
Abstract
Background
Colloid cyst (CC) is a rare and benign cyst found in the third ventricle near the foramen of Monro. Although the role of surgical resection is well established in symptomatic large-sized CC, it remains debatable whether surgical removal of CC with no symptoms or minimal symptoms is necessary.
Case presentation
A 49-year-old male patient visited our institute for incidentally detected intracranial mass. MRI demonstrated typical, 12 mm-sized CC located in the third ventricle. It was noticed that the cyst spontaneously decreased in size from 12 mm to 4 mm on MRI at 18 months after the first visit.
Conclusion
Although spontaneous regression is a very rare phenomenon in CC, regular imaging study and frequent neurologic examination can be an alternative option for well-selected, asymptomatic cases.
Similar content being viewed by others


Background
Colloid cyst (CC) is a benign cyst found in the third ventricle near the foramen of Monro [1]. It is rare, with an incidence of 0.5-1% of all intracranial tumors [2]. This lesion occurs rarely in children. Most cases of CC have been found in adults [3]. CC is especially common among people in their 30 and 50 s, with a possible familial predisposition. Its incidence rate decreases in age after adulthood.
Although CC is thought to be congenital, the pathogenesis of CC remains controversial [4]. This cyst shows a variety of clinical courses [5]. It can remain indolent for years and become discovered incidentally in asymptomatic patients. Clinically, this lesion presents in various ways, including headaches, gait disturbance, nausea, blurred vision and urinary incontinence. It is mainly associated with acute or chronic hydrocephalus. Sometimes CC can suddenly block foramen of Monro, causing drop attacks or sudden death [3, 6, 7]. Surgical resection is considered first for symptomatic CC treatment, even if hydrocephalus is absent [7]. In cases with minimal or no symptoms, the lesion could be surgically resected or observed through serial neuroimaging. Since spontaneous regression is very rare, we report such a case and discuss the pathological mechanism with a review of related literature.
Case presentation
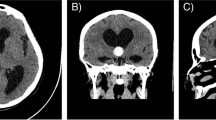
A 49-year-old male patient visited our institute for an incidentally detected intracranial mass. The patient had no underlying disease. He did not complain of any symptoms such as headaches or dizziness. On neurological and physical examination, there were no specific findings or neurological deficits associated with intracranial hypertension. Brain MRI revealed a 12 mm-sized CC located in the third ventricle. The cystic lesion was a round and well-demarcated lesion located in the right foramen of Monro and the upper third ventricle. The lesion was isointense on T1-weighted images and predominantly hyperintense on T2 with a hypointense focus within the lesion. The signal intensity pattern was the same on fluid-attenuated inversion recovery (FLAIR) images likely due to the highly proteinaceous nature of cyst fluid. There was neither hydrocephalus nor any signs of hemorrhage. The patient was followed up with regular imaging protocol. It was noticed that the cyst spontaneously decreased in size from 12 mm to 4 mm on MRI at 18 months after the first visit. As a result of follow-up at 30 months, the size of the lesion was maintained constant without any clinical symptoms (Fig. 1).

Chronologic evolution of the signal and morphology of a colloid cyst on serial MRI (T1- & T2-weighted, and FLAIR images). Follow-up MRI showed significant regression of the colloid cyst from 12 mm to 4 mm at 18 months after the initial diagnosis. This regression was maintained in follow-up MRI at 30 months
Discussion and conclusions
CC is a pathologically benign intracranial mass [5]. The clinical course of the CC is not yet fully understood [6]. Although there are some well-known typical clinical patterns and radiologic findings, unpredictable neurological symptoms and variable radiological findings could be present [8]. Most CCs show indolent behavior. However, there are CC cases with sudden death [9] due to sudden blockage of cerebrospinal fluid (CSF) with brain herniation [5]. Based on this, even if there are no symptoms for large-sized CCs, surgical resection should be considered. However, whether surgical removal of CC with no symptom or minimal symptoms is necessary remains debatable.
The present case is the tenth report on spontaneous regression of CC [1, 7, 9,10,11,12,13,14,15] (Table 1). All previously reported cases were incidentally discovered or complained of minor symptoms. The initial size was reported to be 5 to 30 mm. Radiologically, the lesion decreased in size or disappeared over an observation period from 15 months to 9 years. There was no deterioration of symptoms during the observation period. Although the natural history of CC remains unclear, it was found that asymptomatic CC could be monitored through regular imaging based on a retrospective study of 162 CCs [6]. In the case of asymptomatic or incidentally detected CC, prophylactic surgery is also possible. However, the risk of complications that may occur during surgery should be considered. Moreover, physicians should remember that an asymptomatic CC naturally could decrease in size over time without specific treatment, as shown in reported cases including the present case.
Although the pathophysiological cause of spontaneous regression has not been elucidated yet, a scenario in which the size decreases due to unrecognized cyst rupture is conceivable. Motoyama et al. were the first to report spontaneous regression of CC. They radiologically confirmed it as a cyst rupture. The cyst might rupture at an unknown time and all its contents could be absorbed into the ventricle, leaving only traces of the cyst wall in CC with no or minimal symptoms [7]. All spontaneous regression cases were up to 30 mm or less. The small volume of cyst wall suggests that it may appear lost on follow-up images. Aseptic meningitis might develop after rupture, although the probability is relatively low [1, 7, 9,10,11,12,13,14,15,16]. Further studies on changes in CC size are needed to understand the pathophysiological mechanisms of spontaneous regression.
For asymptomatic CCs, careful definition of the asymptomatic criteria is necessary because observation with follow-up imaging can be considered as a treatment option. Some patients say that they have no symptoms if the headache is minor, whereas others may report or feel it severe even if the headache is mild. In addition, if the size of CC increases, other signs of increased intracranial pressure should not be overlooked, and the patient should be educated.
Surgery should be considered, especially if symptoms develop during observation with an increase in the size of CC. One analysis has suggested predictors of asymptomatic to symptomatic progression, such as younger age, increased cyst size, ventricular dilatation, and increased signal on T2-weighted MRI [6]. Hussein et al. have proposed a Colloid Cyst Risk Score (CCRS) to determine the treatment of CC [16]. They suggested the following indicators as risk factors: under 65 years of age, at least 7 mm in length, anterior location, high signal intensity for FLAIR/T2 and lesion-related headaches. If CCRS is at least 3 points in total, asymptomatic cases are considered high risk. Of the 10 reported CC with spontaneous regression, 5 cases including our case were classified as medium-risk, 3 low-risk, and 2 high-risk (Table 1). Further studies are needed to predict worsening of CC based on the natural course of asymptomatic cases.
In conclusion, surgical resection is a main treatment for symptomatic or asymptomatic large CC. However, it sometimes regresses spontaneously without specific treatment. Therefore, well-selected asymptomatic CC can be observed with regular imaging study and frequent neurologic examination.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CC:
-
Colloid cyst
- MRI:
-
Magnetic resonance image
- FLAIR:
-
fluid-attenuated inversion recovery
References
Annamalai G, Lindsay KW, Bhattacharya JJ. Spontaneous resolution of a colloid cyst of the third ventricle. Br J Radiol. 2008;81(961):e20-2.
Hernesniemi J, Leivo S. Management outcome in third ventricular colloid cysts in a defined population: a series of 40 patients treated mainly by transcallosal microsurgery. Surg Neurol. 1996;45(1):2–14.
Farooq MU, Bhatt A, Chang HT. Hemorrhagic colloid cyst in a 9-year-old girl. Pediatr Neurol. 2008;38(6):443–4.
Bavil MS, Vahedi P. Familial colloid cyst of the third ventricle in non-twin sisters: case report, review of the literature, controversies, and screening strategies. Clin Neurol Neurosurg. 2007;109(7):597–601.
Joshi SM, Gnanalingham KK, Mohaghegh P, Wilson A, Elsmore A. A case of familial third ventricular colloid cyst. Emerg Med J. 2005;22(12):909–10.
Pollock BE, Schreiner SA, Huston J. 3rd: A theory on the natural history of colloid cysts of the third ventricle Neurosurgery. 2000;46(5):1077–81 discussion 1081 – 1073.
Motoyama Y, Hashimoto H, Ishida Y, Iida J. Spontaneous rupture of a presumed colloid cyst of the third ventricle–case report. Neurol Med Chir (Tokyo). 2002;42(5):228–31.
Osborn AG. Nonneoplastic Cysts. In: Osborn AG, Hedlund GL, Salzman KL, editors. Osborn's Brain. 2nd ed. Philadelphia: Elsevier; 2018. p. 895–8.
Gbejuade H, Plaha P, Porter D. Spontaneous regression of a third ventricle colloid cyst. Br J Neurosurg. 2011;25(5):655–7.
Peeters SM, Daou B, Jabbour P, Ladoux A, Abi Lahoud G. Spontaneous Regression of a Third Ventricle Colloid Cyst. World Neurosurg. 2016;90:704 e719-704.
Turel MK, Kucharczyk W, Gentili F. Spontaneous resolution of colloid cyst of the third ventricle: Implications for management. Asian J Neurosurg. 2017;12(2):203–6.
Mulcahy MJ, Chaganti J, Al-Khawaja D. The Case of the Disappearing Colloid Cyst. World Neurosurg. 2020;135:100–2.
Magalhaes-Ribeiro C, Mascarenhas L, Santos RB, Resende M. Spontaneous asymptomatic resolution of a third ventricle colloid cyst. Neurochirurgie. 2020;66(2):137–8.
Menendez-Cortezon B, Lopez-Garcia E, Roman-Pena P, Gelabert-Gonzalez M. Spontaneous resolution of colloid cyst of the third ventricle in a pediatric patient. Neurocirugia (Astur: Engl Ed) 2020.
Cosgrove ME, Saadon J, Chesler DA. Colloid cyst curtailed: A case report of spontaneous colloid cyst regression. Surg Neurol Int. 2020;11:465.
Zeineddine HA, Westmark K, Khanpara S, Conner C, Zhang X, Tandon N, Day AL. Risk Analysis and Management of Third Ventricular Colloid Cysts. World Neurosurg. 2021;146:e1071-8.
Acknowledgements
Not applicable.
Funding
This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Minist (2020R1C1C1007832 for KSM). There was no role of the funding bodies in the design of the study, in the collection, analysis, and interpretation of data or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
KSM developed conception and designed the study. JHL, JHH & YJK collected data and performed analysis and interpretation of data. JHL, JHH & KSM wrote the initial draft of the article. YJK critically revised the article. All the authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of Chonnam National University Hwasun Hospital waived for ethical approval for this study, due to the fact that this was a single case repot.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that we have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lee, JH., Hong, JH., Kim, Y.J. et al. Spontaneous regression of colloid cyst on the third ventricle: a case report with the review of the literature. BMC Neurol 22, 397 (2022). https://doi.org/10.1186/s12883-022-02933-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-022-02933-6