
Abstract
Background
Renal function is a key factor of cardiovascular disease. Carotid intima-media thickness (IMT) has been widely used as a marker of early subclinical atherosclerosis. The determinants of cystatin C, a novel marker of renal function, have not been extensively studied in the Asian population. This study aimed to assess the determinants of cystatin C and explore whether carotid thickening was associated with urinary albumin-creatinine ratio and cystatin C in community-living Taiwanese adults.
Methods
A cross-sectional study was conducted on participants from Taichung City, Taiwan. All the participants underwent carotid ultrasonography. Carotid IMT-mean and IMT-maximum were derived. Kidney biomarkers were measured on the basis of urinary albumin-to-creatinine ratio (ACR) and cystatin C. Multiple linear regression analysis was used.
Results
A total of 1032 individuals were recruited, and 469 (45.44%) of them were men. An increased cystatin C level was significantly associated with older age, male gender, lack of physical activity, low HDL cholesterol, abdominal obesity, high hs-CRP, and high ACR. The multivariate-adjusted mean carotid IMT-mean and IMT-maximum values significantly increased by 80.49 and 195.23 μm for every one unit of increase in cystatin C level and by 0.07 and 0.14 μm for every one unit of increase in ACR, respectively (all p < 0.001 except ACR on IMT-maximum with p < 0.01). Lack of physical activity, low HDL, abdominal obesity, high hs-CRP, and high ACR were the determinants of cystatin C.
Conclusion
Cystatin C and ACR were strongly and linearly associated with carotid thickening, a marker of subclinical atherosclerosis.
Similar content being viewed by others

Background
Cardiovascular disease (CVD) is one of the causes of morbidity and premature mortality and the main cause of death worldwide, including Taiwan. The development of metabolic syndrome, including the cluster of CVD risk factors, results from two determinants, namely, genetic influence and environments, which increases the risk of developing atherosclerosis. Renal function has been regarded as a risk factor of CVD [1, 2].
Cystatin C is considered as an ideal marker of renal function [3] and more precise than serum creatinine levels in detecting early kidney dysfunction [4, 5]. Plasma cystatin C measurement is superior to creatinine-based methods for estimating the glomerular filtration rate [3, 6] in terms of its greater sensitivity than creatinine as a predictor of cardiovascular risk and for the early diagnosis of early chronic renal disease. Cystatin C is linked to pathophysiological changes in the vascular wall [7, 8]. In addition to cystatin C, albuminuria is a renal marker associated with an increased risk of CVD. Albuminuria, a marker of kidney damage, is the consequence of albumin leakage across the glomerular podocyte filtration barrier into the urine and the increased excretion of urinary albumin. Albuminuria is also a marker of generalized endothelial dysfunction in which accelerated atherosclerosis [9] has been known as a sensitive prognostic marker to evaluate the increased risk of CVD [10, 11]. Urinary albumin-creatinine ratio (ACR) is a preferred approach for albuminuria detection.
Carotid intima-media thickness (IMT), the measurement of the intima and media layers of the artery, has been described as a quantitative measure of subclinical atherosclerosis [12]. A gradual increase in carotid IMT is characterized by changes in arterial wall vessels during atherosclerosis progression. Carotid IMT, which is used as a biomarker for the early clinical diagnosis of CVD, is one of the most commonly employed and well established for early surrogate biomarkers of atherosclerosis [13, 14] and has been reported to predict CVD and myocardial infarction [13, 15]. Recent studies on the association between cystatin C and carotid IMT have yielded inconsistent results [16,17,18,19,20,21,22,23,24,25,26]. Some prior research demonstrated that increased cystatin C is associated with carotid IMT [24]. On the contrary, no association between cystatin C and carotid IMT has been found in another study [22]. Among the investigations that confirmed an association between cystatin C and carotid IMT, only one study has been performed in the general population. The association between cystatin C and arteriosclerosis in adults residing in the community has been rarely discussed. Thus, this study evaluated whether independent cross-sectional associations existed between urinary ACR and cystatin C with subclinical atherosclerosis in participants of the Taichung Community Health Study (TCHS). This study also explored the determinants of cystatin C.
Methods
Study design and study subjects
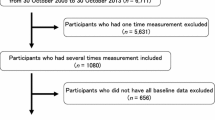
A community-based cross-sectional study was conducted in 2015. All participants from three studies on TCHS, TCHS for elders (TCHS-E), and TCHS for family members (TCHS-F) were contacted individually via a phone call and a letter to invite them to participate in this study, including providing extracranial carotid artery ultrasound measurement and a fasting blood sample. The TCHS, TCHS-E, and TCHS-F studies are described in the Supplementary Information for the Study Subjects. In brief, TCHS was a population-based prospective cohort study conducted in 2004. The sampling design was a two-stage approach, with each stage having a sampling rate proportional to size. The target population was defined as residents aged 40 years and over in Taichung City, Taiwan, in 2004. A total of 2359 participants were involved, with an overall response rate of 66.83%. In the second wave, 1666 participants were included, with a follow-up rate of 70.62%. A total of 1136 participants returned, with an overall follow-up rate of 50.8% in the third wave (2010–2013). TCHS-E was also a population-based cohort study. The study population included residents aged 65 years and over in eight Lis (administrative neighborhoods) in North District in Taichung City, Taiwan, in 2009. A total of 2750 subjects were eligible, and 1347 agreed to participate, with an overall response rate of 49.0%. After 1 year, 1078 subjects were followed up, with a follow-up rate of 81.3%. TCHS-F was a family study that aimed to examine the familiar aggregation of cardiovascular risk factors. In this family study, 807 families with at least one first-degree relative of participants from TCHS or TCHS-E were recruited. The inclusion criteria of TCHS-F were individuals who were spouses or first-degree blood relatives (parents, full siblings, and offspring) aged 20 years or over of the participants of TCHS or TCHS-E. A total of 1919 family members of TCHS or TCHS-E participated. In the present cross-sectional study, the cystatin C levels of 1039 study subjects who were participants of TCHS, TCHS-E, and TCHS-F studies and had their attendance in August 2016–April 2018 were measured because of the budget limit. Seven subjects with missing values were excluded from the analysis. This study was approved by the Human Research Committee of China Medical University Hospital (CMUH105-REC1–002), all methods were carried out in accordance with relevant guidelines and regulation, and informed consent was obtained from each participant.
Measurements
A standardized physical check-up procedure and a questionnaire were used to complete data collection. Sociodemographic factors included age and sex. Lifestyle behaviors included alcohol drinking, physical activity, and smoking. Disease histories of diabetes, hypertension, heart disease, hyperuricemia, hyperlipidemia, stroke, cancer, and medication history were obtained. Lifestyle behaviors and disease histories were categorized as “Yes” and “No” classes.
Anthropometric measurements and blood samples were obtained. Weight and height were measured using an autoanthropometer (super-view, HW-666). During measurement, the subjects were shoeless and wearing light clothing. Body mass index (BMI) was derived by dividing weight (kg) by (height)2 (m2). Waist circumference was measured as the midway point between the crest of the ilium and the inferior margin of the last rib in a horizontal plane while the participant was standing. WC was measured to the nearest 0.1 kg. Blood pressure was measured in a seated position by using an electronic device (OMRON, HEM-770A, Japan).
Blood was drawn in the morning after a 12-h overnight fasting with minimal trauma from an antecubital vein. Biochemical markers, including fasting plasma glucose, triglyceride, HDL (high density lipoprotein)-cholesterol, uric acid, urine albumin, and creatinine, were analyzed with a biochemical autoanalyzer (Beckman Coluter, Lx-20, USA) at the Clinical Laboratory Department of China Medical University Hospital. Fasting plasma glucose level was measured via a glucose oxidase method (Astra-8, Beckman, CA, USA). Urinary ACR was measured using the morning urine sample as a marker of the albumin excretion rate. Urinary ACR ranging from 30 mg g− 1 creatinine to 300 mg g− 1 creatinine was defined as microalbuminuria, while urinary ACR above 300 mg g− 1 was defined as macroalbuminuria. The hs-CRP (high sensitivity C-reactive protein) level was determined through nephelometry, a latex particle-enhanced immunoassay (TBA-200FR, Tokyo, Japan) with the inter- and intra-assay coefficient of variations of < 2.0 and 1.9%, respectively. The lower detection limit of the assay was 0.1 mg/L. Cystatin C was identified via a particle-enhanced immunonephelemetric assay (N Latex Cystatin C, Dade-Behring, Marburg, Germany) with a nephelometer (BNII, Dade Behring). The modified definition of metabolic syndrome as described in the Third Report of the National Cholesterol Education Program’s Adult Treatment Panel (ATP III) was used [27]. According to the ATP III, the metabolic syndrome components were as follows: hyperglycemia (fasting plasma glucose ≥110 mg/dl), hypertriglyceridemia (serum triglycerides ≥150 mg/dl), hypertension (blood pressure ≥ 130/85 mmHg), abdominal obesity (waist circumference > 90 cm in men and waist circumference > 80 cm in women), and low HDL cholesterol (serum HDL-cholesterol < 40 mg/dl in men and HDL-cholesterol < 50 mg/dl in women).
Extracranial carotid artery ultrasound measurement
The IMT measurements of all the study subjects were measured with the same machine (GE L7000, GE, Milwaukee, Wis., USA) under the standardized procedure. After resting for about 10 min in the supine position with their necks in a slight hyperextension, all the study subjects underwent carotid ultrasound examination with a 7.5 MHz probe to bilaterally scan the far and near walls of arterial segments and obtain the transverse and longitudinal (posterior oblique, lateral, and anterior oblique) views. Each ultrasound image, including atherosclerotic plaques and the intima-media complex thicknesses, was recorded in an online digital filing system via a computer. The arterial segments were as follows: (1) the proximal (first 1 cm) of the internal carotid arteries (ICAs); (2) 1–2 cm proximal to the tip of the flow divider into the right common carotid arteries (CCAs); and (3) the carotid bifurcations (bulb) beginning at the tip of the flow divider and extending 1 cm proximal to the flow divider tip. The maximal IMT of each segment at the CCA was derived from a minimum of three frames as the maximum IMT (segment-specific IMT-maximum) and mean IMT (segment-specific IMT-mean) of each segment by averaging these frames. The total carotid IMT (IMT-mean or IMT-maximum) was calculated as a composite measure (mean or maximum of the eight carotid sites) that combined the near and far walls of CCA IMT, bulb IMT, and ICA IMT of both sides of the neck. IMT-maximum was expressed as the mean of the maximum values of the eight carotid sites, while the IMT-mean was defined as the mean of the average values of the eight carotid sites. The IMT measurements were operated by two operators. The intra-operators reliability of IMT-mean for the first and second operators were 0.85 and 0.89, respectively; the intra-operators reliability of IMT-maximum were 0.85 and 0.97, respectively; and the inter-operators reliability of IMT-mean and IMT-maximum were both 0.88.
Statistical analysis
Simple descriptive analyses, such as proportion, mean, and standard deviation, were applied to analyze data when appropriate. The differences between cystatin C and ACR groups were evaluated through analysis of variance. For categorical variables, comparisons were assessed via a Chi-square or Fisher’s exact test. Multiple linear regression models were used on the basis of cross-sectional data to investigate the determinants of cystatin C and whether cystatin C and ACR were associated with carotid IMT after the metabolic syndrome components, inflammation markers, and lifestyle behaviors that were significantly associated with carotid IMT were considered. In order to estimate the independent association between cystatin C or ACR with carotid IMT, cystatin C and ACR were entered into the multivariate models simultaneously. All analyses were conducted with SAS version 9.4 (SAS, Cary, NC). P values were two tailed, and significance level was set at 0.05.
Results
A total of 1032 subjects were analyzed between August 2016 and December 2018. About half of the participants were female (55%). The mean ages of men and women were 69.80 years (standard deviation = 9.71 years) and 66.07 years (9.44 years), respectively. The characteristics of the study subjects across the tertiles of cystatin C and albuminuria status are presented in Table 1. The highest tertile of cystain C was associated with the high proportions of men, smoking, lack of physical activity, hyperglycemia, hypertriglyceridemia, hypertension, low HDL cholesterol, and high mean values of age, fasting insulin, hs-CRP, carotid IMT-mean, and IMT-maximum. The results of the comparison of the characteristics of the three albuminuria groups (normal albuminuria [< 30 mg/g], microalbuminuria [30–300 mg/g], and macroalbuminuria [≥300 mg/g]) are shown in Table 1. The values of carotid IMT-mean and IMT-maximum in the normal group were significantly lower than those in the microalbuminuria and macroabluminuria groups.
Table 2 presents the multiple linear regression models used to explore the determinants of cystatin C. When age and gender were entered into the model, 12.2% of the variation in cystatin C was explained, and both age and gender were significantly associated with cystatin C. When the lifestyle behaviors of alcohol drinking, smoking, and physical activity were further considered, physical activity was the only significant variable. The effect of age and gender remained similar and explained 1.1% of additional variation in cystatin C. When metabolic syndrome components were entered into the model, abdominal obesity and low HDL cholesterol were the two significant variables, and the effect of physical activity was attenuated but was still significant. When the biochemical lab parameters were included, hs-CRP and ACR were the significant variables that were associated with cystatin C, and the variation in cystatin C improved from 15.0 to 34.3%.
Table 3 shows the adjusted means of IMT-mean IMT-maximum across various cystatin C levels and albuminuria status. After adjustments for age and sex were made, the mean carotid IMT-mean and IMT-maximum were significantly different in cystatin C levels and albuminuria status. After the lifestyle behaviors of smoking, alcohol drinking, and physical activity were further considered, the results remained similar. After further adjustments for metabolic syndrome components, fasting insulin, and hs-CRP were made, the differences in the IMT-mean of the cystatin C levels became borderline significant and remained significant across albuminuria categories. The following adjusted mean values (95% confidence interval) were obtained on the basis of the tertiles of cystatin C: for the carotid IMT-mean, 1069.09 (1021.26, 1116.92), 1075.83 (1030.80, 1120.87), and 1112.06 (1066.09, 1158.04); for IMT-maximum, 1790.81 (1670.17, 1911.46), 1797.65 (1684.04, 1911.25), and 1937.21 (1821.24, 2053.18); for the IMT-mean of the ACR groups (normal albuminuria, microalbuminuria, and macroalbuminuria), 1077.27 (1036.05, 1118.50), 1123.70 (1066.55, 1180.84), and 1201.22 (1097.91, 1304.52); and for the IMT-maximum, 1819.39 (1715.07, 1923.70), 1974.65 (1830.06, 2119.24), and 2013.4 (1752.02, 2274.77).
Table 4 lists the estimated differences in the carotid IMT-mean and IMT-maximum. The carotid IMT-mean and IMT-maximum values from the first to the third tertile groups of cystatin C and from the normal to the macroalbuminuria group increased. The multivariate-adjusted mean carotid IMT-mean and IMT-maximum values significantly increased by 80.49 and 195.23 μm for every one unit increase in cystatin C, respectively, and by 0.07 and 0.14 μm for every one unit increase in ACR (all p < 0.001 except ACR on IMT-maximum with p < 0.01), respectively.
Discussion
In this cross-sectional study performed with 1032 community-dwelling adults, older age, male gender, lack of physical activity, low HDL cholesterol, abdominal obesity, high hs-CRP, and high ACR were associated with increased cystatin C levels. High cystatin C and ACR levels were independently associated with an increase in carotid IMT-mean and IMT-maximum measurements.
Our findings showed that the metabolic components of abdominal obesity and low HDL cholesterol were determinants of cystatin C, and they were consistent with those of prior studies showing that cystatin C is associated with metabolic syndrome [28, 29], obesity determined by BMI [30,31,32], and HDL [33]. A cross-sectional study on 925 patients with dyslipidemia and 26% prevalence of metabolic syndrome has revealed that cystatin C is associated with metabolic syndrome in these patients [28]. The Chennai Urban Rural Epidemiology Study, a population-based study in southern India, included 40 subjects with four or five metabolic components, 40 subjects with three metabolic components, 37 subjects with two metabolic components, 44 subjects with one metabolic component, and 43 subjects without a metabolic component. Their findings indicated that cystatin C is linearly associated with the number of metabolic components [28, 29]. In a national cross-sectional study from the Third National Health and Nutrition Examination Survey on 5083 participants with a normal renal function defined by an estimated glomerular filtration rate of ≥60 mL/min/1.73 m2 without albuminuria, the association between BMI and increased serum cystatin C levels is explored, revealing a graded relationship between higher BMI and increased serum cystatin C [30]. A cross-sectional study on 2583 participants without clinically recognized chronic kidney disease from the National Health and Nutrition Examination Survey 1999 to 2002 identified the association between obesity determined by BMI and cystatin C independent of age, sex, race, education, smoking, alcohol intake, cholesterol, and CRP levels [32]. In a cross-sectional study on 159 community-living elderly Japanese women, HDL is negatively linked with cystatin C after adjustments for creatinine-based estimated glomerular filtration rate are made [33]. According to the definition of metabolic syndrome by the Third Report of the National Cholesterol Education Program’s Adult Treatment Panel [27], abdominal obesity should be determined by waist circumference. However, most prior studies adopted obesity as determined by BMI by estimating the overall body fat mass. Our study demonstrated that abdominal obesity, as determined by waist circumference, was correlated with cystatin C.
The pathogenesis of CVD appears to be multifactorial, involving genetic and acquired factors that play a key role in the pathway of inflammation that leads to CVD. Inflammation is crucial in various endothelial function aspects, which are critical to an early stage of atherosclerosis and its associated clinical risk factors [34]. Our study found that cystatin C was linked with hs-CRP, thereby suggesting that cystatin C was involved in the pathway of the potential pathogenesis of CVD; this result can be supported by previous findings, which indicated that cystatin C is a relevant marker of the risk of CVD among relatively healthy middle-aged adults [35], predicts incident type 2 diabetes [36] and progression from normal fasting plasma glucose to prediabetes [37], and predicts the cardiovascular risk in elderly persons [38, 39] and adults of the general population [40].
Increased cystatin C levels are associated with carotid IMT in a multi-ethnic study on atherosclerosis [24], in the general population [23], in the health check-up population [20], in postmenopausal women [21], in metabolic syndrome patients [19], in patients with hypertension [16, 17, 25], and in patients with type 2 diabetes [26, 41]. By contrast, a study investigated 446 Japanese adults without chronic kidney disease and proteinuria and did not find the relationship of cystatin C and carotid IMT [22]. In a study on a healthy Chinese population with a normal renal function and without cardiovascular disease, cystatin C is associated with carotid IMT, but this association is explained when BMI, systolic and diastolic blood pressure, lipid profiles, albumin, fasting blood glucose, and inflammatory markers are considered [18]. A study on African descent has revealed that cystatin C is not associated with carotid IMT beyond traditional cardiovascular risk factors [42]. The association between cystatin C and arteriosclerosis in middle-aged adults has been less consistent. Thus, we measured cystatin C and investigated its association with carotid IMT in TCHS. Our study supported previous results, which indicated that cystatin C can be used as a precise indicator to help the early diagnosis of atherosclerosis in community-based adults.
Our study found that ACR can explain the variation in cystatin C in this community-based sample, but both are independently associated with carotid IMT. Prior studies explored the associations between renal biomarkers and carotid IMT in the general population by focusing on the measures of the blood urea nitrogen [24] and creatinine-based estimated glomerular filtration rate [19, 24]. Our study reported an association between ACR and carotid IMT values in the participants of the general population, and this result was consistent with previous findings in patients with type 2 diabetes [43, 44].
In order to evaluate whether serum cystatin C is more important than creatinine or creatinine-based estimated glomerular filtration rate (eGFR) in term of capturing their relationship with IMT, we performed additional analysis by adding the eGFR and creatinine separately into the multivariate models with cystatin C and ACR (Supplemental Tables 1 and 2). The reason why we cannot enter eGFR and serum creatinine into the multivariate models at the same time is because eGFR is derived from serum creatinine and they shared too much common information. We found cystatin C was significantly associated with IMT-maximum when eGFR or creatinine was considered while either eGFR or creatinine was not associated with IMT-maximum. Cystatin C was associated with IMT-mean at borderline significant when creatinine was considered but cystatin C was not associated with IMT-mean when eGFR was taken into account. Our findings support prior studies that cystatin C may be a better measurement than creatinine-based methods in terms of capturing its relation to carotid IMT.
The strengths of this study included a well-defined sample of adults from the general population in Taiwan by using standard questionnaires and instruments. A complete physical check-up was taken by all the participants. Vigorous quality assurance programs and a strict personnel training process were set up. Thus, the percentage of missing data was low (< 0.5%). Our study also had standard laboratory approaches for glucose and lipid measurements within a central clinical lab for the same assays.
This study also had three notable limitations. First, the use of a cross-sectional study design would be relevant to the interpretation of our results; thus, we could not infer the causal pathways underlying the observed relationships. Second, the study was restricted to the first 1032 participants, and a potential selection bias might exist. The demographic characteristics of the individuals with and without cystatin C measurement were assessed by comparing age and gender for the possibility of selection bias, and similar distributions were found. Given that age and gender distributions did not differ, this kind of selection error might be random. Thus, the resulting bias in the effect might be negligible, and it could pose a low threat to the internal validity of our study findings. Lastly, our study was based on a Taiwanese population with main Han Chinese. Such a selection bias may limit our findings to be generalized to other ethnic populations, but they may be generalizable to other Chinese populations having similar characteristics as our study sample.
Conclusions
In a cross-sectional study on 1032 community-living Taiwanese adults, older age, male gender, lack of physical activity, low HDL cholesterol, abdominal obesity, high hs-CRP, and high ACR were independently linked with a high cystatin C level. Increased serum cystatin C and ACR were linearly associated with carotid IMT measurements. The early detection of subclinical atherosclerosis might target those with increased cystatin C and ACR levels. Further research is warranted to assess whether reducing the risk factors of increased serum cystatin C favorably affected serum cystatin C levels and subclinical atherosclerosis development.
Availability of data and materials
The dataset analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CVD:
-
Cardiovascular disease
- ACR:
-
Albumin-creatinine ratio
- IMT:
-
Intima-media thickness
- TCHS:
-
Taichung Community Health Study
- TCHS-E:
-
Taichung Community Health Study for elders
- TCHS-:
-
Taichung Community Health Study for family members
- BMI:
-
Body mass index
- HDL:
-
High density lipoprotein
- hs-CRP:
-
High sensitivity C-reactive protein
- ATP III:
-
Third Report of the National Cholesterol Education Program’s Adult Treatment Panel
- ICA:
-
Internal carotid arteries
- CCAs:
-
Common carotid arteries
- Bulb:
-
Bifurcations
- eGFR:
-
Estimated glomerular filtration rate
References
Makin SD, Cook FA, Dennis MS, Wardlaw JM. Cerebral small vessel disease and renal function: systematic review and meta-analysis. Cerebrovasc Dis. 2015;39(1):39–52.
Tonkin AM, Blankenberg S, Kirby A, Zeller T, Colquhoun DM, Funke-Kaiser A, Hague W, Hunt D, Keech AC, Nestel P, et al. Biomarkers in stable coronary heart disease, their modulation and cardiovascular risk: the LIPID biomarker study. Int J Cardiol. 2015;201:499–507.
Dharnidharka VR, Kwon C, Stevens G. Serum cystatin C is superior to serum creatinine as a marker of kidney function: a meta-analysis. Am J Kidney Dis. 2002;40(2):221–6.
Newman DJ, Thakkar H, Edwards RG, Wilkie M, White T, Grubb AO, Price CP. Serum cystatin C measured by automated immunoassay: a more sensitive marker of changes in GFR than serum creatinine. Kidney Int. 1995;47(1):312–8.
Coll E, Botey A, Alvarez L, Poch E, Quinto L, Saurina A, Vera M, Piera C, Darnell A. Serum cystatin C as a new marker for noninvasive estimation of glomerular filtration rate and as a marker for early renal impairment. Am J Kidney Dis. 2000;36(1):29–34.
Roos JF, Doust J, Tett SE, Kirkpatrick CM. Diagnostic accuracy of cystatin C compared to serum creatinine for the estimation of renal dysfunction in adults and children--a meta-analysis. Clin Biochem. 2007;40(5–6):383–91.
Rautou PE, Vion AC, Amabile N, Chironi G, Simon A, Tedgui A, Boulanger CM. Microparticles, vascular function, and atherothrombosis. Circ Res. 2011;109(5):593–606.
VanWijk MJ, VanBavel E, Sturk A, Nieuwland R. Microparticles in cardiovascular diseases. Cardiovasc Res. 2003;59(2):277–87.
Brevetti G, Schiano V, Chiariello M. Endothelial dysfunction: a key to the pathophysiology and natural history of peripheral arterial disease? Atherosclerosis. 2008;197(1):1–11.
Hillege HL, Janssen WM, Bak AA, Diercks GF, Grobbee DE, Crijns HJ, Van Gilst WH, De Zeeuw D, De Jong PE. Microalbuminuria is common, also in a nondiabetic, nonhypertensive population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity. J Intern Med. 2001;249(6):519–26.
Weiner DE, Tighiouart H, Amin MG, Stark PC, MacLeod B, Griffith JL, Salem DN, Levey AS, Sarnak MJ. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004;15(5):1307–15.
Annest JL, Sing CF, Biron P, Mongeau JG. Familial aggregation of blood pressure and weight in adoptive families. II. Estimation of the relative contributions of genetic and common environmental factors to blood pressure correlations between family members. Am J Epidemiol. 1979;110(4):492–503.
Nezu T, Hosomi N, Aoki S, Matsumoto M. Carotid intima-media thickness for atherosclerosis. J Atheroscler Thromb. 2016;23(1):18–31.
O'Leary DH, Polak JF. Intima-media thickness: a tool for atherosclerosis imaging and event prediction. Am J Cardiol. 2002;90(10c):18l–21l.
van der Meer IM, Bots ML, Hofman A, del Sol AI, van der Kuip DA, Witteman JC. Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: the Rotterdam study. Circulation. 2004;109(9):1089–94.
Cabarkapa V, Ilincic B, Deric M, Vucaj Cirilovic V, Kresoja M, Zeravica R, Sakac V. Cystatin C, vascular biomarkers and measured glomerular filtration rate in patients with unresponsive hypertensive phenotype: a pilot study. Ren Fail. 2017;39(1):203–10.
Dzielinska Z, Januszewicz A, Wiecek A, Prejbisz A, Zielinski T, Chudek J, Makowiecka-Ciesla M, Demkow M, Tyczynski P, Januszewicz M, et al. Reduced kidney function estimated by cystatin C and clinical outcomes in hypertensive patients with coronary artery disease: association with homocysteine and other cardiovascular risk factors. Kidney Blood Press Res. 2010;33(2):139–48.
Han L, Bai X, Lin H, Sun X, Chen XM. Lack of independent relationship between age-related kidney function decline and carotid intima-media thickness in a healthy Chinese population. Nephrol Dial Transplant. 2010;25(6):1859–65.
Huang R, Gu J, Cao Q, Ma J, Gu W, Fan Z. The association between serum cystatin C and carotid intima-media thickness in metabolic syndrome patients with normal estimated glomerular filtration rate. Clin Chim Acta. 2015;448:170–3.
Kobayashi T, Yokokawa H, Fujibayashi K, Haniu T, Hisaoka T, Fukuda H, Naito T. Association between high cystatin C levels and carotid atherosclerosis. World J Cardiol. 2017;9(2):174–81.
Lambrinoudaki I, Tourlakis D, Armeni E, Kaparos G, Rizos D, Augoulea A, Alexandrou A, Kreatsa M, Deligeoroglou E, Stamatelopoulos K. Variations in glomerular filtration rate are associated with subclinical atherosclerosis in healthy postmenopausal women. Menopause. 2015;22(3):317–24.
Yamashita H, Nishino T, Obata Y, Nakazato M, Inoue K, Furusu A, Takamura N, Maeda T, Ozono Y, Kohno S. Association between cystatin C and arteriosclerosis in the absence of chronic kidney disease. J Atheroscler Thromb. 2013;20(6):548–56.
Zhu Y, Zhang HP, Wang YC, Ren TT, Li J, Xu ML, Wang XQ, Liu FC, Lau A, Wen YF. Serum cystatin C level is associated with carotid intima-media thickening and plaque. Scand J Clin Lab Invest. 2015;75(3):265–72.
Bui AL, Katz R, Kestenbaum B, de Boer IH, Fried LF, Polak JF, Wasserman BA, Sarnak MJ, Siscovick D, Shlipak MG. Cystatin C and carotid intima-media thickness in asymptomatic adults: the multi-ethnic study of atherosclerosis (MESA). Am J Kidney Dis. 2009;53(3):389–98.
Watanabe S, Okura T, Liu J, Miyoshi K, Fukuoka T, Hiwada K, Higaki J. Serum cystatin C level is a marker of end-organ damage in patients with essential hypertension. Hypertens Res. 2003;26(11):895–9.
Zang L, Fu P, Liu F, Wu M, Huang YQ, Li L, Zang J. The correlation of serum cystatin C level with the severity of carotid atherosclerosis in patients with type 2 diabetes mellitus. Sichuan Da Xue Xue Bao Yi Xue Ban. 2012;43(6):882–7.
Expert Panel on Detection, E. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). Jama. 2001;285(19):2486–97.
Servais A, Giral P, Bernard M, Bruckert E, Deray G, Isnard Bagnis C. Is serum cystatin-C a reliable marker for metabolic syndrome? Am J Med. 2008;121(5):426–32.
Surendar J, Indulekha K, Aravindhan V, Ganesan A, Mohan V. Association of cystatin-C with metabolic syndrome in normal glucose-tolerant subjects (CURES-97). Diabetes Technol Ther. 2010;12(11):907–12.
Muntner P, Winston J, Uribarri J, Mann D, Fox CS. Overweight, obesity, and elevated serum cystatin C levels in adults in the United States. Am J Med. 2008;121(4):341–8.
Parikh NI, Hwang SJ, Yang Q, Larson MG, Guo CY, Robins SJ, Sutherland P, Benjamin EJ, Levy D, Fox CS. Clinical correlates and heritability of cystatin C (from the Framingham offspring study). Am J Cardiol. 2008;102(9):1194–8.
Shankar A, Teppala S. Relationship between body mass index and high cystatin levels among US adults. J Clin Hypertens (Greenwich). 2011;13(12):925–30.
Tsuboi A, Takeuchi M, Terazawa-Watanabe M, Fukuo K, Kazumi T. Association of cystatin C with leptin and TNF-alpha in elderly Japanese women. Asia Pac J Clin Nutr. 2015;24(4):626–32.
Wilcox G. Insulin and insulin resistance. Clin Biochem Rev. 2005;26(2):19–39.
Kestenbaum B, Rudser KD, de Boer IH, Peralta CA, Fried LF, Shlipak MG, Palmas W, Stehman-Breen C, Siscovick DS. Differences in kidney function and incident hypertension: the multi-ethnic study of atherosclerosis. Ann Intern Med. 2008;148(7):501–8.
Sahakyan K, Lee KE, Shankar A, Klein R. Serum cystatin C and the incidence of type 2 diabetes mellitus. Diabetologia. 2011;54(6):1335–40.
Donahue RP, Stranges S, Rejman K, Rafalson LB, Dmochowski J, Trevisan M. Elevated cystatin C concentration and progression to pre-diabetes: the Western New York study. Diabetes Care. 2007;30(7):1724–9.
Shlipak MG, Katz R, Sarnak MJ, Fried LF, Newman AB, Stehman-Breen C, Seliger SL, Kestenbaum B, Psaty B, Tracy RP, et al. Cystatin C and prognosis for cardiovascular and kidney outcomes in elderly persons without chronic kidney disease. Ann Intern Med. 2006;145(4):237–46.
Shlipak MG, Sarnak MJ, Katz R, Fried LF, Seliger SL, Newman AB, Siscovick DS, Stehman-Breen C. Cystatin C and the risk of death and cardiovascular events among elderly persons. N Engl J Med. 2005;352(20):2049–60.
Cepeda J, Tranche-Iparraguirre S, Marin-Iranzo R, Fernandez-Rodriguez E, Riesgo-Garcia A, Garcia-Casas J, Hevia-Rodriguez E. Cystatin C and cardiovascular risk in the general population. Rev Esp Cardiol. 2010;63(4):415–22.
Kaneko R, Sawada S, Tokita A, Honkura R, Tamura N, Kodama S, Izumi T, Takahashi K, Uno K, Imai J, et al. Serum cystatin C level is associated with carotid arterial wall elasticity in subjects with type 2 diabetes mellitus: a potential marker of early-stage atherosclerosis. Diabetes Res Clin Pract. 2018;139:43–51.
Rodondi N, Yerly P, Gabriel A, Riesen WF, Burnier M, Paccaud F, Bovet P. Microalbuminuria, but not cystatin C, is associated with carotid atherosclerosis in middle-aged adults. Nephrol Dial Transplant. 2007;22(4):1107–14.
Huang Y, Chen Y, Xu M, Gu W, Bi Y, Li X, Ning G. Low-grade albuminuria is associated with carotid intima-media thickness in Chinese type 2 diabetic patients. J Clin Endocrinol Metab. 2010;95(11):5122–8.
Li MF, Tu YF, Li LX, Lu JX, Dong XH, Yu LB, Zhang R, Bao YQ, Jia WP, Hu RM. Low-grade albuminuria is associated with early but not late carotid atherosclerotic lesions in community-based patients with type 2 diabetes. Cardiovasc Diabetol. 2013;12:110.
Acknowledgements
Not applicable.
Funding
This study was supported primarily by the Ministry of Science and Technology of Taiwan (MOST 104–2314-B-039-016, MOST 105–2314-B-039-021-MY3, MOST 105–2314-B-039-025-MY3, MOST 107–2314-B-039-049, MOST 108–2314-B-039-039, MOST 108–2314-B-039-035-MY3 and MOST 108–2314-B-039-031-MY2) and China Medical University (CMU108-AWARD-02). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
CSL, TCL and CCL contributed to the conception, design of the work, and drafted the paper. YCG, CHLin, WYL, CHLiu, MCW and CWY contributed to acquisition, interpretation and critically revised manuscript. CIL and SYY contributed to analysis of data. All authors critically revised the manuscript for important intellectual content, approved the final version submitted and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Human Research Committee (HRC) of China Medical University Hospital (CMUH105-REC1–002). Written informed consent was obtained from each participant for the first and second waves of data collection.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Time points of the data collection for the Taichung Community Health Study (TCHS), Taichung Community Health Study-Elder (TCHS-E), and Family Study of TCHS and TCHS-E. Table S1. Multivariate analysis of carotid intima-media thickness for serum cystain C, albumin-to-creatinine ration, and estimated glomerular filtration rate along with traditional risk factors. Table S2. Multivariate analysis of carotid intima-media thickness for serum cystain C, albumin-to-creatinine ration, and serum creatinine along with traditional risk factors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, CS., Li, CI., Guo, YC. et al. Independent associations of urinary albumin-to-creatinine ratio and serum cystatin C with carotid intima-media thickness in community-living Taiwanese adults. BMC Nephrol 21, 454 (2020). https://doi.org/10.1186/s12882-020-02123-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-020-02123-x