
Abstract
Purpose
To investigate the prognosis value of a combined model based on 18F-fluoro-deoxyglucose positron emission tomography-computed tomography (18F-FDG PET-CT) baseline and interim parameters in patients with diffuse large B-cell lymphoma (DLBCL).
Methods
We retrospectively analyzed the PET metabolic parameters and clinical data of 154 DLBCL patients between December 2015 and October 2020. All of these patients underwent 18F-FDG PET/CT scan before treatment and after three or four courses of chemotherapy. The optimal cut-off values for quantitative variables were determined by the receiver operating characteristic (ROC) curve. The baseline and interim PET/CT parameters, which respectively included maximum standardized uptake value (SUVmax0), total metabolic tumor volume (TMTV0), standardized total metabolic tumor volume (STMTV0), and the distance between the two furthest lesions (Dmax) and total tumor lesion glycolysis (TTLG1), SUVmax1, TMTV1, and the rate of change of SUVmax (%ΔSUVmax), and clinical characteristics were analyzed by chi-squared test, Kaplan-Meier survival curve, and Cox regression analysis.
Results
Of 154 patients, 35 exhibited disease progression or recurrence. ROC analysis revealed that baseline 18F-FDG PET/CT metabolic parameters, including maximum standardized uptake value (SUVmax0), total metabolic tumor volume (TMTV0), standardized total metabolic tumor volume (STMTV0), and the distance between the two furthest lesions (Dmax), along with interim 18F-FDG PET/CT metabolic parameters such as total tumor lesion glycolysis (TTLG1), SUVmax1, TMTV1, and the rate of change of SUVmax (%ΔSUVmax), were predictive of relapse or progression in DLBCL patients (P < 0.05). The chi-squared test showed that TMTV0, STMTV0, Dmax, SUVmax1, TMTV1, TTLG1, %ΔSUVmax, Deauville score, IPI, Ann Arbor stage, and LDH were associated with patient prognosis (P < 0.05). Multivariate Cox regression analysis showed that Dmax (P = 0.021) and %ΔSUVmax (P = 0.030) were independent predictors of prognosis in DLBCL patients. There were statistically significant differences in PFS among the three groups with high, intermediate, and low risk according to the combination model (P < 0.001). The combination model presented higher predictive efficacy than single indicators.
Conclusion
The combined model of baseline parameter Dmax and intermediate parameter %ΔSUVmax of 18F-FDG PET/CT improved the predictive efficacy of PFS and contributed to the risk stratification of patients, providing a reference for clinical individualization and precision treatment.
Similar content being viewed by others
Diffuse large B-cell lymphoma, (DLBCL) is one of the most common subtypes of non-Hodgkin’s lymphoma, accounting for 1/3 of all non-Hodgkin’s lymphomas, with genetic mutational heterogeneity. Immunochemotherapy significantly improves the prognosis for most DLBCL patients, but 20–40% fail first-line therapy, leading to an extremely poor prognosis [1]. The prognosis of such patients is expected to be improved if they are screened before treatment and a personalized treatment plan is developed.
As DLBCL high affinity for 18F-fluoro-deoxyglucose (18F-FDG), the evaluation of efficacy and prognosis by 18F-fluoro-deoxyglucose positron emission tomography-computed tomography (18F-FDG PET-CT) is a hot research topic in recent years [2]. Studies revealed that 18F-FDG PET/CT parameters, including maximum standardized uptake value (SUVmax), metabolic tumor volume (MTV), total lesion glycolysis (TLG), and %ΔSUVmax hold significant prognostic value [3,4,5]. However, it is still not uniform which parameters should be included in the prognostic criteria, so it is still relevant to further investigate the clinical value of each parameter of PET/CT. Most studies have focused on analyzing single parameters at baseline or midterm, with fewer studies incorporating characteristics reflecting tumor spread. Even fewer studies discuss the prognostic value of combining baseline and midterm PET/CT parameters in DLBCL patients [6, 7]. We analyzed the clinical data and PET/CT baseline and interim parameters of 154 DLBCL patients who received first-line treatment. We aimed to investigate how PET/CT baseline and interim parameters could predict prognosis. This could provide more information about poor prognosis and help clinical treatment.
Materials and methods
Clinical data
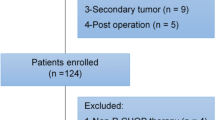
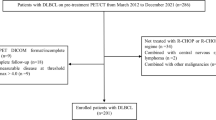
Retrospectively analyzed the clinical data of 154 patients with DLBCL admitted to Sichuan Cancer Hospital from December 2015 to October 2020. The study has been approved by the hospital ethics committee, the inclusion criteria were as follows: patients with pathologically and immunohistochemically confirmed DLBCL; patients who received firstline CHOP (cyclophosphamide, hydroxydaunomycin, oncovin, and prednisone) chemotherapy or rituximab plus CHOP (R-CHOP); patients all underwent 18F-FDG PET/CT scans before and after 3 or 4 cycles of chemotherapy; with complete clinical data. Exclusion criteria: combined history of other tumors; without baseline 18F-FDG PET/CT examination or who received antitumor therapy before undergoing baseline 18F-FDG PET/CT examination.
PET/CT imaging
Siemens Biography MCT-64 PET/CT scanning equipment was used for the examination. 18F-FDG developer automatically synthesized by Sumitomo cyclotron and a chemical synthesis module, radiochemical purity > 99%. Patients fasting for more than 6 h before the examination, with blood glucose < 11.1mmol/L after injection of 18F-FDG at 4.0 MBq/kg body mass, the patients were instructed to lie still for 1 h. PET/CT imaging was performed after urination, with the acquisition range from the cranial vault to the mid-femur, and 6 to 7 beds were acquired. Prior CT scan: tube voltage 140 kV, effective current 42 mAs, pitch 0.8, spherical tube single-turn rotation time 0.5 s, layer thickness 8 mm. PET scans were acquired in 3D, 1.5 min/bed, with delayed imaging, if necessary. Images were reconstructed using the ordered subsets expectation maximization (OSEM) iterative algorithm, and image fusion and post-processing were performed on a Siemens MMWP workstation.
Image analysis
PET image data in anonymized Digital Imaging and Communications in Medicine (DICOM) format were collected for functional parameter measurements using LIFEx software [8]. Lesions were defined as areas with increased uptake of 18F-FDG on PET and abnormal density on CT. Two experienced physicians then reviewed the resulting clusters to remove physiological uptake based on interim PET/CT results. Finally, Dmax, SUVmax, TMTV, and TTLG are automatically generated. MTV was calculated based on a supervised segmentation of tumor regions involving 41% SUVmax thresholding of automatically detected hypermetabolic regions. The dissemination feature Dmax was defined as the distance between the two lesions that were the furthest apart. Each lesion location was defined as the position of its center, and the distances between two lesions were calculated using the Euclidian distance between their centers. TMTV was defined as the sum of every individual lesion’s metabolic volume. TTLG was obtained by summing the tumor lesion glycolysis over all lesions. Other parameters such as %ΔSUVmax= (baseline SUVmax - interim SUVmax) / baseline SUVmax. %ΔTMTV, %ΔTTLG were calculated as above. Standardized total tumor metabolic volume pair (STMTV) = TMTV/weight, standardized total tumor lesion glycolysis (STTLG0) as above. The Deauville score was defined as positive if it was ≥ 4 and negative if it was < 4.
Follow-up assessment
All patients were followed up by telephone or outpatient visits, dated through December 31, 2021. Progression-free survival (PFS) was the clinical endpoint of this retrospective study, which refers to the time from diagnosis to disease recurrence, progression, or final follow-up.
Statistical analysis
SPSS 26.0 software and GraphPad Prism 9 were used for statistical analysis and measured data within a normal distribution are expressed as the mean ± standard deviation (SD), those not conforming are expressed as median (upper and lower quartiles). The receiver operating characteristics (ROC) curves were used to determine the optimal cutoff values for SUVmax, TMTV0, STMTV0, TTLG0, STTLG0, Dmax, SUVmax1, TMTV1, TTLG1, %ΔSUVmax, %ΔTMTV, and %ΔTTLG and performed to evaluate the predictive efficacy of the indicators. Comparison between groups by chi-squared test and the meaningful parameters were included in the multivariate Cox regression analyses. A Kaplan-Meier (K-M) survival analysis was used to complete the survival analysis. Statistical significance was defined as a P value less than 0.05.
Results
The study included 154 patients with DLBCL available for evaluation and analysis. Among them, 78 cases were males and 76 cases were females. The median age was 56 (43, 65) years and the range was 16–87 years. Table 1 shows the clinical characteristics of the 154 DLBCL patients. The median follow-up time was 28 months, with a range of 3.0 to 73.5 months. There were 35 cases of disease progression at the time of follow-up to date.
Of the 154 patients, 61 cases were ≥ 60 years and 93 cases were < 60 years; 56 cases in Ann Arbor stage I-II and 98 cases in stage III-IV; the international prognostic index (IPI) was > 2 points in 43 cases and ≤ 2 points in 111 cases; the lactate dehydrogenase (LDH) level was normal in 94 cases and abnormal in 60 cases. Among them, patients with Ann Arbor stage III-IV (P < 0.001), IPI > 2 points (P < 0.001), and abnormal LDH (P = 0.004) had a higher risk of disease progression or recurrence (Table 2).
We defined AUC > 0.6 as having diagnostic value and performed ROC analysis. The results showed that the cutoff values of TMTV0, STMTV0, Dmax, SUVmax1, TMTV1, TTLG1, and %ΔSUVmax for PFS were 152.11, 2.63, 53.20, 5.31, 30.03, 78.97, and 87.82%, respectively (Table 3). Of these metabolic parameters, patients with TMTV0, STMTV0, Dmax, SUVmax1, TMTV1, TTLG1 above the cutoff (P < 0.05), %ΔSUVmax below the cutoff (P < 0.05) and Deauville score ≥ 4 points (P < 0.05) had a higher risk of disease progression or recurrence (Table 4).
The parameters that were meaningful in the chi-squared test were included in the multivariate cox regression analyse. Due to the close correlation between TMTV0 and STMTV0, TMTV1 and TTLG1, only STMTV0 and TTLG1 were included in the multivariate analysis. The analysis indicated that %ΔSUVmax (HR = 2.765, 95% CI = 1.103–6.935, P = 0.030) and Dmax (HR = 2.410, 95% CI = 1.139–5.099, P = 0.021) were independent risk factors for PFS in patients with DLBCL (Fig. 1). Kaplan-Meier survival curve analysis showed that PFS was better in the group with Dmax < 53.20 cm than in the group with Dmax ≥ 53.20 cm (Fig. 2); PFS was better in the group with %ΔSUVmax ≥ 87.82% than in the group with %ΔSUVmax < 87.82% (Fig. 3), suggesting that patients with high Dmax before treatment and low %ΔSUVmax after treatment had a poorer prognosis and were more likely to recur or progress.

Multivariate Cox regression analyses of clinical characteristics, baseline and intermediate PET/CT parameters for PFS, and Comparison of 95% confidence intervals for various parameters

Kaplan‑Meier survival analysis of PFS according to Dmax

Kaplan‑Meier survival analysis of PFS according to %ΔSUVmax
A new model was established by combining the parameters of Dmax and %ΔSUVmax, and patients were divided into three groups: the high-risk group was Dmax ≥ 53.20+%ΔSUVmax < 87.82%; the low-risk group was Dmax < 53.20+%ΔSUVmax ≥ 87.82%; and the remaining combination was the medium-risk group. Kaplan-Meier survival curve showed that PFS was statistically different between all three groups (P < 0.001), PFS in the low-risk group was significantly higher than in the medium- and high-risk groups (Fig. 4).

Kaplan‑Meier survival analysis of PFS according to the Combination Model
According to the ROC of Dmax, %ΔSUVmax and the combination of both to PFS, the AUCs, sensitivities and specificities were 0.707, 51.4%, 82.4%, 0.686, 77.1%, 57.1% and 0.779, 57.1%, 84.9%, respectively. The combined model improves the predictive performance compared to single parameters (Fig. 5).

ROC curves of Dmax and %ΔSUVmaxand the Combination Model for prediction of PFS
Discussion
DLBCL is a clinically and pathologically heterogeneous disease, which poses a challenge for determining treatment efficacy and prognosis. Hence, the prognostic factors in DLBCL have been a hot topic of research. The IPI score is a clinical index often used to determine the prognosis of non-Hodgkin’s lymphoma, especially DLBCL. As rituximab therapy becomes available, the IPI has also been improved by introducing variants such as R-IPI, aa-IPI and NCCN-IPI, which can better reflect the prognosis of DLBCL patients with different chemotherapy regimens [9]. In the present study, there was a significant difference in PFS between the low and high IPI subgroups, which is consistent with the findings of previous studies, suggesting that IPI has important value in prognostic assessment. However, the multifactorial analysis indicated that IPI was not an independent predictor, similar to previous results [7, 10, 11]. This study also showed that the prognosis could vary among patients with the same IPI score. The IPI score was based on the patient’s pretreatment status and did not incorporate the patient’s treatment response to chemotherapy, so its use as a prognostic evaluation index has some limitations. In addition, Ann Arbor stage and LDH levels were also associated with prognosis, but they were not independent predictors.
The imaging agent 18F-FDG of PET/CT can accumulate in tumour cells with increased metabolism and proliferation, thus indicating lesion activity more accurately than conventional imaging [12]. Therefore, baseline and interim 18F-FDG PET/CT parameters are widely used to study the prognosis of DLBCL patients. In our study, Dmax was the only independent predictor of PFS among all baseline parameters, and the risk of disease progression in patients with high Dmax was 1.410 times higher than that in the low-value group. Patients with Dmax ≥ 53.20 cm had significantly lower PFS than those with Dmax < 53.20 cm, indicating that high Dmax was associated with poor prognosis. This result was similar to Zhou et al.‘s finding (57.4 cm) [13]. Cottereau’s study [4] also led to the conclusion that high Dmax was associated with poor prognosis and indicated that there was no significant difference in Dmax among patients with different heights. In addition, baseline parameters such as TMTV0 and STMTV0, although not independent predictors, were all associated with patient PFS. This is further evidence that baseline metabolic parameters are valuable for prognostic prediction. Some previous studies [14,15,16] found that pretreatment TMTV was an independent risk factor for prognosis in DLBCL patients. Some studies [6, 17, 18] have also conclusively indicated that TTLG is an independent predictor of prognosis. Our findings are not fully consistent with the abovementioned studies, which may be due to the inconsistent methods of outlining TMTV and the different survival endpoints selected. For example, in MIKHAEELNG [16], a fixed threshold method with SUV = 2.5 was used as the absolute limit, and all metabolic regions > 2.5 were included in the metabolic volume, yet the results were often higher than the true level for patients with high background metabolic levels as well as low overall tumour metabolic levels. In this study, the percentage threshold method was used, and the 41% recommended by the EANM guidelines [19] was chosen as the outline threshold. However, when the tumour SUVmax is too large, the outlined TMTV will underestimate the actual tumour volume and vice versa. Weiler-Sagie [2] analysed 766 DLBCL patients with 18F-FDG uptake before chemotherapy and found that more than 97% of lesions exhibited high uptake of 18F-FDG. Therefore, there are many interfering factors in the outline of TMTV, while Dmax, as the distance between the centres of the two most distant lesions, can be used to visualize the spatial distribution of the disease, which is not highly dependent on the lesion contour and is not seriously affected by PET/CT instrument performance and image outline, promoting its widespread use.
Compared to baseline parameters, interim 18F-FDG PET/CT metabolic parameters can reflect tumour sensitivity to first-line treatments such as R-CHOP, thereby identifying patients who are not sensitive to first-line treatment regimens and guiding clinical changes to improve prognosis. The Deauville score [20] is a widely used clinical method to assess the efficacy of lymphoma by interim 18F-FDG PET/CT. It measures the SUVmax of the lesion and compares it with the SUVmax of the liver and mediastinal blood pool on the current imaging. The present study showed poorer PFS in patients with an interim PET/CT Deauville score ≥ 4, which is consistent with the results of previous studies [9]. However, in this study, %ΔSUVmax was the only independent predictor among all interim metabolic parameters and the Deauville score. Patients with low %ΔSUVmax had a 1.765 times higher risk of disease progression than those with high %ΔSUVmax. The results showed that PFS was significantly higher in patients with %ΔSUVmax ≥ 87.82% than in patients with %ΔSUVmax < 87.82%, similar to the results of Zhang et al. [6] (86.02%). Casasnovas et al. [5] also found that %ΔSUVmax predicted PFS in patients after chemotherapy and found better agreement by comparing three readers using %ΔSUVmax and Deauville score to assess efficacy. Rekowski et al. [21] also concluded by comparing the two that %ΔSUVmax seems to be more appropriate to assess the early metabolic response of DLBCL patients to standard R-CHOP treatment. This result may be explained by two reasons. First, the Deauville score was used to select the SUVmax of the lesion and a comparison was made with the SUVmax of the liver and mediastinal blood pool, but this only reflected the metabolism of the local tumour tissue, not the systemic tumour load. Second, factors such as blood glucose, lipids, and age [22] may confound the SUVmax values of the liver and mediastinal blood pool. In contrast, %ΔSUVmax is a semiquantitative parameter used in mid-term PET/CT imaging which is easy to calculate and can reflect the metabolic level of the tumour more objectively. However, the optimal cutoff values of %ΔSUVmax have been reported differently; for example, some scholars [5, 23, 24] reported cutoff values of 70%, 74%, 81.54%, etc., which may be related to blood glucose levels, selection of target lesions, and different instrument specifications. However, Wang et al. [25] found that the Deauville score and %ΔSUVmax were associated with the prognosis of DLBCL patients, but only the Deauville score was an independent predictor. Ng et al. [26] also showed that compared to %ΔSUVmax, the Deauville score was able to better discriminate the prognosis of DLBCL patients. There are some differences between the results of the above studies and those of the present study, which can be explained as follows: (1) In some studies, time-to-progression (TTP) was chosne as the follow-up endpoint, while the endpoint of our study was PFS; (2) The present study included patients with 3–4 cycles of postchemotherapy, while some studies included patients with 2 or 4 cycles of postchemotherapy; (3) The present study included a large number of clinical and imaging parameters, which might influence each other; (4) Meignan et al. [27] pointed out that %ΔSUVmax may be a false-positive in the condition of a low SUVmax level before treatment. Therefore, whether %ΔSUVmax can replace the Deauville score still needs to be confirmed by large-sample, multicentre studies. In addition, the present study showed that the midterm parameters SUVmax1, TMTV1, and TTLG1 were all associated with patient PFS, similar to the results of previous studies, suggesting that the interim metabolic parameters also have good predictive value for prognosis. We extended the previous studies of baseline combined with interim parameters [6, 7] by adding SMTV0, STLG0, %ΔTMTV and %ΔTTLG as potential prognostic predictors.
Out of 77 patients in this study who had a %ΔSUVmax ≥ 87.82%, indicating a good interim treatment response, 9 patients still experienced relapse or progression. Therefore, judging the prognosis based only on the interim response to chemotherapy in clinical practice is not sufficient. We aimed to develop a combined model that integrated 18F-FDG PET/CT baseline and interim metabolic parameters which could enhance predictive efficacy and identify high-risk patients. We propose a prognostic assessment model that uses these two complementary parameters from baseline and interim PET/CT scans to characterize two distinct aspects of the disease: tumour dissemination and posttreatment response. This study showed that the predictive efficacy of the combined Dmax+%ΔSUVmax was higher than that of the single parameter, and the PFS of patients in all three combined models was significantly different, with medium- and high-risk patients having significantly lower PFS than low-risk patients. Cottereau [28] suggested that combining both Dmax and MTV could further improve the risk stratification of patients. Zhang et al. [6] combined both baseline TLG and %ΔSUVmax and showed good predictive power for recurrence or progression. Zhu et al. [7] suggested that combining the maximum diameter of the largest lesion and midterm treatment response could improve the efficacy of predicting PFS and help identify patients at high risk of recurrence. Few studies have combined baseline and intermediate metabolic parameters to build a combined model to predict prognosis, and the indicators used vary, but all suggest that PET/CT baseline and intermediate parameters should be used as a reference for patient risk stratification, thus aiding in the detection of high-risk patients and guiding clinical personalized treatment.
Due to insufficient follow-up time, only PFS was observed in this study, and adequate overall survival was not yet observed, pending continued long-term follow-up to enrich the data. In addition, this study is a retrospective study, and a prospective study is feasible at a later stage to validate the findings.
In conclusion, combining 18F-FDG PET/CT baseline and interim metabolic parameters and even further including clinical and pathological indicators to establish a combined model to comprehensively assess patient prognosis may be a future research direction. By combining Dmax, which can reflect lesion dissemination, and %ΔSUVmax, which can indicate treatment response, the predictive efficacy of PFS can be improved, and the risk stratification of patients can be facilitated. This can provide a basis for clinical individualization and precision treatment.
Data availability
The datasets presented in this article are not readily available. Requests to access the datasets should be directed to dangjun0913@163.com.
References
Candelaria M. Advances in the diagnosis and control of Lymphomas. Salud Publica Mex. 2016;58(2):296–301. https://doi.org/10.21149/spm.v58i2.7800. PMID: 27557389.
Weiler-Sagie M, Bushelev O, Epelbaum R, Dann EJ, Haim N, Avivi I. 18)F-FDG avidity in Lymphoma readdressed: a study of 766 patients. J Nucl Med. 2010;51(1):25–30. https://doi.org/10.2967/jnumed.109.067892. Epub 2009 Dec 15.
Kostakoglu L, Nowakowski GS. End-of-treatment PET/Computed tomography response in diffuse large B-Cell Lymphoma. PET Clin. 2019;14(3):307–15. https://doi.org/10.1016/j.cpet.2019.03.001.
Cottereau AS, Nioche C, Dirand AS, Clerc J, Morschhauser F, Casasnovas O, et al. 18F-FDG PET dissemination features in diffuse large B-Cell Lymphoma are Predictive of Outcome. J Nucl Med. 2020;61(1):40–5. https://doi.org/10.2967/jnumed.119.229450.
Casasnovas RO, Meignan M, Berriolo-Riedinger A, Bardet S, Julian A, Thieblemont C, et al. SUVmax reduction improves early prognosis value of interim positron emission tomography scans in diffuse large B-cell Lymphoma. Blood. 2011;118(1):37–43. https://doi.org/10.1182/blood-2010-12-327767.
Zhang YY, Song L, Zhao MX, Hu K. A better prediction of progression-free survival in diffuse large B-cell Lymphoma by a prognostic model consisting of baseline TLG and %∆SUVmax. Cancer Med. 2019;8(11):5137–47. https://doi.org/10.1002/cam4.2284.
Zhu L, Meng Y, Guo L, Zhao H, Shi Y, Li S, et al. Predictive value of baseline 18F-FDG PET/CT and interim treatment response for the prognosis of patients with diffuse large B-cell Lymphoma receiving R-CHOP chemotherapy. Oncol Lett. 2021;21(2):132. https://doi.org/10.3892/ol.2020.12393.
Nioche C, Orlhac F, Boughdad S, Reuzé S, Goya-Outi J, Robert C, et al. LIFEx: a freeware for Radiomic feature calculation in Multimodality Imaging to accelerate advances in the characterization of Tumor Heterogeneity. Cancer Res. 2018;78(16):4786–9. https://doi.org/10.1158/0008-5472.CAN-18-0125.
Huang HH, Xiao F, Chen FY, Wang T, Li JM, Wang JM, et al. Reassessment of the prognostic value of the International Prognostic Index and the revised International Prognostic Index in patients with diffuse large B-cell Lymphoma: a multicentre study. Exp Ther Med. 2012;4(3):475–80. https://doi.org/10.3892/etm.2012.607.
Kwon SH, Kang DR, Kim J, Yoon JK, Lee SJ, Jeong SH, et al. Prognostic value of negative interim 2-[18F]-fluoro-2-deoxy-d-glucose PET/CT in diffuse large B-cell Lymphoma. Clin Radiol. 2016;71(3):280–6. https://doi.org/10.1016/j.crad.2015.11.019.
de Oliveira Costa R, Hallack Neto A, Siqueira S, Lage LA, de Paula HM, Coutinho AM, et al. Interim fluorine-18 fluorodeoxyglucose PET-computed tomography and cell of origin by immunohistochemistry predicts progression-free and overall survival in diffuse large B-cell Lymphoma patients in the Rituximab era. Nucl Med Commun. 2016;37(10):1095–101. https://doi.org/10.1097/MNM.0000000000000553.
Gallamini A, Borra A. Role of PET in Lymphoma. Curr Treat Options Oncol. 2014;15(2):248–61. https://doi.org/10.1007/s11864-014-0278-4.
Zhou Y, Zhu Y, Chen Z, Li J, Sang S, Deng S. Radiomic features of 18F-FDG PET in Hodgkin Lymphoma are Predictive of outcomes. Contrast Media Mol Imaging. 2021;2021:6347404. https://doi.org/10.1155/2021/6347404.
Sasanelli M, Meignan M, Haioun C, Berriolo-Riedinger A, Casasnovas RO, Biggi A, et al. Pretherapy metabolic tumour volume is an Independent predictor of outcome in patients with diffuse large B-cell Lymphoma. Eur J Nucl Med Mol Imaging. 2014;41(11):2017–22. https://doi.org/10.1007/s00259-014-2822-7.
Guo B, Tan X, Ke Q, Cen H. Prognostic value of baseline metabolic Tumor volume and total lesion glycolysis in patients with Lymphoma: a meta-analysis. PLoS ONE. 2019;14(1):e0210224. https://doi.org/10.1371/journal.pone.0210224.
Mikhaeel NG, Smith D, Dunn JT, Phillips M, Møller H, Fields PA, et al. Combination of baseline metabolic tumour volume and early response on PET/CT improves progression-free survival prediction in DLBCL. Eur J Nucl Med Mol Imaging. 2016;43(7):1209–19. https://doi.org/10.1007/s00259-016-3315-7.
Esfahani SA, Heidari P, Halpern EF, Hochberg EP, Palmer EL, Mahmood U. Baseline total lesion glycolysis measured with (18)F-FDG PET/CT as a predictor of progression-free survival in diffuse large B-cell Lymphoma: a pilot study. Am J Nucl Med Mol Imaging. 2013;3(3):272–81.
Ceriani L, Martelli M, Zinzani PL, Ferreri AJ, Botto B, Stelitano C, et al. Utility of baseline 18FDG-PET/CT functional parameters in defining prognosis of primary mediastinal (thymic) large B-cell Lymphoma. Blood. 2015;126(8):950–6. https://doi.org/10.1182/blood-2014-12-616474.
Boellaard R, Delgado-Bolton R, Oyen WJ, Giammarile F, Tatsch K, Eschner W, et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging. 2015;42(2):328–54. https://doi.org/10.1007/s00259-014-2961-x.
Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-hodgkin Lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059–68. https://doi.org/10.1200/JCO.2013.54.8800.
Rekowski J, Hüttmann A, Schmitz C, Müller SP, Kurch L, Kotzerke J, et al. Interim PET evaluation in diffuse large B-Cell Lymphoma using published recommendations: comparison of the Deauville 5-Point scale and the ∆SUVmax Method. J Nucl Med. 2021;62(1):37–42. https://doi.org/10.2967/jnumed.120.244145.
Liu G, Hu Y, Zhao Y, Yu H, Hu P, Shi H. Variations of the liver standardized uptake value in relation to background blood metabolism: an 2-[18F]Fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography study in a large population from China. Med (Baltim). 2018;97(19):e0699. https://doi.org/10.1097/MD.0000000000010699.
Li X, Sun X, Li J, Liu Z, Mi M, Zhu F, et al. Interim PET/CT based on visual and semiquantitative analysis predicts survival in patients with diffuse large B-cell Lymphoma. Cancer Med. 2019;8(11):5012–22. https://doi.org/10.1002/cam4.2404. Epub 2019 Jul 10.
Li X, Xie X, Zhang L, Li X, Li L, Wang X, et al. Research on the midterm efficacy and prognosis of patients with diffuse large B-cell Lymphoma by different evaluation methods in interim PET/CT. Eur J Radiol. 2020;133:109301. https://doi.org/10.1016/j.ejrad.2020.109301.
Wang RM, Li F, Liu CB, Guan ZW, Fu LP, Xu BX, et al. Prognostic Value of Interim PET/CT in 227 patients of DLBCL. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2019;27(1):74–9. https://doi.org/10.7534/j.issn.1009-2137.2019.01.012. Chinese.
Ng DZ, Lee CY, Lam WW, Tong AK, Tan SH, Khoo LP, et al. Prognostication of diffuse large B-cell Lymphoma patients with Deauville score of 3 or 4 at end-of-treatment PET evaluation: a comparison of the Deauville 5-point scale and the ∆SUVmax method. Leuk Lymphoma. 2022;63(1):256–9. https://doi.org/10.1080/10428194.2021.1992624.
Meignan M, Barrington S, Itti E, Gallamini A, Haioun C, Polliack A. Report on the 4th International Workshop on Positron Emission Tomography in Lymphoma held in Menton, France, 3–5 October 2012. Leuk Lymphoma. 2014;55(1):31 – 7. https://doi.org/10.3109/10428194.2013.802784.
Cottereau AS, Meignan M, Nioche C, Capobianco N, Clerc J, Chartier L, et al. Risk stratification in diffuse large B-cell Lymphoma using lesion dissemination and metabolic Tumor burden calculated from baseline PET/CT†. Ann Oncol. 2021;32(3):404–11. https://doi.org/10.1016/j.annonc.2020.11.019.
Acknowledgements
The authors wish to thank the clinical staff from all the clinical centers for their contributions to recruiting patients and providing clinical care.
Funding
This study was supported by funds from Science & Technology Department of Sichuan Province (No. 22ZDYF1359), Sichuan Medical Health and Health Care Promotion Institute (KY2022SJ0260) and Sichuan Cancer Hospital Outstanding Youth Funding (YB 2023022).
Author information
Authors and Affiliations
Contributions
JD, XP, PW and CZ designed the project, JD and XP wrote the manuscript. XT, ZY, and XJ organized data. SC and YL analyzed data. XJ, YY and ZC reviewed the data and the manuscript. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was ethically approved by Sichuan Cancer Hospital Ethics Committee and in accordance to the local regulations of China. All patients signed a written informed consent form.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Declarations.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dang, J., Peng, X., Wu, P. et al. Predictive value of Dmax and %ΔSUVmax of 18F-FDG PET/CT for the prognosis of patients with diffuse large B-cell lymphoma. BMC Med Imaging 23, 173 (2023). https://doi.org/10.1186/s12880-023-01138-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-023-01138-8