
Abstract
Background
Migraine headaches affect all ages, from childhood to old age. Migraine attacks cause significant changes in the living conditions of the sick person, including a decrease in personal, social, and occupational performance. This study was conducted to determine the prevalence of migraine in Iran through a systematic review and meta-analysis.
Method
In this systematic review and meta-analysis study, the studies associated with the prevalence of migraine using the keywords: migraine, prevalence, and Iran its equivalents in international databases PubMed, Web of Science, Scopus, Science direct, and Iranian internal information databases, including SID and MagIran, was searched without limit until November 2022. Comprehensive Meta-Analysis software (Version 2) was used to analyze the data. Due to the high number of studies reviewed in this systematic review, the Begg and Mazumdar test was used at a significance level of 0.1, and the corresponding Funnel plot was used to check publication bias. Also, the I2 test was used to check the heterogeneity in this study.
Results
22 records were included in the final analysis. The prevalence of migraine in the general population of Iran was 15.1% (confidence interval 95%: 10.7–20.9), and in this population, the prevalence of migraine was higher in women than in men. The prevalence of migraine based on The International Classification of Headache Disorders (ICHD) 2 criteria was reportedly 16.4% (95% CI: 10.8–24.1), and with ICHD3 criteria, this value was reported as 17.1% (95% CI: 7.7–33.6). Based on a survey of 4571 children, the prevalence of migraine was reported to be 5.2% (95% CI: 1.3–18.7). Also, the prevalence of migraine in adolescents was calculated based on eight studies (n = 8820). Accordingly, 11.2% (95% CI: 5.8–20.4) of adolescents have migraines. Meanwhile, the prevalence of migraine in boys was 8.2% (95% CI: 4.8–13.7), and in girls was 8% (95% CI: 6.2–12.7).
Conclusion
As a result, the prevalence of migraine in Iran, based on population-based studies, was reported as 15.1%. The result showed a higher prevalence of migraine in the general population than in children and adolescents. It was also found that the prevalence of migraine in women is higher than in men.
Similar content being viewed by others


Introduction
Migraine is a debilitating and common disease affecting millions worldwide [1]. The Headache Classification Committee of the International Headache Society (IHS) defines migraine as recurrent episodes of headache often accompanied by nausea, vomiting, photophobia, and phonophobia [2]. According to the results obtained from global burden disease 2019, migraine is the second cause of disability in the general population and the first disabling factor in women under 50 [3] in such a way that migraine attacks cause significant changes in the patient’s living conditions, including a decrease in personal, social and occupational performance [4].
Migraine prevalence varies in different geographical areas. Some studies have shown that the prevalence of migraine in Asian countries is lower than in other countries [5]. In general, the prevalence of migraine is reported between 2.6% and 21.7%, with an average of 12% [2]. The National Health Survey (NHIS) results in the United States showed that 15.3% of Americans, including 9.7% of men and 20.7% of women, reported migraines and severe headaches [6]. The review of epidemiological studies in European countries showed that the prevalence of migraine among adults is between 8 and 17.6%, while it is between 5.2 and 9.1% among children and adolescents[7]. In Iran, the prevalence of migraine in adults has varied from 5.4–41.6% [8, 9] and in children and adolescents from 4.8 to 28.1% in various studies [10, 11]. Based on the previous meta-analysis in Iran in 2016, the prevalence of migraine in Iran was reported as 14% [12].
Understanding prevalence as a function of age and sex informs how likely migraine might be in a particular patient. Also, discernment of how migraine manifests in different populations can improve the diagnosis of people with unusual presentations. On the other hand, a systematic review and meta-analysis study in 2016 investigated the prevalence of migraine in Iran. Based on this, the present study was conducted to update the results of the mentioned research and estimate the prevalence of migraine in Iran.
Method
This study aimed to estimate the prevalence of migraine based on population-based studies in Iran and the prevalence of migraine in Iranian schoolchildren. Also, subgroup analyses were performed based on diagnostic criteria, gender, and age.
In this systematic review and meta-analysis, the data of the studies were conducted to determine the prevalence of migraine in Iran without a time limit until November 2022. This study was done following the statement of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) [13]. Therefore, after obtaining the documents, two reviewers (ND, HGH) independently and blind screened based on the title and abstract of the articles. After that, the full text of the articles was evaluated. If there is a difference in the approved articles, the opinion of the third reviewer (KV) was used as a criterion.
Search strategy and inclusion and exclusion criteria
The inclusion criteria included all cross-sectional observational studies that investigated the prevalence of migraine, studies that: the full text of which was available and the information for the study, including the sample size and the criteria for diagnosing migraine; and studies that were published in English and Persian. The exclusion criteria included case report, case series, case-controls, and cohort studies.
After determining the inclusion and exclusion criteria, a systematic search of articles in three Iranian databases, MagIran and SID, with Iranian keywords and four international databases, Science Direct, Scopus, and ISI Web of Science and PubMed, with English keywords Done. The keywords used for searching in this study were selected according to the inclusion criteria based on published primary studies and Medical Subject Headings (MESH Terms) (in the reviewed database) and after a detailed examination of the questions of the study [14]. The search strategy was added to the supplementary appendix.
Quality evaluation of the studies
The quality of confirmatory (observational) studies was measured in the previous stages using observational studies’ methodological quality measurement tool. The Strobe checklist [15] was used in this study. This checklist examines various aspects of writing a study, including the title, problem statement, study objectives, study type, statistical population, sampling method, determining the appropriate sample size, defining variables and procedures, study data collection tools, statistical analysis methods, and findings. The assessments in this checklist are done using 32 different items. The studies were given a score in the range of 0–32. Since this systematic reviewincluded studies with good or medium to high quality in the analysis, articles with a score of 16 and above were selected by the authors, and studies with a score of less than 16 were considered poor quality and were omitted.
Data extraction and analysis
Pre-designed forms provided us with information. Various criteria were extracted and entered into the relevant forms, including the number of migraine patients and demographic information (first author, year of publication, country, continent, study population, and average age). We used Comprehensive Meta-Analysis software (Version 2) to analyze the data. The Begg and Mazumdar test was used at a significance level of 0.1. Also, this study used a corresponding Funnel plot and I2 test to check publication bias and heterogeneity, respectively. Also, subgroup analyses were performed based on gender and migraine diagnostic criteria.
Results
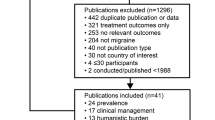
Based on the initial search in the following databases, 162 potential related articles were selected and transferred to the information management software (EndNote). Thirty-three studies were duplicated and excluded. In the screening phase, 75 articles were excluded by reading the title and abstract based on the inclusion and exclusion criteria from the remaining 129. In the eligibility evaluation stage, from the remaining 54 studies, 32 articles were excluded by reading the full text of the article based on the inclusion and exclusion criteria due to their irrelevance. Finally, 22 studies were included in the final analysis (Fig. 1).

The flowchart indicating the steps involved in reviewing the studies included in the systematic review and meta-analysis (PRISMA 2020)
Prevalence in the population-based studies
The prevalence of migraine in the general population was calculated based on data from 10 studies (Table 1). These studies investigated 12,534 people in the age range of 10–95 years. Due to the high heterogeneity of the studies (I2 = 98.5%), statistical analysis was performed using the random effects model. The studies showed no publication bias among the studies (P = 0.107) Fig. 2. Based on this, the prevalence of migraine in the general population of Iran was calculated as 15.1% (CI 95%: 10.7–20.9) Fig. 3.

Funnel plot of migraine prevalence in the general population based on population-based studies

Forest plot of migraine prevalence in the general population based on population-based studies
Based on Table 2, subgroup analyses were performed based on gender, diagnostic criteria, and migraine symptoms. Three studies were used to estimate the prevalence of migraine in men and women. The obtained results indicated that the prevalence of migraine in women is higher than in men (26.9% (CI 95%: 21.3–33.3) versus 14.9% (CI 95%: 8.9–23.7)).
Migraine diagnostic criteria were also examined in this study. Based on this, in 7 studies, migraine diagnosis was made with the help of the second version of the International Classification of Headache Disorders (ICHD2). The prevalence of migraine based on diagnosis using the ICHD2 criteria was reported as 16.4% (CI 95%: 10.8–24.1) (Table 2). Two studies used ICHD3, and one used other diagnostic criteria. Migraine prevalence was calculated based on ICHD 3 criteria to be 17.1% (CI 95%:7.7–33.6((Table 1).
Prevalence of migraine in schoolchildren:
Fourteen studies examined schoolchildren (5–20 years). (Table 3). Due to the high heterogeneity among the studies, all statistical analyses were performed based on the random effects model (Table 4). The publication bias in the results of these studies was not significant (P = 0.443) Fig. 4. Based on the 14 studies (n = 20,130), the prevalence of migraine in schoolchildren was reported as 11% (CI 95%: 7.5–15.9%) (Fig. 5). The subgroup analyses showed the prevalence of migraine in girls was 8.6% (CI 95%: 5-14.2) and in boys 7.5% (CI 95%: 4.1–13.4). Statistical analysis by diagnostic criteria can also be seen in Table 4.

Funnel plot of migraine prevalence in schoolchildren

Forest plot of migraine prevalence in schoolchildren,
Four studies (n = 4571) were used to investigate the prevalence of migraine in primary schoolchildren. Based on the results obtained from these studies, the prevalence of migraine in primary schoolchildren was reported as 5.2% (CI 95: 1.3–18.7). Also, statistical analysis was done by gender, and the results were not statistically significant (Table 4). Also, the prevalence of migraine in high school children based on eight studies was 11.2% (CI 95%: 5.8–20.4). Also, the prevalence of migraine in boys was 8.2% (CI 95%: 4.8–13.7) and 8% (CI 95%: 5.6–11.2%) in girls. Table 4.
Discussion
Based on the results of our study, the prevalence of migraine in the general population of Iran was 15.1% (CI 95%: 10.7–20.9). Subgroup analyses were performed based on gender, diagnostic criteria, and migraine symptoms. Three studies were used to estimate the prevalence of migraine in men and women. According to the results, the prevalence of migraine was reported in women at 26.9% (CI 95%: 21.3–33.3) and in men at 14.9% (CI 95%: 8.9–23.7). This result overlaps with the results of previous studies.
According to a study conducted in Germany, 23% of people over 20 have migraines [34]. A systematic review and meta-analysis conducted in 2014 examined 21 population-based studies. Based on these results, the statistical results of migraine in the general population of Africa have been reported as 5.61% (95% CI 4.61, 6.70;) which indicates less migraine compared to Iran, also the number of migraines in students has been reported as 14.89% (14.06, 15.74) [35]. In another systematic review aimed at the epidemiological investigation of migraine in Arab-speaking countries, 23 studies were examined. The prevalence of migraine in the general population was reported in the range between 2.6 and 32%. This study also observed that migraine in school children is in the range of 7.1–13.7% [36].
Different diagnostic criteria have been introduced to diagnose migraine worldwide. In 1988, the International Headache Society (IHS) introduced the first version of the International Classification of Headache Disorders (ICHD-1) [37]. Doctors and clinical researchers widely used this new diagnostic classification system. The ICHD-3 was released in early 2018. This version replaced the beta version of ICHD-3 released in 2013 [37]. Based on the results of our study, the diagnostic criteria of migraine were also examined in this study. Based on this, in 6 studies, migraine diagnosis was made with the help of the second version of the International Headache Criteria (ICHD2), and the prevalence of migraine based on the diagnosis using the ICHD2 tool was reported as 13.7% (CI 95%: 9.6–19.3). With the help of the ICHD3 tool, this value was reported as 17.1% (CI 95%: 7.7–33.6), and with the help of other diagnostic tools, this value was 17.6% (CI 95%: 1.9–69.7).
The prevalence of migraine is related to age and gender [38]. Out of this number, 77.3% of patients reported a positive family history of migraine. In that study, positive family history was defined as a migraine report in at least one relative, including father, mother, siblings, grandparents, and children [39].
Although migraine is a common disease in people aged,, its prevalence decreases in this group compared to adults [40]. According to the results, the prevalence of migraine in Iranian children and adolescents was 11% (CI 95%: 7.5–15.9%). Four studies were used to investigate the prevalence of migraine in children. These studies examined 4571 people aged 5–11 years. Based on the results obtained from these studies, the prevalence of migraine in children was reported as 5.2% (CI 95: 1.3–18.7). Also, a statistical analysis was done by gender, and the results obtained were not statistically significant.
A study stated that the prevalence of migraine in children increases with age [41]. According to another study, people aged 35 to 44 experienced minor migraines with the least intensity, and people over 45 experienced the most severe headaches [42]. In another study, it has been stated that the prevalence of migraine reaches its peak between the ages of 35 and 39 years, while the amount of this prevalence is lower at all ends of life (i.e., the relatively low prevalence in children or adolescents and the elderly) [38].
Although few studies have specifically addressed the prevalence of migraine in children, some population-based studies report a similar increase in migraine in women during puberty [43]. Based on the results of a Turkish study in school children (6–17 years), the prevalence of migraine was reported to be 26% [44], while a US study reported this rate to be 6% [45]. The ratio of migraine prevalence between men and women is not constant in all age ranges. Data from 40,892 men, women, and children in the 2003 US National Health Interview Survey (NHIS) showed that boys and girls have a similar prevalence of migraine until puberty, after which the prevalence increases in both sexes, but the increase of this value is more in women than in men [43].
Before puberty, girls and boys get migraines at about the same rate. It has been mentioned that migraine occurs earlier in boys [46]. The peak prevalence of migraine occurs in women of reproductive age, and women experience a more significant burden of migraine symptoms and disability than men. Sex hormones play an important role in migraine epidemiology [47]. The ratio of prevalence of migraine in women compared to men is approximately 3:1. Although the diagnostic criteria for migraine are the same for men and women, the clinical profile of migraine expression in women is more severe than in men [48]. Women with migraines experience more prolonged headaches, associated symptoms, migraine-related disabilities, a higher burden of co-morbidities, and worsening with age than men [43].
A review study examined related articles from China, Japan, and Korea. Based on the results of that study, the prevalence of migraine (based on IHS criteria) among adults was between 6 and 14.3%. Also, the highest complication prevalence was reported between 11 and 20% among women and between 3 and 8% among men [41]. Global prevalence data from the Global Burden of Disease Study in 2015 show that migraine is two to three times higher in women than in men, but in terms of prevalence, it peaks between 30 and 39 years of age in both sexes [43].
Limitation
One of the limitations of this study was the small number of studies reviewed. Among the other limitations, we can point out the very high heterogeneity of studies, which made it impossible to perform meta-analysis with many studies. Also, since the studies examined a small number of people, the results of this study cannot be definitively generalized to the general population. Also, this study is not registered in PROSPERO.
Conclusion
According to the results of this study, the prevalence of migraine in Iran’s general population was 15.1%, which is a significant amount. It was also observed that the prevalence of migraine in women is higher than in men. It was also observed that the prevalence of migraine in schoolchildren is 11%, which increases with age.
Data Availability
Datasets are available through the corresponding author, upon reasonable request.
References
Peles I, Asla M, Abayev M, Gordon M, Novack V, Ribalov R, Lengil T, Maor R, Elizur M, Ifergane G. Migraine epidemiology and comorbidities in Southern Israel: a clinical database study in a universal health coverage setting. J Headache Pain. 2022;23(1):160.
Yeh WZ, Blizzard L, Taylor BV. What is the actual prevalence of migraine? Brain and behavior. 2018;8(6):e00950.
Stovner LJ, Hagen K, Linde M, Steiner TJ. The global prevalence of headache: an update, with analysis of the influences of methodological factors on prevalence estimates. J Headache Pain. 2022;23(1):34.
S RP. Migraine Disability, Quality of Life, and its predictors. Annals of neurosciences. 2020;27(1):18–23.
Hashemilar M, Aminisani N, Savadi Oskoui D, Yosefian M. The prevalence of Migraine among Student of Ardabil University of Medical Sciences, 2003. J Ardabil Univ Med Sci. 2004;4(1):64–9.
Burch RC, Buse DC, Lipton RB. Migraine: Epidemiology, Burden, and Comorbidity. Neurol Clin. 2019;37(4):631–49.
Sadeghi O, Nasiri M, Saiedi SG. The Prevalence of Migraine in Different Parts of Iran: Review of the Current Evidence. 2015, 4(3):e27678.
Bahrami P, Zebardast H, Zibaei M, Mohammadzadeh M, Zabandan N. Prevalence and characteristics of headache in Khoramabad, Iran. Pain Physician. 2012;15(4):327–32.
Momayyezi M, Fallahzadeh H, Momayyezi M. Prevalence of migraine and tension-type headache in Yazd, Iran. Zahedan J Res Med Sci 2015, 17(4).
Ayatollahi S, Khosravi A. Prevalence of migraine and tension-type headache in primary-school children in Shiraz. EMHJ-Eastern Mediterranean Health Journal, 12 (6), 809–817, 2006 2006.
Moaiedi A, Boroomand S. Causes of headache in patients referring to Bandar Abbas pediatric hospital. J Hormozgan Univ Med Sci. 2004;2(1):73–6.
Farhadi Z, Alidoost S, Behzadifar M, Mohammadibakhsh R, Khodadadi N, Sepehrian R, Sohrabi R, Mirghaed MT, Salemi M, Ravaghi H. The prevalence of migraine in Iran: a systematic review and meta-analysis. Iran Red Crescent Med J 2016, 18(10).
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Morgan RL, Whaley P, Thayer KA, Schünemann HJ. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018;121(Pt 1):1027.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, Initiative S. The strengthening the reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–9.
Ahmadpanah M, Ghaderzadeh P. Investigation of prevalence and clinical characteristics of migraine patients referred to the neurology department of Sina Hospital, 2010. Pajouhan Scien J. 2014;12(4):1–6.
Foroughipour M, AZAR PM, Rasii M, Faraji M, REZAEI TF, Sadry S, EVALUATION OF THE CAUSES OF HEADACHE IN PATIENTS REFERRED TO NEUROLOGICAL AND CLINIC OF GHAEM HOSPITAL. Iran J Otorhinolaryngol. 2005;7(1):64–9.
Lankarani KB, Akbari M, Tabrizi R. Association of Gastrointestinal Functional Disorders and Migraine Headache: a Population Base Study. Middle East journal of digestive diseases. 2017;9(3):139–45.
Martami F, Ghorbani Z, Abolhasani M, Togha M, Meysamie A, Sharifi A, Jahromi SR. Comorbidity of gastrointestinal disorders, migraine, and tension-type headache: a cross-sectional study in Iran. Neurol Sci. 2018;39(1):63–70.
Rabiee B, Zeinoddini A, Kordi R, Yunesian M, Mohammadinejad P, Mansournia MA. The epidemiology of Migraine Headache in General Population of Tehran, Iran. Neuroepidemiology. 2016;46(1):9–13.
Shahbeigi S, Fereshtehnejad S-M, Mohammadi N, Golmakani MM, Tadayyon S, Jalilzadeh G, Pakdaman H. Epidemiology of headaches in Tehran urban area: a population-based cross-sectional study in district 8, year 2010. Neurol Sci. 2013;34(7):1157–66.
Zangeneh FA, Chitsaz A, Najafi MR, Norouzi R. Epidemiologic and Clinical Characteristics of Migraine Headaches: A Descriptive Study in Isfahan, Iran. J Isfahan Med School 2012, 30(187).
Saadat SMS, Hosseininezhad M, Bakhshayesh B, Hoseini M, Naghipour M. Epidemiology and clinical characteristics of chronic daily headache in a clinic-based cohort of iranian population. Neurol Sci. 2014;35(4):565–70.
Abdollahpour I, Salimi Y, Hajji M, Jarjaran Shoshtari Z. Prevalence of Migraine and its Triggers in High School Student in Boukan, 2010. Stud Med Sci. 2013;23(6):661–9.
Ayatollahi SMT, Moradi F, Ayatollahi SAR. Prevalences of migraine and tension-type headache in adolescent girls of Shiraz (Southern Iran). Headache. 2002;42(4):287–90.
Bahrami p. Incidence of Migraine in high school students in Khorramabad. Yafteh. 2006;7(1):55–60.
Fallahzadeh H, Alihaydari M. Prevalence of migraine and tension-type headache among school children in Yazd, Iran. J Pediatr neurosciences. 2011;6(2):106–9.
Ghayeghran A, FATHE SS. Survey on prevalence of migraine in highschool students of rasht-city. 2004.
Gholam-reza. Mirzaei m: a review of cammon migraine in girls high school and related fall in education in Shahrekord region. Shahrekord-University-of-Medical-Sciences. 2004;5(4):55–62.
Khazaie T, Dehghani Firoozabadi M, Sharifzadeh GR. Prevalence of migraine and its relationship to educational performance in adolescents of Brijand city (2010). Yektaweb. 2011;18(2):94–101.
Khazaie T, Dehghany M, Sharifzadeh G, Reyasie H, Phani J, Usefi H. Migraine population in primary school children of Birjand, 2010. Iran J Epidemiol. 2014;10(1):73–80.
Togha M, Rafiee P, Ghorbani Z, Khosravi A, Şaşmaz T, Akıcı Kale D, Uluduz D, Steiner TJ. The prevalence of headache disorders in children and adolescents in Iran: a schools-based study. Cephalalgia: an international journal of headache. 2022;42(11–12):1246–54.
Yaghini O, Mahmoudian T, Behfar S, Alavirad M, Ghorbani R, Pooya B. Prevalence of Headache in 11 to 18-Year-old students in Isfahan, Iran. J Isfahan Med School. 2011;29(149):1046–54.
Seddik AH, Branner JC, Ostwald DA, Schramm SH, Bierbaum M, Katsarava Z. The socioeconomic burden of migraine: an evaluation of productivity losses due to migraine headaches based on a population study in Germany. Cephalalgia: an international journal of headache. 2020;40(14):1551–60.
Woldeamanuel YW, Andreou AP, Cowan RP. Prevalence of migraine headache and its weight on neurological burden in Africa: a 43-year systematic review and meta-analysis of community-based studies. J Neurol Sci. 2014;342(1):1–15.
El-Metwally A, Toivola P, AlAhmary K, Bahkali S, AlKhathaami A, Al Ammar SA, Altamimi IM, Alosaimi SM, Jawed M, Almustanyir S. The epidemiology of Migraine Headache in Arab Countries: a systematic review. Sci World J. 2020;2020:4790254.
Tinsley A, Rothrock JF. What are we missing in the Diagnostic Criteria for Migraine? Curr Pain Headache Rep. 2018;22(12):84.
Ashina M, Katsarava Z, Do TP, Buse DC, Pozo-Rosich P, Özge A, Krymchantowski AV, Lebedeva ER, Ravishankar K, Yu S, et al. Migraine: epidemiology and systems of care. Lancet (London England). 2021;397(10283):1485–95.
Schürks M, Buring JE, Kurth T. Agreement of self-reported migraine with ICHD-II criteria in the Women’s Health Study. Cephalalgia: an international journal of headache. 2009;29(10):1086–90.
Wijeratne T, Tang HM, Crewther D, Crewther S. Prevalence of Migraine in the Elderly: a narrated review. Neuroepidemiology. 2019;52(1–2):104–10.
Takeshima T, Wan Q, Zhang Y, Komori M, Stretton S, Rajan N, Treuer T, Ueda K. Prevalence, burden, and clinical management of migraine in China, Japan, and South Korea: a comprehensive review of the literature. J Headache Pain. 2019;20(1):111.
Shauly O, Gould DJ, Patel KM. The Public’s perception of interventions for Migraine Headache Disorders: a Crowdsourcing Population-Based study. Aesthetic Surg J Open forum. 2019;1(2):ojz007.
Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017;16(1):76–87.
Wöber C, Wöber-Bingöl Ç, Uluduz D, Aslan TS, Uygunoglu U, Tüfekçi A, Alp SI, Duman T, Sürgün F, Emir GK. Undifferentiated headache: broadening the approach to headache in children and adolescents, with supporting evidence from a nationwide school-based cross-sectional survey in Turkey. J Headache Pain. 2018;19(1):1–9.
Bigal ME, Lipton RB, Winner P, Reed M, Diamond S, Stewart WF. Migraine in adolescents: association with socioeconomic status and family history. Neurology. 2007;69(1):16–25.
Broner SW, Bobker S, Klebanoff L. Migraine in women. Semin Neurol. 2017;37(6):601–10.
Burch R. Epidemiology and treatment of menstrual migraine and migraine during pregnancy and lactation: a narrative review. Headache. 2020;60(1):200–16.
Arnold M. Headache classification committee of the international headache society (IHS) the international classification of headache disorders. Cephalalgia: an international journal of headache. 2018;38(1):1–211.
Acknowledgements
The authors thank the faculty members of the Student Research Committee of Kermanshah University of Medical Sciences. This research project has been registered with code 50002521 at Kermanshah University of Medical Sciences, Iran (IR.KUMS.REC.1401.556).
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
P.M. and N.D. and K.V. contributed to the design, H.G.H. statistical analysis, participated in most of the study steps. M.H. and H.G.H. and M.K.H. prepared the manuscript. N.D. and P.M. assisted in designing the study, and helped in the, interpretation of the study. All authors have read and approved the content of the manuscript.
Corresponding authors
Ethics declarations
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mohammadi, P., Khodamorovati, M., Vafaee, K. et al. Prevalence of migraine in Iran: a systematic review and meta-analysis. BMC Neurol 23, 172 (2023). https://doi.org/10.1186/s12883-023-03215-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03215-5