
Abstract
Background
An improper host immune response to Mycoplasma pneumoniae generates excessive inflammation, which leads to the impairment of pulmonary ventilation function (PVF). Azithromycin plus inhaled terbutaline has been used in the treatment of Mycoplasma pneumoniae pneumonia (MPP) in children with impaired pulmonary function, but previous randomized controlled trials (RCTs) showed inconsistent efficacy and safety. This study is aimed to firstly provide a systematic review of the combined therapy.
Methods
This study was registered at the International Prospective Register of Systematic Reviews (PROSPERO CRD42023452139). A PRISMA-compliant systematic review and meta-analysis was performed. Six English and four Chinese databases were comprehensively searched up to June, 2023. RCTs of azithromycin sequential therapy plus inhaled terbutaline were selected. The revised Cochrane risk of bias tool for randomized trials (RoB2) was used to evaluate the methodological quality of all studies, and meta-analysis was performed using Stata 15.0 with planned subgroup and sensitivity analyses. Publication bias was evaluated by a funnel plot and the Harbord’ test. Certainty of evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation recommendations.
Results
A total of 1,938 pediatric patients from 20 RCTs were eventually included. The results of meta-analysis showed that combined therapy was able to significantly increase total effectiveness rate (RR = 1.20, 95%CI 1.15 to 1.25), forced expiratory volume in one second (SMD = 1.14, 95%CIs, 0.98 to 1.29), the ratio of forced expiratory volume in one second/forced vital capacity (SMD = 2.16, 95%CIs, 1.46 to 2.86), peak expiratory flow (SMD = 1.17, 95%CIs, 0.91 to 1.43). The combined therapy was associated with a 23% increased risk of adverse reactions compared to azithromycin therapy alone, but no significant differences were found. Harbord regression showed no publication bias (P = 0.148). The overall quality of the evidence ranged from moderate to very low.
Conclusions
This first systematic review and meta-analysis suggested that azithromycin sequential therapy plus inhaled terbutaline was safe and beneficial for children with MPP. In addition, the combined therapy represented significant improvement of PVF. Due to lack of high-quality evidence, our results should be confirmed by adequately powered RCTs in the future.
Similar content being viewed by others

Introduction
Mycoplasma pneumoniae (M. pneumoniae) is one of the most important pathogens for community-acquired pneumonia in hospitalized children [1]. As reported, M pneumoniae was detected in nearly 50% of the specimens of hospitalized children with acute respiratory infection in some cities of China [2]. It is estimated that approximately 5–12% of the hospitalized children with Mycoplasma pneumoniae pneumonia (MPP) were admitted to the intensive care unit [3]. An improper host immune response to M. pneumoniae generates excessive inflammation, which causes the impairment of pulmonary ventilation function (PVF) affecting both the large and small airways [4, 5].
According to the latest guidelines for MPP in China, macrolides represented by azithromycin have been the first-line antibiotics against M. pneumoniae [6]. To reduce complications such as pain and infection caused by intravenous injection, azithromycin sequential therapy (sequential switch from intravenous formulation to oral formulation) is applied as a new mode of antibiotic use in clinic. It is currently believed that MPP is a combination of a direct pathogen invasion and immune injury [7, 8].Thus, seeking for medication to reduce excessive immune reactions and improve PVF is urgently needed. Terbutaline has been widely used to improve lung resistance and reduce the incidence of respiratory distress, for example in asthma [9]. This \({{\beta }}_{2}\)-agonist can relax bronchial smooth muscles, inhibit the release of endogenous spasmogenic substances and endogenous neurotransmitter-induced edema, and improve the clearance ability of bronchial mucosa cilia [10]. Terbutaline was well tolerated without irreversible adverse effects [9], and could decrease the incidence of acute respiratory failure in children with severe asthma exacerbations [11].
Currently, aerosols of terbutaline have been widely used in China [10], and there have been increasing number of randomized controlled trials (RCTs) on the efficacy and safety of azithromycin sequential therapy plus inhaled terbutaline for pediatric MPP, but they showed inconsistent results. This study is aimed to firstly provide a well-powered support on the combination therapy for MPP through a systematic review and meta-analysis.
Materials and methods
Protocol registration and reporting
The study protocol was registered at the International Prospective Register of Systematic Reviews (CRD42023452139). This systematic review was designed based on the Cochrane Handbook for Systematic Reviews of Interventions [12] and was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [13] (see Appendix S11).
Eligibility criteria
The strict PICOS framework is as follows:
(P) Participants
After laboratory tests and imaging tests, children (aged ≤ 16 years old) were diagnosed with MPP without any underlying serious disease or other acute infectious disease. Only the studies in which the clinical diagnostic criteria followed clinical guidelines or expert consensus were considered [14, 15]. Alternatively, the diagnosis of MPP was based on relevant clinical symptoms and chest imaging tests plus microbiologic tests by one of the following methods: culture, polymerase chain reaction (PCR) testing or serologic tests [6].
(I) Intervention
Azithromycin sequential therapy (sequential switch from intravenous formulation to oral formulation of azithromycin when the patient has an adequate clinical response and can efficiently absorb orally administered medication [16]) plus inhaled terbutaline was used for intervention group.
(C) Control
Azithromycin sequential therapy alone was used for control group. There was no restriction on drug dose in either group. When necessary, researchers should administer basic treatments such as reducing fever, relieving cough, expectoration, and so on.
(O) Outcomes
The primary outcomes were total effectiveness rate (TER) and the incidence of total adverse events (TAEs). The clinical responses were classified as cure (complete disappearance of all signs and symptoms of pneumonia with complete regression of infiltrate on control chest radiograph), improvement (defervescence with incomplete disappearance of other signs and symptoms of pneumonia with partial regression of infiltrate on control chest radiograph, and without need for additional antimicrobial therapy), or failure (lack of improvement or progression or recurrence of signs and symptoms of pneumonia after the treatment) [16]. Total effective rate = (number of cured patients + number of improved patients)/total number of patients× 100% [17]. TAEs mainly include nausea, vomiting, abdominal distension, abdominal pain, diarrhea, headache, rash and so on. The secondary outcomes included pulmonary function indexes, such as forced expiratory volume in one second (FEV1), the ratio of forced expiratory volume in one second/forced vital capacity (FEV1/FVC) and peak expiratory flow (PEF); Clinical symptom indexes: time to disappearance of fever, cough as well as lung rales, time to relief of asthma and return to normal of chest X-ray; Inflammation indicators: C-reactive protein (CRP), tumor necrosis factor-alpha (TNF-α), interleukin-2 (IL-2), interleukin-4 (IL-4), interleukin-6 (IL-6) and interleukin-8 (IL-8).
(S) Study design
RCTs published in English or Chinese. For different studies with the same research object, the latest research results were adopted.
Exclusion criteria
The exclusion criteria are as follows:
-
1)
Patients were treated with detailed interventions other than azithromycin and terbutaline in their studies, such as glucocorticoids, special nursing, and traditional Chinese medicine;
-
2)
The treatment duration or efficacy assessment was unclear;
-
3)
Patients who did not receive a clear standard of diagnosis or treatment;
-
4)
Clinical studies that did not correctly describe randomized grouping methods. Their design was actually retrospective, observational study with controls.
-
5)
There were no full text, incomplete articles, or duplicate publications.
Search methods for identification of studies
Medline, Embase, Web of Science, Science Direct, Cochrane Library, Epistemonikos, CBM, CNKI, Wan-Fang and CQVIP databases were comprehensively searched up from database inception to June 2023. The search terms included: Mycoplasma pneumonia, Mycoplasma infection, MPP, primary atypical pneumonia, Mycoplasma ovipneumoniae infection, Mycoplasma dispar infection, azithromycin, and terbutaline (see Appendix S1 for full details of the search strategy).
All relevant studies were retrieved based on consensus, and the reference lists of the selected articles were further searched for additional relevant studies.
Data collection and extraction
Two researchers (YCS and YL) independently completed the study screening, data extraction by using NoteExpress and Excel. Disagreements were resolved through discussion or with the assistance of DYK. Studies were initially screened based on the title and abstract, followed by full-text screening. The following basic data were extracted: (1) year of publication and first author’s name; (2) patient age; (3) course of disease; (4) sample size; (5) sex ratio; (6) therapy regime of the intervention and control groups; (7) treatment duration; and (8) details of outcomes.
Assessment of risk of bias in included studies
The risk of bias of each included study was assessed using five dimensions of the revised Cochrane risk of bias tool for randomized trials (RoB2) [18]. Studies were graded as “low risk”, “some concerns”, or “high risk”, resulting in an overall bias assessment. YCS and YL independently rated all the articles. Conflicting ratings were discussed and resolved by consensus.
Statistical analysis
The full meta-analysis was performed using Stata 15.0 and the results are represented as forest maps. Relative risk (RR) was used to calculate the effect for dichotomous variables, while standardized mean difference (SMD) was used for continuous variables. Each effect size provides a 95% confidence interval (CI). The heterogeneity among the studies was evaluated by Chi-square test (α = 0.1), and the differences in heterogeneity were evaluated by \({I}^{2}\). If there was no significantly statistical heterogeneity among the results, the fixed-effect model was used for statistical analysis. On the contrary, the main sources of relevant heterogeneity should be further analyzed. After excluding the influencing factors of clinical heterogeneity, the random-effect model was used for the statistical analysis. A rough choice between fixed- and random-effect meta-analysis was as follows: when\({I}^{2}\) < 50%, a fixed-effect model was chosen to analyze the data. In contrast, when \({I}^{2}\)≥ 50%, a random-effect model was used for statistical analysis. For all the test in these analyses, the statistical significance level was set in P < 0.05. If there was significant clinical heterogeneity, subgroup analysis or leave-one-out sensitivity analysis was used. A subgroup analysis with treatment durations was conducted. In addition, considering the quality of the original studies, we performed sensitivity analyses excluding trials at high risk of bias.
Assessment of publication bias
To assess the risk of publication bias, we used funnel plots for visual inspection. Harbord regression was performed to assess publication bias, and if the hypothesis test P > 0.1, there was no significant publication bias.
GRADE approach assessment
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach [19, 20] was used to assess the certainty of evidence in primary outcomes and pulmonary function indexes. The assessment criteria in the previous study were referred [21]. The GRADE approach categorizes the quality of evidence on four levels ranging from high to very low, with low levels of evidence indicating that future trials with high quality are likely to change the estimates.
Results
Description of studies
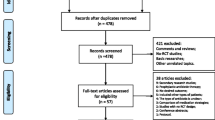
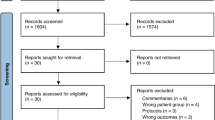
The search process revealed 598 articles, and a total of 20 RCTs were ultimately included, as shown in Fig. 1 (see Appendix S2 for the full reference list). A total of 1,938 children (1,061 boys and 877 girls) participated, including 969 patients in the intervention group and 969 patients in the control group. They all came from China. All included children were patients with general MPP. The median age of the enrolled children was 5.32 years with a range of 0.33 ~ 13 years. The median course of disease was 4.00 days with a range of 1 ~ 28 days. Sixteen RCTs were conducted on one cycle of azithromycin sequential therapy (14 days) while 4 studies doubled the cycle of sequential therapy, that was 28 days. The common regimen of azithromycin sequential therapy was as follows: (1) azithromycin: 10 mg/(kg·d), qd (for 3–5 consecutive days), and ivgtt; (2) azithromycin therapy was stopped for 4 days; (3) azithromycin dry suspension: 10 mg/(kg·d), qd (for 3 days), and po; (4) azithromycin was stopped for 4 days. Terbutaline inhalation regimen was as follows: 2.5 mg (in 5 mL of 0.9% sodium chloride) at one time, and bid (the treatment time was the same as that of azithromycin). The basic characteristics of all included studies are shown in Table 1(see Appendix S3 for information on the diagnostic criteria and therapy regimens for each included RCT; see Appendix S4 for the characteristics of patient age and course among the 20 RCTs).

Flow diagram of studies considered for inclusion
Risk of bias in included studies
Figure 2 showed an overview of the risk of bias assessment, and the quality of the included RCTs was overall moderate according to the intention-to-treat principle. A more detailed description of the risk of bias assessment for each study can be found in Appendix S5. Six studies (30%) were assessed to have an overall high risk of bias while fourteen (70%) were assessed to have “some concerns” regarding their overall bias. The most common reason for a high risk was missing outcome data (for incomplete drop-out information). However, there are several some potential risks of bias, such as inadequate blinding of assessors and selection of the reported result, due to the lack of pre-registration of RCTs.

Overview of risk of bias assessment according to the revised Cochrane risk of bias tool for randomized trials (Rob2). Each colored area represents the percentage of studies in the respective bias assessments categories
Results of primary outcomes
TER
A total of 18 RCTs reported TER, and the analysis included 885 patients in each group. The meta-analysis revealed no obvious heterogeneity (\({I}^{2}\)=26.5%, P = 0.145). Therefore, the fixed-effect model was selected for meta-analysis. The results showed that TER of the intervention group was significantly higher than that of the control group for the treatment of pediatric MPP (RR = 1.22, 95%CI 1.17 to 1.27, Z = 9.64, P < 0.001; Appendix S6.1 A). In fact, fixed-effect meta-analyses ignore heterogeneity. However, there are often many clinical characteristics that vary across studies. Thus, a random-effect model would be better for meta-analyses and we found that the result based on random-effect model changed slightly (RR = 1.20, 95%CI 1.15 to 1.25, Z = 8.06, P < 0.001; Fig. 3A).

Results of meta-analysis for primary outcomes. A, Total effectiveness rate (TER); B, Incidence of total adverse events (TAEs)
Incidence of TAEs
The incidence of TAEs was evaluated according to the outcomes from 14 RCTs with 702 patients in each group. Regarding no obvious heterogeneity (\({I}^{2}\)=0.0%, P = 0.805), meta-analysis of fixed-effect model showed that the incidence of TAEs in the intervention group was higher than that of the control group in the treatment of MPP, but there was no significant difference between the two groups (RR = 1.20, 95%CI 0.91 to 1.59, Z = 1.27, P = 0.205; Appendix S6.1B). According to random-effect model, the confidence interval estimates were wider (RR = 1.23, 95%CI 0.92 to 1.64, Z = 1.41, P = 0.159; Fig. 3B). The main adverse events, such as nausea and vomiting, abdominal distension, abdominal pain, diarrhea, headache and rash, were common (1–10%) according to the criteria of the Council for International Organizations of Medical Sciences. These adverse reactions were mild and disappeared spontaneously after stopping the medication, and there was no significant difference in different adverse events between the two groups (see Appendix S10).
Results of secondary outcomes
Outcomes of pulmonary function indexes
FEV1
Eight RCTs with 354 patients in each group were included to investigate how azithromycin sequential therapy plus inhaled terbutaline affected FEV1. As no significant interstudy heterogeneity (\({I}^{2}\)=0%, P = 0.962) was observed, the fixed-effect model was used and the results showed that FEV1 of the intervention group was significantly higher than that of the control group (SMD = 1.14, 95%CI 0.98 to 1.29, Z = 9.64, P < 0.001; Fig. 4A).

Results of meta-analysis for outcomes of pulmonary function indexes. A, Forced expiratory volume in one second (FEV1); B, the ratio of Forced expiratory volume in one second/Forced vital capacity (FEV1/FVC); C, Peak expiratory flow (PEF)
Ratio of FEV1/FVC
Seven studies were included to investigate the difference in the ratio of FEV1/FVC between the two groups. The analysis showed that there were 314 patients in each group. There was obvious heterogeneity (\({I}^{2}\)=92.0%, P< 0.001), and meta-analysis results of random-effect model showed that the ratio of FEV1/FVC in the intervention group was significantly higher than that in the control group (SMD = 2.16, 95%CI 1.46 to 2.86, Z = 6.04, P < 0.001; Fig. 4B).
PEF
Eight RCTs with 354 patients in each group reported PEF. The random-effect model was selected for meta-analysis because of its obvious heterogeneity (\({I}^{2}\)=61.6%, P = 0.011) and PEF in the intervention group was significantly higher than that in the control group (SMD = 1.17, 95%CI 0.91 to 1.43, Z = 8.84, P < 0.001; Fig. 4C).
Outcomes of clinical symptom indexes
A total of 13, 13, 13, 5 and 3 RCTs reported the time to disappearance of clinical symptoms, in term of fever, cough, lung rales, asthma relief, and return to a normal chest X-ray, respectively. The random-effect model was used due to relatively high heterogeneity, and the results demonstrated that the intervention group had significantly shorter time than the control group. The pooled results are shown in Table 2 and Appendix S6.
Outcomes of inflammatory indicators
There were respectively 6, 8, 5, 4, 5 and 4 RCTs reported levels of inflammatory indicators, namely, CRP, TNF-α, IL-2, IL-4, IL-6 and IL-8. Two indicators had no obvious heterogeneity but four outcomes did. The meta-analysis results of random-effect model showed an obviously increased level of IL-4 and lower levels of other inflammatory indicators in the intervention group than those in the control group. The pooled results are shown in Table 3 and Appendix S6.
Subgroup analysis of different treatment durations
We conducted subgroup analysis based on treatment duration using data from 14 RCTs with a duration of 14 days and 4 RCTs of with a duration of 28 days (see Appendix S7). Regarding the duration of 14 days, a random-effect meta-analysis using data from 14 RCTs yielded an RR of 1.22 for TER by the intervention group compared with the control group (95% CI 1.17 to 1.28, Z = 8.75, P < 0.001) with no heterogeneity (\({I}^{2}\)=0.0%, P for heterogeneity = 0.998). However, regarding the duration of 28 days, the pooled RR for TER in the intervention group compared with the control group was 1.17 (95%CI 1.01 to 1.25, Z = 2.16, P < 0.001) with substantial heterogeneity (\({I}^{2}\)=71.7%, P = 0.014). This subgroup analysis suggested that TER at14 days was higher than that at 28 days, and TER of both subgroups was significantly higher than that of the control group.
Sensitivity analysis
We found that high heterogeneity appeared when conducting meta-analyses. Therefore, we further conducted leave-one-out sensitivity analysis to explore the potential source of heterogeneity, and there was no substantial modification of our estimates after the exclusion of individual studies one by one (see Appendix S8.1-2). The sensitivity analysis showed that the results were statistically robust. A further sensitivity analysis excluding all trials judged to be at high risk of bias confirmed these substantial results (see Appendix S8.3-6). Thus, we believe that the high heterogeneity may arise from the following factors: course of disease, treatment duration and the differences in measurements of the included trials.
Publication bias
The funnel plot of TER was asymmetrical upon visual inspection while the funnel plot of the incidence of TAEs was symmetric. The results of the Harbord linear regression showed that there was a potential risk of publication bias in TER (P < 0.001) and no significant publication bias in the incidence of TAEs (P = 0.148; see Appendix S9).
GRADE Certainty of evidence
The certainty of the evidence for the primary outcomes and pulmonary function indexes ranged from moderate to very low, as tabulated in the summary of findings table (Table 4). The reasons for downgrading the evidence included reporting bias, publication bias, inadequate precision, and heterogeneity.
Discussion
In our study, the results showed that azithromycin sequential therapy plus inhaled terbutaline had higher efficacy (low-certainty evidence) and no more adverse reactions (moderate-certainty evidence) than azithromycin therapy alone.
This study showed that the combined therapy could increase the total efficacy by 20% compared to azithromycin therapy alone, suggesting that active treatment for MPP is highly important. Subgroup analysis of TER showed that different treatment durations could be potential causes of heterogeneity, but more RCTs of 28-day duration are needed to confirm these finding. In addition, no increase in efficacy was found after 28 days of therapy, which indicated that macrolide-resistant M. pneumoniae might develop after longer durations of azithromycin therapy and that patients cannot benefit from this therapy.
To avoid damage to pulmonary function, terbutaline was added to azithromycin sequential therapy to dilate the bronchus and promote pulmonary ventilation. Compared with the control treatment, the combined therapy improved FEV1 and the ratio of FEV1/FVC. Studies have shown that PEF can be used to screen impaired pulmonary function when spirometry is unavailable [22]. Our pooling results also showed that the intervention group had better PEF than the control group. The improvement in FVF could be confirmed by the time to the disappearance of cough, lung rales and asthma. The time of other clinical symptoms, such as fever and chest X-ray, also showed good improvement.
Host protein assays based on CRP are widely used in the diagnosis of community-acquired pneumonia, but CRP alone cannot be used to precisely separate bacterial from viral infection and mild from severe disease [23]. In the context of M. pneumoniae infection, it stimulates epithelial cells and macrophages to release a variety of cytokines, including pro-inflammatory cytokines (TNF-α, IL-2, IL-6, and IL-8) and anti-inflammatory cytokines (for example, IL-4) [7, 24]. The induction of pro-inflammatory cytokines is extensively involved in MPP development and can cause excessive immune inflammation, which includes local inflammation, airflow obstruction, air-way remodeling, emphysema and impaired lung function [24]. In our study, the levels of these pro-inflammatory cytokines in the intervention group were lower than those in the control group, suggesting that the combined therapy could downregulate the levels of pro-inflammatory factors and prevent the aggravation of MPP. Cytokines produced by \({\text{T}\text{h}}_{1}\) cells can be blocked by IL-4 produced by \({\text{T}\text{h}}_{2}\) cells and the \({\text{T}\text{h}}_{1}\)/\({\text{T}\text{h}}_{2}\) balance plays a significant role in anti-infectious immunity [25]. Therefore, the level of IL-4 in the intervention group was higher than that in the control group. The levels of pro-inflammatory cytokines decreased and anti-inflammatory cytokines increased in children with MPP, indicating that these cytokines are promising biomarkers for the diagnosis and treatment of this disease in clinical practice.
Compared with previous meta-analyses for MPP, there are a few points to be noted: Firstly, most of studies seemed to have unclear definitions of the diagnostic criteria for MPP [26,27,28], while the clinical symptoms of this disease are similar to those of viral and bacterial respiratory tract infections [5, 27], and Zhang et al [29]. even recruited patients regardless of the disease intensity. Secondly, the included interventions for MPP were not strict because extra medications such as acupuncture or special nursing were used in some studies [28, 30]. Thirdly, an observational study with controls, in which the patients were grouped by therapy regimens [27], could not be identified as an RCT, because it is highly likely that this was a retrospective analysis of clinical cases. In contrast, our study proposed a clear PICOS framework to decrease clinical and methodological heterogeneity.
To the best of our knowledge, this is the first systematic review and meta-analysis of azithromycin sequential therapy plus inhaled terbutaline for children with MPP. A comprehensive search was performed to obtain all relevant RCTs in our study and we paid more attention to pulmonary function indexes. Previous meta-analyses have reported overall response rate, total safety, improvement time of clinical symptoms and levels of inflammatory factors [31,32,33], while our study involved FEV1, the ratio of FEV1/FVC and PEF, which are the gold standards for the diagnosis of impaired pulmonary function [22]. To avoid misdiagnosis, pathogen identification was added as one of the inclusion criteria, which has never been highlighted before. We excluded some observational studies with controls to reduce methodological heterogeneity, which was different from previous meta-analyses [27]. This study was registered ahead of writing and performed in accordance with the PRISMA Checklist to reduce reporting bias as much as possible.
However, there were some limitations in our study. Firstly, the main limitation was the significant heterogeneity observed across the included studies. This heterogeneity remained in subgroup analyses of children stratified by treatment duration, which indicated that clinical characteristics such as age, onset time of MPP, and outcome measurements might be potential sources of bias. Although significant heterogeneity was detected, sensitivity analyses showed that the pooled results were statistically robust. Secondly, due to the overall moderate risk of bias and moderate to very low certainty of evidence, the results of this study should be interpreted with caution and high-quality RCTs are urgently needed. Thirdly, there was some risk in publication bias of TER and all included RCTs were conducted in China, whose underrepresentation could lead to inapplicable or non-generalizable results. More publications of relevant trials performed by researchers from different language backgrounds are needed to confirm the findings of the study. Fourthly, what element of any benefits attributed to terbutaline may in fact be a placebo in nature is difficult to estimate without blinded RCTs [34]. Fifthly, the inflammatory indicators including CRP, TNF-α, and IL-2 have potential prognostic value as diagnostic biomarkers for MPP, as well as make meta-analyses more valuable [35]. However, only a few studies have examined inflammatory indicators, which makes it difficult to analyze the immune response patterns of the host [36].
Conclusions
This is the first systematic review and meta-analysis of azithromycin combined with terbutaline, which has shown good efficacy and safety. In addition, PVF and the levels of relevant indexes were significantly improved. However, there was no high-quality evidence and the results of this study should be interpreted with caution. Thus, we conditionally recommend azithromycin sequential therapy plus inhaled terbutaline for children with MPP. High-quality RCTs are needed to ensure safe medication practices for the combined therapy. In addition, the precise mechanism underlying effects of the combined therapy and inflammatory factors requires further in-depth study.
Data availability
All data generated or analyzed during the present study are included in this published article and Appendix.
Abbreviations
- MPP:
-
Mycoplasma pneumoniae pneumonia
- PVF:
-
Pulmonary ventilation function
- RCTs:
-
Randomized controlled trials
- PRISMA:
-
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROSPERO:
-
The International Prospective Register of Systematic Reviews
- RoB2:
-
The revised Cochrane risk of bias tool for randomized trials
- TER:
-
Total effectiveness rate
- FEV1:
-
Forced expiratory volume in one second
- FEV1/FVC:
-
Forced expiratory volume in one second/forced vital capacity
- PEF:
-
Peak expiratory flow
- M. pneumoniae :
-
Mycoplasma pneumoniae
- PICOS:
-
P–participants; I–intervention; C–control; O–outcomes; S–study design
- TAEs:
-
Total adverse events
- CRP:
-
C-reactive protein
- TNF-α:
-
Tumor necrosis factor-alpha
- IL-2:
-
Interleukin-2
- IL-4:
-
Interleukin-4
- IL-6:
-
Interleukin-6
- IL-8:
-
Interleukin-8
- RR:
-
Relative risk
- SMD:
-
Standardized mean difference
- CI:
-
Confidence interval
References
Tong L, Huang S, Zheng C, Zhang Y, Chen Z. Refractory Mycoplasma pneumoniae Pneumonia in Children: early recognition and management. J CLIN MED 2022, 11(10).
Su M, Wang Q, Li D, Wang LL, Wang CY, Wang JL, Zhang Q, Du LY, Liu JY, Xie GC. Prevalence and clinical characteristics of hospitalized children with community-acquired Mycoplasma pneumoniae pneumonia during 2017/2018, Chengde, China. Medicine. 2021;100(5):e23786.
Guo Q, Li L, Wang C, Huang Y, Ma F, Cong S, Tan J, Yao L, Chen A, Zheng L. Comprehensive virome analysis of the viral spectrum in paediatric patients diagnosed with Mycoplasma pneumoniae pneumonia. VIROL J. 2022;19(1):181.
Leng J, Yang Z, Wang W. Diagnosis and Prognostic Analysis of Mycoplasma pneumoniae Pneumonia in Children Based on High-Resolution Computed Tomography. CONTRAST MEDIA MOL I 2022, 2022:1985531.
Li W, Liu T, Yao M, Yu R, Shu M, Zhang M, Huang J. Effect of interesting respiratory rehabilitation training for the treatment of refractory Mycoplasma pneumoniae pneumonia in children. BMC INFECT DIS. 2023;23(1):561.
China NHCO. Guidelines for the diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2023 edition). Inter J Epidemiol Infect Dis 2023, 50(2).
Yin L, Ma Y, Wang W, Zhu Y. The critical function of miR-1323/Il6 axis in children with Mycoplasma pneumoniae pneumonia. J PEDIAT-BRAZIL. 2021;97(5):552–8.
Zhang H, Sun C, Yu Z. Effect of azithromycin sequential therapy combined with budesonide nebulization on chest CT changes in children with mycoplasma pneumonia. MINERVA GASTROENTERO. 2023;69(3):447–9.
Doymaz S, Schneider J. Safety of Terbutaline for treatment of acute severe Pediatric Asthma. PEDIATR EMERG CARE. 2018;34(5):299–302.
Bian F, Wu YE, Zhang CL. Use of aerosol inhalation treatment with budesonide and terbutaline sulfate on acute pediatric asthmatic bronchitis. EXP THER MED. 2017;14(2):1621–5.
Doymaz S, Schneider J, Sagy M. Early administration of terbutaline in severe pediatric asthma may reduce incidence of acute respiratory failure. ANN ALLERG ASTHMA IM. 2014;112(3):207–10.
Higgins JPTTJCJ. Cochrane Handbook for Systematic Reviews of Interventions version 6.4updated August (2023). In.: Cochrane; 2023.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ-BRIT MED J. 2021;372:n71.
Association RBOC. Expert consensus on diagnosis and treatment of mycoplasma pneumoniae pneumonia. Chin J Appl Clin Pediatr 2015, 30(17).
Jiang ZF, Shen KL, Shen Y. Zhu Futang Practical Pediatrics, 8th edition edn. Beijing: People’s Medical Publishing House; 2014.
Kuzman I, Daković-Rode O, Oremus M, Banaszak AM. Clinical efficacy and safety of a short regimen of azithromycin sequential therapy vs standard cefuroxime sequential therapy in the treatment of community-acquired pneumonia: an international, randomized, open-label study. J Chemother. 2005;17(6):636–42.
Sheng Y, Liu X, Wang Q, Zhang Y, Huang L, Hu D, Ren P, Hong Q, Kang D. Herbal Granules of Heat-Clearing and Detoxifying for Children with Mild Hand, Foot, and Mouth Disease: A Bayesian Network Meta-Analysis. EVID-BASED COMPL ALT 2022, 2022:6818406.
Sterne J, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ-BRIT MED J. 2019;366:l4898.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schunemann HJ. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ-BRIT MED J. 2008;336(7650):924–6.
Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, Vist GE, Falck-Ytter Y, Meerpohl J, Norris S, et al. GRADE guidelines: 3. Rating the quality of evidence. J CLIN EPIDEMIOL. 2011;64(4):401–6.
Santos FF, Lourenço BM, Souza MB, Maia LB, Oliveira VC, Oliveira MX. Prevention of low back and pelvic girdle pain during pregnancy: a systematic review and meta-analysis of randomised controlled trials with GRADE recommendations. PHYSIOTHERAPY. 2023;118:1–11.
Hansen M, Schmid JM. Screening for impaired pulmonary function using peak expiratory flow: performance of different interpretation strategies. RESPIR MED RES-FRANC. 2023;83:101015.
Wang H, Zhou Q, Dai W, Feng X, Lu Z, Yang Z, Liu Y, Xie G, Yang Y, Shen K, et al. Lung Microbiota and Pulmonary Inflammatory cytokines expression Vary in Children with Tracheomalacia and Adenoviral or Mycoplasma pneumoniae Pneumonia. FRONT PEDIATR. 2019;7:265.
Wang Z, Chu C, Ding Y, Li Y, Lu C. Clinical significance of serum microRNA-146a and inflammatory factors in children with Mycoplasma pneumoniae pneumonia after azithromycin treatment. J PEDIAT-BRAZIL 2023.
Li W, Liu YJ, Zhao XL, Shang SQ, Wu L, Ye Q, Xu H. Th1/Th2 Cytokine Profile and its diagnostic value in Mycoplasma pneumoniae Pneumonia. Iran J PEDIATR. 2016;26(1):e3807.
Li Q, Li ZY, Zhang J, Guo WN, Xu XM, Sun FX, Xu H. Xiyanping Plus Azithromycin Chemotherapy in Pediatric Patients with Mycoplasma pneumoniae Pneumonia: A Systematic Review and Meta-Analysis of Efficacy and Safety. EVID-BASED COMPL ALT 2019, 2019:2346583.
Peng Y, Chen Z, Li Y, Lu Q, Li H, Han Y, Sun D, Li X. Shuanghuanglian oral preparations combined with azithromycin for treatment of Mycoplasma pneumoniae pneumonia in Asian children: a systematic review and meta-analysis of randomized controlled trials. PLoS ONE. 2021;16(7):e0254405.
Wang J, Ma X, Wei S, Yang T, Tong Y, Jing M, Wen J, Zhao Y. Clinical efficacy and safety of Shashen Maidong Decoction in the treatment of Pediatric Mycoplasma Pneumonia: a systematic review and Meta-analysis. FRONT PHARMACOL. 2021;12:765656.
Zhang GM, Huang ZY, Sun R, Ye SL, Feng Q. Xiao’er Xiaoji Zhike Oral Liquid Combined with Azithromycin for Mycoplasma pneumoniae Pneumonia in Children: A Systematic Review and Meta-Analysis. EVID-BASED COMPL ALT 2020, 2020:9740841.
Chen Z, Shi Q, Peng Y, Chen Y, Cao L, Pang B, Ji Z, Liu C, Zhang J. Traditional Chinese medicine oral liquids combined with azithromycin for Mycoplasma pneumoniae Pneumonia in children: a bayesian network Meta-analysis. FRONT PHARMACOL. 2021;12:652412.
Ashy N, Alharbi L, Alkhamisi R, Alradadi R, Eljaaly K. Efficacy of erythromycin compared to clarithromycin and azithromycin in adults or adolescents with community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials. J INFECT CHEMOTHER. 2022;28(8):1148–52.
Peng Y, Chen Z, Li Y, Lu Q, Li H, Han Y, Sun D, Li X. Combined therapy of Xiaoer Feire Kechuan oral liquid and azithromycin for mycoplasma Pneumoniae pneumonia in children: a systematic review & meta-analysis. Phytomedicine. 2022;96:153899.
Wang H, Zhao M, Liu S, Wang X. Efficacy and safety of reduning injection combined with azithromycin in the treatment of mycoplasma pneumonia among children: a systematic review and meta-analysis. Phytomedicine. 2022;106:154402.
Jones GH, Scott SJ. Continuous infusions of terbutaline in asthma - a review. J ASTHMA. 2011;48(8):753–6.
Wang Y, Zhang Y, Lu W, Wang L. Serum Tumor Necrosis Factor-α and Interferon-γ Levels in Pediatric Mycoplasma pneumoniae Pneumonia: A Systematic Review and Meta-Analysis. CAN RESPIR J 2018, 2018:8354892.
Zhang Z, Dou H, Tu P, Shi D, Wei R, Wan R, Jia C, Ning L, Wang D, Li J, et al. Serum cytokine profiling reveals different immune response patterns during general and severe Mycoplasma pneumoniae pneumonia. FRONT IMMUNOL. 2022;13:1088725.
Acknowledgements
We would like to appreciate all editors/reviewers for their helpful comments and valuable suggestions.
Funding
The study was funded by “1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYGD23002)”.
Author information
Authors and Affiliations
Contributions
This study was designed and developed by YCS. DYK contributed to the conception and design of the study. YCS and YL collected the data and performed the first-level analysis; CYZ and XTL conducted the second-level, in-depth analysis and interpretation. YCS and YL wrote the first draft. All the authors reviewed and approved the final version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sheng, Y., Liang, Y., Zhao, C. et al. Azithromycin sequential therapy plus inhaled terbutaline for Mycoplasma Pneumoniae pneumonia in children: a systematic review and meta-analysis. BMC Infect Dis 24, 653 (2024). https://doi.org/10.1186/s12879-024-09564-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09564-x