
Abstract
Background
Cerebral folate deficiency (CFD) is a neurological disease, hallmarked by remarkable low concentrations of 5-methyltetrahydrofolic acid (5-MTHF) in cerebrospinal fluid (CSF). The primary causes of CFD include the presence of folate receptor (FR) autoantibodies, defects of FR encoding gene FOLR1, mitochondrial diseases and congenital abnormalities in folate metabolism.
Case presentation
Here we first present a Chinese male CFD patient whose seizure onset at 2 years old with convulsive status epilepticus. Magnetic Resonance Imaging (MRI) revealed the development of encephalomalacia, laminar necrosis in multiple lobes of the brain and cerebellar atrophy. Whole Exome Sequencing (WES) uncovered a homozygous missense variant of c.524G > T (p.C175F) in FOLR1 gene. Further laboratory tests demonstrated the extremely low level of 5-MTHF in the CSF from this patient, which was attributed to cerebral folate transport deficiency. Following the intravenous and oral treatment of calcium folinate, the concentrations of 5-MTHF in CSF were recovered to the normal range and seizure symptoms were relieved as well.
Conclusions
One novel variation of FOLR1 was firstly identified from a Chinese male patient with tonic-clonic seizures, developmental delay, and ataxia. The WES and laboratory results elucidated the etiology of the symptoms. Clinical outcomes were improved by early diagnosis and proper treatment.
Similar content being viewed by others


Background
As defined in 2004 by Ramaekers and Blau, Cerebral Folate Deficiency (CFD) encompasses a collection of neurological syndromes associated with low cerebrospinal fluid (CSF) concentrations of 5-methyltetrahydrofolate (5-MTHF), the normal folate metabolism in nervous system [1]. The circumstantial evidence show that CFD is caused by congenital metabolic disorders and the acquired folic acid deficiency [2, 3]. The most common cause of CFD is the presence of folate receptor (FR) autoantibodies [4]. In addition, defects of FR encoding gene FOLR1, mitochondrial diseases and congenital abnormalities in folate metabolism could also lead to CFD. FOLR1 (OMIM#613068), located in the long arm of chromosome 11, encodes for folate receptor α (FRα) [5]. Binding of FRα with 5-MTHF in high affinity is essential for the transportation of folate to the brain [6, 7]. Thus, pathogenic variants of FOLR1 could result in brain-specific 5-MTHF deficiency, and ultimately cause a series of neuropsychiatric symptoms [5]. Normally, the onset of CFD caused by mutated FOLR1 begins from late infancy [8], with the major clinical manifestations including developmental retardation, dyskinesia, epileptic seizure, leukodystrophy and slow EEG background activity. In infant patients, 5-MTHF concentration in cerebrospinal fluid is also extremely low, but remains normal in peripheral nervous system, indicating that the cerebral 5-MTHF deficiency is the underlying mechanism for infant CFD.
Case presentation
Patient
The Chinese patient was born at full term through normal vaginal delivery, weighting 3.25 kg that fell in the normal range of newborn weights. He showed developmental delay and mental retardation since one and half years old. He was able to raise his head at 3 months, sit at 6 ~ 7 months, walk at 24 months, and learn limited vocabulary at 12 months. The patient was in poor physical health since he was 2 years old.
At 2 years of age, the patient started to have tonic-clonic seizures that lasted for 20–30 min with high fever (39 degrees Celsius) and was initially diagnosed as febrile seizure at local hospital. The patient was treated with anticonvulsive medications. The symptoms were relieved afterwards. However, a similar yet more severe symptoms appeared around age of four. Following similar treatments, the patient was transferred to another hospital to seek out a detailed clinical examination. CT scan of brain did not detect lesions. The patient was subsequently diagnosed with viral meningitis treated with anti-virus medicine. At the age of 6 years and 9 months, the symptom relapsed. The patient manifested vomiting, headache, tonic-clonic seizure, symptomatic generalized epilepsy that could last for half an hour. The patient was intubated and treated with the combination of antibiotics, phenobarbitone and sodium valproate.
Although the symptoms were relieved to some extent when the patient took sodium valproate at dose of 0.2 g Tid (26 mg/kg/d), the etiology of the symptoms remained unknown. Therefore, at age of 6 years and 11 months, after about 4 years of repeatedly suffering from status epilepticus, the patient was referred to Xiangya Hospital, Central South University, Hunan Province, China. The detailed neurological exams showed that the patient clinically manifested global developmental delay, slurred speech, hyperactivity, sialorrhea, difficulty in managing behavior, unsteady gait, hypotonia. His head circumference was 46 cm (less than the 3rd percentile). An extensive laboratory and genetic analysis were performed to uncover the etiology of his disease.
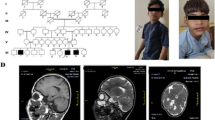
We performed brain MRI, diffusion weighted imaging (DWI). First, we found encephalomalacia and laminar necrosis in the brain left parietotemporal lobe, hippocampus and bilateral frontal lobe with diffuse white matter disorder (Fig. 1a). Second, cerebellar atrophy was also diagnosed from the brain scan (Fig. 1b). No abnormality was identified in the craniocerebral MRA scan. Clinical data of the family were collected and analyzed under the approval by the Ethics Committee Xiangya Hospital, Central South University. Informed consent was obtained from the parents of this proband.

Enhanced Brain MRI of a 6 years and 11 months old male patient. a MRI image of brain scan showed encephalomalacia and laminar necrosis with diffuse white matter disorder. b MRI scan of the brain demonstrated cerebellar atrophy in the patient
Genetic analysis
Whole exome sequencing (WES) was performed to search for potential pathogenic variants in an unbiased way. Genomic DNA was extracted from peripheral blood of the proband and his parents as previously described [8]. The putative mutations in Genomic DNA were subsequently screened by WES. Sequence variants were checked with population databases gnomAD (http://gnomad.broadinstitute.org/) and evaluated using multiple bioinformatic programs. Variant pathogenicity was interpreted according to the American College of Medical Genetics (ACMG) guidelines [9]. The variant was further confirmed by Sanger sequencing.
A novel variant c.524G > T (p.C175F) in folate receptor alpha (FOLR1) was identified. The Sanger sequencing confirmed the homozygous state of the variant in the affected individual, with the parents of being the heterozygous carrier (Fig. 2a). The variant was absent from population database gnomAD. Multiple bioinformatic analysis results (Polyphen2 score 0.995, probably damaging; Mutation Taster score 0.998, disease causing; and SIFT score 0, deleterious) indicated that the variant was deleterious.

Whole-exome sequencing (WES) and Sanger sequencing revealed missense variant of c.524G > T (p.C175F) in FOLR1 gene. a Homozygous variant in proband and heterozygous variant in his parents were identified. b Evolutionary conservation of cysteine residue at position 175 (red box) in the FOLR1 gene among species. wt, wildtype
Further diagnostic assessment
Laboratory blood routine tests revealed the total folate was 2.20 μg/L, lower than the minimal normal density of (3 μg/L) and the intracellular folate was 82.66 μg/L, lower than minimal normal range (93 μg/L).
Further examination revealed that the patient had almost undetectable levels of CSF 5-MTHF. The average concentration of 5-MTHF was 1.38 nmol/L, which is dramatically lower than the normal concentrations (60 ~ 210 nmol/L) for 6 ~ 15 years old children. The results indicated the cerebral folate deficiency. Taken together, laboratory results and WES analysis demonstrated that the mutation in FOLR1 and therefore the CSF 5-MTHF deficiency serves as the major etiology of patient’s symptoms.
Treatment
We devised the following treatment procedures based on genetic and laboratory test results: calcium folinate was given to the patient by intravenous (iv) injection at dosage of 2 mg/kg/d for 1 week, and adjusted to 6 mg/kg/d by oral administration, and gradually increased to 11 mg/kg/d orally at last. The CSF-5MTHF concentration was monitored closely during the treatment with calcium folinate. We gradually reduced the supplement of antiepileptic drugs (AEDs) until the patient was seizure free at the end. After 2 months of treatment, the CSF 5-MTHF concentration was elevated to 36.24 nmol/L, and 6 months later, the CSF 5-MTHF concentration was increased to 78.76 nmol/L that fell into the normal range of 60 ~ 210 nmol/L for 6 ~ 15 years old children. Besides, the symptoms including unsteady gait, failure to hold objects readily, epileptic seizure, etc. were considerably improved. Furthermore, after the treatment, seizure no longer concomitantly happened with fever.
Conclusions and discussion
In this report, we documented a first case of CFD patient in China caused by a novel mutation of FOLR1 gene (Fig. 1a). The young patient had been transferred between hospitals and the symptoms relapsed frequently prior to the elucidation of the underlying cause of his symptoms. The elaboration of the association between the mutation of FOLR1 gene and the clinical manifestations greatly expedited the treatment of CFD in this case.
FOLR1 is glycophosphatidylinositol (GPI)-anchored cell membrane protein, which regulates folate transport into the cells [6]. Chen et al. studied the crystal structure of human FOLR1 in complex with folic acid at 2.8 Å resolution [7]. Another group determined discrete structural conformations dependent on pH changes [10]. No direct evidence has been found to support that the novel variant c.524G > T (p.C175F) is involved in ligand binding. However, C175 is conserved among different species, and clinical data shown in this study demonstrated the importance of this residue. Possibly, mutation of this site will somehow sabotage the protein function. The further experiments will shed light on how this variant affects FOLR1 function as well as folate binding ability.
Pathogenic variants attributed to neurological disorders have been recovered in FOLR1 gene locus [2, 5, 8, 10, 11]. Homozygous mutations or compound heterozygous mutations led to autosomal recessive disorders, while a homozygous 18-bp in-frame duplication in FOLR1 gene also linked to neurodegeneration [5]. It transpires that patients carrying FOLR1 mutations exclusively end up with substantial low concentrations of CSF 5-MTHF (≤ 5 nmol/L), which lead to multiple brain lesions as revealed by neuroimaging studies. By reviewing pertinent literatures, we summarized all existing 15 variants from 23 patients in Fig. 3 [2, 5, 8, 10, 12,13,14,15,16,17]. In this case, we added a novel homozygous p.C175F variant in FOLR1 genotype spectrum. Alignment of the protein sequences of human FOLR1 with those from other organisms shows that the residue C175 is conserved across different species (Fig. 2b), implying that this site is critical for normal protein function and mutant protein may be defective in 5-MTHF binding and translocation. To improve the low concentrations of 5-MTHF caused by p.C175F variant, we deployed calcium folinate, the racemic stable form of folate, through oral or iv administration [18]. The treatment regime alleviated the symptoms efficiently. Given that the overdose of folic acid treatment could cause neurotoxicity [19], it is imperative to distinguish folinic acid from folic acid, and the latter may deteriorate the patient symptoms by sequestration of folic receptors through tight binding. In this respect, we meticulously monitored the changes in CSF 5-MTHF concentrations to avoid any side effect of the treatment.

Lollipop graph shows mutations in FOLR1 gene reported in literatures. Red star indicates the variant identified in this study. Green dots: missense mutation; Red dots: inframe mutation; Blue dots: Truncating mutation. Green bar: Folate receptor family domain where folate binds. Note: g.3576 T > G splice mutation (from ref. [8]) is not included in this graph due to its being out of the scope after re-annotation
In conclusion, the understanding of the genetic basis of frequently relapsed epileptic syndrome is critical for devising an effective treatment. This could be a tremendous benefit to the young patient, because the earlier the effective treatment is applied, the better recovery can be.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Data has been deposited and is publicly available in NCBI SRA database at weblink: https://www.ncbi.nlm.nih.gov/Traces/study/?acc=PRJNA672777
Abbreviations
- CFD:
-
Cerebral folate deficiency
- 5-MTHF:
-
5-methyltetrahydrofolic acid
- CSF:
-
Cerebrospinal fluid
- FR:
-
Folate receptor
- MRI:
-
Magnetic Resonance Imaging
- WES:
-
Whole Exome Sequencing
- DWI:
-
Diffusion weighted imaging
- ACMG:
-
American College of Medical Genetics
- AEDs:
-
Antiepileptic drugs
References
Ramaekers VT, Blau N. Cerebral folate deficiency. Dev Med Child Neurol. 2004;46:843–51.
Cario H, Bode H, Debatin K-M, Opladen T, Schwarz K. Congenital null mutations of the FOLR1 gene: a progressive neurologic disease and its treatment. Neurology. 2009;73:2127–9.
Desai A, Sequeira JM, Quadros EV. The metabolic basis for developmental disorders due to defective folate transport. Biochimie. 2016;126:31–42.
Frye RE, Slattery JC, Quadros EV. Folate metabolism abnormalities in autism: potential biomarkers. Biomark Med. 2017;11:687–99. https://doi.org/10.2217/bmm-2017-0109.
Steinfeld R, Grapp M, Kraetzner R, Dreha-Kulaczewski S, Helms G, Dechent P, et al. Folate receptor alpha defect causes cerebral Folate transport deficiency: a treatable neurodegenerative disorder associated with disturbed myelin metabolism. Am J Hum Genet. 2009;85:354–63. https://doi.org/10.1016/j.ajhg.2009.08.005.
Della-Longa S, Arcovito A. Structural and functional insights on folate receptor α (FRα) by homology modeling, ligand docking and molecular dynamics. J Mol Graph Model. 2013;44:197–207.
Chen C, Ke J, Zhou XE, Yi W, Brunzelle JS, Li J, et al. Structural basis for molecular recognition of folic acid by folate receptors. Nature. 2013;500:486–9.
Grapp M, Just IA, Linnankivi T, Wolf P, Lücke T, Häusler M, et al. Molecular characterization of folate receptor 1 mutations delineates cerebral folate transport deficiency. Brain. 2012;135:2022–31. https://doi.org/10.1093/brain/aws122.
Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17:405–24.
Al-Baradie RS, Chaudhary MW. Diagnosis and management of cerebral folate deficiency. A form of folinic acid-responsive seizures. Neurosciences (Riyadh). 2014 Oct;19(4):312–6.
Dill P, Schneider J, Weber P, Trachsel D, Tekin M, Jakobs C, et al. Pyridoxal phosphate-responsive seizures in a patient with cerebral folate deficiency (CFD) and congenital deafness with labyrinthine aplasia, microtia and microdontia (LAMM). Mol Genet Metab. 2011;104:362–8. https://doi.org/10.1016/j.ymgme.2011.05.019.
Kobayashi Y, Tohyama J, Akiyama T, Magara S, Kawashima H, Akasaka N, et al. Severe leukoencephalopathy with cortical involvement and peripheral neuropathy due to FOLR1 deficiency. Brain and Development. 2017;39:266–70.
Pérez-Dueñas B, Toma C, Ormazábal A, Muchart J, Sanmartí F, Bombau G, et al. Progressive ataxia and myoclonic epilepsy in a patient with a homozygous mutation in the FOLR1 gene. J Inherit Metab Dis. 2010;33:795–802.
Delmelle F, Thöny B, Clapuyt P, Blau N, Nassogne M-C. Neurological improvement following intravenous high-dose folinic acid for cerebral folate transporter deficiency caused by FOLR-1 mutation. Eur J Paediatr Neurol EJPN Off J Eur Paediatr Neurol Soc. 2016;20:709–13.
Ohba C, Osaka H, Iai M, Yamashita S, Suzuki Y, Aida N, Shimozawa N, Takamura A, Doi H, Tomita-Katsumoto A, Nishiyama K, Tsurusaki Y, Nakashima M, Miyake N, Eto Y, Tanaka F, Matsumoto N, Saitsu H. Diagnostic utility of whole exome sequencing in patients showing cerebellar and/or vermis atrophy in childhood. Neurogenetics. 2013 Nov;14(3–4):225–32. https://doi.org/10.1007/s10048-013-0375-8.
Ferreira P, Luco SM, Sawyer SL, Davila J, Boycott KM, Dyment DA. Late diagnosis of cerebral folate deficiency: fewer seizures with folinic acid in adult siblings. Neurol Genet. 2015 Dec 22;2(1):e38. https://doi.org/10.1212/NXG.0000000000000038.
Toelle SP, Wille D, Schmitt B, Scheer I, Thöny B, Plecko B. Sensory stimulus-sensitive drop attacks and basal ganglia calcification: new findings in a patient with FOLR1 deficiency. Epileptic Disord Int Epilepsy J Videotape. 2014;16:88–92.
Ormazabal A, Artuch R, Vilaseca MA, Aracil A, Pineda M. Cerebrospinal fluid concentrations of folate, biogenic amines and pterins in Rett syndrome: treatment with folinic acid. Neuropediatrics. 2005;36:380–5.
Shorvon SD. The etiologic classification of epilepsy. Epilepsia. 2011;52:1052–7.
Acknowledgements
We thank the patient and his family for the cooperation and contribution. We would like to thank Dr. Xiaodong Wang from Cipher Gene, Inc. for assisting in manuscript editing.
Funding
This work was kindly supported by Hunan Provincial Natural Science Foundation of China (No. 2020JJ5946) and National Natural Science Foundation of China (No. 81801297; No. 81771408). Whole exome sequencing was paid by funding money.
Author information
Authors and Affiliations
Contributions
CZ, was the primary care physician of the patient. She analyzed the Sanger sequencing data, conceptualized the paper and drafted the initial manuscript and revised the paper. XD and YW helped to collect the clinical information, followed up the patient and interpreted the data. FH evaluated the patient’s MRI. FY provided case consulting, treatment suggestions and revised the paper. JP was responsible for analyzing the Sanger sequencing data, drafting of the manuscript, carrying critical revision of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures were performed in accordance with the ethical standards of the responsible Ethics Committee of Xiangya Hospital, Central South University (Changsha, China) on human experimentation and with the Declaration of Helsinki. For this work written informed consent was obtained from all participants. For participants under 16 years old written informed consent was obtained from the participant’s parent.
Consent for publication
Written informed consent was obtained from the parents for publication of this case report. Copy of the written consent is available for review by the editor of this journal.
Competing interests
None of the authors has any conflict of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, C., Deng, X., Wen, Y. et al. First case report of cerebral folate deficiency caused by a novel mutation of FOLR1 gene in a Chinese patient. BMC Med Genet 21, 235 (2020). https://doi.org/10.1186/s12881-020-01162-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12881-020-01162-3