
Abstract
Background
Post-transplant malignancy is major morbidity complicated in kidney transplantation (KT). In Korea, a few studies have investigated the sex- and age-dependent risk for post-transplant malignancy among KT recipients on a large scale.
Methods
We utilized a national health insurance database in Korea to investigate the relative risk of post-transplant malignancy in 12,634 KT recipients between 2007 and 2017. The same number of patients with acute appendicitis was included as a control group. The relative risk of malignancy was estimated using a multivariable-adjusted Cox model, and interaction analysis was performed to investigate age- and sex-predominant patterns.
Results
KT recipients had an overall 1.8-fold higher risk for post-transplant malignancy with an increased risk for 14 of 29 cancer types, among which Kaposi’s sarcoma, non-Hodgkin’s lymphoma, kidney, uterus, and bladder/urinary tract cancers were most prominent. Although the overall risk for post-transplant malignancy was similar between male and female KT recipients, head and neck cancer had a higher risk among male KT recipients, whereas non-Hodgkin’s lymphoma and bladder/urinary tract cancer had a higher risk among female KT recipients. Overall, the young (< 50 years) KT recipients had a higher risk for post-transplant malignancy than older ones (≥ 50 years), whose pattern was most prominent in non-Hodgkin’s lymphoma. In contrast, breast and nonmelanoma skin cancer showed a higher risk among older KT recipients.
Conclusion
KT recipients had an increased risk for a wide range of cancer types, some of which showed differential risk patterns with age and sex. Our result suggests that focused screening for predominant post-transplant malignancies may be an effective strategy for selected KT recipients.
Similar content being viewed by others

Introduction
Patients with severely impaired renal function ultimately require renal replacement therapy, among which kidney transplantation (KT) provides superior survival benefit and better quality of life than dialysis [1, 2]. Over the past few decades, graft survival after KT has improved with the introduction of immunosuppressive drugs such as cyclosporine, tacrolimus, and mycophenolate mofetil [3, 4], and patient survival after KT has improved with decreased post-transplant cardiovascular death [5, 6]. However, the occurrence of malignancy after KT remains a major concern to overcome in post-transplant management. Population-based studies in Australia, New Zealand, and Spain demonstrated that the death rate due to post-transplant malignancy after the first KT year has surpassed the cardiovascular death rate as a result of a relatively greater reduction in cardiovascular death [5, 7]. Exact knowledge of post-transplant malignancies may help to improve patient survival after KT and guide the development of an optimal screening and surveillance plan for post-transplant malignancies.
KT recipients have an overall 2- to fourfold increased risk of post-transplant malignancy compared to the general population [8,9,10]. In particular, the incidence and type of post-transplant malignancy differ considerably depending on geographic location and ethnicity. For example, non-melanoma skin cancer is the most common in Western populations and comprises more than half of post-kidney transplant malignancies [11,12,13], whereas non-Hodgkin lymphoma is the most common in Hong Kong [14] and kidney cancer is the most frequent in Taiwan and Japan [15, 16]. Previous Korean studies on post-kidney transplant malignancies were limited by either undersampling or a relatively short follow-up period [17,18,19]. In this study, using the 10-year nationwide claims database in Korea, we explored the relative risk of post-kidney transplant malignancies with the comparison to the healthy general population randomly sampled from subjects undergoing acute appendicitis.
Patients and methods
Data source
This study was a retrospective nationwide population-based study based on Health Insurance Review and Assessment (HIRA) data, which contains all inpatient and outpatient data since 1989 in Korea. South Korea has a compulsory national health reimbursement system, which covers approximately 97% of the population and is operated under the law of fee-for-service. HIRA reviews all claims, which contain information on personal demographics, diagnostic codes, and procedures, to reimburse health care services claimed by physicians [20]. Since all personal information used in the HIRA database was encrypted into scrambled numbers before data processing, deidentified HIRA data were obtained and the requirement of informed consent was therefore waived.
Study population
We identified KT recipients using KT procedure code (R3280) of the International Classification of Diseases, 10th revision (ICD-10) claimed between January 1, 2007, and December 31, 2017, given that procedure codes in physician claim databases almost exactly matched with data in medical charts in a previous study [21]. The following individuals were excluded from the analysis: 1) those whose KT was not the first time, 2) those who were diagnosed with any type of malignancy before KT, and 3) those who had multi-organ transplantation.
As a proxy for the general population, the same number of control population was randomly selected from individuals who had acute appendicitis (ICD-10 procedure code K35) and had not received KT during the same study period. Individuals who were diagnosed with any type of malignancy before enrollment were also excluded from the control group. The subjects in both groups were observed until the event of cancer or the study endpoint (December 31, 2018).
Study variable
The main outcome in this study was the relative risk, which is a ratio of risk for incident cancer in KT recipients to cancer risk in control group. Since relative risk is not a raw outcome, we also presented the number of incident cases as an ancillary outcome. In our analysis, we only counted the first diagnosis of specific cancer as an event because the second diagnosis of the same cancer type probably indicates recurrence. In the case of a subject who was diagnosed with two or more cancer types, we counted all and analyzed each cancer type independently. Subgroup analyses were conducted according to sex and age groups.
Site-specific cancers were identified on the basis of ICD-10 codes according to anatomic site: head and neck, digestive, lung, connective tissue and skin, reproductive and genital tract, urinary tract, brain, thyroid, hematopoietic system, and unknown primary site (Supplementary Table 1). Cancers arising in the breast and female genital tracts were investigated only in females, whereas prostate and testicular cancers were analyzed only in males. In this study, non-melanoma skin cancers were defined as a composite of Merkel, squamous, and basal cell carcinomas. Because the Korean government implements a national insurance program that pays 95% of medical expenses for malignancy since 2005, all patients diagnosed with malignancy are registered into national database at the time of their diagnosis. Thus, the diagnostic codes for malignancy are reliable and are considered accurate epidemiologic data representing real-world situations in Korea [22, 23].
Baseline clinical characteristics collected at the time of KT (or diagnosis of acute appendicitis) included sociodemographic information, such as age, sex, socioeconomic status (represented by the insurance type), as well as comorbidities (diabetes mellitus, ischemic heart disease, heart failure, liver cirrhosis, and chronic obstructive pulmonary disease). Age groups were classified into young (< 50 years) and older (≥ 50 years) groups. Underlying comorbidities were identified using ICD-10 codes (Supplementary Table 1) and the presence of each comorbidity was defined as any relevant diagnostic code within the preceding year of enrollment.
Statistical analysis
Baseline characteristics were displayed as numbers (percentages), and comparisons between the study groups were performed using the chi-square test. Cox proportional hazards analyses were performed to determine relative risk and its 95% confidence intervals (CIs) for malignancy in KT recipients. In Cox model, the subject was censored at the time of the first diagnosis of specific cancer. We found that proportional hazards assumption was satisfied using a plot of the log cumulative hazard which showed the parallel curves of the two groups. Multivariable models were constructed with adjustment for age (as a continuous variable), sex, and the presence of any of investigated comorbidities. We simplified comorbidity burden into the presence or absence of any comorbidities among diabetes mellitus, ischemic heart disease, heart failure, liver cirrhosis, and chronic obstructive pulmonary disease. This processed variable was incorporated as covariates instead of putting each comorbidity individually into Cox regression model to avoid unnecessary over-adjustment. Subgroup analyses were conducted according to sex and age groups. The interaction of sex (age group) and study group was additionally included as a covariate in Cox models to investigate the association of these factors. Firth’s penalized likelihood method was applied to the Cox regression model to estimate the relative risk for the cancer type that had no occurrence in the control group. All statistical analyses were conducted using SAS Enterprise Guide version 6.1 (SAS Institute, Cary, NC) or R 3.0.2 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided P value of < 0.05 was considered statistically significant.
Results
Characteristics of the study population
Using a nationwide health insurance database from 2007 to 2017, a total of 12,634 KT recipients were included in this study with the same number of people diagnosed with acute appendicitis as a control group. Because acute appendicitis is a disease that usually occurs in relatively young people who have good health status [24], KT recipients were older and had more comorbidities compared to the control group. Specifically, 53% of KT recipients were over 50 years old, whereas more than two-thirds of acute appendicitis occurred in people under 50 years old (Table 1). In addition, KT recipients had a greater prevalence in all of the investigated comorbidities (diabetes, ischemic heart disease, heart failure, chronic obstructive pulmonary disease, and liver cirrhosis) than the control group. Besides, compared to the control group, the proportion of males was greater in the KT group, while the percentage of medical aid, indicative of low economic status, was also higher in KT recipients.
Post-kidney transplantation malignancies
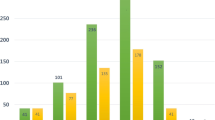
A total of 1087 malignancies occurred in KT recipients, which was higher than the 864 events in the control group (P < 0.001). The most frequently diagnosed malignancies were stomach cancer (127 vs. 119), thyroid cancer (120 vs. 125), and colorectal cancer (72 vs. 111) in KT recipients and the control group, respectively (Supplementary Table 2). The overall risk for malignancies was significantly higher in KT recipients than in the control group (adjusted relative risk[aRR], 1.8; 95% CI, 1.6–2.0; P < 0.001). In detail, the risk was significantly higher in the KT recipients with the following malignancies (sites) in the order of risk: Kaposi’s sarcoma (aRR, 23.6; 95% CI, 1.3–416.8), kidney (aRR, 14.9; 95% CI, 7.9–28.3), uterus (aRR, 7.5; 95% CI, 2.0–27.6), non-Hodgkin’s lymphoma (aRR, 4.2; 95% CI, 2.7–6.6), bladder/urinary tract (aRR, 4.1; 95% CI, 2.3–7.3), non-melanoma skin (aRR, 3.7; 95% CI, 2.0–7.2), head and neck (aRR, 3.6; 95% CI, 1.5–9.1), gallbladder and bile duct (aRR, 2.5; 95% CI, 1.2–5.5), unknown primary (aRR, 2.4; 95% CI, 1.4–4.4), breast (aRR, 2.3; 95% CI, 1.5–3.5), thyroid (aRR, 2.2; 95% CI, 1.6–3.0), pancreas (aRR, 2.1; 95% CI, 1.1–4.3), stomach (aRR, 1.7, 95% CI, 1.3–2.3), and lung (aRR, 1.6; 95% CI, 1.1–2.4) (Table 2).
Post-kidney transplantation malignancy according to sex
The total cancer occurrences per 10,000 male subjects were 882 vs. 650 in KT recipients and control groups, whose predominant cancer types showed different patterns; the top most common cancers were kidney, stomach, and liver cancers in KT recipients and stomach, prostate, and colorectal cancers in control group in the order of incident cases (Supplementary Table 2). In the case of females, a total of 819 vs. 715 cancers were newly diagnosed per 10,000 KT recipient and control subjects, among which thyroid, breast, and stomach cancers comprise the most common cancer in both groups.
Overall, the relative risk for malignancy did not differ between male and female KT recipients (Fig. 1a and Supplementary Table 3). In both sexes, KT recipients had a significantly increased risk of kidney cancer, non-Hodgkin’s lymphoma, thyroid, and stomach cancers compared to the control group (Fig. 1b). The relative risk was specifically increased in male KT recipients for head and neck, gallbladder and bile duct, non-melanoma skin, and unknown primary cancers with greater than twofold excess (Fig. 1c), whereas the relative risk for bladder/urinary tract and lung cancers was only significant in females (Fig. 1d). Of those, the interaction between sex (male vs. female) and the study group (KT vs. control group) was statistically significant for head and neck cancer (P = 0.016) in males and non-Hodgkin’s lymphoma (P = 0.004) and bladder/urinary tract cancer (P = 0.006) in females.

Forest plot presenting the relative risk for post-transplant malignancy according to sex. The forest plot was depicted for the composite of cancers A and cancers whose risk was elevated in both sexes B, only in males C, or females D. The circles represent relative risks, and the horizontal lines indicate 95% confidence intervals. The dashed lines represent male sex, while the solid lines denote female sex. The relative risk was obtained from the Cox regression model adjusted for age, sex, and the presence or absence of any of investigated comorbidities as in Table 1
Post-kidney transplantation malignancy according to age
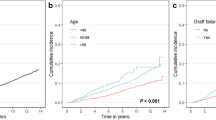
Observed events of nearly all cancer types were more common in older people (≥ 50 years). Specifically, a total of 463 vs. 1212 cancers were newly diagnosed per 10,000 young and older KT recipients, while 323 vs. 1907 cases occurred per 10,000 young and older control subjects. Kidney cancer, thyroid cancer, and non-Hodgkin’s lymphoma were the most frequent cancers among young KT recipients (< 50 years), while stomach, kidney, and thyroid cancers were the most common cancers among older ones in the order of incidence (Supplementary Table 2).
Despite lower incident cases in young KT recipients, young people showed a relatively higher risk for post-transplant malignancies than older people (aRR, 1.99 vs. 1.63) (Fig. 2a and Supplementary Table 4). This pattern was statistically significant in the interaction analysis between age (young vs. older) and the study group (KT vs. control group) (P < 0.001, Fig. 2a), which was largely attributed to a much greater risk for kidney cancer (aRR, 20.0 vs. 11.1) and non-Hodgkin’s lymphoma (aRR, 8.1 vs. 3.2) in young KT recipients (Fig. 2b).

Forest plot presenting the relative risk for post-transplant malignancy according to age group.The forest plot was depicted for the composite of cancers A and cancers whose risk was elevated in both young (< 50) and older (≥ 50) people B or only in older ones C. The circles represent relative risks, and the horizontal lines indicate 95% confidence intervals. The dashed lines represent the young, while the solid lines denote the older. The relative risk was obtained from the Cox regression model adjusted for age, sex, and the presence or absence of any of investigated comorbidities as in Table 1
In both young and older groups, an approximately fourfold higher relative risk was noted for bladder/urinary tract cancer, and an approximately twofold higher relative risk was observed for breast and thyroid cancers. In particular, older KT recipients had elevated relative risk for head and neck (5.4-fold), non-melanoma skin (4.2-fold), pancreas (2.3-fold), and stomach (50%) cancers in contrast to the non-significant risk in young KT recipients (Fig. 2c).
In the interaction analysis between age (young vs. older) and the study group (KT vs. control group), non-Hodgkin’s lymphoma (P = 0.010) had a higher risk among young KT recipients, while breast (P = 0.002) and nonmelanoma skin cancers (P = 0.028) had higher risk among older KT recipients.
Time to cancer diagnosis in the study population
The interval time to cancer diagnosis in KT recipients was shorter than that in the control group for all cancer types except for testicular and brain cancers. The median time to composite cancer diagnosis was 2.9 and 5.0 years in the KT recipients and control groups, respectively (Table 3). Of the cancer types whose cases were more than 10 in both study groups, KT recipients had an earlier diagnosis of ≥ 2 years in ovarian (4.9 years earlier), kidney (3.7 years earlier), breast (2.8 years earlier), thyroid (2.8 years earlier), and liver (2.0 years earlier) cancers compared to the control group.
Discussion
This nationwide study provides a landscape of cancer-type-specific risk after KT with comparison to the control group based on a population database of over 12,000 Korean KT recipients. Overall, KT recipients had a 1.8-fold higher risk for post-transplant malignancies in this study. This risk was similar in male and female KT recipients but differed by age, with a higher risk in young people.
The incidence of each type of cancer has geographic and racial variations. In Korea, the top five most common cancers are stomach, colorectal, thyroid, lung, and breast cancers [25]. The control group in this study demonstrated this pattern, indicating adequate sampling representative of the general population. In contrast, KT recipients have different profiles of cancer development largely due to immunosuppression and impaired immunosurveillance against oncogenic virus. In this study, the greatest risk was observed with Kaposi’s sarcoma, whose etiology is human herpesvirus 8, whereas none of the control groups developed Kaposi’s sarcoma. In addition, the two cases of anal cancer, most of which are developed by human papillomavirus infection, were seen only in KT recipients. The incidence of non-Hodgkin’s lymphoma, Epstein-Barr virus-related malignancy, was also elevated by a factor of 4.5 times in KT recipients.
Korea is one of the most prevalent areas in the world for stomach cancer [26], with the risk for this malignancy being 1.7-times higher in KT recipients in this study. The reason for this observation may be speculated to enhanced Helicobacter pylori infection under immunosuppression, but this association is neither certain nor proven [27,28,29].
Lip cancer in East Asia is not as prevalent as in Western countries [30]. In Western studies, lip cancer accounted for two-thirds or more cases of oral cavity cancer in KT recipients [8, 9, 12], while only one and two cases of lip cancer were detected among KT recipients and control group in this study, respectively.
KT recipients were at increased risk for kidney, bladder/urinary tract, and thyroid cancers as well. These cancers were previously categorized as end-stage renal disease (ESRD)-related cancers since their risk was already elevated during the dialysis period before KT [8, 31] and were not increased in other immunosuppressive states, such as human immunodeficiency virus infection (30). A higher incidence of cancer arising in the urinary system is likely to be an intrinsic factor to this anatomical region associated with ESRD, rather than solely due to immunosuppression. Interestingly, bladder/urinary tract cancer in KT recipients showed female predominance in contrast to male predominance in the general population [32]. This epidemiologic feature was also evident in previous studies conducted in Taiwan and Hong Kong [14, 16, 33], and our study validated this finding again by interaction analysis. The higher incidence of thyroid cancer in KT recipients may be explained by the lingering effect of precedent uremic milieu, although its risk was alleviated after KT compared to the dialysis period [34]. Our study showed a high incidence of thyroid cancer in both groups, and this phenomenon is thought to be a result of widespread and easily accessible screening for thyroid cancer in Korea [35].
Aging is a well-established risk factor for malignancy; however, when compared to the general population, the relative risk for post-transplant malignancy was higher in young KT recipients as evidenced by the statistical significance of the interaction analysis. Our finding is consistent with those of Canadian, Taiwanese, and Australian studies [9, 16, 31]. Contrary to this overall pattern, older people had a significantly higher risk of non-melanoma skin cancers than young people. Squamous and basal cell carcinomas comprise the vast majority of non-melanoma skin cancers [12, 36], and accumulated prior exposure to ultraviolet light possibly accounts for this older preponderance. The incidence of head and neck cancers was also much more pronounced in older people with a male-predominant pattern, which could be confounded by habitual status such as smoking.
This study had several limitations. First, the two study groups were not balanced in terms of baseline demographic and comorbidity status. Although we adjusted for age, sex, and comorbidities in Cox proportional hazard model, a portion of relative risk could be derived from the residual effect of unbalanced covariables given their probable positive associations with some cancer types [37, 38]. Nonetheless, we believe that our data genuinely represents the real world that a physician commonly encounters in clinical practice. Second, some of the cancers may be unrelated to KT since the events of malignancy were counted right after KT without a washout period to obtain incidence under the same condition in the control group. Third, detailed demographic data, such as smoking and alcohol use, as well as clinical information on donor types, immunosuppressive medications, histologic types, and stages of cancer were not available in the HIRA database, and we were thus unable to consider the impact of those factors on the relative risk for post-transplant malignancies. Lastly, the relative risk derived from Cox model was not death- or graft loss-censored. Thus, ignoring potential competing risks possibly overestimates the risk for post-transplant malignancies, but the overall relative risk in this study (1.8) was lower than previously reported results (2.5 to 3.8) calculated as a standardized incidence ratio [9, 14, 16].
In conclusion, this study reaffirmed a higher risk of malignancy among KT recipients for 14 of 29 cancer types, most of which were diagnosed earlier than the control group. Despite the life-threatening impact of post-transplant malignancies, cancer screening in KT recipients generally follows the guidelines for the general population because of the lack of well-designed randomized controlled trials in this at-risk population [39, 40]. Given differential risk patterns in some cancers according to age and sex, our results suggest that focused and more thorough screening for those cancer types may be warranted for a subset of KT recipients.
Conclusion
This study highlights the differential risks for post-transplant malignancies in Korean KT recipients depending on age and sex. For example, head and neck cancer showed a higher risk in male KT recipients, whereas non-Hodgkin’s lymphoma and bladder/urinary tract cancer had a higher risk in female ones. Although the overall risk for post-transplant malignancy was higher among young KT recipients despite its lower incidence compared to older ones, the relative risk for breast and nonmelanoma skin cancers was higher among older ones. Our result suggests that focused screening for predominant post-transplant malignancies may be an effective strategy among a subset of KT recipients who have particularly at higher risk.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- aRR:
-
Adjusted Relative Risk
- CI:
-
Confidence Interval
- COPD:
-
Chronic Obstructive Pulmonary Disease
- ESRD:
-
End-stage Renal Disease
- HIRA:
-
Health Insurance Review and Assessment
- KT:
-
Kidney Transplantation
- NA:
-
Not Applicable
- NHL:
-
Non–Hodgkin’s Lymphoma
References
Schnuelle P, Lorenz D, Trede M, Van Der Woude FJ. Impact of renal cadaveric transplantation on survival in end-stage renal failure: evidence for reduced mortality risk compared with hemodialysis during long-term follow-up. J Am Soc Nephrol. 1998;9(11):2135–41.
Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–30.
Hariharan S, Johnson CP, Bresnahan BA, Taranto SE, McIntosh MJ, Stablein D. Improved graft survival after renal transplantation in the United States, 1988 to 1996. N Engl J Med. 2000;342(9):605–12.
Knight SR, Russell NK, Barcena L, Morris PJ. Mycophenolate mofetil decreases acute rejection and may improve graft survival in renal transplant recipients when compared with azathioprine: a systematic review. Transplantation. 2009;87(6):785–94.
Ying T, Shi B, Kelly PJ, Pilmore H, Clayton PA, Chadban SJ. Death after Kidney Transplantation: An Analysis by Era and Time Post-Transplant. J Am Soc Nephrol. 2020;31(12):2887–99.
Awan AA, Niu J, Pan JS, Erickson KF, Mandayam S, Winkelmayer WC, Navaneethan SD, Ramanathan V. Trends in the Causes of Death among Kidney Transplant Recipients in the United States (1996–2014). Am J Nephrol. 2018;48(6):472–81.
Mazuecos A, Munoz Terol JM, Garcia Alvarez T, Sola E, Rodriguez Benot A, Dsuna A, Bedoya R, Gentil MA. Increase in malignancies as cause of death in renal transplant patients. Transpl Proc. 2009;41(6):2159–62.
Vajdic CM, McDonald SP, McCredie MR, van Leeuwen MT, Stewart JH, Law M, Chapman JR, Webster AC, Kaldor JM, Grulich AE. Cancer incidence before and after kidney transplantation. JAMA. 2006;296(23):2823–31.
Villeneuve PJ, Schaubel DE, Fenton SS, Shepherd FA, Jiang Y, Mao Y. Cancer incidence among Canadian kidney transplant recipients. Am J Transplant. 2007;7(4):941–8.
Wang Y, Lan GB, Peng FH, Xie XB. Cancer risks in recipients of renal transplants: a meta-analysis of cohort studies. Oncotarget. 2018;9(20):15375–85.
Collett D, Mumford L, Banner NR, Neuberger J, Watson C. Comparison of the incidence of malignancy in recipients of different types of organ: a UK Registry audit. Am J Transplant. 2010;10(8):1889–96.
Krynitz B, Edgren G, Lindelof B, Baecklund E, Brattstrom C, Wilczek H, Smedby KE. Risk of skin cancer and other malignancies in kidney, liver, heart and lung transplant recipients 1970 to 2008–a Swedish population-based study. Int J Cancer. 2013;132(6):1429–38.
Tessari G, Naldi L, Boschiero L, Minetti E, Sandrini S, Nacchia F, Valerio F, Rugiu C, Sassi F, Gotti E, et al. Incidence of primary and second cancers in renal transplant recipients: a multicenter cohort study. Am J Transplant. 2013;13(1):214–21.
Cheung CY, Lam MF, Chu KH, Chow KM, Tsang KY, Yuen SK, Wong PN, Chan SK, Leung KT, Chan CK, et al. Malignancies after kidney transplantation: Hong Kong renal registry. Am J Transplant. 2012;12(11):3039–46.
Hoshida Y, Tsukuma H, Yasunaga Y, Xu N, Fujita MQ, Satoh T, Ichikawa Y, Kurihara K, Imanishi M, Matsuno T, et al. Cancer risk after renal transplantation in Japan. Int J Cancer. 1997;71(4):517–20.
Li WH, Chen YJ, Tseng WC, Lin MW, Chen TJ, Chu SY, Hwang CY, Chen CC, Lee DD, Chang YT, et al. Malignancies after renal transplantation in Taiwan: a nationwide population-based study. Nephrol Dial Transplant. 2012;27(2):833–9.
Park B, Yoon J, Choi D, Kim HJ, Jung YK, Kwon OJ, Lee KG. De novo cancer incidence after kidney and liver transplantation: Results from a nationwide population based data. Sci Rep. 2019;9(1):17202.
Heo J, Noh OK, Oh YT, Chun M, Kim L. Cancer risk after renal transplantation in South Korea: a nationwide population-based study. BMC Nephrol. 2018;19(1):311.
Hwang JK, Moon IS, Kim JI. Malignancies after kidney transplantation: a 40-year single-center experience in Korea. Transpl Int. 2011;24(7):716–21.
Cheol Seong S, Kim YY, Khang YH, Heon Park J, Kang HJ, Lee H, Do CH, Song JS, Hyon Bang J, Ha S, et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int J Epidemiol. 2017;46(3):799–800.
Cha JM, Kim HS, Kwak MS, Park S, Park G, Kim JS, Kim JH, Kim WH. Big Data Research G: Features of Postcolonoscopy Colorectal Cancer and Survival Times of Patients in Korea. Clin Gastroenterol Hepatol. 2019;17(4):786–8.
Hwang YJ, Kim N, Yun CY, Yoon H, Shin CM, Park YS, Son IT, Oh HK, Kim DW, Kang SB, et al. Validation of Administrative Big Database for Colorectal Cancer Searched by International Classification of Disease 10th Codes in Korean: A Retrospective Big-cohort Study. J Cancer Prev. 2018;23(4):183–90.
Hwang YJ, Park SM, Ahn S, Lee JC, Park YS, Kim N. Accuracy of an administrative database for pancreatic cancer by international classification of disease 10(th) codes: A retrospective large-cohort study. World J Gastroenterol. 2019;25(37):5619–29.
Wu MC, Tsou HK, Lin CL, Wei JC. Incidence and risk of sepsis following appendectomy: a nationwide population-based cohort study. Sci Rep. 2020;10(1):10171.
Jung KW, Won YJ, Kong HJ, Lee ES. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2016. Cancer Res Treat. 2019;51(2):417–30.
Collaborators GBDSC: The global, regional, and national burden of stomach cancer in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease study 2017. Lancet Gastroenterol Hepatol 2020, 5(1):42–54.
Park JM, Choi MG, Yang CW, Jung CK, Lee SK, Yoon AR, Kim YS, Chung IS. Increased incidence of gastric cancer in renal transplant recipients. J Clin Gastroenterol. 2012;46(10):e87-91.
Sarkio S, Rautelin H, Kyllonen L, Honkanen E, Salmela K, Halme L. Should Helicobacter pylori infection be treated before kidney transplantation? Nephrol Dial Transplant. 2001;16(10):2053–7.
Ueda Y, Chiba T. Helicobacter pylori in solid-organ transplant recipient. Curr Opin Organ Transplant. 2008;13(6):586–91.
Shield KD, Ferlay J, Jemal A, Sankaranarayanan R, Chaturvedi AK, Bray F, Soerjomataram I. The global incidence of lip, oral cavity, and pharyngeal cancers by subsite in 2012. CA Cancer J Clin. 2017;67(1):51–64.
Stewart JH, Vajdic CM, van Leeuwen MT, Amin J, Webster AC, Chapman JR, McDonald SP, Grulich AE, McCredie MR. The pattern of excess cancer in dialysis and transplantation. Nephrol Dial Transplant. 2009;24(10):3225–31.
Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur Urol. 2017;71(1):96–108.
Chiang YJ, Yang PS, Wang HH, Lin KJ, Liu KL, Chu SH, Hsieh CY. Urothelial cancer after renal transplantation: an update. Transplant Proc. 2012;44(3):744–5.
van Leeuwen MT, Webster AC, McCredie MR, Stewart JH, McDonald SP, Amin J, Kaldor JM, Chapman JR, Vajdic CM, Grulich AE. Effect of reduced immunosuppression after kidney transplant failure on risk of cancer: population based retrospective cohort study. BMJ. 2010;340: c570.
Ahn HS, Kim HJ, Welch HG. Korea’s thyroid-cancer “epidemic”–screening and overdiagnosis. N Engl J Med. 2014;371(19):1765–7.
de Fijter JW. Use of proliferation signal inhibitors in non-melanoma skin cancer following renal transplantation. Nephrol Dial Transplant. 2007;22(Suppl 1):i23-26.
Bjornsdottir HH, Rawshani A, Rawshani A, Franzen S, Svensson AM, Sattar N, Gudbjornsdottir S. A national observation study of cancer incidence and mortality risks in type 2 diabetes compared to the background population over time. Sci Rep. 2020;10(1):17376.
de Boer RA, Meijers WC, van der Meer P, van Veldhuisen DJ. Cancer and heart disease: associations and relations. Eur J Heart Fail. 2019;21(12):1515–25.
Manickavasagar R, Thuraisingham R. Post renal-transplant malignancy surveillance. Clin Med (Lond). 2020;20(2):142–5.
Disease K. Improving Global Outcomes Transplant Work G: KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant. 2009;9(Suppl 3):S1-155.
Acknowledgements
This study was performed using a database from the Health Review and Assessment Service (M20200312381).
Funding
None.
Author information
Authors and Affiliations
Contributions
JMC participated in research design, ethics approval, and supervision. HL managed the data and performed statistical analysis. SWJ and JMC interpreted the data. SWJ drafted the manuscript. SWJ and JMC revised the manuscript. All the authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Kyung Hee University Hospital at Gangdong (KHNMC 2020–03-031). This study analyzed deidentified HIRA data and the requirement for informed consent was therefore waived by the Institutional Review Board of Kyung Hee University Hospital at Gangdong. All methods were performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that there are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jung, S.W., Lee, H. & Cha, J.M. Risk of malignancy in kidney transplant recipients: a nationwide population-based cohort study. BMC Nephrol 23, 160 (2022). https://doi.org/10.1186/s12882-022-02796-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-022-02796-6