
Abstract
Background
The aim was to compare the diffusion tensor imaging (DTI) indices derived from human hearts between 1.5 T and 3.0 T scanners. Additionally, the reproducibility of DTI indices was assessed between 1.5 T and 3.0 T scanners.
Methods
A total of 18 ex-vivo hearts were derived from patients who underwent heart transplantation. The DTI schemes were performed at 1.5 T and 3.0 T, respectively. Then, the same slices from each ex-vivo heart were selected for image analysis. The student’s t-test or Wilcoxon-rank test was used to compare the statistical differences. The agreement of DTI indices was mainly reported as the interclass correlation coefficient (ICC).
Results
No significant differences (all P > 0.05) were found in the DTI indices between 1.5 T and 3.0 T scanners. Interestingly, the ICC of all DTI indices was relatively lower with a low b-value. The reproducibility of the helix angle (HA) was relatively lower when compared to the other DTI indices.
Conclusion
The DTI indices of ex-vivo human hearts between 1.5 T and 3.0 T scanners had no significant differences. The consistency of DTI indices needed caution using a low b-value with different field strengths, and the relatively low reproducibility of HA should be considered.
Similar content being viewed by others


Background
Recently, cardiovascular magnetic resonance (CMR) diffusion tensor imaging (DTI) has emerged as a promising technique for the determination of myocardial fiber orientation [1, 2] and tissue characterization. DTI could investigate water diffusion within the tissue and derive additional scalar metrics for quantifying structural integrity [3, 4]. Consequently, CMR DTI has become a non-invasive method to illustrate the alterations of cardiac microstructure in patients with dilated cardiomyopathy (DCM), amyloidosis, and hypertrophic cardiomyopathy in recent studies [1, 2, 5,6,7].
Theoretically, the DTI indices should remain constant at different field strengths [8]. Since DTI is inherently a low-resolution and low-signal-to-resolution technique, the image quality needs to be seriously concerned [9]. DTI is sensitive to the translational motion of water molecules and a small amount of subject motion can lead to a significant signal phase shift or signal loss, which severely affects image quality [9, 10]. In addition, DTI with single-shot echo-planar imaging (EPI) sequence is commonly used. The EPI sequence is particularly sensitive to susceptibility artifacts and magnetic field inhomogeneities due to a long echo train. Moreover, the magnetic field inhomogeneities and related artifacts that increase with rising field strength probably cause the difference of DTI indices in CMR DTI protocols with different field strengths.
With the growing interests of CMR DTI, it has been performed in human hearts with various MRI systems at different field strengths, mainly at 1.5 T [6, 11, 12] or 3.0 T [2, 13]. The comparison between 1.5 T and 3.0 T DTI scanners, however, is an important and essential procedure for adoption in clinical routine [8, 10, 14]. Because DTI indices should not be influenced by the external magnetic field theoretically, the difference of signal-to-noise ratios caused by field strength may affect the DTI indices [8, 15]. If CMR DTI is sought to be clinically useful, the DTI indices should be robust for the external field strength, which may be helpful for the initial diagnosis and monitoring of the therapeutic effects. However, little is known about the reproducibility and consistency of DTI indices in cardiac at different field strengths. Therefore, the purpose of this prospective study was to acquire the CMR DTI data from ex-vivo human hearts, and compare the DTI indices between 1.5 T and 3.0 T scanners. Furthermore, we investigated the impact of different b-values on the DTI indices, and assessed the consistency and reproducibility of these DTI indices.
Methods
Study population
A total of 18 ex-vivo hearts were derived from patients who had undergone heart transplantation due to various cardiovascular causes in Guangdong Provincial People's Hospital from April 2020 to January 2021. This study was approved by the Institutional Review Board of Guangdong Provincial People's Hospital (reference number: KY2020-039–01-01).
Ex-vivo human heart preparation
The ex-vivo hearts from patients were collected and fixed in 10% buffered formalin within 1 h of excision from the recipients at the time of heart transplantation. All ex-vivo hearts were fixed in 10% buffered formalin for at least 24 h before the CMR examination, and the average time between fixation and CMR examination was three days. It has been reported that CMR DTI indices remained constant 24 h after the initial cross-linking by formalin fixation for several weeks [16].
Image acquisition
The DTI sequence was scanned at a 3.0 T scanner (Ingenia, Philips Healthcare, Amsterdam, The Netherlands) and a 1.5 T scanner (Achieva, Philips Healthcare, Amsterdam, The Netherlands), respectively. A sixteen-channel receiving array coil was used for the 3.0 T MRI scanner and an eight-channel receive array coil was used for the 1.5 T MRI scanner. The DTI was performed with a multi-shot spin-echo sequence with an EPI readout. Multi-slice short axis views of the heart were acquired covering the entire left ventricular. And a 4-chamber 3D T1WI scan was performed to localize the ex-vivo hearts, and ensured that imaging planes were placed in short-axis view orientation at apical, mid-ventricular and basal. Five diffusion series with 5 different b-values were performed separately on ex-vivo hearts, including b-values of 200 s/mm2, 400 s/mm2, 600 s/mm2, 800 s/mm2 and 1000 s/mm2, respectively. The detailed imaging parameters are shown in Table 1.
Image analysis
Diffusion tensors were calculated on a pixel-by-pixel basis from the CMR diffusion images and diagonalized to yield three eigenvalues (L1, L2 and L3, sorted in descending order and commonly referred to as primary, secondary and tertiary diffusivities, respectively) and eigenvectors (the corresponding eigenvectors E1, E2 and E3). The mean diffusivity (MD), fractional anisotropy (FA), helix angle (HA), E2 angle (E2A), HA transmural gradient and transverse angle (TA) were obtained by the diffusion tensor eigensystem, and E2A values were stated as absolute from 0 to 90 degrees [17,18,19]. The HA transmural gradient was calculated by dividing the myocardium into five transmural concentric rings. The mean HA for each ring against the transmural depth was obtained, and the gradient was defined as the slope extracted from the linear regression of the mean HA [19].
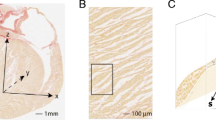
In the present study, we selected only one slice without any myocardium excision for the image analysis of each ex-vivo heart. All the DTI indices were reported as the average values over the entire left ventricular myocardial area on the selected slice for each ex-vivo heart. All the post-processing computation was performed as Fig. 1 using custom codes written in Matlab (Version R2019a, Mathworks, Natick, MA, USA).

The region of interests of DTI images and DTI indices analysis. FA, fractional anisotropy; MD, mean diffusivity; HA, helix angle; E2A, E2 angle; TA, transverse angle
Statistical analysis
Continuous variables were described as mean ± standard deviation. The normal distribution of variables was tested using the Shapiro–Wilk test. The Student’s t-test was used to compare the means of normally distributed variables, while the Wilcoxon-rank test was used to compare the median of skewed variables. The agreement of DTI indices between 1.5 T and 3.0 T scanners was tested by calculating mean bias and 95% limits of agreement on a Bland–Altman test, and interclass correlation coefficient (ICC).
For the reproducibility analysis, we randomly selected one slice from each ex-vivo heart and sketched the region of interest (ROI) on the left ventricular myocardium. To assess intra-observer reproducibility, the first experienced observer was blinded to the clinical information, and then sketched ROIs twice at 2-week intervals. For inter-observer reproducibility, another experienced observer did the same thing in the selected images. The agreement of reproducibility was also tested by calculating mean bias and 95% limits of agreement on a Bland–Altman test, and ICC. All tests were two-sided, and P values < 0.05 were considered statistically significant.
All statistical analyses were performed with the statistical software GraphPad Prism (version 6.0; GraphPad Software, San Diego, California, USA) and in R version 3.4.1 (R Foundation, Vienna, Austria).
Results
Study Population
A total of 18 patients (41 ± 17 years, 11 males) were included in the analysis who had undergone heart transplantation. In detail, nine patients had dilated cardiomyopathy, five had coronary heart disease, one had rheumatic heart disease, one had Arrhythmia right ventricular cardiomyopathy, one had cardiac malignancy, and one had myocarditis proven by pathology.
The comparison between 1.5 T and 3.0 T
Among the DTI indices analyzed, no significant differences (all P > 0.05) were found between 1.5 T and 3 T scanners (Table 2). Interestingly, the ICCs of all DTI indices between 1.5 T and 3.0 T scanners were relatively low with a low b-value. In detail, the ICC of FA, MD, HA, E2A, HA transmural gradient, and TA between 1.5 T and 3.0 T were 0.395 (− 0.074, 0.721), 0.319 (− 0.160, 0.676), 0.726 (0.403, 0.888), 0.556 (0.134, 0.807), 0.024 (− 0.437, 0.474), and 0.107 (− 0.367, 0.536), respectively, when the b-value was 200 s/mm2. The ICC of FA, MD, HA, E2A, HA transmural gradient, TA between 1.5 T and 3.0 T were 0.903 (0.760, 0.963), 0.937 (0.841, 0.976), 0.957 (0.889, 0.984), 0.835 (0.613, 0.935), 0.400 (− 0.067, 0.724), and 0.306 (− 0.174, 0.668), respectively, when the b-value equaled 1000 s/mm2 (Table 3). The mean absolute difference and 95% confidence interval of the mean difference of measurements between 1.5 T and 3.0 T were shown in Table 4 and Additional file 1: Figure S1.
The difference among various b-values
As the b-value increased, MD decreased at both 1.5 T and 3.0 T scanners, while FA, HA, E2A, HA transmural gradient, and TA did not show significant trend varied with b-values, which were shown in Fig. 2. In Fig. 2B, MD with a b-value of 200 s/mm2 was significantly higher than MD with a b-value of 1000 s/mm2 (P = 0.032) at 3.0 T. In addition, HA, E2A, HA transmural gradient and TA at both 1.5 T and 3.0 T did not show any statistical difference with different b-values.

The bar chart shows DTI indices with different b-values. A fractional anisotropy; B mean diffusivity; C helix angle; D E2 angle; E helix angle transmural gradient; F transverse angle. The E2A values were stated as absolute from 0 to 90 degrees
Reproducibility
The intra- and inter-observer reproducibility of DTI indices were shown in Table 5 and Additional file 1: Figure S2. The intra-observer ICC and inter-observer ICC of FA, MD, E2A, HA transmural gradient, and TA were all over 0.85. However, the intra-observer ICC and inter-observer ICC of HA were the lowest. The intra-observer ICC of HA was 0.888 (0.726, 0.957), while the inter-observer ICC was 0.814 (0.569, 0.926).
Discussion
The DTI has emerged as a promising technique in CMR, which was mainly performed with human hearts at 1.5 T or 3.0 T scanners. Given present trends, the DTI scanning in ex-vivo human hearts was performed, and the DTI indices and reproducibility were compared between 1.5 T and 3.0 T scanners. The main findings of our study were included as follows: (1) There were no significant differences in DTI indices between 1.5 T and 3.0 T; (2) the ICC of all DTI indices between 1.5 T and 3.0 T was relatively low with a low b-value; (3) the reproducibility of HA was relatively lower compared with the other DTI indices.
Theoretically, DTI indices should not be influenced by the external magnetic field. However, the comparison of DTI indices at 1.5 T and 3.0 T scanners seemed to reveal contradicting findings in clinical practice. In the evaluation of the brain, Hunsche et al. concluded that MD and FA did not differ significantly comparing 1.5 T and 3.0 T [14], while Guilfoyle et al. observed the changes of DTI indices varied with field length [20]. In the evaluation of kidneys, Notohamiprodjo et al. concluded that none of the DTI indices did not differ significantly when comparing 1.5 T and 3.0 T, while Kido et al. [10] found that both FA and MD were significantly different at different field strengths. The other reason might be the different settings with Lohr et al. [21] reported that there is no difference found at porcine hearts between CMR DTI at 3.0 T and 7.0 T, similar to the present study. However, the comparison of field strength was different between Lohr’s and our study (3.0 T/7.0 T vs. 1.5 T/ 3.0 T). Furthermore, the human ex-vivo hearts were fixed in Formalin in this study, while the porcine hearts were not fixed in Formalin or other substances in Lohr’s study [21]. Whether the DTI indices in the specimens without fixation varied with time was still unclear, and whether it affected their findings remained unknown. Further experiments are urgently needed before the CMR DTI technique is used in clinical practice.
The difference of DTI indices varied with b-value in CMR DTI has not been reported yet, and the b-value mostly ranged from 200 s/mm2 to 1000 s/mm2 in recent research [2, 6, 17, 22, 23]. In the present study, DTI indices derived from the 1.5 T and 3.0 T with 5 different b-values were analyzed, respectively. It was shown that the MD was affected by b-value in the present study, which was similar to Chou et al. They reported that DTI indices were influenced by echo time and b-value, the variations of MD slightly increased with echo time but decreased with the b-value [15]. The reproducibility and accuracy of DTI indices were both improved by increasing the b-value, when the b-value was lower than 1000 s/mm2. In the present study, the ICC of FA and MD was the highest when the b-value equaled 1000 s/mm2, which was similar to the results of Chou et al.
The reproducibility of the DTI indices was also essential, in line with other similar studies in different organs [8, 24]. In the present study, we randomly selected one slice from each ex-vivo heart and sketched ROIs of the myocardium. Not surprisingly, it was shown that the ICC of FA and MD were all over 0.95 in CMR DTI, because FA and MD were the most widely used diffusion scalars in DTI. The reproducibility of HA has not been reported yet. In the present study, the ICC of HA was lower than the other diffusion scalars. The intra-observer ICC of HA was 0.888 (0.726, 0.957), while the inter-observer ICC was 0.814 (0.569, 0.926). Though some of the studies showed good reproducibility of HA in normal control and in patients with hypertrophic cardiomyopathy [25, 26], however, in the present study, half of the patients who underwent heart transplantation were diagnosed DCM. In patients with DCM, the thickness of the myocardium was commonly decreased in the end stage, and the thin myocardium would probably cause the value of HA more sensitive to the sketched ROIs. That might have it challenged the accurate quantification of HA, resulting in the relatively lower ICC of HA [5].
Limitations
There were several limitations in the present study when interpreting the results. First, the sample sizes of the study need to be improved, and the results should be also proved using the MRI systems from other manufacturers as well in the future. Second, the excision of the ex-vivo hearts could be found in some of the slices, but we only analyzed the slices without myocardium excision to address this problem. Third, the ex-vivo hearts were fixed by formalin, and the DTI indices could be different from the ones from in-vivo hearts. However, the present study focused on comparing the DTI indices between 1.5 T and 3.0 T scanners, given the same ex-vivo hearts. At last, the inconsistent echo time and large slice thickness might be the potential limitations in the present study.
Conclusion
In conclusion, the magnetic resonance DTI indices of ex-vivo human hearts between 1.5 T and 3.0 T showed no significant difference in the present study. However, the consistency of DTI indices needed caution using a low b-value with different field strengths, and the relatively low reproducibility of HA should be considered in clinical research or clinical practice in the future using the CMR DTI technique.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to the data being also a part of an ongoing study but are available from the corresponding author on reasonable request.
Abbreviations
- CMR:
-
Cardiovascular magnetic resonance
- DTI:
-
Diffusion tensor imaging
- EPI:
-
Echo-planar imaging
- DCM:
-
Dilated cardiomyopathy
- FA:
-
Fractional anisotropy
- MD:
-
Mean diffusivity
- HA:
-
Helix angle
- E2A:
-
E2 angle
- TA:
-
Transverse angle
- ICC:
-
Interclass correlation coefficient
- ROI:
-
Region of interest
References
MacGowan GA, Parikh JD, Hollingsworth KG. Diffusion tensor magnetic resonance imaging of the heart: Looking into the layers of the myocardium. J Am Coll Cardiol. 2017;69(6):677–8.
Nielles-Vallespin S, Khalique Z, Ferreira PF, de Silva R, Scott AD, Kilner P, et al. Assessment of myocardial microstructural dynamics by in vivo diffusion tensor cardiac magnetic resonance. J Am Coll Cardiol. 2017;69(6):661–76.
Wu MT, Tseng WY, Su MY, Liu CP, Chiou KR, Wedeen VJ, et al. Diffusion tensor magnetic resonance imaging mapping the fiber architecture remodeling in human myocardium after infarction: correlation with viability and wall motion. Circulation. 2006;114(10):1036–45.
McGill LA, Scott AD, Ferreira PF, Nielles-Vallespin S, Ismail T, Kilner PJ, et al. Heterogeneity of fractional anisotropy and mean diffusivity measurements by in vivo diffusion tensor imaging in normal human hearts. PLoS ONE. 2015;10(7): e0132360.
Nguyen CT, Buckberg G, Li D. Magnetic resonance diffusion tensor imaging provides new insights into the microstructural alterations in dilated cardiomyopathy. Circ Cardiovasc Imaging. 2016;9(10): e005593.
Gotschy A, von Deuster C, van Gorkum RJH, Gastl M, Vintschger E, Schwotzer R, et al. Characterizing cardiac involvement in amyloidosis using cardiovascular magnetic resonance diffusion tensor imaging. J Cardiovasc Magn Reson Off J Soc Cardiovasc Magn Reson. 2019;21(1):56.
Abdullah OM, Drakos SG, Diakos NA, Wever-Pinzon O, Kfoury AG, Stehlik J, et al. Characterization of diffuse fibrosis in the failing human heart via diffusion tensor imaging and quantitative histological validation. NMR Biomed. 2014;27(11):1378–86.
Notohamiprodjo M, Dietrich O, Horger W, Horng A, Helck AD, Herrmann KA, et al. Diffusion tensor imaging (DTI) of the kidney at 3tesla–feasibility, protocol evaluation and comparison to 1.5 tesla. Investig Radiol. 2010;45:245–54.
Tournier JD, Mori S, Leemans A. Diffusion tensor imaging and beyond. Magn Reson Med. 2011;65(6):1532–56.
Kido A, Kataoka M, Yamamoto A, Nakamoto Y, Umeoka S, Koyama T, et al. Diffusion tensor MRI of the kidney at 3.0 and 1.5 Tesla. Acta Radiol. 2010;51(9):1059–63.
Stoeck CT, Kalinowska A, von Deuster C, Harmer J, Chan RW, Niemann M, et al. Dual-phase cardiac diffusion tensor imaging with strain correction. PLoS ONE. 2014;9(9): e107159.
Stoeck CT, von Deuster C, Genet M, Atkinson D, Kozerke S. Second-order motion-compensated spin echo diffusion tensor imaging of the human heart. Magn Reson Med. 2016;75(4):1669–76.
Mekkaoui C, Jackowski MP, Kostis WJ, Stoeck CT, Thiagalingam A, Reese TG, et al. Myocardial scar delineation using diffusion tensor magnetic resonance tractography. J Am Heart Assoc. 2018;7(3):e007834.
Hunsche S, Moseley ME, Stoeter P, Hedehus M. Diffusion-tensor MR imaging at 1.5 and 3.0 T: Initial observations. Radiology. 2001;221:550–6.
Chou MC. Effects of b-value and echo time on magnetic resonance diffusion tensor imaging-derived parameters at 15 T: a voxel-wise study. J Med Biol Eng. 2013;33(1):45.
Watson BR, Hsu EW. Effects of formalin fixation on diffusion tensor imaging of myocardial tissues. In: Proceedings of the 20th Annual Meeting ISMRM, Melbourne Australia. 2012.
Ferreira PFKP, McGill LA, Nielles-Vallespin S, Scott AD, Ho SY, McCarthy KP, Haba MM, Ismail TF, Gatehouse PD, de Silva R, Lyon AR, Prasad SK, Firmin DN, Pennell DJ. In vivo cardiovascular magnetic resonance diffusion tensor imaging shows evidence of abnormal myocardial laminar orientations and mobility in hypertrophic cardiomyopathy. J Cardiovasc Magn Reson. 2014;16:87.
Le Bihan D, Mangin JF, Poupon C, Clark CA, Pappata S, Molko N, et al. Diffusion tensor imaging: concepts and applications. J Magn Reson Imag JMRI. 2001;13(4):534–46.
Nguyen C, Fan Z, Xie Y, Pang J, Speier P, Bi X, et al. In vivo diffusion-tensor MRI of the human heart on a 3 tesla clinical scanner: an optimized second order (M2) motion compensated diffusion-preparation approach. Magn Reson Med. 2016;76(5):1354–63.
Guilfoyle DN, Suckow RF, Baslow MH. The apparent dependence of the diffusion coefficient of N-acetylaspartate upon magnetic field strength: evidence of an interaction with NMR methodology. NMR Biomed. 2003;16(8):468–74.
Lohr D, Terekhov M, Weng AM, Schroeder A, Walles H, Schreiber LM. Spin echo based cardiac diffusion imaging at 7T: An ex vivo study of the porcine heart at 7T and 3T. PLoS ONE. 2019;14(3): e0213994.
McClymont D, Teh I, Schneider JE. The impact of signal-to-noise ratio, diffusion-weighted directions and image resolution in cardiac diffusion tensor imaging—insights from the ex-vivo rat heart. J Cardiovasc Magn Reson Off J Soc Cardiovasc Magn Reson. 2017;19(1):90.
Mazumder R, Choi S, Clymer BD, White RD, Kolipaka A. Diffusion tensor imaging of healthy and infarcted porcine hearts: study on the impact of formalin fixation. J Med Imag Radiat Sci. 2016;47(1):74–85.
Vollmar C, O’Muircheartaigh J, Barker GJ, Symms MR, Thompson P, Kumari V, et al. Identical, but not the same: intra-site and inter-site reproducibility of fractional anisotropy measures on two 3.0T scanners. NeuroImage. 2010;51(4):1384–94.
Nielles-Vallespin S, Mekkaoui C, Gatehouse P, Reese TG, Keegan J, Ferreira PF, et al. In vivo diffusion tensor MRI of the human heart: reproducibility of breath-hold and navigator-based approaches. Magn Reson Med. 2013;70(2):454–65.
McGill LA, Ismail TF, Nielles-Vallespin S, Ferreira P, Scott AD, Roughton M, et al. Reproducibility of in-vivo diffusion tensor cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Cardiovasc Magn Reson. 2012. https://doi.org/10.1186/1532-429X-14-86.
Acknowledgements
We thank Yingjie Mei and Yongzhou Xu from Philips Healthcare for the help in CMR technique support and English editing.
Funding
This work was supported by the funding: Natural Science Foundation of Guangdong Province (No. 2020A1515010650), National Natural Science Foundation of China (No. 81974262) and (No. 81971611).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Acquisition of data, analysis and interpretation of data were performed by XL, RC, XX, XW, ZX, YY, ZZ and ZW. The first draft of the manuscript was written by XL, RC, XX, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board in Guangdong Provincial People's Hospital (reference number: KY2020-039-01-01). All participating patients had provided written informed consent for use of the data. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Patients signed informed consent regarding publishing their data and photographs.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Supplementary figures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, X., Chen, R., Xu, X. et al. The comparison of diffusion tensor imaging in human hearts between 1.5 T and 3.0 T. BMC Med Imaging 23, 14 (2023). https://doi.org/10.1186/s12880-023-00969-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-023-00969-9