It objectively rates an individual patient’s disability at a particular moment in time. Its score is a reflection of disease burden on the individual patient and is useful in describing disease progression and treatment response with time. The UPDRS is scored from a total of 195 points; higher scores reflect marked disability. It is made up of the following sections: Part I: evaluation of cognition, behavior, and mood, Part II: self-evaluation of the activities of daily life, Part III: clinician-evaluation of motor function, part IV: complication of medical treatment, and part V: other complications.
Optical coherence tomography (OCT)
Retinal imaging was done using RTVue-OCT ‘Optovue’ (Optovue Inc.,Fremont, California, USA) device with a software version 2018.1.1.63. The RTVue-100 is one of the SD-OCT devices with a scan rate of 26000 A scans per second and an axial resolution of 5 pm, allowing fast cross-sectional imaging of the retinal microstructure at high resolution in a rapid, objective, reproducible manner. Optic nerve head (ONH) protocol and ganglion cell complex (GCC) protocols were used. Good quality images with a signal strength index (SS1) 250 were included. OCT images were obtained from both eyes of each patient (three images were obtained and the average was taken).
Optic nerve head (ONH) scan
The ONH protocol was used to obtain RNFL and ONH measurements. In the measurement of RNFL parameters, ONH protocol generates a polar RNFL thickness map from which RNFL thickness is measured along a circle 3.45 mm in diameter centered on the optic disc. Parameters including overall average, superior hemisphere, inferior hemisphere, temporal quadrant, superior quadrant, inferior quadrant, and nasal quadrant were provided [17].
Ganglion cell complex scan (GCC)
The GCC was used to obtain macular measurements. In the measurement of macular parameters, GCC protocol scans a 7 mm square region with 15 vertical lines at 0.55 mm intervals and 1 horizontal line. Macular B-scan evaluates macular total retinal (TR) measurement in two layers: GCC and outer retina OR layers. GCC is composed of ganglion cell layer, nevre fiber layer, and inner plexiform layer. GCC parameters including overall average thickness, superior thickness, inferior thickness, superior minus inferior thickness, global loss volume (GLV), and focal loss volume (FLV) are provided [17].
The eyes of all participants were dilated using mydriatic eye drops before image acquisition. Participants were instructed to fixate on an intrinsic fixation target during the process of OCT scanning. If the participant was not fixating well and the center of image was not on the center of the fovea, a manual adjustment was performed. All OCT scans were performed by the same experienced optometrist.
Full-field clinical electroretinography (ffERG)
The ffERG was performed at the Neuro Diagnostic & Research Center (NDRC), Beni-Suef Hospital, Egypt, using Roland consult electrophysiological diagnostic systems [utilizing Reti-Scan 21 (Roland Consult, Brandenburg a.d. Havel, Germany)]. The parameters for the Standard flash (ganzfeld) stimuli were revised to ISCEV guidelines [18] that specified six responses based on the adaptation state of the eye and the flash strength.
-
1.
Dark-adapted 0.01 ERG (a rod-driven response of on bipolar cells).
-
2.
Dark-adapted 3 ERG (combined responses arising from photoreceptors and bipolar cells of both the rod and cone systems; rod dominated).
-
3.
Dark-adapted 10 ERG (combined response with enhanced a-waves reflecting photoreceptor function).
-
4.
Dark-adapted oscillatory potentials (responses primarily from amacrine cells).
-
5.
Light-adapted 3 ERG (responses of the cone system; a-waves arise from cone photoreceptors and cone Off- bipolar cells; the b-wave comes from On- and Off-cone bipolar cells).
-
6.
Light-adapted 30 Hz flicker ERG (a sensitive cone-pathway-driven response) [18].
Statistical analysis
The data were coded and entered using: the statistical package for social science (SPSS) version 25 (Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). We used Kolmogorov–Smirnov test to check the normality of the quantitative variables. The data were presented using mean and standard deviation for quantitative data such as age, disease duration, H & Y staging, UPDRS, OCT, and ffERG parameters. Categorical variables such as sex and antiparkinsonian medications were presented as number and percent. Independent sample t- test was used for comparison between PD patients and controls in age, OCT, and ffERG parameters. Chi square test was for comparison between PD patients and controls in sex. The Pearson correlation coefficient (r) was used to correlate disease duration, H & Y staging, and UPDRS with OCT and ffERG parameters. The P-values were adjusted for multiple testing by performing the Benjamini–Hochberg procedure. P-value ≤ 0.05 was considered significant.
Results
Demographics and clinical characteristics of PD patients
This case–control study was conducted on 50 PD patients and 50 healthy controls. The mean value for age in PD patients was 60.36 ± 11.38 years, while the mean value for age in controls was 60.72 ± 11.79 years. There was no statistically significant difference between patients and controls regarding age (P-value = 0.77). As for sex, 68% (n = 34) of PD patients were males and 32% (n = 16) were females. As for controls, 64% (n = 32) were males and 36% (n = 18) were females. There was no statistically significant difference between patients and controls regarding sex (P-value = 0.673).
Regarding clinical characteristics of PD patients, the mean value for disease duration was 3.64 ± 2.32 years, for H&Y staging was 2.59 ± 0.81, and for UPDRS total score was 33.44 ± 15.12 (Table 1).
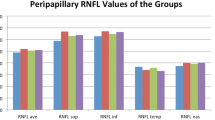
Reduced peripapillary RNFL thickness in PD patients
The peripapillary RNFL thickness (superior, inferior & average) on both sides were all significantly reduced in PD patients compared to healthy controls (P-value < 0.001, < 0.001, < 0.001, < 0.001, 0.003, < 0.001 respectively) (Table 2, Fig. 1).

RNFL& GCC thickness in PD patients and controls GCC: ganglion cell complex, PD: Parkinson's disease, RNFL: Retinal nerve fiber layer
The macular ganglion cell complex (GCC) thickness was significantly reduced in PD patients compared to healthy controls regarding right (RT) eye (P- value = 0.02), whereas, it was insignificantly reduced regarding left (LT) eye (P-value = 0.09) (Table 2, Fig. 1).
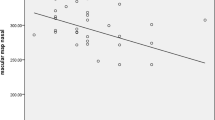
There were statistically significant negative correlations between disease duration, and LT superior (r. coef. = -0.327, P-value = 0.02), RT inferior (r. coef. = -0.301, P-value = 0.034), and RT average (r. coef. = -0.275, P-value = 0.054), and LT average RNFL thickness (r. coef. = -0.285, P-value = 0.045) (Table 3, Figs. 2, 3, 4 and 5).

Correlations between disease duration and left superior RNFL thickness. RNFL: Retinal nerve fiber layer

Correlations between disease duration and right inferior RNFL thickness. RNFL: Retinal nerve fiber layer

Correlations between disease duration and right average RNFL thickness. RNFL: Retinal nerve fiber layer

Correlations between disease duration and left average RNFL thickness. RNFL: Retinal nerve fiber layer
There were no statistically significant correlations between either H&Y staging or UPDRS, and OCT parameters including RNFL and GCC thickness (P-values > 0.05) (Table 4).
Delayed latency and reduced amplitude in both dark-adapted rods and the light-adapted cone for both a & b waves in PD patients
The dark-adapted rods a & b wave responses showed significantly delayed latency in PD patients as compared to healthy controls, (P- value < 0.001 in all comparisons). At the same time, amplitudes for a and b waves were significantly lower in PD patients as compared to healthy controls (P- value < 0.001 in all parameters) (Table 5).
The light adapted cone a and b waves response showed significantly delayed latency in PD patients as compared to healthy controls, (p-values < 0.001). At the same time, amplitudes for a and b waves were significantly lower in the PD patients as compared to healthy controls (p-values < 0.001) (Table 5).
There were no statistically significant correlations between disease duration and either photopic or scotopic ERG parameters (P-values > 0.05) (Table 6).
There were no statistically significant correlations between H&Y staging and either light adapted or dark-adapted ERG parameters (P-values > 0.05). However, UPDRS showed a statistically significant negative correlation with the amplitude of light-adapted of both a & b wave UPDRS total score was negatively correlated with the amplitude of light-adapted of both RT and LT a & b wave [(r. coef. = -0.311, P-value = 0.028), (r. coef. = -0.395, P-value = 0.005), (r. coef. = -0.362, P-value = 0.011), (r. coef. = -0.419, P-value = 0.002) respectively] and with dark-adapted RT b-wave latency (r. coef = -0.342, P-values = 0.015). There were no statistically significant correlations between total UPDRS and the other ff-ERG values (P-values > 0.05) (Table 7).
Discussion
The current study revealed that the retinal structure and function were significantly affected in patients with PD in comparison to healthy controls. The retinal changes observed were significantly correlated with the disease duration and the degree of motor dysfunction.
Clearly, the superior, inferior, and average peripapillary RNFL thickness in the included PD patients in this study were significantly reduced compared to the healthy controls. These findings are in line with those of Satue et al., 2013 [19] who showed significant reduction in the inferior, inferotemporal and superotemporal RNFL thicknesses in a large sample size of 100 PD patients compared to 100 healthy controls using SD-OCT.
Moreover, Moschos MM et al., 2018 [20] observed a significant reduction in the average RNFL thickness as well as average GCC thickness in PD patients compared to controls. The same findings were also obtained by Ascaso F et al., 2013 and Pilat A et al., 2016 [21, 22]. The main explanation for these findings is fact that neurodegeneration in PD is not restricted to the brain, but also occurs in the retina [23].
On the contrary, several studies have shown non-significant differences in RNFL thickness between PD and healthy control [24, 25].
Regarding, macular GCC, the current study revealed a significant reduction in GCC thickness (in one eye but not in the other eye) in patients with PD compared to healthy controls. Other studies which used segmentation analysis, also observed a significant thinning of the GCL in patients with PD compared to healthy controls [26, 27].
The reported significant reduction in GCC in PD patients may be attributed to RNFL loss, which is suggested to produce consecutive degeneration of the RGC layer and its axons as the disease progresses [28, 29].
These conflicting results regarding the RNFL as well as GCC measurements in PD patients compared to healthy control may be attributed to difference in OCT equipment which can affect retinal measurements and to the differences in retinal segmentation algorithm [30].
With regard to disease duration, our study revealed that longer duration of the disease was associated with decreased RNFL thickness especially in LT superior, RT inferior and RT < average RNFL thickness. This agreed with a study conducted by Garcia-Martin et al. 2014 [31] which revealed that the inner retinal layer thicknesses was significantly thinner in PD patients with disease duration longer than 10 years compared to those with shorter disease duration. Also, El-Kattan, M.M et al., 2022 [23] reported in their study that retinal thickness inversely correlated with disease duration.
These results, therefore, reflect the presence of progressive degeneration in the retinal layers with disease progression and indicate that the neurodegenerative process runs in parallel in the brain and the retina in PD.
In contrast to our results, no abnormalities were observed in the OCT of PD patients in relation to disease duration in the study of Roth, N.M et al., 2014 [32].
In our study, we observed that there were no statistically significant correlations between the severity of motor symptoms assessed by H&Y staging and UPDRS, and OCT parameters including RNFL and GCC thickness.
Our findings were in agreement with Aydin, T.S et al., 2018 [33] who revealed non-significant correlations between structural parameters in the retina using OCT and the scores of either HY scale or UPDRS. Also, several studies showed the same findings [34, 35].
On the other hand, a previous study revealed that peripapillary RNFL as well as retinal and macular RNFL thicknesses were negatively correlated with H &Y [36]. Likewise, other studies reported an inverse correlation between the foveal thickness measured by TD-OCT and the UPDRS total and motor scores [37, 38]. These discrepant and equivocal data on the relationship between OCT measures and severity of motor symptoms in PD are likely to be explained by differences in the applied OCT devices and technologies.
Interestingly, Visser et al. and Lee et al. found in their studies that visual hallucinations in PD patients were associated with thinning of the inner retinal layers and, possibly, with reduced visual acuity. Lee et al. found a significant parafoveal inner nuclear layer thinning in PD patients in comparison to controls, whereas other retinal layers, including the retinal nerve fiber layer, as well as total macular thicknesses were not different. In contrast to our results, they didn’t find a significant correlation between retinal thicknesses and disease duration. The lack of correlation with disease duration was mostly attributed to the presence of early retinal involvement in PD patients due to retinal dopamine deficiency as well as deposition of abnormal alpha synuclein in the inner retinal layers. These pathological changes may cause RNFL thinning in recently diagnosed PD patients [39,40,41].
Regarding flash ERG, our study showed affection of both a and b waves. These were demonstrated in prolonged latencies and reduced amplitudes of the a and b waves of both dark-adapted and the light-adapted responses in PD patients compared to controls. This signifies dysfunction of both rod and cone photoreceptors as well as bipolar cells of the whole retina [42].
Similar to our findings, some studies showed significant reduction in ffERG amplitudes in PD patients relative to control groups [43,44,45]. Furthermore, delayed latencies of the cone or combined rod/cone ERG responses in PD patients has previously been demonstrated [41, 46, 47]. Interestingly, Barbara Nowacka et al., 2015 [46] found that ffERG changes can be detectable early in the course of the disease, even in the absence of structural retinal damage detected by OCT.
It is suggested that the reason for the susceptibility of pigment epithelial function to dopamine deficiency in Parkinson's disease may be related to its site being at the extremity away from dopamine release sites at the inner plexiform layer [41].
On the other hand, other studies have found no significant differences in ffERG latency and/or amplitude between PD patients and control [45, 48,49,50,51].
These contradictory results regarding ffERG in PD patients versus controls could be attributed to the different phenotypes, stages of PD patients and difference in disease duration, and whether the patients were on dopaminergic therapy or not.
Our study revealed that there were no statistically significant correlations between H&Y staging and either light adapted or dark-adapted ERG parameters. However, UPDRS showed statistically significant negative correlations with the amplitude of light-adapted of both a & b wave but didn’t show significant correlations with the other ffERG values.
These results come in agreement with previous studies which found that during PD, the reduced amplitudes of the photopic a and b waves were observed [43, 45].
The alterations in the retinal dopamine seem to be a primary factor coordinating shift from nighttime to daytime vision. Therefore, lower concentration of retinal dopamine in course of PD may cause disruption of the functional transition from a rod to cone dominated state [52]. This was observed as reduction in the photopic a and b-wave amplitude in the present study.
On the other hand, Mello, L. G. M. et al., 2022 [53] and Devos D et al., 2005 [49] found no statistically significant correlation between ffERG and clinical data.
The strength of our study was that it was the first study to correlate the combined structural–functional changes in the retina and optic nerve (assessed by OCT and ffERG) in patients with PD to the disease duration and the motor dysfunction. Such retinal changes may reflect the presence of dopaminergic dysfunction along the retinocortical pathway.
Conclusion
PD patients had significantly impaired retinal structure and function in comparison to healthy controls. The retinal thickness in PD patients was negatively correlated with disease duration. The amplitude of light-adapted of both a & b wave, and the dark-adapted b-wave latency in PD patients was significantly correlated with motor function.
Availability of data and materials
Authors report that the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
de Lau LM, Breteler MM. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006;5(6):525–35.
Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–70.
Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of Parkinson’s disease. Lancet Neurol. 2021;20(5):385–97.
Satue M, Polo V, Otin S, Larrosa J, Obis JF, Garcia-Martin E. Neuro-Ophthalmologic Evaluation as a Biomarker for Diagnosis and Progression in Parkinson Disease. 2016.
Chaudhuri KR, Schapira AH. Non-motor symptoms of Parkinson’s disease: dopaminergic pathophysiology and treatment. Lancet Neurol. 2009;8(5):464–74.
Brandão PRP, Munhoz RP, Grippe TC, Cardoso FEC, de Almeida ECBM, Titze-de-Almeida R, et al. Cognitive impairment in Parkinson’s disease: A clinical and pathophysiological overview. J Neurol Sci. 2020;419:117177.
Armstrong RA. Oculo-Visual Dysfunction in Parkinson’s Disease. J Parkinsons Dis. 2015;5(4):715–26.
Bodis-Wollner I. Retinopathy in Parkinson disease. J Neural Transm (Vienna). 2009;116(11):1493–501.
Polo V, Satue M, Rodrigo MJ, Otin S, Alarcia R, Bambo MP, Fuertes MI, Larrosa JM, Pablo LE, Garcia-Martin E. Visual dysfunction and its correlation with retinal changes in patients with Parkinson's disease: an observational cross-sectional study. BMJ Open. 2016;6(5):e009658. https://doi.org/10.1136/bmjopen-2015-009658.
Garcia-Martin E, Satue M, Otin S, Fuertes I, Alarcia R, Larrosa JM, et al. Retina measurements for diagnosis of Parkinson Disease. Retina (Philadelphia, Pa). 2014;34(5):971–80.
Sakata LM, DeLeon-Ortega J, Sakata V, Girkin CA. Optical coherence tomography of the retina and optic nerve–a review. Clin Experiment Ophthalmol. 2009;37(1):90–9.
He SB, Liu CY, Chen LD, Ye ZN, Zhang YP, Tang WG, et al. Meta-analysis of visual evoked potential and Parkinson’s Disease. Parkinsons Dis. 2018;2018:3201308.
Tagliati M, Bodis-Wollner I, Yahr MD. The pattern electroretinogram in Parkinson’s disease reveals lack of retinal spatial tuning. Electroencephalogr Clin Neurophysiol. 1996;100(1):1–11.
Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J Neurol Neurosurg Psychiatry. 1988;51(6):745–52.
Goetz CG, Poewe W, Rascol O, Sampaio C, Stebbins GT, Counsell C, Giladi N, Holloway RG, Moore CG, Wenning GK, Yahr MD, Seidl L. Movement Disorder Society Task Force on Rating Scales for Parkinson's Disease. Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord. 2004;19(9):1020–8. https://doi.org/10.1002/mds.20213.
Fahn S, Elton RL; UPDRS program members. Unified Parkinsons Disease Rating Scale. In: Fahn S, Marsden CD, Goldstein M, Calne DB, editors. Recent developments in Parkinsons disease, vol 2. Florham Park: Macmillan Healthcare Information; 1987. p. 153–63.
Aydogan T, Akçay BİS, Kardeş E, Ergin A. Evaluation of spectral domain optical coherence tomography parameters in ocular hypertension, preperimetric, and early glaucoma. Indian J Ophthalmol. 2017;65(11):1143–50.
McCulloch DL, Marmor MF, Brigell MG, Hamilton R, Holder GE, Tzekov R, Bach M. ISCEV Standard for fullfield clinical electroretinography (2015 update). Doc Ophthalmol. 2015;130(1):1–12. https://doi.org/10.1007/s10633-014-9473-7. Epub 2014 Dec 14. Erratum in: Doc Ophthalmol. 2015;131(1):81–3.
Satue M, Garcia-Martin E, Fuertes I, Otin S, Alarcia R, Herrero R, et al. Use of Fourier-domain OCT to detect retinal nerve fiber layer degeneration in Parkinson’s disease patients. 2013;27(4):507–14.
Moschos MM, Chatziralli IP. Evaluation of Choroidal and Retinal Thickness Changes in Parkinson's Disease Using Spectral Domain Optical Coherence Tomography. Semin Ophthalmol. 2018;33(4):494–7. https://doi.org/10.1080/08820538.2017.1307423.
Ascaso F, Jimenez B, del Val JL, Lozano IP, Perez-Garcia D, Ibanez-Alperte J, et al. Is retinal optical coherence tomography an imaging biomarker for Parkinson disease? Invest. Ophthalmol Vis Sci. 2013;54(15):1435.
Pilat A, McLean RJ, Proudlock FA, Maconachie GD, Sheth V, Rajabally YA, et al. In vivo morphology of the optic nerve and retina in patients with Parkinson's disease. 2016;57(10):4420-7.
El-Kattan MM, Esmat SM, Esmail EH, Deraz HA, Ismail RS. Optical coherence tomography in patients with Parkinson’s disease. Egypt J Neurol Psychiatr Neurosurg. 2022;58(1):21.
Mailankody P, Battu R, Khanna A, Lenka A, Yadav R, Pal PK. Optical coherence tomography as a tool to evaluate retinal changes in Parkinson’s disease. Parkinsonism Relat Disord. 2015;21(10):1164–9.
Albrecht P, Müller AK, Südmeyer M, Ferrea S, Ringelstein M, Cohn E, Aktas O, Dietlein T, Lappas A, Foerster A, Hartung HP, Schnitzler A, Methner A. Optical coherence tomography in parkinsonian syndromes. PLoS One. 2012;7(4):e34891. https://doi.org/10.1371/journal.pone.0034891.
Sari ES, Koc R, Yazici A, Sahin G, Ermis SS. Ganglion cell-inner plexiform layer thickness in patients with Parkinson disease and association with disease severity and duration. J Neuroophthalmol. 2015;35(2):117–21. https://doi.org/10.1097/WNO.0000000000000203.
Bayhan HA, Aslan Bayhan S, Tanık N, Gürdal C. The association of spectral-domain optical coherence tomography determined ganglion cell complex parameters and disease severity in Parkinson's disease. Curr Eye Res. 2014;39(11):1117–22. https://doi.org/10.3109/02713683.2014.894080.
Almarcegui C, Dolz I, Pueyo V, Garcia E, Fernandez FJ, Martin J, Ara JR, Honrubia F. Correlation between functional and structural assessments of the optic nerve and retina in multiple sclerosis patients. Neurophysiol Clin. 2010;40(3):129–35. https://doi.org/10.1016/j.neucli.2009.12.001.
Davies EC, Galetta KM, Sackel DJ, Talman LS, Frohman EM, Calabresi PA, et al. Retinal ganglion cell layer volumetric assessment by spectral-domain optical coherence tomography in multiple sclerosis: application of a high-precision manual estimation technique. 2011;31(3):260-4.
Girkin CA, McGwin G Jr, Sinai MJ, Sekhar GC, Fingeret M, Wollstein G, Varma R, Greenfield D, Liebmann J, Araie M, Tomita G, Maeda N, Garway-Heath DF. Variation in optic nerve and macular structure with age and race with spectral-domain optical coherence tomography. Ophthalmology. 2011;118(12):2403–8. https://doi.org/10.1016/j.ophtha.2011.06.013.
Garcia-Martin E, Larrosa JM, Polo V, Satue M, Marques ML, Alarcia R, et al. Distribution of retinal layer atrophy in patients with Parkinson disease and association with disease severity and duration. 2014;157(2):470–8. e2.
Roth NM, Saidha S, Zimmermann H, Brandt AU, Isensee J, Benkhellouf-Rutkowska A, et al. Photoreceptor layer thinning in idiopathic Parkinson’s disease. 2014;29(9):1163–70.
Aydin TS, Umit D, Nur OM, Fatih U, Asena K, Nefise OY, Serpil Y. Optical coherence tomography findings in Parkinson's disease. Kaohsiung J Med Sci. 2018;34(3):166–71. https://doi.org/10.1016/j.kjms.2017.11.006.
La Morgia C, Barboni P, Rizzo G, Carbonelli M, Savini G, Scaglione C, Capellari S, Bonazza S, Giannoccaro MP, Calandra-Buonaura G, Liguori R, Cortelli P, Martinelli P, Baruzzi A, Carelli V. Loss of temporal retinal nerve fibers in Parkinson disease: a mitochondrial pattern? Eur J Neurol. 2013;20(1):198–201. https://doi.org/10.1111/j.1468-1331.2012.03701.x.
Roth NM, Saidha S, Zimmermann H, Brandt AU, Isensee J, Benkhellouf‐Rutkowska A, et al. Photoreceptor layer thinning in idiopathic Parkinson's disease. 2014;29(9):1163-70.
Garcia-Martin E, Rodriguez-Mena D, Satue M, Almarcegui C, Dolz I, Alarcia R, Seral M, Polo V, Larrosa JM, Pablo LE. Electrophysiology and optical coherence tomography to evaluate Parkinson disease severity. Invest Ophthalmol Vis Sci. 2014;55(2):696–705. https://doi.org/10.1167/iovs.13-13062.
Altintaş O, Işeri P, Ozkan B, Cağlar Y. Correlation between retinal morphological and functional findings and clinical severity in Parkinson's disease. Doc Ophthalmol. 2008;116(2):137–46. https://doi.org/10.1007/s10633-007-9091-8.
Satue M, Seral M, Otin S, Alarcia R, Herrero R, Bambo M, et al. Retinal thinning and correlation with functional disability in patients with Parkinson's disease. 2014;98(3):350–5.
Lee J-Y, Kim JM, Ahn J, Kim H-J, Jeon BS, Kim TW. Retinal nerve fiber layer thickness and visual hallucinations in Parkinson’s Disease. Mov Disord. 2014;29(1):61–7.
Visser F, Apostolov VI, Vlaar AMM, Twisk JWR, Weinstein HC, Berendse HW. Visual hallucinations in Parkinson’s disease are associated with thinning of the inner retina. Sci Rep. 2020;10(1):21110.
Ikeda H, Head GM, Ellis CJ. Electrophysiological signs of retinal dopamine deficiency in recently diagnosed Parkinson’s disease and a follow up study. Vision Res. 1994;34(19):2629–38.
Robson AG, Nilsson J, Li S, Jalali S, Fulton AB, Tormene AP, et al. ISCEV guide to visual electrodiagnostic procedures. Doc Ophthalmol. 2018;136(1):1–26.
Burguera JA, Vilela C, Traba A, Ameave Y, Vallet M. The electroretinogram and visual evoked potentials in patients with Parkinson’s disease. Arch de Neurobiol. 1990;53(1):1–7.
Nightingale S, Mitchell KW, Howe JW. Visual evoked cortical potentials and pattern electroretinograms in Parkinson’s disease and control subjects. J Neurol Neurosurg Psychiatry. 1986;49(11):1280–7.
Gottlob I, Schneider E, Heider W, Skrandies W. Alteration of visual evoked potentials and electroretinograms in Parkinson’s disease. Electroencephalogr Clin Neurophysiol. 1987;66(4):349–57.
Nowacka B, Lubiński W, Honczarenko K, Potemkowski A, Safranow K. Bioelectrical function and structural assessment of the retina in patients with early stages of Parkinson's disease (PD). Doc Ophthalmol. 2015;131(2):95–104. https://doi.org/10.1007/s10633-015-9503-0.
Burguera J, Vilela C, Traba A, Ameave Y, Vallet M. The electroretinogram and visual evoked potentials in patients with Parkinson's disease. 1990;53(1):1-7.
Kupersmith MJ, Shakin E, Siegel IM, Lieberman A. Visual system abnormalities in patients with Parkinson’s disease. Arch Neurol. 1982;39(5):284–6.
Devos D, Tir M, Maurage CA, Waucquier N, Defebvre L, Defoort-Dhellemmes S, Destée A. ERG and anatomical abnormalities suggesting retinopathy in dementia with Lewy bodies. Neurology. 2005;65(7):1107-10. https://doi.org/10.1212/01.wnl.0000178896.44905.33.
Filipová M, Terziivanov D, Balík J, Janků I, Filip V, Stika L, Krejcová H. Electroretinogram in parkinsonism and effects of L-DOPA. Act Nerv Super (Praha). 1981;23(4):301–2.
Krejcova H, Jerabek J, Filipova M, Bojar M, Polechova PJJN. Vestibilo-ocular and ERG changes in Parkinson patients. 1985;232(Suppl.):130.
Jackson CR, Capozzi M, Dai H, McMahon DG. Circadian perinatal photoperiod has enduring effects on retinal dopamine and visual function. J Neurosci. 2014;34(13):4627–33.
Mello LGM, Paraguay IBB, Andrade TS, Rocha A, Barbosa ER, Oyamada MK, et al. Electroretinography reveals retinal dysfunction in Parkinson’s disease despite normal high-resolution optical coherence tomography findings. Parkinsonism Relat Disord. 2022;101:90–5.
Acknowledgements
Not applicable.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB). Authors did not receive any funding for this work.
Author information
Authors and Affiliations
Contributions
RE participated in neurophysiological assessment and revised the manuscript. HA participated in study design, interpretation of data, and revised the manuscript. AI participated in collection and interpretation of data and helped to draft manuscript. MH participated in study design, analysis and interpretation of data and helped to draft manuscript. SI participated in study design, ophthalmological assessment, interpretation of data and helped to draft manuscript. MM participated in study design, interpretation of data and helped to draft manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was explained to all participants and written informed consent was obtained from them or their first-degree relatives before participation in the study. The study was ethically approved by Faculty of medicine, Beni Suef University Research Ethical Committee (FM-BSU REC). The approval number is FMBSUREC/06122020/ Mohammed. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Elanwar, R., Al Masry, H., Ibrahim, A. et al. Retinal functional and structural changes in patients with Parkinson’s disease. BMC Neurol 23, 330 (2023). https://doi.org/10.1186/s12883-023-03373-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03373-6