
Abstract
Background
Evidence of diastolic dysfunction (DD) required for the diagnosis of heart failure with preserved ejection fraction (HFpEF) is elusive in atrial fibrillation (AF). Left ventricular (LV) and left atrial (LA) speckle-tracking echocardiography (STE) may provide rhythm independent indications of DD. We aimed to find common LV/LA myocardial mechanics parameters to demonstrate DD, using STE in patients with AF.
Methods
176 echocardiographic assessments of patients were studied retrospectively by STE. 109 patients with history of AF were divided in three groups: sinus with normal diastolic function (n = 32, ND), sinus with DD (n = 35, DD) and patients with AF during echocardiography (n = 42). These assessments were compared to 67 normal controls. Demographic, clinical, echocardiographic and myocardial mechanic characteristics were obtained.
Results
The patients with DD in sinus rhythm and patients with AF were similar in age, mostly women, and had cardiovascular risk factors as well as higher dyspnea prevalence compared to either controls or patients with ND. In the AF group, LV ejection fraction (LVEF) (p = 0.008), global longitudinal strain and LA emptying were lower (p < 0.001), whereas LA volumes were larger (p < 0.001) compared to the other groups. In a multivariable analysis of patients in sinus rhythm, LA minimal volume indexed to body surface area (Vmin-I) was found to be the single significant factor associated with DD (AUC 83%). In all study patients, Vmin-I correlated with dyspnea (AUC 80%) and pulmonary hypertension (AUC 90%).
Conclusions
Vmin-I may be used to identify DD and assist in the diagnosis of HFpEF in patients with AF.
Similar content being viewed by others

Background
More than half of all patients suffering from heart failure (HF) have preserved left ventricle ejection fraction (LVEF) [1,2,3,4,5,6]. The underlying mechanism of HFpEF is left ventricle (LV) diastolic dysfunction (DD), which is also the potential mechanism underlying the most common arrhythmia, atrial fibrillation (AF) [7, 8]. Furthermore, DD is associated with increase in all-cause mortality and is not unique only to HFpEF, it is observed in patients with HF with reduced EF (HFrEF) as well [6].
The diagnosis of HFpEF, according to The European Society of Cardiology guidelines, is based on signs and symptoms of HF in patients with preserved LVEF of a non-dilated LV and elevated LV filling pressures with evidence of DD: impaired LV relaxation or increased LV diastolic stiffness [4, 9]. Invasive catheterization can provide the accurate diagnosis of DD in HFpEF. However, common practice is to establish the diagnosis non-invasively by echocardiographic assessment to ascertain preserved LV systolic function and estimate diastolic pressures [4, 6, 10]. Current DD echocardiographic recommendations [11] mostly focus on diagnostic criteria for patients in sinus rhythm, whereas DD diagnosis in AF is addressed as “in special populations”, pointing out that maximal left atria (LA) volume may be directly related to AF, and that Doppler assessment of LV diastolic function is limited by the variability in cycle length [11]. A multitude of parameters are presented that “can be used to predict LV filling pressures”, most of which are not consistently acquired in routine clinical studies.
LA maximal volume is part of the assessment of DD by echocardiography. Recently, LA phasic volumes have been suggested as an LA function assessment in relation to DD [12,13,14], since LA emptying actually reflects LV filling. Patients in sinus rhythm and patients with AF both have maximal and minimal LA volumes. Thus, LA global phasic function parameters can be compared and correlated to heart failure symptoms in patients in sinus rhythm and AF, where the active phase of LA contraction is absent. Moreover, as both LA and LV volumes are analyzed in tandem in the evaluation of LA function, the effects of variable cycle lengths in AF are probably minimized.
Myocardial mechanics, using feature tracking software, offer a unique method to elucidate both LV and LA function, creating strain and volume curves for analysis [15,16,17]. The objective of this study was to identify common LA function correlates of diastolic dysfunction and HF symptoms in patients in sinus and AF to suggest a method to diagnose DD in patients with AF and correlate them to HF symptoms in patients with preserved EF.
Methods
Patients
Medically stable patients between 19 and 90 years of age with history of AF (current or past) who had a transthoracic echocardiography assessment at Baruch Padeh Poriya Medical Center between January 2014 and October 2015 were retrospectively screened for this study. Patients were included if they had a LVEF ≥ 45%, and none of the following: more than mild valvular disease, cardiomyopathy, history of myocardial infarction or other non-cardiac sources of dyspnea, technically inadequate echocardiographic images, tachycardia, complete atrioventricular (AV) block, or electronic pacing. Patient had no prior diagnosis of HFpEF. After screening the departmental database, 109 patients met our inclusion criteria and remained after exclusion. These were divided into two groups according to their cardiac rhythm: patients with AF at the time of echocardiography and patients in sinus rhythm. Patients in sinus rhythm were then divided into two groups according to their diastolic function: patients with normal diastolic function (ND) and patients with abnormal diastolic function (DD). The control group was composed of 67 healthy subjects with no comorbidities and normal echocardiographic studies.
Patients were suspected to have HFpEF according to the following criteria of presenting symptoms: dyspnea, fatigue, weakness, reduced ability to exercise, pulmonary edema, and/or peripheral edema.
Echocardiography
Routine clinical 2D and Doppler echocardiography were performed and collected retrospectively according to the American Society of Echocardiography recommendations. DD was determined for patients in sinus rhythm according to recent guidelines [11, 18, 19] and as previously published by our group. Diastolic function was evaluated using the mitral inflow pulsed-wave Doppler, septal and lateral mitral annular tissue-Doppler velocities, and pulmonary vein pulse wave Doppler velocities [5, 7]. DD was determined either as a pseudonormal (mitral E/A 0.8–1.9, E deceleration time (EDt) 140–280 ms) or restrictive pattern (E/A N 2, EDt b 140 ms). Evidence of elevated left atrial pressure (either E/E′ ≥ 14 or pulmonary S/D b 1.0) and left atrial (LA) enlargement was a pre-requisite for all patients (LA systolic diameter ≥ 38 mm for women, ≥ 40 mm for men) [20]. Since the guidelines refer only to specific parameters when EF is reduced to suggest (rather than diagnose) DD in patients in atrial fibrillation [11], LA emptying parameters were addressed to find correlates of DD and symptomatic HF.
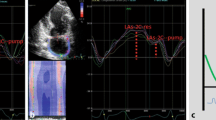
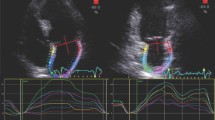
Myocardial mechanics were analyzed retrospectively. LA and LV measurements were performed offline by a single operator who was blinded to clinical and echocardiographic findings, using dedicated software (eSie VVI, us v.3.0.1.45 b.140211, Siemens Medical System, Mountain View). By using the dedicated clip editor, two to three cardiac cycles were selected for each representative view and the onset of R wave was used as the reference point for both LA and LV strain and volume curves [12, 13, 15, 16, 21]. Endocardial surface was manually traced using a point and click approach (Fig. 1) and then after automatically processed by the software. Apical views (4, 2 and 3 chambers) were analyzed for LV and LA Myocardial mechanics. Previous studies report consistently the fact that LV systolic and diastolic functions are tightly coupled. Additionally, association between LV systolic and diastolic strain together with LA strain and LV diastolic function was reported in studies using STE [11]. Variables included: strain (% shortening); global longitudinal strain (average strain at aortic valve closure, GLS); Global mechanical synchrony index (GMSi, equals to GLS/average of segmental strain peaks; equals to1 if peaks coincide at aortic valve closure); and the ratio of early diastolic strain rate to systolic strain rate (SR E/S ratio). Bi-plane (4 and 2 chambers) LV End diastolic and systolic volumes (ml) were assessed by VVI, as were LA myocardial mechanics, [11] LA reservoir strain, LA volumes (as seen in Fig. 2): LA maximal volume indexed to body surface area (Vmax-I, The volume measured just before the opening of the mitral valve, coinciding with the end systole phase of the LV on the echocardiography (ECG) trace); LA minimum volume indexed to body surface area (Vmin-I, The volume measured at the closure of the mitral valve, coinciding with the end diastole phase of the LV on the ECG trace); total emptying volume indexed to body surface area (, equals to Vmax-I minus Vmin-I); Conduit volume indexed to body surface area, (equals to LV stroke volume indexed minus LA total emptying volume indexed); and LA reservoir strain (%).

An example of measurements obtained by endocardial surface manual tracing using a point and click approach in a patient with sinus rhythm with diastolic dysfunction. The volume acquired automatically with endocardial tracking performed by the VVI software thereafter

Left Atrial volumes and function, and the cardiac cycle acquired automatically by the VVI software following endocardial surface manual tracing using a point and click approach as seen in a patient with sinus rhythm on echocardiography
Statistical analysis
Statistical analysis was performed using MedCalc® (version 13.1.2.0, Belgium). Data are presented as mean ± standard deviations (SD). Comparisons between groups’ variables were performed using the analysis of variance (ANOVA), followed by Tukey post-hoc analyses. Receiver operating characteristic (ROC) analysis and curve were used with a stepwise approach to determine models, calculate Odds Ratio (OR), 95% Confidence Intervals (CI) and the areas under the curve (AUC). Youden index was used in order to obtain the sensitivity and specificity of the correlation between variables in the different models and defined classification variables. Pairwise comparison was used in the multivariate statistical analysis between different models. Uni- and multivariable associates of DD and heart failure symptoms were assessed by logistic regression analysis. Statistical significance was defined using a p value of less than 0.05.
Results
Clinical characteristics
As summarized in Table 1, compared to the normal diastolic function with sinus rhythm patients (ND group) or normal controls, DD patients in sinus rhythm and patients with AF were more than a decade older. Furthermore, the AF group had more hypertension and dyspnea, whereas the DD group did not. In comparison with the ND group, the DD group had more diabetes mellitus (DM) and chronic kidney disease (CKD), whereas the AF group did not.
Conventional 2-D Doppler echocardiographic characteristics
As summarized in Table 2, bi-plane LVEF was in the normal range (63% ± 4) and similar for all groups. Patients with DD and patients with AF demonstrated a higher calculated LV mass index, suggesting concentric LV hypertrophy. Pulmonary pressure showed gradual increments from normal controls through AF, ranging from normal values in the control group and the sinus ND group, to mildly elevated in patients with DD, and moderate pulmonary hypertension in the AF group.
Left ventricular myocardial mechanics
As summarized in Table 3, Bi-plane LV ejection fraction calculated by speckle tracking of endocardial contour and longitudinal strain were decreased in groups of patients in sinus rhythm with history of AF and was lowest in patients with AF at examination. GMSi was significantly lower in patients with current AF, representing LV micro-dyssynchrony in this group. The ratio of early diastolic to systolic strain rate (SR E/S) was significantly increased in patients in AF in comparison to all other groups.
Left atrial phasic volumes and myocardial mechanics
As summarized in Table 4, the volumes progressively increased from normal controls to ND group, DD group and the AF group, being the largest in patients in AF. The largest differences were noted in LA minimal volume index (Vmin-I). Functional parameters, such as the reservoir strain and diastolic emptying index (LA “ejection fraction”) were gradually decreased from normal controls to ND group, DD group and the AF group; passive emptying rate gradually decreased from normal controls to ND group and the DD group. Conduit volume remained with no significant difference among ND group, DD group and the AF group.
Association with DD (patients in sinus rhythm)
In order not to over-fit the model due to the small number of subjects and prevalence of DD, we needed to limit the number of variables in the model. At the first run we include age, LV functional parameters, and LA size and functional parameters. Age (HR = 1.12, CI 1.06–1.18, p < 0.0001) and Vmin-I (HR = 1.2, CI = 1.08–1.27, p < 0.0001) were the only associates of DD in a stepwise logistic regression analysis for all subjects in sinus rhythm (parameters rejected were: LVEF, LA total emptying volume, LA reservoir strain, and diastolic emptying index).. Re-running the model with other LV functional parameters, such as LV GLS, the ratio of early diastolic to systolic strain rate or pulmonary pressure replacing LVEF in the model, did not change the results, as they were all rejected. The ROCs for the association of DD to Vmin-I ≤ 16 ml/m2 alone vs. Vmin-I + age model were not different (AUC 83%) (Fig. 3a, b).

Receiver operating curves for association with DD and Dyspnea. Vmin-I LA minimal Volume index; Vmax-I LA maximal Volume index; Dia-empt-index Diastolic emptying index, (Vmax-I-Vmin-I)/Vmax-I; L-SR-E/S, longitudinal strain rate E to S ratio. a The association of LA minimal volume index (Vmin-I) with diastolic dysfunction in patients in sinus rhythm. b The association of age and Vmin-I model (coefficients derived from logistic regression) with diastolic dysfunction. c The association of Vmin-I with dyspnea/heart failure symptoms. d Comparison of various parameters for the association of heart failure symptoms
Association with heart failure symptoms (all patients)
Applying the same model to all patients with heart failure symptoms yielded Vmin-I as the single significant parameter associated with heart failure symptoms (HR = 1.04, CI 1.02–1.05, p < 0.0001) (Fig. 3c). Comparing ROCs for various parameters (Table 5, Fig. 3d) shows overlapping curves for Vmin-I and LA diastolic emptying index, both better and significantly different from the LV strain Rate E/S ratio and LA Vmax-I.
Creating a new association parameter—patient in sinus, with normal diastolic function (controls and patients with history of AF) vs. the rest of the study patients (patients in sinus rhythm with history of AF with diastolic dysfunction + patients in AF), Vmin-I remained as the single associate with heart failure symptoms, rejecting all other parameters in a stepwise logistic regression model. The hazard ratio (HR) of the latter group for heart failure was found to be HR = 38 (CI 5–293, p < 0.0001) with an AUC of 0.8, sensitivity of 63%, and specificity 96%.
Discussion
To the best of our knowledge, this is the first study that aims to find common LV/LA myocardial mechanics parameters to demonstrate DD, using STE in patients with AF.
Few studies are related to the subject of atrial dysfunction in circumstances of AF in patients with HFpEF. For example, our study may seem complementary to the work of Reddy et al. [22] which demonstrated the mechanical decline of LA function, resulting in AF, in patients with HFpEF. While the above mentioned study aimed to determine the consequence of LA dysfunction to emphasize the AF burden in HFpEF patients, the goal of our study was to find common LV/LA myocardial mechanics parameters, to demonstrate DD in patients with AF and associate these parameters with symptomatic HFpEF.
Patients with AF at the echocardiography examination and patients in sinus rhythm with DD were clinically and echocardiographically similar. In fact, DD augments the risk of developing AF and is probably the underlying mechanism for AF [7, 8, 23]. The high clinical and echocardiographic resemblance between AF and sinus-DD groups suggests a high rate of DD in patients with AF.
As seen in previous studies [24,25,26], Bi-plane LV ejection fraction calculated by speckle tracking of endocardial contour was decreased relatively to conventional 2-D Doppler echocardiographic assessment, due to the higher precision of determining end-systole and diastole together with defining the endocardial boundaries.
In patients in sinus rhythm, E/E’ and Vmin-I were significantly correlated with DD, while end systolic LA volume indexed (Vmax-I) was not. Notably, although E/E’ can be assessed in AF, mitral E velocities and annular E’ tissue velocities are not measured simultaneously and probably require averaging in multiple beats to bear significance [16]. Left atrial volumes (maximal, minimal, conduit and reservoir function) are measurable in AF and sinus rhythm. LA emptying directly represents LV filling, and is especially and probably less rate dependent, as both LA emptying and LV filling are measured in in the same cycle. Furthermore, in multiple-variable analysis, the left atrial minimal volume was correlated with both DD and presence of dyspnea/heart failure symptoms, indicating that the minimal volume of the atria during LV diastole and heart failure symptoms are likely related. Since the presence of DD cannot be accurately determined in the AF group, as no gold-standard is available, the study results suggest correlation of the minimal volume of the LA with symptoms of heart failure and raised filling pressures.
Patients presented with sinus rhythm and DD or AF had more symptoms of heart failure (HR = 38, CI 5–293, p < 0.0001) than patients presented with normal diastolic function and in sinus rhythm (controls and patients with history of AF). This high specificity that we found suggests that heart failure diagnosis could likely be excluded in patients in sinus rhythm and normal diastolic function with history of AF. In a multivariable model, Vmin-I was correlated with dyspnea more than any other parameters, including Vmax-I and SR E/S ratio which was previously found to correlate with LV end diastolic pressure [16]. Left atrial strain has been shown to aid in the categorization of DD [27]. The advantage of measuring the left atrial minimal volume is that it is simple to perform as a single volume measurement that can be derived from a conventional echocardiography assessment without the need of any software post-processing. In addition to association of LA with DD and HF symptoms, pulmonary hypertension is also presented by dyspnea and is a common complication of left HF. Pulmonary hypertension is also regarded as a component of the DD score, according to the latest guidelines [11]. In our study, pulmonary pressure was demonstrated to be significantly correlated with Vmin-I and may contribute to the mechanism of DD causing HF.
Katbeh, et al. [28] presented the diagnostic advantage of LA strain to differ between HFpEF and non-cardiac causes of dyspnea in patients with paroxysmal AF. As shown, our above results distinguish the probability of the existence of DD in AF patients, by means of measuring the minimal volume of the left atrium, a rhythm independent variable in order to suggest the presence of diastolic dysfunction in patients with suspected HFpEF, regardless of the heart rhythm they present during their examination, especially and notably, AF.
As previously published, Vmin correlates better to DD than Vmax [29]. Atrial volume is correlated to atrial fibrillation [30], The left atrial volume is affected by the various phases of the heart cycle and therefore it depends upon LV and LA systolic function, LV stiffness (reduced compliance) and geometry. All of these parameters define how the LA is passively filled, passively and actively emptied, and also how it remodels in size and stiffness. Stiffening and reduced compliance of the LA and LV can lead to an enlargement of the LA [12, 15], and thus may preserve the pressure gradients needed to maintain diastolic filling. LA size may also exceed the optimal sarcomere length of the LA myocytes and consequently reduces contractility. Diastolic function can be defined by not only the conventional Vmax-I, which reflects the size, but also by LA Vmin-I, which expresses both size and function. As we showed, Vmin-I was tightly related to the total LA diastolic emptying (LAEF). Therefore, high Vmin-I may indicate DD, which can be assessed regardless of cardiac rhythm, as an important tool for its estimation both in sinus rhythm and AF. As it is also associated with HF symptoms, it probably bears more than just a designation of DD and is likely a more comprehensive clinical informative parameter. Further studies are needed to assess its prognostic power as well.
The clinical significance of the study
Vmin demonstrated a strong correlation to dyspnea/HF and is thus proposed, as a simple, single, rhythm-independent variable that could be used to ascertain the presence of diastolic dysfunction in patients suspected of heavy diastolic dysfunction, regardless of their heart rhythm they have during their examination. The suggested measurement can be assessed at the bedside, as an efficient test that does not require extensive off-line post-processing tools and is usually already acquired in standard echocardiographic studies. The use of Vmin in standard echocardiographic studies could facilitate in reflecting a much more realistic quantification of incidence and prevalence of HFpEF, and thus may help identify patients at different risks of developing dyspnea and HF. If the right diagnosis can be made, progress to better treatment strategies may be found and thereafter could be offered to patients, with an impact that would perhaps reduce hospitalizations, the economic burden on the society, and may be eventually augment a better quality of life for patients as well. Secondly, based on our findings we could assume that a patient referred for an echocardiographic examination, following the history of AF, found in sinus rhythm with ND at the time of examination, has probably a very low risk of developing dyspnea or HF symptoms.
The left atrial minimal volume was significantly correlated with both diastolic dysfunction and symptomatic heart failure. Thus, the left atrial minimal volume may be used as a rhythm independent variable to suggest the presence of diastolic dysfunction in patients with suspected HFpEF, regardless of the heart rhythm they have during their examination. In addition to the presence of HF symptoms, we found that a Vmin-I cut off > 16 ml/m2, in the presence of sinus rhythm or AF, may suggest increased probability of HFpEF that might need a closer follow-up and earlier therapeutic intervention. Measuring Vmin-I is a simple, single, rhythm independent, bed-side, non-time consuming echocardiographic assessment, which does not require extensive off-line post processing tools and can be incorporated easily in a routine standard echocardiographic examination [13,14,15, 31, 32].
Limitations
The study was conducted retrospectively in a tertiary health care center. Selection bias cannot be excluded. Most patients were examined in an outpatient setting during a single visit, and therefore, medical data such as laboratory results (e.g. NT-proBNP) and follow-up assessments were unavailable. In addition, gold-standard measurements, such as cardiac catheterization, were also not available in this ambulatory setting. Offline analysis of echocardiographic exams was done by a single operator. Some echocardiographic studies were excluded due to inadequate echocardiographic quality for off-line strain analysis 3D strain and volume were not used, and this is due to the intention of applying methods used in real-life clinics. Excluded patients’ demographic and clinical characteristics did not differ from included patients. Naturally, patients with AF were much older and composed of a majority of women compared to the studied control group, composed of relatively young and healthy subjects, and therefore were not age nor sex matched. Furthermore, we acknowledge patient’s comorbidities could affect LA function and DD, and yet due to small size of groups we could not match groups by these different risk factors.
Conclusions
The left atrial minimal volume may be used to suggest the presence of DD in patients with AF and help with the identification of patients at high risk for developing HFpEF. The use of Vmin-I should be validated by larger multicenter studies. Furthermore, patients with a history of AF who undergo echocardiographic examination in sinus rhythm and demonstrate normal diastolic function at the time of examination may be at lower risk for developing HFpEF.
Availability of data and materials
The data is available from the corresponding author upon request.
Abbreviations
- DD:
-
Diastolic dysfunction
- HFpEF:
-
Heart failure with preserved ejection fraction
- HFrEF:
-
Heart failure with reduced ejection fraction
- AF:
-
Atrial fibrillation
- ND:
-
Normal diastolic function
- HF:
-
Heart failure
- LV:
-
Left ventricle
- LA:
-
Left atria
- LVEF:
-
Left ventricle ejection fraction
- AV:
-
Atrioventricular
- EDt:
-
E deceleration time
- GLS:
-
Global longitudinal strain
- GMSi:
-
Global mechanical synchrony index
- SR E/S ratio:
-
Systolic strain rate
- ECG:
-
Echocardiography
- SD:
-
Standard deviations
- HR:
-
Hazard ratio
- ANOVA:
-
Analysis of variance
- OR:
-
Odds ratio
- CI:
-
Confidence intervals
- AUC:
-
Areas under the curve
- DM:
-
Diabetes mellitus
- CKD:
-
Chronic kidney disease
References
Lam CS, Donal E, Kraigher-Krainer E, Vasan RS. Epidemiology and clinical course of heart failure with preserved ejection fraction. Eur J Heart Fail. 2011;13(1):18–28.
Lam CS, Carson PE, Anand IS, Rector TS, Kuskowski M, Komajda M, McKelvie RS, McMurray JJ, Zile MR, Massie BM, et al. Sex differences in clinical characteristics and outcomes in elderly patients with heart failure and preserved ejection fraction: the Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial. Circ Heart Fail. 2012;5(5):571–8.
Udelson JE. Heart failure with preserved ejection fraction. Circulation. 2011;124(21):e540-543.
Paulus WJ, Tschöpe C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539–50.
Borlaug BA, Paulus WJ. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur Heart J. 2011;32(6):670–9.
Penicka M, Vanderheyden M, Bartunek J. Diagnosis of heart failure with preserved ejection fraction: role of clinical Doppler echocardiography. Heart. 2014;100(1):68–76.
Rosenberg MA, Gottdiener JS, Heckbert SR, Mukamal KJ. Echocardiographic diastolic parameters and risk of atrial fibrillation: the Cardiovascular Health Study. Eur Heart J. 2012;33(7):904–12.
Rosenberg MA, Manning WJ. Diastolic dysfunction and risk of atrial fibrillation: a mechanistic appraisal. Circulation. 2012;126(19):2353–62.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–200.
Lanier GM, Vaishnava P, Kosmas CE, Wagman G, Hiensch R, Vittorio TJ. An update on diastolic dysfunction. Cardiol Rev. 2012;20(5):230–6.
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016;29(4):277–314.
Otani K, Takeuchi M, Kaku K, Haruki N, Yoshitani H, Tamura M, Abe H, Okazaki M, Ota T, Lang RM, et al. Impact of diastolic dysfunction grade on left atrial mechanics assessed by two-dimensional speckle tracking echocardiography. J Am Soc Echocardiogr. 2010;23(9):961–7.
Okamatsu K, Takeuchi M, Nakai H, Nishikage T, Salgo IS, Husson S, Otsuji Y, Lang RM. Effects of aging on left atrial function assessed by two-dimensional speckle tracking echocardiography. J Am Soc Echocardiogr. 2009;22(1):70–5.
Blume GG, McLeod CJ, Barnes ME, Seward JB, Pellikka PA, Bastiansen PM, Tsang TS. Left atrial function: physiology, assessment, and clinical implications. Eur J Echocardiogr. 2011;12(6):421–30.
Geyer H, Caracciolo G, Abe H, Wilansky S, Carerj S, Gentile F, Nesser HJ, Khandheria B, Narula J, Sengupta PP. Assessment of myocardial mechanics using speckle tracking echocardiography: fundamentals and clinical applications. J Am Soc Echocardiogr 2010, 23(4):351–369; quiz 453–355.
Garceau P, Carasso S, Woo A, Overgaard C, Schwartz L, Rakowski H. Evaluation of left ventricular relaxation and filling pressures in obstructive hypertrophic cardiomyopathy: comparison between invasive hemodynamics and two-dimensional speckle tracking. Echocardiography (Mount Kisco, NY). 2012;29(8):934–42.
Thomas L, Marwick TH, Popescu BA, Donal E, Badano LP. Left atrial structure and function, and left ventricular diastolic dysfunction: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(15):1961–77.
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1-39.e14.
Quiñones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA. Recommendations for quantification of Doppler echocardiography: a report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr. 2002;15(2):167–84.
Carasso S, Williams LK, Hazanov Y, Halhla Y, Ghanim D, Amir O. Comparison of echocardiographic parameters between pre-clinical and clinical advanced diastolic dysfunction patients. Int J Cardiol. 2016;224:165–9.
Takamura T, Dohi K, Onishi K, Tanabe M, Sugiura E, Nakajima H, Ichikawa K, Nakamura M, Nobori T, Ito M. Left ventricular contraction-relaxation coupling in normal, hypertrophic, and failing myocardium quantified by speckle-tracking global strain and strain rate imaging. J Am Soc Echocardiogr. 2010;23(7):747–54.
Reddy YNV, Obokata M, Verbrugge FH, Lin G, Borlaug BA. Atrial dysfunction in patients with heart failure with preserved ejection fraction and atrial fibrillation. J Am Coll Cardiol. 2020;76(9):1051–64.
Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, Tu JV, Levy D. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the framingham heart study of the national heart, lung, and blood institute. Circulation. 2009;119(24):3070–7.
Carasso S, Cohen O, Mutlak D, Adler Z, Lessick J, Reisner SA, Rakowski H, Bolotin G, Agmon Y. Differential effects of afterload on left ventricular long- and short-axis function: insights from a clinical model of patients with aortic valve stenosis undergoing aortic valve replacement. Am Heart J. 2009;158(4):540–5.
Carasso S, Mutlak D, Lessick J, Reisner SA, Rakowski H, Agmon Y. Symptoms in severe aortic stenosis are associated with decreased compensatory circumferential myocardial mechanics. J Am Soc Echocardiogr. 2015;28(2):218–25.
Carasso S, Cohen O, Mutlak D, Adler Z, Lessick J, Aronson D, Reisner SA, Rakowski H, Bolotin G, Agmon Y. Relation of myocardial mechanics in severe aortic stenosis to left ventricular ejection fraction and response to aortic valve replacement. Am J Cardiol. 2011;107(7):1052–7.
Singh A, Addetia K, Maffessanti F, Mor-Avi V, Lang RM. LA strain for categorization of LV diastolic dysfunction. JACC Cardiovasc Imaging. 2017;10(7):735–43.
Katbeh A, De Potter T, Geelen P, Di Gioia G, Kodeboina M, Balogh Z, Albano M, Vanderheyden M, Bartunek J, Barbato E et al. Heart failure with preserved ejection fraction or non-cardiac dyspnea in paroxysmal atrial fibrillation: The role of left atrial strain. Int J Cardiol 2020.
Russo C, Jin Z, Homma S, Rundek T, Elkind MS, Sacco RL, Di Tullio MR. Left atrial minimum volume and reservoir function as correlates of left ventricular diastolic function: impact of left ventricular systolic function. Heart. 2012;98(10):813–20.
Wang WH, Hsiao SH, Lin KL, Wu CJ, Kang PL, Chiou KR. Left atrial expansion index for predicting atrial fibrillation and in-hospital mortality after coronary artery bypass graft surgery. Ann Thorac Surg. 2012;93(3):796–803.
Williams LK, Chan RH, Carasso S, Durand M, Misurka J, Crean AM, Ralph-Edwards A, Gruner C, Woo A, Lesser JR, et al. Effect of left ventricular outflow tract obstruction on left atrial mechanics in hypertrophic cardiomyopathy. Biomed Res Int. 2015;2015:481245.
Schweitzer A, Agmon Y, Aronson D, Abadi S, Mutlak D, Carasso S, Walker JR, Lessick J. Assessment of left sided filling dynamics in diastolic dysfunction using cardiac computed tomography. Eur J Radiol. 2015;84(10):1930–7.
Acknowledgements
Not applicable.
Funding
No funding was provided.
Author information
Authors and Affiliations
Contributions
ABA performed data collection and wrote the manuscript; DG designed the study and performed critical review of the manuscript, EH interpreted the findings and performed critical revision of the article; GR interpreted the findings and performed critical revision of the article; IM performed data collection and interpreted the findings; LGR interpreted the findings and wrote the manuscript; EK designed the study, interpreted the findings, and approved the final manuscript; OA designed the study and approved the final manuscript. SC designed the study, data collection and analysis and approved the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate consent for publication
The study protocol was reviewed and approved by the Poriya Medical Center’s Ethical Review Board. Verbal informed consent was obtained from each patient prior to participating in the study. Consent for publication – Not Applicable, the manuscript contains no potentially identifying information. The research study was conducted in accordance with the World Medical Association Declaration of Helsinki.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ben-Arzi, A., Hazanov, E., Ghanim, D. et al. Left atrial minimal volume: association with diastolic dysfunction and heart failure in patients in sinus rhythm or atrial fibrillation with preserved ejection fraction. BMC Med Imaging 21, 76 (2021). https://doi.org/10.1186/s12880-021-00606-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-021-00606-3