
Abstract
Background
Recent studies have shown that donor nephrectomy can induce renal function impairment. However, few meta-analysis studies about this have proceeded. Therefore, the objective of this systematic review and meta-analysis including all data of recent research studies was to determine whether living donor nephrectomy (LDN) could induce renal function impairment.
Methods
By November 2020, comprehensive literature searches were performed on PubMed, Embase, and Cochrane databases. Inclusion criteria were: (1) observational studies with data about overall end-stage renal disease (ESRD) or chronic kidney disease (CKD) of living kidney donors, (2) control group consisted of people without donor nephrectomy, and (3) outcomes of studies included long-term end-stage renal disease risks after living kidney donation. Risk of Bias in Non-randomized Studies of interventions (ROBINS-I) assessment tool was used to evaluate our methodological quality.
Results
The qualitative review included 11 studies and the meta-analysis included 5 studies. In the meta-analysis, the integrated overall ESRD risk was 5.57 (95% CI: 2.03—15.30). Regarding the overall risk of bias using ROBINS-I assessment tool, 0 studies was rated as "Low", 7 studies were rated as "moderate", 2 studies were rated as "Serious", and two studies were rated as "Critical".
Conclusions
Our study showed that LDN increased ESRD risk in LDN patients. However, in our meta-analysis, variables in included studies were not uniform and the number of included studies was small. To have a definite conclusion, meta-analyses of well-planned and detailed studies need to be conducted in the future.
Similar content being viewed by others


Introduction
End-stage renal disease (ESRD) is observed in overall world, posing huge financial burden for health-care systems [1]. Kidney transplantation (KT) is known to be an ideal renal replacement therapy for ESRD [2]. Compared with patients undergoing dialysis including hemodialysis (HD) and peritoneal dialysis (PD), successful KT can improve patients’ quality of life and survival rates as well as their daily activity limitations [3, 4]. KT is typically classified as deceased-donor or living-donor transplantation. Living-donor transplantations yield much better outcomes than deceased-donor transplantations [5].
According to World Health Organization (WHO), about 39% of all KTs were living-donor KTs, with about 27.000 kidney transplantations performed annually [6]. Although death during surgery or major complication due to kidney transplantation are very rare [7], living with one kidney affects person throughout a lifetime. For patients who have undergone living donor nephrectomy (LDN), long and short term outcomes of mortality, life expectancy, quality of life, risks of ESRD, and hypertension have been assessed and validated by several studies [8]. Long-term risk of chronic kidney disease (CKD) and ESRD following LDN has been recognized [9, 10]. Impaired renal function after LDN frequently presents with augmented urine protein levels and elevated blood pressure, beyond what is anticipated from a natural aging process [9, 11].
Previously, some studies showed that the risk of ESRD in donors was not significantly high. Ibrahim et al. reported that the risk of ESRD in donors was not significantly high [12]. Rather, in large-scale case–control studies, it was not low or different from the general population. [12]. However, recent studies comparing donors to healthy non-donors on ESRD risk associated with kidney donation showed that kidney donation is related to a small but statistically significant increase in ESRD risk [13, 14].
The purpose of our study was to investigate the actual effect of LDN on long-term overall ESRD risk. In order to surmount the above issue, a retrospective cohort study was performed which included kidney donors and multiple control groups, i.e., unscreened individuals from the general population, members of the general population who had no established pathology, and healthy controls that were matched to the donor group. Risks of mortality, ESRD, and CKD were assessed. Additionally, previous systematic review had limited sample size and inappropriate comparison groups without focusing on the incidence of ESRD in living kidney donors [9]. Recently, several observational studies have been reported. They were not included in pervious systematic reviews. Therefore, we proceeded a systematic review and meta-analysis including all data of recent research studies. Risk of Bias in Non-randomized Studies of interventions (ROBINS-I) assessment tool was used to evaluate our methodological quality.
Materials and methods
This review was conducted in accordance with the PRISMA checklist.
Search strategy
We conducted comprehensive literature searches in PubMed, Embase, and Cochrane databases through November 2020. We set as PICO; Patient/population: living kidney donor, Intervention: living donor nephrectomy, Comparison: general population or healthy population, Outcomes: CKD including ESRD. Keywords included ‘kidney transplantation’ and ‘kidney donor’ and ‘living donor’ and ‘ESRD’ or ‘end stage of renal disease’ or ‘chronic kidney disease’. Two authors (JYP and DKK) reviewed the title and abstract in accordance with inclusion criteria independently. If authors’ opinions were different, two authors had a discussion.
Study selection
Inclusion criteria were: (1) observational studies with data about overall ESRD or CKD of living kidney donors, (2) control group consisted of people without donor nephrectomy, (3) outcomes of studies included long-term ESRD risks after LDN. Studies without a control group were excluded. Studies were limited to English literature and conference abstracts were excluded. When duplicate studies targeting the same cohort were confirmed, the latest and appropriate results were selected through strict discussions between researchers. Two authors (JYP and DKK) independently reviewed the titles and abstracts of all articles using inclusion criteria and investigated full-text articles to ensure that they met inclusion criteria and extracted data using a data extraction forms. All investigators judged the last inclusions through discussion and evaluation. Data from the included study were cross-checked to ensure that there was no duplicate data and to improve the integrity of the meta-analysis.
Statistical analysis
Almost all studies had a long duration and a large population size. These kinds of results are most appropriately analyzed using the risk of long-term ESRD after LDN compared to control group. Also, we divided subgroups whose outcomes were eGFR less than 60 ml/min/m2 versus ESRD. Two studies set outcome as eGFR less than 60 ml/min/m2. Three studies set outcome as ESRD which means condition that requires acute dialysis in follow-up up period. Using the random effects model published by DerSimonian and Lairdwas, we determined the overall risk ratio (HR) with a 95% confidence interval (CI) for the results. We evaluated the statistical heterogeneity using the Cochran’s Q test and the I2 statistics.
Analysis of methodological quality
The ROBINS-I tool was used to assess the risk of bias in included studies. The bias caused by confounding domains was evaluated depending on whether control groups were matched or HR was adjusted. We evaluated the bias caused by selection of participant domain based on whether the control group was composed of a healthy group, a general group, or no control group. The bias due to classification of the intervention domain was considered low because all included studies included donor nephrectomy. We determined the bias due to deviations from intended interventional domains by other factors affecting donor nephrectomy such as hospital size, surgical volume, procedure type, and single/multi-center study. The bias due to missing data was evaluated in accordance with analysis of the claimed data or description of the tracking method. We evaluated the bias in measurement of outcomes domain by the presence or absence of HR, median follow-up period, and ESRD ratio. Bias in selection of the reported result was assessed according to HR, ESRD rates, and causes of ESRD.
Analysis of heterogeneity
We evaluated the statistical heterogeneity using the Cochran’s Q test and the I2 statistics. Cochran’s Q statistic P –value < 0.1 or an I2 statistic index > 50% indicated significant heterogeneity between studies. Insignificant X2 test result (P ≥ 0.1) and I2 statistic ≤ 50% indicated a lack of evidence to support heterogeneity, but lack of statistical power to detect heterogeneity did not necessarily mean homogeneity. Thus, random effects model was used.
Analysis of potential publication bias
Funnel plot was used to determine publication bias and without publication bias, the combined effect sizes of studies should be symmetrically distributed.
Results
Study selection
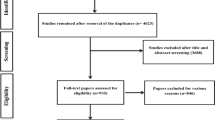
We searched 440 articles from various electronic databases (PubMed, n = 249; Cochrane, n = 4; Embase, n = 187) by November 2020. 133 studies were excluded due to overlapping data or data appearing in more than one database. After reviewing the title and abstract, 235 studies were excluded because they were not related to the topic of the present study. A more detailed review found that 72 studies were suitable. Of these, 52 studies were further excluded due to off-target disease. Some studies were excluded because of poor relevance with ESRD or donors. Eleven studies fulfilled selection criteria for methodological quality analysis. But, six studies were excluded due to insufficient data through manual search. Finally, five studies fulfilled our selection criteria for qualitative evaluation. Pairwise meta-analyses were included in the quantitative meta-analysis (Fig. 1). We conducted a systematic review of these five studies to evaluate experimental differences and topic descriptions (Tables 1 and 2). In the quantitative meta-analysis, the number of patients was 1137 to 119,769 and the follow-up period was 6.8 to 15.1 years.

Flowchart of Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA)
Methodological quality
In each study, seven domains were evaluated using the ROBINS-I tool to determine the risk of bias. In the category of bias caused by confounding domains, the number of ‘Low’ articles was 6, ‘Moderate’ was 2, ‘Serious’ was 1, and ‘Critical’ was 2. In the category of bias caused by selection of participant domain, the number of ‘Low’ articles was 4, ‘Moderate’ was 5, and ‘Serious’ was 2. Classification bias in the interventional domain was ‘low’ because all studies included donor nephrectomy. In the category of bias due to deviations from intended interventional domains, the number of ‘Low’ articles was 8 and ‘Moderate’ was 3. In the category of bias due to missing data, the number of ‘Low’ articles was 6, ‘Moderate’ was 4, and ‘Serious’ was 1. In the category of bias in measurement of outcomes domain, the number of ‘Low’ articles was 5, ‘Moderate’ was 3, and ‘Serious’ was 3. In the category of bias in selection of the reported result, the number of ‘Low’ articles was 5, ‘Moderate’ was 2, and ‘Serious’ was 4. Finally, we determined the overall risk of bias based on results of previous evaluation. As a result for an overall risk of bias, the number of ‘Low’ articles was 0, ‘Moderate’ was 7, ‘Serious’ was 2, and ‘Critical’ was 2 (Fig. 2).

Risk of bias according to ROBINS-I
Outcomes
Detailed results for ESRD risk compared to control groups are described in Fig. 3. In the meta-analysis, the pooled overall ESRD or CKD risk had an HR of 5.57 (95% CI: 2.03—15.30). Cochran’s Q test indicated a high heterogeneity (I2 = 92.0%). The pooled ESRD risk had an HR of 3.29 (95% CI: 0.94 – 11.51) and I2 was 81.0%. The pooled CKD (eGFR < 60 ml/min/1.73 m2) risk had an HR of 13.59 (95% CI: 9.42 – 19.61) and I2 was 0%.

Forest plot of end stage renal disease risk and chronic kidney disease. CI: Confidence interval, eGFR: Estimated glomerular filtration rate, ESRD: End stage renal disease, IV: Inverse variance, LDN: Living donor nephrectomy, SE: Standard error
Publication bias
Funnel plot of ESRD risk was symmetrical. Results are shown in Fig. 4. P-value for Begg and Mazumdar’s correlation test was 0.6242 and Egger’s regression coefficient test was 0.7911. This showed that evidence of publication bias or small-scale research effect did not exist in this meta-analysis.

Funnel plot of end stage renal disease risk
Discussion
Our study demonstrated that LDN patients had a higher risk of progression to ESRD compared to the control group (general group and healthy group). We conducted a quality analysis for included studies using ROBINS-I. As a result of overall risk of bias, 7 studies were rated as "moderate", 2 studies were rated as "Serious", and 2 studies were rated as "Critical".
In long-term follow-up, incidence of ESRD in donors is 0.04% to 0.5%, [18, 19] which is lower than that of the general population. Several studies showed similar or much better survival [12, 20] than the general population, because a healthy people with no comorbidities were selected by donors. This contradicts previous reports that kidney donors do not have CKD [9, 21, 22]. One reason for this is that many studies that used the MDRD formula to calculate reported the mean eGFR of the entire cohort rather than the CKD categories. All studies including our analysis calculated eGFR by the CKD-EPI equation. It is suggested that the newly developed CKD-EPI equation for GFR estimation is more accurate than the MDRD equation, especially when GFR is high [23]. It also has fewer biases, better precision, and better accuracy [23].
A reduction in eGFR after LDN is an inevitable result for donors [24]. The risk of renal failure in solitary kidney has been studied extensively over the past 30 years [16]. Brenner et al. have suggested that renal ablation can result in progressive glomerular damage to the remaining kidney associated with glomerular hypertrophy, hyperfiltration, and systemic hypertension [25]. These are related to increases of proteinuria and blood pressure [9, 11]. However, there are also more recent articles around adaptation of the remaining kidney after donation away from glomerular hypertension. Lenihan et al. showed that adaptive hyperfiltration after LDN can be induced by hyperperfusion and hypertrophy of the remaining glomeruli and argued against the progression of significant glomerular hypertension following LDN [26]. Since these factors can increase the risk of cardiovascular and all-cause mortality in the general population [27,28,29] and kidney donors after nephrectomy [14], it is important to evaluate renal function of donors before and after LDN.
Some studies have evaluated renal function after donor nephrectomy [24, 30] considering the following factors: age, gender, preoperative serum uric acid level, and pre-donation eGFR [24]. With increasing age, renal cortical volume decreases with decreasing GFR, whereas medullary volume increases, balancing the effect of reduced cortical volume on entire kidney volume to some extent [31]. Microscopically, aging in kidney is characterized by nephrosclerosis, for example, increasing focal and global (not segmental) glomerulosclerosis (FGGS), interstitial fibrosis/tubule atrophy, and arteriolosclerosis [32]. The mechanism by gender difference in association between single kidney and risk of CKD has not yet fully identified, but several studies showed the risk of CKD by gender differences [16]. Some studies have demonstrated that estrogen has an antioxidative effect and might protect the kidney through the renal nitric oxide system by weakening oxidative stress or by its effect on components of the renin–angiotensin system [33, 34]. The renal functional reserve (RFR) represents the difference between baseline eGFR and peak eGFR after experiencing difficult situations such as acute kidney injury, pregnancy, and post-nephrectomy state [35]. GFR can maintain normal ranges until 50% of nephron is lost or in patients with a single kidney. So, the RFR test can be a sensitive and early method for evaluation of decreased renal function [35]. Kim et al. [24] also reported that eGFR before donation, quartile range of eGFR percent change after 1 month of donation, and age are important factors associated with long-term renal function results after LDN. In addition, renal functional reserve, indicated through changes in eGFR percentage after 1 month of donation had a greater effect on renal outcomes in patients with lower eGFR before donation than in those with higher eGFR before donation [24]. Therefore, patients with low eGFR should be strictly observed by evaluating their renal functional reserve before donation [36] and with regular checkup after donation. A systematic follow-up program and active examination are needed after transplantation, and closer follow-up is needed for risk groups.
Our study was the first meta-analysis that evaluated ESRD risk in living donor nephrectomy. We conducted a study of individual controls containing healthy groups that met living kidney donor criteria and a comparative study examining various variables. Also, the methodological quality of included studies was evaluated using the ROBINS-I tool. ROBINS-I is a professional tool for assessing risk of bias in non-randomized studies of interventions. There are seven domains including signal questions that provide information related to the determination of each domain which includes confounding, selection of participants, classification of intervention, deviation from intended intervention, missing data, measurement of outcomes, and selection of the reported result. ROBINS-I requires considerable review content and methodology [37].
Despite several advantages, our study has some limitations. Firstly, the design of meta-analysis was based on retrospective studies and the level of evidence was bound to be low because it included only retrospective studies. Secondly, analysis based on variable factors such as age, gender, preoperative serum uric acid level, and pre-donation eGFR was not performed due to insufficient information available. Effects of variable factors on ESRD were not investigated either. Third, outcome of included 2 studies were eGFR less than 60. High levels of within-group heterogeneity and uneven covariate distribution among groups were present. Because the number of included studies was small, studies on the prevalence of CKD were included to confirm the tendency towards ESRD. Fourth, studies had medium term because most of the observational studies have a short observation period.
Conclusion
Results of this study are consistent with results of recent studies showing an increase in ESRD morbidity in LDN patients. Thus, this study supports the hypothesis from recent studies that ESRD morbidity is increased in LDN patients. However, in our meta-analysis, variables in included studies were not uniform and the number of included studies was small. In order to have a definitive conclusion, meta-analyses of well-planned and detailed studies need to be conducted in the future.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
References
Vanholder R, Annemans L, Brown E, Gansevoort R, Gout-Zwart JJ, Lameire N, Morton RL, Oberbauer R, Postma MJ, Tonelli M, et al. Reducing the costs of chronic kidney disease while delivering quality health care: a call to action. Nat Rev Nephrol. 2017;13(7):393–409.
Jeon HJ, Bae HJ, Ham YR, Choi DE, Na KR, Ahn MS, Lee KW. Outcomes of end-stage renal disease patients on the waiting list for deceased donor kidney transplantation: A single-center study. Kidney Res Clin Pract. 2019;38(1):116–23.
Laupacis A, Keown P, Pus N, Krueger H, Ferguson B, Wong C, Muirhead N. A study of the quality of life and cost-utility of renal transplantation. Kidney Int. 1996;50(1):235–42.
Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–30.
Opelz G, Wujciak T, Döhler B, Scherer S, Mytilineos J. HLA compatibility and organ transplant survival Collaborative Transplant Study. Rev Immunogenet. 1999;1(3):334–42.
Horvat LD, Shariff SZ, Garg AX. Global trends in the rates of living kidney donation. Kidney Int. 2009;75(10):1088–98.
Segev DL, Muzaale AD, Caffo BS, Mehta SH, Singer AL, Taranto SE, McBride MA, Montgomery RA. Perioperative mortality and long-term survival following live kidney donation. JAMA. 2010;303(10):959–66.
Wirken L, van Middendorp H, Hooghof CW, Rovers MM, Hoitsma AJ, Hilbrands LB, Evers AW. The Course and Predictors of Health-Related Quality of Life in Living Kidney Donors: A Systematic Review and Meta-Analysis. Am J Transplant. 2015;15(12):3041–54.
Garg AX, Muirhead N, Knoll G, Yang RC, Prasad GV, Thiessen-Philbrook H, Rosas-Arellano MP, Housawi A, Boudville N. Proteinuria and reduced kidney function in living kidney donors: A systematic review, meta-analysis, and meta-regression. Kidney Int. 2006;70(10):1801–10.
Kim Y, Yu MY, Yoo KD, Jeong CW, Kim HH, Min SI, Ha J, Choi Y, Ko AR, Yun JM, et al. Long-term Mortality Risks Among Living Kidney Donors in Korea. Am J Kidney Dis. 2020;75(6):919–25.
Boudville N, Prasad GV, Knoll G, Muirhead N, Thiessen-Philbrook H, Yang RC, Rosas-Arellano MP, Housawi A, Garg AX. Meta-analysis: risk for hypertension in living kidney donors. Ann Intern Med. 2006;145(3):185–96.
Ibrahim HN, Foley R, Tan L, Rogers T, Bailey RF, Guo H, Gross CR, Matas AJ. Long-term consequences of kidney donation. N Engl J Med. 2009;360(5):459–69.
Muzaale AD, Massie AB, Wang MC, Montgomery RA, McBride MA, Wainright JL, Segev DL. Risk of end-stage renal disease following live kidney donation. JAMA. 2014;311(6):579–86.
Mjøen G, Hallan S, Hartmann A, Foss A, Midtvedt K, Øyen O, Reisæter A, Pfeffer P, Jenssen T, Leivestad T, et al. Long-term risks for kidney donors. Kidney Int. 2014;86(1):162–7.
Lam N, Huang A, Feldman LS, Gill JS, Karpinski M, Kim J, Klarenbach SW, Knoll GA, Lentine KL, Nguan CY, et al. Acute dialysis risk in living kidney donors. Nephrol Dial Transplant. 2012;27(8):3291–5.
Kim S, Chang Y, Lee YR, Jung HS, Hyun YY, Lee KB, Joo KJ, Yun KE, Shin H, Ryu S. Solitary kidney and risk of chronic kidney disease. Eur J Epidemiol. 2019;34(9):879–88.
Haugen AJ, Hallan S, Langberg NE, Dahle DO, Pihlstrøm H, Birkeland KI, Reisaeter A, Midtvedt K, Hartmann A, Holdaas H, et al. Increased long-term risk for hypertension in kidney donors - a retrospective cohort study. Transpl Int. 2020;33(5):536–43.
Fehrman-Ekholm I, Nordén G, Lennerling A, Rizell M, Mjörnstedt L, Wramner L, Olausson M. Incidence of end-stage renal disease among live kidney donors. Transplantation. 2006;82(12):1646–8.
Ellison MD, McBride MA, Taranto SE, Delmonico FL, Kauffman HM. Living kidney donors in need of kidney transplants: a report from the organ procurement and transplantation network. Transplantation. 2002;74(9):1349–51.
Fehrman-Ekholm I, Elinder CG, Stenbeck M, Tydén G, Groth CG. Kidney donors live longer. Transplantation. 1997;64(7):976–8.
Goldfarb DA, Matin SF, Braun WE, Schreiber MJ, Mastroianni B, Papajcik D, Rolin HA, Flechner S, Goormastic M, Novick AC. Renal outcome 25 years after donor nephrectomy. J Urol. 2001;166(6):2043–7.
Lane BR, Poggio ED, Herts BR, Novick AC, Campbell SC: Renal function assessment in the era of chronic kidney disease: renewed emphasis on renal function centered patient care. J Urol. 2009;182(2):435–443; discussion 443–434.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Kim Y, Kang E, Chae DW, Lee JP, Lee S, Kim SW, Cho JH, Han M, Han S, Kim YC et al: Insufficient early renal recovery and progression to subsequent chronic kidney disease in living kidney donors. Korean J Intern Med. 2022;37(5):1021–30.
Brenner BM. Nephron adaptation to renal injury or ablation. Am J Physiol. 1985;249(3 Pt 2):F324-337.
Lenihan CR, Busque S, Derby G, Blouch K, Myers BD, Tan JC. Longitudinal study of living kidney donor glomerular dynamics after nephrectomy. J Clin Invest. 2015;125(3):1311–8.
Cinà CS, Devereaux PJ. Coronary-artery revascularization before elective major vascular surgery. McFalls EO, ward HB, Moritz TE, Goldman S, Krupski WC, Littooy F, Pierpont G, Santilli S, Rapp J, Hattler B, Shunk K, Jaenicke C, Thottapurathu L, Ellis N, Reda DJ, Henderson WG. N Engl J Med. 2004; 351: 2795–804. Vasc Med. 2006;11(1):61–3.
Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Gansevoort RT. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–81.
Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, McAlister F, Garg AX. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006;17(7):2034–47.
Kakuta Y, Imamura R, Okumi M, Horio M, Isaka Y, Ichimaru N, Takahara S, Nonomura N, Tanabe K. Assessment of renal function in living kidney donors before and after nephrectomy: A Japanese prospective, observational cohort study. Int J Urol. 2019;26(4):499–505.
Wang X, Vrtiska TJ, Avula RT, Walters LR, Chakkera HA, Kremers WK, Lerman LO, Rule AD. Age, kidney function, and risk factors associate differently with cortical and medullary volumes of the kidney. Kidney Int. 2014;85(3):677–85.
Kremers WK, Denic A, Lieske JC, Alexander MP, Kaushik V, Elsherbiny HE, Chakkera HA, Poggio ED, Rule AD. Distinguishing age-related from disease-related glomerulosclerosis on kidney biopsy: the Aging Kidney Anatomy study. Nephrol Dial Transplant. 2015;30(12):2034–9.
Silbiger S, Neugarten J: Gender and human chronic renal disease. Gend Med. 2008;5 Suppl A:S3-s10.
Yanes LL, Sartori-Valinotti JC, Reckelhoff JF. Sex steroids and renal disease: lessons from animal studies. Hypertension. 2008;51(4):976–81.
Sharma A, Mucino MJ, Ronco C. Renal functional reserve and renal recovery after acute kidney injury. Nephron Clin Pract. 2014;127(1–4):94–100.
Spinelli A, Sharma A, Villa G, Samoni S, Ramponi F, Brocca A, Brendolan A, Chiaramonte S, Castellano G, Gesualdo L, et al. Rationale for the Evaluation of Renal Functional Reserve in Living Kidney Donors and Recipients: A Pilot Study. Nephron. 2017;135(4):268–76.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355: i4919.
Acknowledgements
This work was supported by the Soonchunhyang University Research Fund.
Funding
This work was supported by Soonchunhyang University Research Fund.
Author information
Authors and Affiliations
Contributions
Conceptualization, DKK, JHK; methodology, WJY; validation, YNK, KMK, and JJP; formal analysis, DKK and SWD; investigation, DKK; resources DKK; data curation, DKK, JHK; writing—original draft preparation, JYP; writing—review & editing, JYP, DKK; visualization, DKK; supervision, DKK, JHK; project administration, DKK. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA 2020 Checklist.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Park, J.Y., Yang, W.J., Doo, S.W. et al. Long-term end-stage renal disease risks after living kidney donation: a systematic review and meta-analysis. BMC Nephrol 24, 152 (2023). https://doi.org/10.1186/s12882-023-03208-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-023-03208-z