
Abstract
Background
Self-efficacy concerns individuals’ beliefs in their capability to exercise control in specific situations and complete tasks successfully. In people with multiple sclerosis (PwMS), self-efficacy has been associated with physical activity levels and quality of life. As a validated German language self-efficacy scale for PwMS is missing the aims of this study were to translate the Unidimensional Self-Efficacy Scale for Multiple Sclerosis (USE-MS) into German, establish face and content validity and cultural adaptation of the German version for PwMS in Austria. A further aim was to validate the German USE-MS (USE-MS-G) in PwMS.
Methods
Permission to translate and validate the USE-MS was received from the scale developers. Following guidelines for translation and validation of questionnaires and applying Bandura’s concept of self-efficacy, the USE-MS was forward-backward translated with content and face validity established. Cultural adaptation for Austria was performed using cognitive patient interviews. Reliability was assessed using Cronbach’s alpha, Person separation index and Lin’s concordance correlation coefficient. Rasch analysis was employed to assess construct validity. Comparison was made to scales for resilience, general self-efficacy, anxiety and depression, multiple sclerosis fatigue and health-related quality of life. Data were also pooled with an historic English dataset to compare the English and German language versions.
Results
The translation and cultural adaptation were successfully performed in the adaptation process of the USE-MS-G. Pretesting was conducted in 30 PwMS, the validation of the final USE-MS-G involved 309 PwMS with minimal to severe disability. The USE-MS-G was found to be valid against the Rasch model when fitting scale data using a bifactor solution of two super-items. It was shown to be unidimensional, free from differential item functioning and well targeted to the study population. Excellent convergent and known-groups validity, internal consistency, person separation reliability and test-retest reliability were shown for the USE-MS-G. Pooling of the English and German datasets confirmed invariance of item difficulties between languages.
Conclusion
The USE-MS-G is a robust, valid and reliable scale to assess self-efficacy in PwMS and can generate interval level data on an equivalent metric to the UK version.
Trial registration
ISRCTN Registry; ISRCTN14843579; prospectively registered on 02. 01. 2019.
Similar content being viewed by others
Background
Multiple Sclerosis (MS) is a chronic demyelinating disease of the central nervous system, with accumulating disability and loss in quality of life [1]. It appears relevant for people with MS (PwMS) to preserve their autonomy, despite functional limitations and an unpredictable disease course.
Self-efficacy is described as belief in one’s ability to perform relevant tasks in order to overcome challenges and to attain desirable goals. Importantly, self-efficacy is not related to people’s level of functioning or their skills but rather their judgement of what can be achieved [2]. This implies that PwMS who are confident in their ability to master challenges and reach their goals may cope with the disease more effectively. Higher levels of self-efficacy may enhance people’s motivation to be physically active as there is a strong relationship with health promoting behaviour and perceived quality of life in PwMS [3].
Several scales have been developed to assess self-efficacy in PwMS [4,5,6]. The Unidimensional Self-Efficacy Scale for Multiple Sclerosis (USE-MS) [5] was developed from the Liverpool Self-efficacy Scale (LSES) [6] and the Multiple Sclerosis Self-Efficacy Scale (MSSS) [4], both of which resulted from in-depth patient interviews and were underpinned by Bandura’s theory of self-efficacy. The USE-MS was the only scale to meet the stringent criteria of a Rasch model [7] used for assessing its psychometric properties in a large sample of PwMS [5]. Accordingly, the USE-MS is a valid and reliable instrument for use in clinical practice and research. So far, however, a validated German language version of the USE-MS is missing. Therefore, the main aim of this study was to translate the USE-MS into German and validate the German language version (USE-MS-G) using correlational and Rasch analysis. A further aim was to examine the scale for language invariance and to equate the English USE-MS and German USE-MS-G.
Methods
Study design and setting
A prospective cross-sectional translation and validation study with repeated measures and consisting of two phases, was conducted at the outpatient MS-Clinic of the Clinical Department of Neurology, Medical University of Innsbruck, Austria and Department of Neurology, Clinic for Rehabilitation Münster, Austria from 12.2.2019 to 15.06.2020. Ethical approval was received from the Ethics Committee of the Medical University of Innsbruck (reference number EK1260/2018; 13.12.2018). See Additional file 1 for a completed STROBE checklist.
Study phases
In Phase 1, the forward-backward translation, establishment of face and content validity and cross-cultural adaptation of the pre-final USE-MS-G were performed. Validity and reliability testing of the USE-MS-G were completed in Phase 2.
Participants
Printed information and invitations to participate in the study were displayed in the MS-Clinic, the Clinic for Rehabilitation, the Austrian MS Society patient magazine and on their website; they were also forwarded to MS support groups. In order to facilitate participation, severely disabled PwMS (Expanded Disability Status Scale (EDSS) [8] ≥8) were visited at home in order to be informed about the study. During their regular visits, PwMS were notified about the study by Clinic staff. All procedures followed the tenets of the Declaration of Helsinki and written informed consent was obtained from all participants.
A random cross-sectional cohort of patients with clinically definite MS in accordance with the McDonald’s criteria [9] version valid at the time of their diagnosis presenting any MS phenotype was recruited into this study. PwMS of any ethnicity with very good German language skills, aged ≥18 years with different levels of functioning were included (EDSS scores from 0 (no disability) to 9.0 (severe disability); the detailed study protocol can be found elsewhere [10].
The exclusion criteria were comorbidities potentially affecting subjective self-efficacy ratings (such as malignant diseases, other neurological or psychiatric disorders), a relapse of MS within 2 months prior to the study or any change in medication within 4 weeks of the study commencement. A relapse or relevant clinical worsening between test and retest required the exclusion of the participant.
Sample size
Phase 1
Patients were recruited until saturation was reached, indicating that no further information could be obtained from conducting additional interviews.
Phase 2
According to previous recommendations, [11, 12] for the Rasch analysis, the aim was to recruit a minimum of 250 cases presenting a wide range of self-efficacy.
Outcome measures and procedures
Demographic (gender, age) and disease specific data (disease duration, MS phenotype, disease-modifying treatment) were retrieved from patients’ files. The current EDSS was assessed by neurologists. The order of the questionnaires was randomised for each participant to minimise order effects and questionnaire data were collected twice within a 14–21-day period (test, retest).
The original self-report USE-MS has been shown to be reliable and valid for self-efficacy assessment in PwMS [5]. Scoring is achieved by summating all 12 items (items 5, 7–9 and 11 are reversed scored). The USE-MS involves a 4-point Likert scale (0 = strongly disagree to 3 = strongly agree). A higher summary score signifies stronger self-efficacy beliefs in people. In this study, the USE-MS-G was self-reported by participants. The approximate completion time is 5–10 min.
Existing validated questionnaires which came at the recommendation of either government or patient organisations [13, 14] were used to evaluate convergent construct validity of the USE-MS-G. These included the validated German language versions of the General Self-Efficacy Scale (GSE) [15], Resilience Scale (RS-13) [16], Multiple Sclerosis International Quality of Life (MusiQoL) [17], Hospital Anxiety Depression Scale (HADS) [18, 19] and the Neurological Fatigue Index Multiple Sclerosis (NFI-MS) [20].
The German GSE [21] is a 10-item self-reported 4-point Likert scale (from 1 = “not at all true” to 4 = “exactly true”). Higher GSE summary scores signify greater self-efficacy. High internal consistency, moderate concurrent validity and unidimensionality have all been shown [15].
The German RS-13 [22] is based on the 25-item Resilience Scale [23] and includes a 7-point Likert scale from which a summary score is calculated. Scores of 13–66 points, 67–72 points or 73–91 points indicate low, moderate or high resilience, respectively [16]. High internal consistency, moderate test-retest reliability and an acceptable construct have been demonstrated [16].
The German MusiQoL [24] is a 31-item self-report health-related quality of life (HRQoL) instrument. Scoring is achieved on a 5-point Likert scale ranging from 1= “never/not at all” to 5 = “always/very much” and involving reverse scoring of negatively worded items. All nine domain scores and global index are standardised on a 0–100 scale, 0 indicating the worst level of HR QoL and 100 the best. Satisfactory internal and convergent validity and acceptable reliability were shown for all MusiQol dimensions [17].
The German HADS [19] is 14-item self-report questionnaire of anxiety and depression using a 4-point Likert scale and reverse scoring of negatively worded items. Higher scores indicate higher levels of anxiety or depression. Odd numbered items are combined to score the anxiety subscale (0–21 points), even items added to generate the depression subscale (0–21 points). A good internal consistency, acceptable test-retest reliability and a two-factor structure of the scale have been demonstrated [19].
The German NFI-MS [25] is a self-report questionnaire of physical (items 1–8) and cognitive (items 9–12) MS related fatigue. A summary score is generated from items 1–7, 9 and 11–12. Scoring is performed on a 4-point Likert scale from 0 = “strongly disagree” to 3 = “strongly agree” and higher scores represent worse fatigue. Good test-retest reliability, external and internal validity [26] and acceptable responsiveness [27] have been found for the NFI-MS.
Translation, face and content validity and cultural adaptation
In Phase 1, following guidelines for the cross-cultural adaptation of patient-reported outcomes [28, 29] and the subsequently enhanced version released by the University of Leeds, UK [30], a forward-backward translation process was conducted by 6 bilingual translators, 3 native in German, 3 in English. This comprised a synthesis of translations and consensus from an expert committee of 3 neurologists, 2 physiotherapists, a clinical neuropsychologist, a methodologist, the translators and one health-care professional diagnosed with MS. Pretesting (Test 1, T1) and face-to-face cognitive interviews regarding the questionnaire wording were carried out in male and female PwMS across the disability range. Saturation was achieved after 30 recorded interviews. Cross-cultural equivalence in conceptual areas relating to semantic, idiomatic and experiential was accomplished between the USE-MS and USE-MS-G [28, 29]. Qualitative content analysis of the verbatim interview transcriptions was performed (described in detail elsewhere [10]). During all stages of the iterative adaptation process of the USE-MS-G, consultation with the UK scale developers [5] ensured that consensus was reached.
Statistical analyses
Internal (construct) validity
Scale data were fitted to the Rasch measurement model [7] in order to test the assumptions required for interval level measurement such as probabilistic ordering of item difficulties and response thresholds, local independence of items, and group invariance (for gender, age, disease duration, timepoint (test, retest), centre, and subsequently language version) as well as unidimensionality [31, 32].
Rasch analysis is now a standard tool for scale validation but details of the analysis used, including fit criteria can found in the supplementary material (Additional file 2). The main challenge to the validity of most health outcome measures is the presence of item local dependency. This can be obviated by adding dependent items together to form ‘super-items’ or ‘testlets’ [33]. Constructing two super-items and incorporating all the items into a scale, is now emerging as useful method of eliminating local dependency. This method allows for the generation of a latent estimate based on a bi-factor solution which can be tested using a (more robust) conditional test of fit [34]. Fit statistics produced when using two super-items includes the explained common variance (ECV). A value of 1 indicates that all non-error variance is contained within the latent estimate with an ECV value of > 0.9 considered sufficient to indicate that the first common factor is unidimensional [35]. Rasch Analysis was conducted using RUMM2030 software (http://www.rummlab.com.au/).
Reliability
According to the COSMIN taxonomy, reliability comprises the measurement properties of internal consistency, reliability, and measurement error [36]. Reliability was evaluated with the Person Separation Index (PSI, range 0–1) and Cronbach’s alpha (as a measure of internal consistency), which should be ≥0.85 for individual use or 0.70 for group use [26]. Cronbach’s alpha was also calculated in the study sample for the GSE, RS-13, MusiQol, HADS and NFI-MS.
Test–retest reliability was determined using Lin’s concordance correlation coefficient [37] (rc) between Test 2 (T2) and Test 3 (T3). The rc (0–1; 95% CI) was used to estimate the agreement level between the test and retest USE-MS-G data and was determined using MedCalc software (https://www.medcalc.org/). The Pearson correlation coefficient was calculated as a measure of precision and a Bias correction factor, Cb as a measure of accuracy [37].
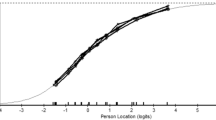
Scale precision was examined by the standard error of measurement (SEM) and minimum detectable change (MDC) based on a 95% confidence interval (CI) [38]. Targeting of the scale was evaluated by inspection of a Person-item distribution map representing both the self-efficacy levels of the persons and the difficulty of the items. Floor and ceiling effects were assessed as the percentage of minimum and maximum extreme scores which should not exceed 5% [39]. The standard error of measurement and minimum detectable change were calculated for the USE-MS-G using the formulas SEM = standard deviation (SD) * (√ (1-Cronbach’s alpha) [40] and MDC = 1.96 * √2 * SEM) [41], where 1.96 is z-value of the 95% CI of a true difference in scores [42].
Convergent and known-groups validity
Spearman’s Rank correlation analyses were performed between the USE-MS-G and other measures to determine convergent construct validity. We expected moderate (rs = 0.5–0.69) to high (rs ≥ 0.7 [43]) positive correlations of the USE-MS-G with the GSE, RS-13 and MusiQol and moderate to high negative correlations with the HADS and NFI-MS. In order to assess the known-groups validity, subgroups of gender (female, male), disease course (relapsing, progressive MS) and levels of disability (EDSS 0–4.0; 4.5–9.0) were compared using the Mann Whitney-U test and Independent-Samples Hodges-Lehman differences (95% CI).
We hypothesised that female and male genders would have similar levels of self-efficacy, PwMS with more severe disability would have lower scores (self-efficacy) than those with milder disability (1) and PwMS with progressive MS phenotype (secondary or primary progressive) would have lower scores than those with relapsing-remitting MS (2).
Questionnaires were checked for missing item responses and participants were asked for completion to avoid missing data. Rasch analysis does not require a complete data set but calculates an estimate from all available data [44]. Descriptive statistics and convergent/known-groups validity estimates were performed using IBM SPSS software (IBM SPSS Statistics; Version 26.0. Armonk, NY: IBM Corp.) or GraphPad Prism Version 8 (GraphPad Software, La Jolla, CA). Statistical significance was defined as two-tailed p-value < 0.05.
Results
Phase 1
The prefinal USE-MS-G resulted from a forward-backward translation procedure. The 30 interviewees (23 female, 3 male) were 26–75 years old and scored 0–8.0 on the EDSS (median 3.5). Their mean disease duration was 20.3 (SD 11.7) years. Some differences were detected between the English and Austrian cultures relating to this scale. For example, feeling ‘happy and satisfied’ in relation to the things somebody does in the day (item 2) appeared somewhat over-stated for the German speaking audience; so, the wording was changed to ‘content and satisfied’. In Austria, the statement ‘Sometimes I feel inadequate as a person because of my condition’ (item 5) seemed morally inacceptable as a concept. Therefore, ‘inadequate’ was changed to ‘limited’. Additionally, the phrase ‘[I can do anything] I set my mind to’ (item 12) implied stubbornness or an extraordinary strong willpower. This was changed to ‘intend to do’ to be more acceptable. Cognitive debriefing analysis showed some discrepancies, greatest with items 3 and 5 which were solved after a second round of interviews and consensus of the expert committee in line with the original test developers.
Phase 2
Population demographics
In total, 623 eligible patients were informed about the study. A number of 309 patients agreed to participate (a response rate of 49.6%) of whom 290 twice completed the questionnaires (93.8%). Nineteen patients did not complete the study as 2 participants had a relapse of MS, 11 participants could not be reached again and 6 participants reported poor health. Population characteristics are presented in Table 1 (for disease modifying treatment, DMT definitions see [10]).
Rasch analysis
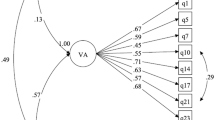
USE-MS-G test data and pooled UK and USE-MS-G data were fitted to the Rasch model separately. Local dependency was detected in the USE-MS-G data, albeit at low level, as well as overall misfit to the Rasch model (Table 2, analysis 1). Hence, the data were combined into two super-items consisting of all alternate items (i.e., one grouping of the even numbered items and one grouping of the odd numbered items) This resulted in excellent fit parameters, unidimensionality and freedom of differential item functioning (Table 2, analysis 2). The ECV was 0.988, indicating that only less than 1% of the total scale variance was lost by using a bifactor solution. Supplementary results from the Rasch analysis are shown in Additional file 3.
The UK and USE-MS-G data (N = 485) were also pooled and were found to be invariant by language (English; German) indicating that person estimates from either language version of the scale could be considered as equitable on a common metric.
Convergent and known-groups validity
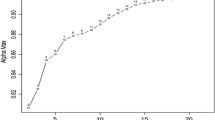
Internal consistency (Cronbach’s alpha) and person separation reliability (PSI) of the USE-MS-G are presented in Table 3, together with Cronbach’s alpha values of the MusiQoL, RS-13, GSE, HADS and NFI-MS calculated in the study sample. Convergent construct validity, Spearman’s Rank correlations (95% CI) of the USE-MG-G with the MusiQoL, RS-13, GSE, HADS and NFI-MS are also demonstrated in Table 3. There were no significant differences in self-efficacy between female (median 22, range 9–36) and male (22, 6–36) genders (p = 0.935, median difference 0 (95% CI − 2 to 2), but there were significant differences between relapsing (24, 10–36) and progressive (19, 6–36) MS groups (p < 0.001; median difference 4 (95% CI 2 to 5) and also between participants with low (24, 10–36) and high (18, 6–32) disability (p < 0.001; median difference 5 (95% CI 4 to 7). An rc of 0.92 (95% CI 0.89 to 0.93), a Pearson phi coefficient (ρ) of 0.92 and a Bias correction factor Cb of 0.99 indicated an at least moderate test-retest reliability.
A standard error of measurement (SEM) of 0.439 and a minimum detectable change (MDC) of 4.56 points were found, as measured on the original scale range of 0–36 points. That is, the smallest amount of change beyond the measurement error, expressed as MDC percentage, would be 12.7%. No floor and a 1% ceiling effect (3/309 persons) were observed and the targeting of the scale was considered good for this particular study population (Additional file 3).
Scoring instructions
Scoring is achieved by creating a summary score for all 12 items. Given fit to the Rasch model, a transformation of the raw score to interval scaling is available (Table 4).
Discussion
The purpose of this study was to translate, cross-culturally adapt the prefinal German USE-MS-G to Austria and validate the final USE-MS-G in PwMS across a wide range of disability. Forward-backward translation and pretesting according to guidelines are critical procedures in enabling and ensuring a high quality and reliable cross-cultural adaptation of a scale, as it is expected to better reflect the latent trait under investigation [29]. In the development studies of the MS-specific self-efficacy scales from which the USE-MS items were derived, qualitative interviews on PwMS’ experiences were used, where Bandura’s theory of self-efficacy underpinned the scales’ conceptual framework [5]. In agreement with the scale developers, we regarded it crucial to involve patients and learn from their feedback. Therefore, PwMS with different levels of disability were selected for Phase 1 of the study to gain insight into their perceptions of the prefinal USE-MS-G wording. However, even if great care is taken with this process, psychometric properties comparable to those of the original scale are not guaranteed. Therefore, fit of the German USE-MS to the Rasch model was examined in a well-powered sample of PwMS, representative of the MS population at large [45] and is comparable to the original validation study [5].
Correlation with comparator measures showed moderate to strong positive correlations with the RS-13, GSE and MusiQoL and hence corroborated the hypotheses of this study. The moderate relationship with the generic GSE stressed the importance of a disease-specific German language self-efficacy scale for PwMS. Similarly, moderate correlations of the English USE-MS with generic self-efficacy and resilience scales were also observed in the English validation study [5]. Symptoms of a chronic disease like MS suggest that affected people may hold divergent beliefs regarding their ability to perform relevant tasks and reach desired goals from those of healthy people. Further analyses showed moderate to strong negative correlations with the HADS and the NFI-MS, confirming the convergent construct being assessed. Supporting our hypotheses, females reported similar self-efficacy levels as males however, PwMS with a relapsing MS phenotype reported significantly higher self-efficacy than those with progressive MS. Likewise, USE-MS-G scores were significantly higher in participants with low disability. Our findings were in line with a previous study that used the MSSS for assessing self-efficacy [46]. Results from both studies suggest that people with severe and progressive MS may benefit from specific self-efficacy enhancing strategies. The USE-MS-G showed excellent reliability with a Cronbach’s alpha of 0.86, as compared to 0.83 in the English USE-MS study [5]. Furthermore, we observed a moderate to good test-retest reliability (rc = 0.92), indicating that similar levels of self-efficacy can be expected within a short period of time from the same participants if their competencies and health status remain consistent.
The USE-MS-G demonstrated good psychometric properties with fit to the Rasch model, proven unidimensionality, and good targeting when used in a typical MS outpatient population. Within Rasch analysis, invariance of the USE-MS-G was shown for groups of different age, gender, disease duration, timepoint and centres. Invariance was also found for the English and German language versions of the USE-MS, indicating their equality. The explained common variance of the two testlets was 0.988, indicating that only less than 1% of the total scale variance was lost by using a bifactor solution. This was in agreement with the original USE-MS validation study, where an ECV of 0.96 was found [5]. Our study sample was representative to the MS population at large, with a similar female-to-male ratio, levels of disability and types of disease course when compared to a nationwide Austrian study [47]. A potential limitation of this study could be that the cultural adaptation was performed only for Austria. However, cultural differences within Germany may be similarly large than between Germany or Switzerland and Austria.
The nomogram (Table 4) can be used to generate interval level estimates of self-efficacy, suitable for parametric analysis. The minimum detectable change was 12.7% i.e., change scores of less than 4.6 points are lower than the measurement error of the scale. Item functioning of the USE-MS-G was found to be equivalent to the English version and therefore direct comparison or meta-analysis of data generated across the two countries is valid.
The English USE-MS is, to our knowledge, the most rigorously developed and tested scale for assessing self-efficacy in PwMS. The German USE-MS-G scale is now available for use in clinical and research practice as its validity and reliability has been demonstrated in this study. The USE-MS-G is easy to use and available free of charge by contacting the study authors. Assessing self-efficacy may be useful to enable an individualised and comprehensive treatment in PwMS.
Conclusions
The USE-MS-G is a robust, valid and reliable scale to assess self-efficacy in PwMS. The translation and cross-cultural adaptation to Austria were performed according to international guidelines, relying on qualitative patient interviews to ensure the comprehensibility of the wording of questions. Fit to the Rasch model given, a transformation table from ordinal to interval scores is available for use clinical practice and research.
Availability of data and materials
The dataset(s) supporting the conclusions of this article (are) included within the article (and its additional file(s)). All data described in the manuscript, including all relevant raw data, are freely available to reviewers and any scientist wishing to use them for non-commercial purposes, without breaching participant confidentiality on reasonable request (barbara.seebacher@i-med.ac.at).
Abbreviations
- Cb:
-
Bias correcting factor
- χ2 :
-
Chi square test
- CI:
-
Confidence interval
- DIF:
-
Differential item functioning
- DMT:
-
Disease modifying treatment
- ECV:
-
Explained common variance
- EDSS:
-
Expanded Disability Status Scale
- GSE:
-
General Self-Efficacy Scale
- HADS:
-
Hospital Anxiety Depression Scale
- LSES:
-
Liverpool Self-efficacy Scale
- MDC:
-
Minimum detectable change
- MSSS:
-
Multiple Sclerosis Self-Efficacy Scale
- MS:
-
Multiple sclerosis
- MusiQoL:
-
Multiple Sclerosis International Quality of Life
- NFI-MS:
-
Neurological Fatigue Index Multiple Sclerosis
- ρ:
-
Pearson phi coefficient
- PSI:
-
Person Separation Index
- PwMS:
-
People with multiple sclerosis
- rc :
-
Lin’s concordance correlation coefficient
- RS-13:
-
Resilience Scale
- SD:
-
Standard deviation
- SEM:
-
Standard error of measurement
- T1:
-
Test 1 (Phase 1)
- T2:
-
Test 2 (rest in Phase 2)
- T3:
-
Test 3 (retest in Phase 2)
- USE-MS:
-
Unidimensional Self-efficacy Scale for Multiple Sclerosis
- USE-MS-G:
-
German version of the Unidimensional Self-efficacy Scale for Multiple Sclerosis
References
Compston A, Confavreux C, Lassmann H, McDonald I, Miller D, Noseworthy J, et al. McAlpine’s multiple sclerosis. 4th ed edn. London: Elsevier; 2006.
Bandura A. Social foundations of thought and action: a social cognitive theory. Englewood Cliffs: Prentice-Hall; 1986.
Finn A. The relationship between self-efficacy and health promoting behaviors, illness severity, mental health, and perceived quality of life in multiple sclerosis patients. Modern Psychol Stud. 2006;11(2):Article 3.
Rigby SA, Domenech C, Thornton EW, Tedman S, Young CA. Development and validation of a self-efficacy measure for people with multiple sclerosis: the multiple sclerosis self-efficacy scale. Mult Scler. 2003;9(1):73–81. https://doi.org/10.1191/1352458503ms870oa.
Young CA, Mills RJ, Woolmore J, Hawkins CP, Tennant A. The unidimensional self-efficacy scale for MS (USE-MS): developing a patient based and patient reported outcome. Mult Scler. 2012;18(9):1326–33. https://doi.org/10.1177/1352458512436592.
Airlie J, Baker GA, Smith SJ, Young CA. Measuring the impact of multiple sclerosis on psychosocial functioning: the development of a new self-efficacy scale. Clin Rehabil. 2001;15(3):259–65. https://doi.org/10.1191/026921501668362643.
Rasch G. Probabilistic models for some intelligence and attainment tests. Chicago: University of Chicago Press; 1980.
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–52. https://doi.org/10.1212/WNL.33.11.1444.
McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the international panel on the diagnosis of multiple sclerosis. Ann Neurol. 2001;50(1):121–7. https://doi.org/10.1002/ana.1032.
Seebacher B, Mills RJ, Reindl M, Zamarian L, Kuisma R, Kircher S, et al. German translation, cultural adaption and validation of the unidimensional self-efficacy scale for multiple sclerosis: a study protocol. BMJ Open. 2019;9(8):e029565. https://doi.org/10.1136/bmjopen-2019-029565.
Linacre JM. Sample size and item calibration stability. Rasch Measure Transact. 1994;7(4):328.
Linacre J. Understanding Rasch measurement: optimizing rating scale category effectiveness. J Appl Measure. 2002;3(1):85–106.
Potter K, Cohen ET, Allen DD, Bennett SE, Brandfass KG, Widener GL, et al. Outcome measures for individuals with multiple sclerosis: recommendations from the American Physical Therapy Association neurology section task force. Phys Ther. 2014;94(5):593–608. https://doi.org/10.2522/ptj.20130149.
Surveillance of Multiple sclerosis in adults: management (NICE guideline CG186). https://www.nice.org.uk/guidance/CG186/documents/surveillance-review-proposal (2018). Accessed 29 Dec 2018.
Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Weinman J, Wright S, Johnston M, editors. Measures in health psychology: a user’s portfolio causal and control beliefs. Windsor, UK: NFER-NELSON; 1995. p. 35–7.
Leppert K, Koch B, Brähler E, Strauß B. Die Resilienzskala (RS) – Überprüfung der Langform RS-25 und einer Kurzform RS-13. Klinische Diagnostik und Evaluation. 2008;2:226–43.
Simeoni M, Auquier P, Fernandez O, Flachenecker P, Stecchi S, Constantinescu C, et al. Validation of the multiple sclerosis international quality of life questionnaire. Mult Scler. 2008;14(2):219–30. https://doi.org/10.1177/1352458507080733.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Petermann F. Hospital anxiety and depression scale, deutsche version (HADS-D). Z Psychiatr Psychol Psychother. 2011;59(3):251–3. https://doi.org/10.1024/1661-4747/a000077.
Mills RJ, Young CA, Pallant JF, Tennant A. Rasch analysis of the modified fatigue impact scale (MFIS) in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2010;81(9):1049–51. https://doi.org/10.1136/jnnp.2008.151340.
Schwarzer R, Jerusalem ME. Skalen zur Erfassung von Lehrer- und Schülermerkmalen: Dokumentation der psychometrischen Verfahren im Rahmen der Wissenschaftlichen Begleitung des Modellversuchs Selbstwirksame Schulen. Berlin: Freie Universität Berlin; 1999.
Schumacher J, Leppert K, Gunzelmann T, Strauß B, Brähler E. Die Resilienzskala – Ein Fragebogen zur Erfassung der psychischen Widerstandsfähigkeit als Personmerkmal. Z Klin Psychol Psychiatr Psychother. 2004;53:16–39.
Wagnild GM, Young HM. Development and psychometric evaluation of the resilience scale. J Nurs Meas. 1993;1(2):165–78.
Flachenecker P, Vogel U, Simeoni MC, Auquier P, Rieckmann P. MusiQol: international questionnaire investigating quality of life in multiple sclerosis: validation results for the German subpopulation in an international comparison. Der Nervenarzt. 2011;82(10):1281–9. https://doi.org/10.1007/s00115-011-3276-9.
NFI-MS Neurologischer Fragebogen zur Müdigkeit. NFI-MS Austria/German - Version of 30 Sep 13 - Mapi ID7555 / NFI-MS_AU10_deu-ATdoc. 2010.
Mills RJ, Young CA, Pallant JF, Tennant A. Development of a patient reported outcome scale for fatigue in multiple sclerosis: the neurological fatigue index (NFI-MS). Health Qual Life Outcomes. 2010;8(1):22. https://doi.org/10.1186/1477-7525-8-22.
Mills RJ, Calabresi M, Tennant A, Young CA. Perceived changes and minimum clinically important difference of the neurological fatigue index for multiple sclerosis (NFI-MS). Mult Scler. 2013;19(4):502–5. https://doi.org/10.1177/1352458512457840.
Beaton D, Bombardier C, Guillemin F, Ferraz M. Recommendations for the cross-cultural adaptation of the DASH & QuickDASH outcome measures. Toronto, Canada: Institute for Work and Health; 2007.
Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417–32. https://doi.org/10.1016/0895-4356(93)90142-N.
Gorecki C, Brown JM, Cano S, Lamping DL, Briggs M, Coleman S, Dealey C, McGinnis E, Nelson AE, Stubbs N et al: Development and validation of a new patient-reported outcome measure for patients with pressure ulcers: the PU-QOL instrument. Health and quality of life outcomes. 2013;11:95. https://doi.org/10.1186/1477-7525-11-95.
Gustafsson J-E. Testing and obtaining fit of data to the Rasch model. Br J Math Stat Psychol. 1980;33(2):205–33. https://doi.org/10.1111/j.2044-8317.1980.tb00609.x.
Teresi JA, Kleinman M, Ocepek-Welikson K. Modern psychometric methods for detection of differential item functioning: application to cognitive assessment measures. Stat Med. 2000;19(11-12):1651–83. https://doi.org/10.1002/(SICI)1097-0258(20000615/30)19:11/12<1651::AID-SIM453>3.0.CO;2-H.
Wainer H, Kiely G. Item clusters and computer adaptive testing: a case for testlets. J Educ Meas. 1987;24(3):185–202. https://doi.org/10.1111/j.1745-3984.1987.tb00274.x.
Andrich D. Components of variance of scales with a bifactor subscale structure from two calculations of α. Educ Meas Issues Pract. 2016;35(4):25–30. https://doi.org/10.1111/emip.12132.
Rodriguez A, Reise SP, Haviland MG. Evaluating bifactor models: calculating and interpreting statistical indices. Psychol Methods. 2016;21(2):137–50. https://doi.org/10.1037/met0000045.
Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010;63(7):737–45. https://doi.org/10.1016/j.jclinepi.2010.02.006.
Lin LI-K. A concordance correlation coefficient to evaluate reproducibility. Biometrics. 1989;45(1):255–68. https://doi.org/10.2307/2532051.
van Kampen DA, Willems WJ, van Beers LWAH, Castelein RM, Scholtes VAB, Terwee CB. Determination and comparison of the smallest detectable change (SDC) and the minimal important change (MIC) of four-shoulder patient-reported outcome measures (PROMs). J Orthop Surg Res. 2013;8(1):40. https://doi.org/10.1186/1749-799X-8-40.
Fisher WPJ. Rating Scale Instrument Quality Criteria. Rasch Measure Transact. 2007;21(1):1095.
Nunnally JC, Bernstein IH. Psychometric theory. 3rd ed edn. New York: McGraw-Hill; 1994.
de Vet HC, Terwee CB, Ostelo RW, Beckerman H, Knol DL, Bouter LM. Minimal changes in health status questionnaires: distinction between minimally detectable change and minimally important change. Health Qual Life Outcomes. 2006;4(1):54. https://doi.org/10.1186/1477-7525-4-54.
Beckerman H, Roebroeck ME, Lankhorst GJ, Becher JG, Bezemer PD, Verbeek AL. Smallest real difference, a link between reproducibility and responsiveness. Qual Life Res. 2001;10(7):571–8. https://doi.org/10.1023/a:1013138911638.
Hinkle DE, Wiersma W, Jurs SG. Applied statistics for the behavioral sciences. 5th ed edn. Boston: Houghton Mifflin; 2003.
Hobart J, Cano S. Improving the evaluation of therapeutic interventions in multiple sclerosis: the role of new psychometric methods. Health Technol Assessment. 2009;13(12):iii, ix-x, 1–177. https://doi.org/10.3310/hta13120.
Pugliatti M, Rosati G, Carton H, Riise T, Drulovic J, Vecsei L, et al. The epidemiology of multiple sclerosis in Europe. Eur J Neurol. 2006;13(7):700–22. https://doi.org/10.1111/j.1468-1331.2006.01342.x.
Fraser C, Polito S. A comparative study of self-efficacy in men and women with multiple sclerosis. J Neurosci Nurs. 2007;39(2):102–6. https://doi.org/10.1097/01376517-200704000-00006.
Baumhackl U, Eibl G, Ganzinger U, Hartung HP, Mamoli B, Pfeiffer KP, et al. Prevalence of multiple sclerosis in Austria. Results of a nationwide survey. Neuroepidemiology. 2002;21(5):226–34 doi: 65640.
Acknowledgements
We would like to warmly acknowledge and thank all the participants of this study and the self-help group leaders who helped to inform their members about this study. We sincerely thank Professor Alan Tennant for sharing his extensive knowledge.
Funding
This work was supported by the Austrian MS Research Society [no grant number]. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
BS designed the study, collected the data, analysed the data, interpreted the data and wrote the manuscript. RJM analysed the data, provided data from the UK dataset, interpreted the data and edited the manuscript. RE, LZ and SK collected the data and helped to draft the manuscript. FD, MR and CB interpreted the data and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was received from the Ethics Committee of the Medical University of Innsbruck (reference number EK1260/2018; 13.12.2018).
Information brochures and invitations for study participation were displayed in the MS-Clinic, the Clinic for Rehabilitation, the Austrian MS Society patient magazine and on their website; they were also forwarded to MS support groups. Upon agreement, severely disabled PwMS (Expanded Disability Status Scale (EDSS) ≥8) were visited at home to facilitate their participation. Additionally, during their regular visits, PwMS were notified about the study by Clinic staff. All procedures followed the tenets of the Declaration of Helsinki and written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
STROBE checklist.
Additional file 2.
Supplementary methods.
Additional file 3.
Supplementary results from Rasch analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Seebacher, B., Mills, R.J., Reindl, M. et al. German translation, cultural adaptation and validation of the unidimensional self-efficacy scale for multiple sclerosis. BMC Neurol 21, 163 (2021). https://doi.org/10.1186/s12883-021-02183-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-021-02183-y