
Abstract
Background
Headache is among the most frequent symptoms of acute COVID-19 infection. Its mechanisms remain obscure, but due to its migraine-like characteristics, the activation of the trigeminal system could account for its underlying pathophysiology.
Methods
Our aim was to compare the serum levels of CGRP, as a theoretical marker of trigemino-vascular activation, in 25 COVID-19 inpatients with lung involvement experiencing headache, against 15 COVID-19 inpatients without headache and with those of 25 matched healthy controls with no headache history.
Results
Morning serum alpha-CGRP levels, as measured by ELISA (Abbexa, UK), were increased in COVID-19 patients with headache (55.2±34.3 pg/mL) vs. controls (33.9±14.0 pg/mL) (p < 0.01). Alpha-CGRP levels in COVID-19 patients without headache were also significantly increased (43.3 ± 12.8 pg/mL; p = 0.05) versus healthy controls, but were numerically lower (-28.2%; p = 0.36) as compared to COVID-19 patients with headache.
Conclusion
CGRP levels are increased in COVID-19 patients experiencing headache in the acute phase of this disease, which could explain why headache frequently occurs in COVID-19 and strongly supports a role for trigeminal activation in the pathophysiology of headache in this viral infection.
Similar content being viewed by others


Introduction
Headache is one of the most frequent initial symptoms in COVID-19 infection [1,2,3,4,5]. Even though headache tends to be bilateral it usually shows migraine properties, such as moderate-severe intensity or a pulsating quality. A recent study has demonstrated that in approximately a fifth of patients who present headache during the acute phase of COVID-19, it becomes persistent. Moreover, in many of these cases headache remains with a migraine-like phenotype and the persistence of headache after COVID-19 infection is higher in patients with a previous history of migraine [6]. Although the pathophysiology of COVID-19 headache is yet unclear, it is tempting to propose that the inflammatory response associated with COVID-19 infection could activate the trigeminal system, which would account for the COVID-19 migraine-like headache. It is true that there is not a fully reliable marker for the activation of the trigeminal system, but a number of studies (see reference 7 for a recent review) have shown that CGRP is increased in acute migraine attacks [8, 9] and interictally in chronic migraine (10,11) in several human compartments, including serum [7,8,9,10,11], saliva [12] and cerebrospinal fluid [13]. The objective of this study was to compare the serum levels of CGRP, as a theoretical marker of trigemino-vascular activation, in COVID-19 inpatients experiencing headache versus COVID-19 patients and healthy controls with no headache history.
Methods
Alpha-CGRP levels were assessed from early morning blood samples in COVID-19 inpatients in their acute phase experiencing headache vs. COVID-19 inpatients without headache and matched healthy controls. Healthy controls were doctor and nurses from our hospital and family members of COVID-19 patients. Healthy controls were included if they had no history of migraine and of other active diseases and if they took no medication. To avoid storage influence, samples of COVID-19 and healthy controls were taken at the same time. All methods were carried out in accordance with relevant guidelines and regulations and declaration of Helsinki. The study was approved by our institutional Ethics Committee and written informed consent was obtained from all participants. We excluded COVID-19 patients with severe comorbidities, chronic pain conditions, with cognitive impairment or those admitted in the Intensive Care Unit. Samples, both from controls and patients, were obtained from January to September 2021. The blood was collected from the antecubital vein, allowed to clot, afterwards serum was separated after centrifugation for 10 min at 3500 rpm. Aliquots were immediately stored at -80ºC until assayed. Alpha-CGRP levels were determined using a commercial ELISA (Abbexa, UK) strictly following manufacturer’s instructions. The detection limit of the assay was 3.12pg/mL. CGRP content was described as mean ± SDs. Comparisons were established using the non-parametric Mann-Whitney test as CGRP measurements were not normally distributed.
Results
Alpha-CGRP levels were assessed from 25 healthy controls (mean age = 56.0±16.5 years; range 27–85 years; 53.3% females), 25 COVID-19 inpatients experiencing headache (mean age = 55.8±15.7 years) and 15 COVID-19 inpatients without headache (mean age 57.8 ± 13.7; range = 36–86; 53.3% females). All patients had active lung involvement directly related to COVID-19 and had headache at the time samples were collected. Headache was at least moderate and required symptomatic treatment. Headache was bilateral in 21 cases and was accompanied by gastrointestinal manifestations in ten cases. There was just one patient with a previous history of primary headache (migraine). Patients without headache did not experience headache during their whole hospital stay. In this group there was also one patient with a history of migraine Main comorbidities of COVID-19 patients are summarized in Table 1. Within the headache group fifteen (60%) patients were receiving methylprednisolone (20–80 mg/24 h) and all 25 were being treated with analgesics (at least 500 mg paracetamol every 8 h). Regarding the non-headache COVID-19 subjects, ten (66%) patients were receiving methylprednisolone (20–80 mg/24 h) and 3 had been treated with paracetamol due to fever or pain in other areas of the body the day before blood samples were taken.
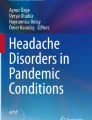
Alpha-CGRP levels were significantly elevated in COVID-19 patients with headache (55.2±34.3 pg/mL) vs. controls (33.9±14.0 pg/mL) (+ 38,5%; p < 0.01) (Fig. 1). Alpha-CGRP levels were also significantly increased (p = 0.05) in COVID-19 patients without headache versus healthy controls (Fig. 1). There was no difference in alpha-CGRP levels of the 25 patients without (51.2 ± 31.4 pg/mL) versus the 15 patients with methylprednisolone (50.5 ± 27.3 pg/mL).

Comparison of alpha-CGRP levels between healthy controls and COVID-19 inpatients with and without headache. Data are presented as mean±standard deviation **p < 0.01; *p = 0.05
Discussion
The main finding of this study is that alpha-CGRP levels are significantly increased in COVID-19 inpatients with acute headache as compared to healthy controls. Serum alpha-CGRP levels were almost 30% higher in COVID-19 inpatients with headache as compared to a similar group of COVID-19 patients without headache. These data indicate, as recently proposed for the COVID-10 anosmia [14], that trigemino-vascular activation is involved in the pathophysiology of acute headache in COVID-19 patients and, as happens in chronic migraine [10, 11], invite to suggest a role of a rather permanent activation of the trigeminal system in the pathophysiology of persistent post-COVID-19 headache.
To our knowledge, serum CGRP levels have been measured in COVID-19 patients in three previous works with heterogeneous results [15–17,]. In the study by Ochoa-Callejero et al., CGRP levels were decreased in COVID-19 patients versus healthy controls, but the samples of healthy volunteers were obtained “before the initiation of the pandemia” and were not matched for age. Just as an example, the mean age of controls in that study was 41 years and that of symptomatic inpatients (those who would be theoretically comparable to our patients) was 81 years [15]. Additionally, they do not report whether their COVID-19 subjects had headache and their serum CGRP levels of control subjects was unusually high (an average of 220.7 pg/mL, when most published studies show CGRP levels in healthy controls below 50 pg/mL) [7, 10, 11]. In a second study, Bolay et al. determined serum CGRP in COVID-19 inpatients with and without headache. The levels of CGRP were similar in both groups, but they did not analyze, for instance, the influence on CGRP levels of acute analgesics or steroids and, what is most important, there was no control group of healthy subjects [16]. Our group has very recently found an increase in both alpha- and beta-CGRP levels in serum of COVID-19 inpatients as compared to healthy controls [17].
Even considering that we obtained data from a limited number of subjects, the increase in alpha-CGRP found here was clear even in the presence of drugs such as corticosteroids or analgesics, which could theoretically diminish CGRP release, and supports a role for this neuropeptide in the headache manifestations of COVID-19 and, together with the recently described specific increase in beta-CGRP serum levels in COVID-19 patients with diarrhea (18), suggests that CGRP could be one of the molecules released in the cytokine storm induced by the COVID-19 infection. CGRP is known to enhance interleukin-6 production, the main biomarker of COVID-19 severity, which has even brought the proposal that CGRP antagonists could be of help in COVID-19 infection [19, 20]. Even though the significant increase in alpha-CGRP serum levels found here fits well with the proposal of an acute activation of the trigemino-vascular system explaining migraine-like headache seen in COVID-19 patients [14], we cannot rule out that the release of CGRP could occur at distance, for instance in the damaged nerves of the disease lungs of our patients [17]. As happens for increased beta-CGRP, which correlates with the presence of diarrhea [18], an excess of alpha-CGRP released from the lung or other body organs could also induce headache at distance by stimulating nerve terminals in the trigemino-vascular system.
Conclusion
Alpha-CGRP levels are increased when compared to healthy subjects with no headache history in COVID-19 inpatients admitted due to lung involvement and mainly in those experiencing headache in the acute phase of this disease, which could explain why headache (and other symptoms, such as anosmia) frequently occur in COVID-19 and supports a role for trigeminal activation in the pathophysiology of headache in this viral infection.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CGRP:
-
calcitonin gene-related peptide
- COVID-19:
-
coronavirus disease 2019
References
Bolay H, Güll A, Baykan B. Covid-19 is a real headache! Headache. 2020;60:1415–21.
Sampaio Rocha-Filho PA, Magalhaes JE. Headache associated with COVID-19: frequency, characteristics and association with anosmia and ageusia. Cephalalgia. 2020;40:1443–51.
Romero-Sánchez CM, Díaz-Maroto I, Fernández-Díaz E, Sánchez-Larsen A, Layos-Romero A, García-García J, et al. Neurologic manifestations in hospitalized patients with COVID-19: the ALBACOVID registry. Neurology. 2020;95:1060–70.
García-Azorín D, Sierra A, Trigo J, Alberdi A, Blanco M, Calcerrada I, et al. Frequency and phenotype of headache in Covid-19: a study of 2194 patients. Sci Rep. 2021;11:14674.
Caronna E, Ballvé A, Llauradó A, Gallardo VJ, Ariton DM, Lallana S, et al. Headache: a striking prodromal and persistent symptom, predictive of COVID-19 clinical evolution. Cephalalgia. 2020;40:1410–21.
García-Azorín D, Layos-Romero A, Porta-Etessam J, Membrilla JA, Caronna E, González-Martínez A, et al. Post-COVID-19 persistent headache: a multicentric 9-months follow-up study of 905 patients. Cephalalgia. 2022. https://doi.org/10.1177/03331024211068074.
Pozo-Rosich P, Coppola G, Pascual J, Schwedt T. How does the brain change in chronic migraine? Developing disease biomarkers. Cephalalgia. 2021;41:613–30.
Goadsby PJ, Edvinsson L, Ekman R. Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann Neurol. 1990;28:183–7.
Rodríguez-Osorio X, Sobrino T, Brea D, Martínez F, Castillo J, Leira R. Endothelial progenitor cells: a new key for endothelial dysfunction in migraine. Neurology. 2012;79:474–9.
Cernuda-Morollón E, Larrosa D, Ramón C, Vega J, Martínez-Camblor P, Pascual J. Interictal increase of CGRP levels in peripheral blood as a biomarker for chronic migraine. Neurology. 2013;81:1191–6.
Domínguez C, Vieites-Prado A, Pérez-Mato M, Rodríguez-Osorio X, López A, Campos F, et al. CGRP and PTX3 as predictors of efficacy of onabotulinum toxin type A in chronic migraine: an observational study. Headache. 2018;58:78–87.
Alpuente A, Gallardo VJ, Asskour L, Caronna E, Torres-Ferrús M, Pozo-Rozich P. Salivary CGRP can monitor the different migraine phases: CGRP (in)dependent attacks. Cephalalgia. 2021. https://doi.org/10.1177/03331024211040467.
van Dogen RM, Zielman R, Noga M, Dekkers OL, Hankeimeier T, van den Maagdenberg AM, et al. Migraine biomarkers in cerebrospinal fluid: a systematic review and meta-analysis. Cephalalgia. 2017;37:49–63.
Messlinger K, Neuhuber W, May A. Activation of the trigeminal system as a likely target of SARS-COV-2 may contribute to anosmia in COVID-19. Cephalalgia. 2022;42:176–80.
Ochoa-Callejero L, García-Sanmartín J, Villoslada-Blanco P, Iñiguez M, Pérez-Matute P, Pujadas E, et al. Circulating levels of calcitonin gene-related peptide are lower in COVID-19 patients. J Endocr Soc. 2021;5:1–8.
Bolay H, Karadas Ö, Oztürk B, Sonkaya R, Tasdelen B, Bulut TDS et al. HMGB1, NLRP3, IL-6 and ACE2 levels are elevated in COVID-19 with headache: A window to the infection-related headache mechanism. J Headache Pain. 2021; https://doi.org/10.1186/s10194-021-01306-7.
Gárate G, Pascual M, Rivero M, Toriello M, Pérez-Pereda M, González-Quintanilla V, et al. Serum calcitonin gene-related peptide alpha and beta levels are increased in COVID-19 inpatients. Arch Med Res. 2023;54:56–63.
Gárate G, Pascual M, Olmos JM, Fariñas C, Rivero M, Crespo J, et al. Increase in calcitonin gene-related peptide (CGRPbeta) levels in COVID-19 patients with diarrhea: and underlying mechanism? Dig Dis Sci. 2022;19:1–2. https://doi.org/10.1007/s10620-022-07473-0.
Robertson CE. Could CGRP antagonists be helpful in the fight against COVID-19? Headache 2020; 60:1450–1452.
Özkan E, Celebi Ö, Keskin Ö, Gursoy A, Gürsoy-Ozdemir Y. Is persistent post-COVID headache associated with protein-protein interactions between antibodies against viral spike protein and CGRP receptor? A case report. Front Pain Res. 2022;3:858709. https://doi.org/10.3389/fpain.2022.858709.
Acknowledgements
We thank the nurses of our hospital who collaborated in obtaining the blood samples.
Funding
This work was supported by grants from the Instituto de Salud Carlos III (PI20/01358) and IDIVAL (INNVAL 20/25 and 21/31)
Author information
Authors and Affiliations
Contributions
J.P. and J.M.O. were responsible for conception and design. V.G.Q., S.P.P. and M.P. for the acquisition of clinical data, G.G. and M.T. performed the laboratory determinations and G.G. and J.P. wrote the main manuscript text and prepared the figure. All authors reviewed the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
All participants received a complete description of the study and granted informed consent. The study was approved by the Ethics Committee of Cantabria (number 27/2020). All the methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gárate, G., Toriello, M., González-Quintanilla, V. et al. Serum alpha-CGRP levels are increased in COVID-19 patients with headache indicating an activation of the trigeminal system. BMC Neurol 23, 109 (2023). https://doi.org/10.1186/s12883-023-03156-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03156-z