
Abstract
Background
Data on persistent candidemia (PC), a recognized complication of candidemia, are lacking in China. This study aimed to investigate the clinical characteristics and risk factors for the mortality of PC among adults in China.
Methods
This 6-year retrospective study analyzed the prevalence, species distribution, antifungal susceptibility, risk factors, and patient mortality of PC among adults in three regional tertiary teaching hospitals in China from 2016 to 2021. We collected electronic laboratory records data of PC and non-PC patients and used the Student test or Mann–Whitney U test for a retrospective study. Logistic regression was used to identify risk factors associated with persistent candidemia.
Results
The definition of PC was fulfilled by 36 patients (13.7%, 36/263). The mean age of the patients was 59.9 years (60 years for patients with PC; 59.8 years for those with non-PC; P > 0.05) and 131 (60.1%) were men [16 with PC (44.4%), 115 with non-PC (63.2%), P < 0.05]. The mean annual incidence was 0.15/1000 admissions (including PC 0.03/1000 admissions vs. non-PC 0.12/1000 admissions, P < 0.05). Candida parapsilosis (14/36, 38.9%) and Candida albicans (81/182, 44.5%) were the predominant pathogens in patients with PC and non-PC, respectively. Most isolates were susceptible to flucytosine (99.0%) and amphotericin B (99.5%), and the activity of antifungal agents against Candida species was not statistically significantly different between patients with PC and non-PC (P > 0.05). The 30-day mortality rate was 20.2% (16.7% with PC vs. 20.9% with non-PC, P > 0.05). Multivariable regression analysis showed that use of broad-spectrum antibiotics (odds ratio (OR), 5.925; 95% confidence interval (CI), 1.886–18.616, P = 0.002), fluconazole (OR, 3.389; 95% CI, 1.302–8.820, P = 0.012) and C. parapsilosis infection (OR, 6.143; 95% CI, 2.093–18.031, P = 0.001) were independent predictors of PC, sex (male) (OR, 0.199; 95% CI, 0.077–0.518, P = 0.001) was the protective factor for PC. Respiratory dysfunction (OR, 5.763; 95% CI, 1.592–20.864, P = 0.008) and length of hospital stay(OR, 0.925; 95% CI, 0.880–0.973, P = 0.002) were independent predictors of 30-day mortality in patients with non-PC. C. tropicalis bloodstream infection (OR, 12.642; 95% CI, 1.059–150.951; P = 0.045) was an independent predictor of 30-day mortality in patients with PC.
Conclusions
The epidemiological data of patients with PC and non-PC were different in the distribution of Candida species, the mean annual incidence and independent predictors of 30-day mortality. Flucytosine and amphotericin B could be used as first-choice drugs in the presence of PC infections.
Similar content being viewed by others


Background
Candidemia is the most common fungal disease among hospitalized patients worldwide and is defined as a condition in which at least one blood culture appears positive for the Candida species [1]. The morbidity and mortality of Candidemia in adults were higher than those in children in the last decades, however, the epidemiology of candidemia has now changed, and the incidence of candidemia in infants and children was gradually increased. It has been reported that the incidence of candidemia was more than 90% in the neonatal intensive care unit [2]. Meanwhile, the outbreak of Candida auris infections [3] and persistent candidemia (PC) have also brought serious challenges to the treatment of candidemia. PC is defined as the isolation of the same Candida species from positive blood culture for ≥ 5 days after the initiation of antifungal therapy [4]. It is an increasingly recognized complication of candidemia [5]. Previous studies reported that 8–15% of patients with candidemia developed PC [6]; meanwhile, PC was associated with significant mortality, which was as high as 20–50% [4, 7]. Some studies reported that PC was associated with the biofilm production of Candida species [8, 9] and antifungal resistance [10]. The other main risk factors for PC included underlying disease status (e.g., hematological malignancies), low serum levels of drugs, endovascular infection, deep-tissue abscesses, metastatic infection foci, ineffective empirical treatment, infections associated with prosthetic materials, central venous catheterization (CVC)-related infection, total parenteral nutrition, hemodialysis and abdominal surgery [11, 12].
PC often leads to poor clinical outcomes. However, only a few studies have reported on PC in adults and neonates worldwide. National or multicenter studies in patients with PC infection are almost absent in most countries and regions in the world, bringing in difficulties for preventing and treating PC. Only a few studies have reported on PC infection in infants in China. The multicenter study data of PC in adult patients are lacking in China. Therefore, we performed a 6-year retrospective study to evaluate the epidemiology, antifungal susceptibility, risk factors and mortality of PC among all adult patients in three tertiary teaching hospitals in three different cities of China.
Methods
Study design
We conducted a retrospective observational study of electronic laboratory records of persistent candidemia patients from the Affiliated Hospital of Southwest Medical University (AHSWMU; Luzhou, China), Zigong Fourth People’s Hospital (ZGFPH; Zigong, China) and the Second People’s Hospital of Neijiang (SPHNJ; Neijiang, China) from January 2016 to December 2021. The AHSWMU is a 3200-bed tertiary care teaching hospital with 43 wards and approximately 130,000 annual admissions, the ZGFPH is a 1600-bed tertiary care teaching hospital with 32 wards and approximately 70,000 annual admissions, the SPHNJ is a 1500-bed tertiary care teaching hospital with 38 wards and approximately 45,000 annual admissions.
Data collection
The fungal specimen data were collected from patients with candidemia admitted to the AHSWMU, ZGFPH and SPHNJ from January 2016 to December 2021. All data were collected from electronic medical records. The following data were retrospectively collected from all adult patients: demographic characteristics, underlying comorbidities, Candida species, susceptibility to antifungal agents, use of broad-spectrum antibiotics, antifungal agents and mortality. Data on the following risk factors associated with candidemia were also collected: indwelling central vascular catheter, mechanical ventilation, systemic corticosteroid treatment (a dose equivalent to prednisone 10 mg/day for at least 14 days), total parenteral nutrition, malnutrition, chemotherapy, hemodialysis, abdominal surgery, intensive care unit (ICU) admission, neutropenia (absolute neutrophil count < 500 cells/µL), concomitant bacterial infections, septic shock, hemorrhagic shock, broad-spectrum antibiotic use, prophylaxis antifungal therapy and treatment with antifungal agents. The study protocol was approved by the Clinical Research Ethics Committee of the Affiliated Hospital of Southwest Medical University (Project No. KY2020043). The need for informed consent was waived by the Clinical Research Ethics Committee of the Affiliated Hospital of Southwest Medical University. All experiments were performed in accordance with the study protocol in three hospitals.
Inclusion/exclusion criteria
The diagnostic criteria of candidemia were based on the guidelines for diagnosing and treating candidiasis: the expert consensus issued by the Chinese Adult Candidiasis Diagnosis and Management Expert Consensus Group [13]. These criteria were also in accordance with the European Society of Clinical Microbiology and Infectious Diseases ESCMID* guidelines for the diagnosis and management of Candida diseases 2012 [14, 15] and the Infectious Diseases Society of America Clinical Practice Guidelines for the Management of Candidiasis: 2016 Update [16]. All patients aged ≥ 18 years who presented to the three tertiary hospitals with candidemia from 2016 to 2021 were investigated; only the first episode was included in our analysis. Patient cultures with two or more Candida species were excluded from the analysis. PC was defined as the isolation of the same Candida species from positive blood culture for ≥ 5 days after the initiation of an antifungal therapy, and non-PC was defined as all other candidemia cases other than the persistent ones, with at least one negative blood culture between two positive blood culture results.
Microorganism identification and antifungal susceptibility
According to the manufacturer’s instructions, blood(10ml) was inoculated into both aerobic and anaerobic BacT/AlerT 3D vials (bioMérieux, France). All positive cultures were manually sampled and inoculated into CHROMagar Candida medium (CHROMagar Company, France) to ensure viability and purity. The identification of all species was confirmed by a Vitek-2 system (bioMérieux, Marcy L’Etoile, France) at SPHNJ and Microflex LT (Bruker Diagnostics Inc., USA) matrix-assisted laser-desorption/ionization time-of-flight mass spectrometry system at AHSWMU and ZGFPH.
Antifungal susceptibility tests for fluconazole (FCA), itraconazole (ITR), voriconazole (VRC), flucytosine (5-FC) and amphotericin B (AMB) were performed for all Candida strain isolates using an ATB FUNGUS 3 kit (bioMérieux, France) in all the three hospitals. The minimal inhibitory concentrations of the antifungal agents were judged by visualization in our laboratory according to the manufacturer’s instructions. The quality control strains were Candida parapsilosis ATCC 22,019 and C. krusei ATCC 6258. The results were interpreted using the Clinical and Laboratory Standards Institute M27-A3 microbroth dilution method [17].
Statistical analyses
The data were analyzed using Microsoft Excel (version 2019, WA, USA) and IBM SPSS software version 26 for Windows (IBM, NY, USA). The categorical data were compared using chi-square or Fisher’s exact tests. The continuous data were analyzed using the Student t test or Mann–Whitney U test. Multivariable logistic regression analysis was performed to identify independent predictors of PC and 30-day hospital mortality. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Biologically plausible variables with a P value < 0.1 according to the univariate analyses were included in the multiple logistic regression model. Statistical significance was determined using two-tailed tests, and P < 0.05 was considered statistically significant [4].

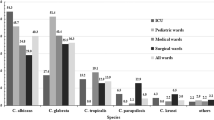
Distribution of the fungal species in adult patients with PC and Non-PC according to different wards
FootNote: *Others include C. guilliermondii (2), C. famata (2), C. dubliniensis (1), C. haemulonii (1) and C. inconspicua (1)
Results
A total of 263 distinct candidemia episodes were identified during our study period. The definition of PC was fulfilled by 36 patients (13.7%, 36/263), and 182 patients (69.2%, 182/263) had non-PC. The mean age of the patients was 59.9 years (60 years for PC, 59.8 years for non-PC, P > 0.05), and 131 (60.1%) were men [16 with PC (44.4%), 115 with non-PC (63.2%), P < 0.05]. Most PC episodes were diagnosed in surgical wards (13, 36.1%), and most non-PC episodes in medical wards (78, 42.9%). The detailed data from the three hospitals are shown in Supplementary Table S1. Most of the patients with PC and non-PC had one or more comorbidities. Pulmonary infection (69.4%), cardiovascular disease (58.3%), neurological diseases (47.2%) and gastrointestinal diseases (47.2%) were the most common underlying comorbidities in patients with PC, whereas pulmonary infection (62.1%), chronic/acute renal failure (57.7%) and cardiovascular disease (53.3%) were the most common underlying comorbidities in those with non-PC. Moreover, the most common underlying conditions documented before PC and non-PC were prior exposure to broad-spectrum antibiotics (80.6% and 60.4%, respectively), CVC (63.9% and 45.1%, respectively), malnutrition (58.3% and 47.8%, respectively), mechanical ventilation (52.8% and 44.5%, respectively), concomitant bacterial infections (47.2% and 33.5%, respectively), ICU admission (44.4% and 36.8%, respectively) and total parenteral nutrition (36.1% and 27.5%, respectively). In total, 13 (36.1%, 13/36) patients with PC had received prophylactic antifungal therapy with FCA, and patients with non-PC accounted for 26.4% (48/182) of the total. Except for chronic/acute renal failure, no statistically significant differences were found in the underlying comorbidities between patients with PC and non-PC. Moreover, no statistically significant differences in the number of underlying conditions were found between patients with persistent and non-PC (except for CVC). After the positive result of blood culture, VRC became the most important antifungal drug. The demographic and clinical characteristics of the patients are summarized in Table 1.
The mean annual incidence of candidemia was 0.15/1000 admissions, including 0.03/1000 admissions for PC (0.04/1000 at AHSWMU, 0.01/1000 at ZGFPH and 0.02/1000 at SPHNJ) and 0.12/1000 admissions for non-PC (0.14/1000 at AHSWMU, 0.12/1000 at ZGFPH and 0.08/1000 at SPHNJ). According to the Candida species, the incidence of the three most commonly isolated Candida species in patients with PC were as follows: C. parapsilosis, 0.010/1000 admissions; C. tropicalis, 0.005/1000 admissions; and C. glabrata, 0.004/1000 admissions, and that in patients with non-PC was as follows: C. albicans, 0.056/1000 admissions; C. glabrata, 0.026/1000 admissions and C. tropicalis, 0.024/1000 admissions. The detailed data in the three hospitals are shown in Supplementary Table S1.

Factors associated with the formation of PC by multivariate analysis
FootNote: Length of hospital stay(days)( 95% CI: 0.996–1.009)
The most common species among all Candida species isolates were C. albicans (39.4%), followed by C. glabrata (20.2%), C. tropicalis (19.3%), C. parapsilosis (15.6%), C. krusei (2.3%) and others (3.2%). The distribution of Candida species in patients with PC and non-PC is shown in Table 1. C. parapsilosis was the predominant species in patients with PC (38.9%), whereas C. albicans was the main species in patients with non-PC (44.5%). The distribution of Candida species in patients with PC and non-PC in surgical, medical and ICU wards is shown in Fig. 1. The detailed data from the three hospitals are shown in Supplementary Table S2.
The results of in vitro susceptibility testing of Candida strain isolates are summarized in Table 2. All isolates were highly susceptible to AMB (99.5%) and 5-FC (99.0%), and the resistance rate of ITR, VRC and FCA was 18.6%, 15.2%, and 14.1%, respectively. C. tropicalis had the highest antifungal agent resistance rate among the Candida species, which was resistant to FCA (36.6%), ITR (36.6%) and VRC (39.0%). The activity of antifungal agents against the Candida species was not significantly different between patients with PC and non-PC (P > 0.05). The detailed data are shown in Table 2.
The all-cause mortality rate in the 218 patients was 26.1% (57/218). The 7-day and 30-day mortality rates were 10.1% (22/218) and 20.2% (44/218), respectively. The 7-day mortality rate for patients with PC and non-PC was 2.8% (1/36) and 11.5% (21/182) and the 30-day mortality rate was 16.7% (6/36) and 20.9% (38/182), respectively. The 30-day mortality rate for medical wards, surgical wards, and ICU wards in patients with PC and non-PC was 9.1% (1/11), 15.4% (2/13) and 16.7% (2/12), and 26.9% (21/78), 10.0% (5/50) and 22.2% (12/54), respectively.
The univariate predictors of poor outcomes due to PC are shown in Table 1. The results of the multivariate analysis showed that use of broad-spectrum antibiotics (OR, 5.925; 95% CI, 1.886–18.616, P = 0.002) and FCA (OR, 3.389; 95% CI, 1.302–8.820, P = 0.012), and C. parapsilosis infection (OR, 6.143; 95% CI, 2.093–18.031, P = 0.001) were independent risk factors for PC, sex (male) (OR, 0.199; 95% CI, 0.077–0.518, P = 0.001) was the protective factor for PC (Fig. 2 and Supplementary Table S3). The variable associated with 30-day mortality for adult patients with PC was C. tropicalis, and the variables for those with non-PC were age, length of hospital stay, respiratory dysfunction, cardiovascular disease, chronic/acute renal failure, other invasive catheters, mechanical ventilation, total parenteral nutrition, concomitant bacterial infections, septic shock, use of broad-spectrum antibiotics and FCA, and surgical wards (Table 3). The results of the multivariate analysis associated with the 30-day mortality in patients with PC and non-PC are listed in Fig. 3 and Supplementary Table S4. C. tropicalis bloodstream infection was the only independent predictor of 30-day mortality in patients with PC (OR, 12.642; 95% CI, 1.059–150.951; P = 0.045). The length of hospital stay(OR, 0.925; 95% CI, 0.880–0.973, P = 0.002) and respiratory dysfunction (OR, 5.763; 95% CI, 1.592–20.864, P = 0.008) were independent predictors of 30-day mortality in patients with non-PC (Fig. 3 and Supplementary Table S4). Other invasive catheters were only the protective factor for 30-day mortality in patients with non-PC (OR, 0.104; 95% CI, 0.019–0.568, P = 0.009).

Factors associated with 30-day mortality by multivariate analysis
FootNote: Non-Persistent candidemia: Age (95%CI: 0.975–1.038), Length of hospital stay(days)(95% CI: 0.880–0.973). All patients: Age (95%CI: 0.986–1.041), Length of hospital stay(days)(95% CI: 0.905–0.973)
Discussion
This was a 6-year multicenter retrospective study of PC and non-PC in three tertiary teaching hospitals in Southwest China. We analyzed the clinical characteristics, including the demographics, underlying comorbidities, risk factors, distribution of Candida species, antifungal therapy, antifungal agent susceptibility results, department of admission and patient outcomes, as well as epidemiologically compared patients with PC and non-PC.
Our data showed no significant difference in age, department of admission, and 30-day mortality between patients with PC and non-PC (P > 0.05). Our data were consistent with the findings of other studies conducted in adult patients with PC and non-PC [11, 18]. The incidence rate in adult patients with PC (0.03/1000 admissions) was significantly lower than in infant patients(5.5/1000 admissions) [19], This may be related to the clinical characteristics of the patients, and the infant’s immune system is even worse [20]. Meanwhile, the proportion of underlying comorbidities in PC and non-PC, except for chronic/acute renal failure, was not significantly different (P > 0.05). The proportion of chronic/acute renal failure was lower in patients with PC than in those with non-PC (P < 0.05) (Fig. 2 and Supplementary Table S3). Among the risk factors, only CVC had higher risks in patients with PC than those with non-PC (P < 0.05), and the proportion of other risk factors was similar for both patients (P > 0.05) (Fig. 2 and Supplementary Table S3), consistent with previous studies [11, 18]. In therapy, the proportion of use of broad-spectrum antibiotics, FCA and capofungin + VRC were higher in patients with PC than in patients with non-PC (P < 0.05). After Candida was identified in blood, VRC and FCA were used as first-line drugs against the Candida infection, which may be related to the high sensitivity of Candida species to azole antifungal drugs (Table 2). Meanwhile, 21.1% (46/218) patients were treated with the combination drug for Candida spp., possibly because of the drug resistance of Candida or the severity of the patient’s condition. Although echinococcus is the first-line therapy of candidemia, caspofungin was the most used echinocandin drug in many countries [21, 22], however, caspofungin was also a higher risk of inducing FKS mutations in comparison to other echinocandins [21, 23], leading to gradual increase in the resistance rate of caspofungin. There are no susceptibility tests for echinococcus in our region, which may be the reason why clinicians were less likely to choose echinococcus as an first-line agent.
Our data showed that the number of female patients with PC was higher than that with non-PC, which was different from the results of other studies. However, the proportion of men was similar to that in other studies [4, 11, 18], however, the proportion of female were similar to the result of infants study in China [19]. Moreover, the present study showed that the length of hospital stay was longer for patients with PC than for those with non-PC (P = 0.016), which was consistent with the reports of other studies [4]. The patients with PC were hospitalized mostly in surgical wards, and those with non-PC mostly in medical wards, which was similar to other studies that reported hospitalization in Spain [18], and different from those in Finland [4]. This phenomenon may be related to the demographic characteristics of the inpatients in different hospitals or regions. According to our study, C. albicans was the most common cause of candidemia in the whole region, but the proportion of non–C. albicans infections was higher than that of C. albicans infections in patients with PC. Moreover, the proportion of C. parapsilosis in surgical, medical and ICU wards was the highest for patients with PC, which was different from other studies in other countries [4, 11, 18]. This may be due to the demographic characteristics of the patients in different hospitals or regions, or few statistical samples (36 cases of PC).
Our data showed that the mean incidence of PC was 0.03 episodes/1000 admissions from 2016 to 2021. However, the incidence rate was different in different hospitals [4, 11, 18, 24], which was mainly related to the diagnosis and treatment characteristics of hospitals and the basic conditions of patients. Further, 36 patients (13.7%) fulfilled the definition of PC, which was higher than that reported by Kang et al. [11], and less than that reported by Ala-Houhala et al. [4]. The 30-day mortality in this study was similar to that in some hospitals in other countries [4], but lower than that in some other hospitals in other countries [11]. The reason may be that the most persistent Candida infections are caused by C. parapsilosis in this region, and they are sensitive to all antifungal agents (Table 2), which may also be one of the reasons for the low mortality rate of persistent Candida infection in this area. The 30-day mortality in ICU wards was the highest among patients with PC and non-PC, which may be related to the severity of underlying diseases in ICU patients, and was consistent with other studies.
Resistance to FCA, ITR and VRC was common in C. albicans and non-C. albicans species (Table 2). In our study, AMB and 5-FC were highly active against all Candida species. In patients with PC, the resistance rate of ITR was the highest, and the resistance rates of ITR and FCA were higher than those in patients with non-PC. However, the resistance rate of Candida species was not significantly different between patients with PC and non-PC (P > 0.05), the resistance rate of Candida species was not associated with the development of persistent candidemia, which is inconsistent with the result of another study [10]. Moreover, FCA was highly active against all Candida species in patients with PC and non-PC and could be used in patients with candidemia as a first-line agent. In the whole region, the resistance rate to azole was similar to those reported in other regions and countries [25,26,27], but C. tropicalis and C. albicans showed high resistance to azole antifungal drugs in patients with PC in this region. The mechanism of drug resistance will be researched in later studies. This may be related to the long-term use of azole antifungal drugs in patients with persistent Candida infection. Therefore, the antifungal susceptibility of the strains isolated from patients with persistent Candida infection needs to be analyzed so as to guide clinicians to choose antifungal drugs reasonably and avoid the continuous increase of drug resistance.
In this study, we analyzed the risk factors in adult patients with PC and non-PC using multifactorial regression, and the results revealed that use of broad-spectrum antibiotics(OR: 5.925) and FCA(OR: 3.389), and C. parapsilosis infection(OR: 6.143) were independent risk factors for patients with PC, and sex (male) (OR: 0.199) was the protective factor for PC, which was different from the results of other studies, the other studies have showed that CVC(OR:2.71), metastatic infection foci(OR:3.60), ineffective empirical treatment (OR: 3.31) and unsuspected sites of infection (OR: 4.28) were independent risk factors for patients with PC [4, 11, 18]. The age, length of hospital stay, respiratory dysfunction, cardiovascular disease, chronic/acute renal failure, other invasive catheters, mechanical ventilation, total parenteral nutrition, concomitant bacterial infections, septic shock, use of broad-spectrum antibiotics such as FCA and Capofungin + AMB, and surgical wards were the common predictors of mortality in the univariate analysis (P < 0.05) in patients with non-PC, and the univariate predictors of poor outcomes in patients with PC were less than those in patients with non-PC (1 vs. 13 predictors), as shown in Table 3. C. tropicalis bloodstream infection was only the common predictor of mortality in the univariate analysis (P < 0.05) in patients with PC; meanwhile, it was also the only independent risk factor for 30-day mortality (OR:12.642). The reason may be because C. tropicalis has a high resistance to the antifungal drugs of azole, leading to the failure of treatment in patients with C. tropicalis infection, finally, the death of patients, which was consistent with the findings of another study in South Korea (OR: 4.12) [11]. Respiratory dysfunction (OR: 5.763) was independent predictors of 30-day mortality in this study, however, some other studies have reported that corticosteroid within past 30 days (OR:5.31) and Septic shock (OR: 5.81) were independent predictors of 30-day mortality. The length of hospital stays (OR: 0.925) and other invasive catheters (OR: 0.104) were the protective factors for 30-day mortality in patients with non-PC. Previous studies have reported respiratory dysfunction(OR: 22.57) as an independent predictor [28]. However, the length of hospital stay (OR: 0.89) and other invasive catheters (OR: 0.04) reported here have rarely been reported in other studies, possibly because the demographic characteristics, underlying diseases and risk factors of the patients in our study were different from those in other studies. This may be why the independent predictors and protective factors in this study differed from those in other studies (see Table 4).
This study has two potential limitations. First, all Candida strain isolates were tested for antifungal susceptibility using ATB FUNGUS 3 kit (bioMérieux, France) in all three hospitals, the kit did not contain echinococcins, we only had data on the use of echinococcins, but no data on drug sensitivity. Second, although we conducted a multicenter retrospective study, our total sample size was still smaller. Our data may be affected by the insufficient sample size. Therefore, the results may not be generalizable to patients with persistent candidemia in other regions of China.
Conclusions
C. albicans was the main Candida species, but C. parapsilosis has become the most common species in PC in the study region. FCA was the main antifungal drug for patients with PC and a prophylaxis antifungal therapy. AMB and 5-FC were highly active against all Candida species. The morbidity and mortality rates in patients with PC and non-PC in this region were lower than those in other regions. The length of hospital stay and respiratory dysfunction were independent predictors of 30-day mortality in adult patients with non-PC. C. tropicalis infection was the independent risk factor for the 30-day mortality in adult patients with PC. This study provides reference data of epidemiological and antifungal drug susceptibility for the prevention and treatment of adult patients with PC in other hospitals in China.
Data Availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- PC:
-
persistent candidemia
- BSI:
-
bloodstream infection
- ICU:
-
intensive care unit
- USA:
-
United States of America
- ATCC:
-
American type culture collection
- MALDI-TOF MS:
-
Matrix-assisted laser desorption/ionization-time of flight mass spectroscopy
- FCA:
-
fluconazole
- ITR:
-
itraconazole
- AMB:
-
amphotericin B
- VRC:
-
voriconazole
- 5-FC:
-
flucytosine
- CVC:
-
central venous catheter
- MIC:
-
minimal inhibitory concentration
- OR:
-
odds ratio
- CI:
-
confidence interval
- SD:
-
standard deviation.
References
Kullberg BJ, Arendrup MC. Invasive candidiasis. N Engl J Med. 2015;373(15):1445–56.
Ahangarkani F, Shokohi T, Rezai MS, Ilkit M, Mahmoodi Nesheli H, Karami H, Tamaddoni A, Alizadeh-Navaei R, Khodavaisy S, Meis JF, et al. Epidemiological features of nosocomial candidaemia in neonates, infants and children: a multicentre study in Iran. Mycoses. 2020;63(4):382–94.
Ruiz-Gaitan A, Moret AM, Tasias-Pitarch M, Aleixandre-Lopez AI, Martinez-Morel H, Calabuig E, Salavert-Lleti M, Ramirez P, Lopez-Hontangas JL, Hagen F, et al. An outbreak due to Candida auris with prolonged colonisation and candidaemia in a tertiary care european hospital. Mycoses. 2018;61(7):498–505.
Ala-Houhala M, Anttila VJ. Persistent vs non-persistent candidaemia in adult patients in 2007–2016: a retrospective cohort study. Mycoses. 2020;63(6):617–24.
Johnson MD, Plantinga TS, van de Vosse E, Velez Edwards DR, Smith PB, Alexander BD, Yang JC, Kremer D, Laird GM, Oosting M, et al. Cytokine gene polymorphisms and the outcome of invasive candidiasis: a prospective cohort study. Clin Infect Dis. 2012;54(4):502–10.
Nucci M. Persistent candidemia: causes and investigations. Curr Fungal Infect Rep. 2011;5(1):3–11.
Hammoud MS, Al-Taiar A, Fouad M, Raina A, Khan Z. Persistent candidemia in neonatal care units: risk factors and clinical significance. Int J Infect Dis. 2013;17(8):e624–628.
Monfredini PM, Souza ACR, Cavalheiro RP, Siqueira RA, Colombo AL. Clinical impact of Candida spp. biofilm production in a cohort of patients with candidemia. Med Mycol. 2018;56(7):803–8.
Li WS, Chen YC, Kuo SF, Chen FJ, Lee CH. The impact of Biofilm formation on the persistence of Candidemia. Front Microbiol. 2018;9:1196.
Rosenberg A, Ene IV, Bibi M, Zakin S, Segal ES, Ziv N, Dahan AM, Colombo AL, Bennett RJ, Berman J. Antifungal tolerance is a subpopulation effect distinct from resistance and is associated with persistent candidemia. Nat Commun. 2018;9(1):2470.
Kang SJ, Kim SE, Kim UJ, Jang HC, Park KH, Shin JH, Jung SI. Clinical characteristics and risk factors for mortality in adult patients with persistent candidemia. J Infect. 2017;75(3):246–53.
Chen CY, Huang SY, Tsay W, Yao M, Tang JL, Ko BS, Chou WC, Tien HF, Hsueh PR. Clinical characteristics of candidaemia in adults with haematological malignancy, and antimicrobial susceptibilities of the isolates at a medical centre in Taiwan, 2001–2010. Int J Antimicrob Agents. 2012;40(6):533–8.
Chinese Adult Candidiasis D, Management Expert Consensus G. [Chinese consensus on the diagnosis and management of adult candidiasis]. Zhonghua nei ke za zhi. 2020;59(1):5–17.
Ullmann A, Cornely O, Donnelly J, Akova M, Arendrup M, Arikan-Akdagli S, Bassetti M, Bille J, Calandra T, Castagnola E et al. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: developing European guidelines in clinical microbiology and infectious diseases.Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases2012:1–8.
M C-E PEV, S A-A MCA, JP JB, C L-F, MD DHEJ. R, M A : ESCMID* guideline for the diagnosis and management of Candida diseases 2012: diagnostic procedures.Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases2012:9–18.
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, Reboli AC, Schuster MG, Vazquez JA, Walsh TJ, et al. Clinical practice Guideline for the management of Candidiasis: 2016 update by the infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1–50.
ZR Z, K GTYHD, JB Y. Surveillance study of the prevalence, species distribution, antifungal susceptibility, risk factors and mortality of invasive candidiasis in a tertiary teaching hospital in Southwest China. BMC Infect Dis. 2019;19(1):939.
Agnelli C, Valerio M, Bouza E, Vena A, Guinea J, Del Carmen Martinez-Jimenez M, Marcos-Zambrano LJ, Escribano P, Munoz P, Group CS. Persistent candidemia in adults: underlying causes and clinical significance in the antifungal stewardship era. Eur J Clin Microbiol Infect Dis. 2019;38(3):607–14.
Fu J, Ding Y, Jiang Y, Mo S, Xu S, Qin P. Persistent candidemia in very low birth weight neonates: risk factors and clinical significance. BMC Infect Dis. 2018;18(1):558.
Pana ZD, Roilides E, Warris A, Groll AH, Zaoutis T. Epidemiology of Invasive Fungal Disease in Children. J Pediatr Infect Dis Soc. 2017;6(suppl1):3–S11.
Coste AT, Kritikos A, Li J, Khanna N, Goldenberger D, Garzoni C, Zehnder C, Boggian K, Neofytos D, Riat A, et al. Emerging echinocandin-resistant Candida albicans and glabrata in Switzerland. Infection. 2020;48(5):761–6.
Lin KY, Chen PY, Chuang YC, Wang JT, Sun HY, Sheng WH, Chen YC, Chang SC. Effectiveness of echinocandins versus fluconazole for treatment of persistent candidemia: a time-dependent analysis. J Infect. 2018;77(3):242–8.
Shields RK, Kline EG, Healey KR, Kordalewska M, Perlin DS, Nguyen MH, Clancy CJ. Spontaneous mutational frequency and FKS Mutation Rates Vary by Echinocandin Agent against Candida glabrata. Antimicrob Agents Chemother. 2019;63(1):e01692–01618.
Robinson JA, Pham HD, Bloom BT, Wittler RR. Risk factors for persistent candidemia infection in a neonatal intensive care unit and its effect on mortality and length of hospitalization. J Perinatol. 2012;32(8):621–5.
Xiao Z, Wang Q, Zhu F, An Y. Epidemiology, species distribution, antifungal susceptibility and mortality risk factors of candidemia among critically ill patients: a retrospective study from 2011 to 2017 in a teaching hospital in China. Antimicrob Resist Infect Control. 2019;8:89.
Sriphannam C, Nuanmuang N, Saengsawang K, Amornthipayawong D, Kummasook A. Anti-fungal susceptibility and virulence factors of Candida spp. isolated from blood cultures. J Mycol Med. 2019;29(4):325–30.
Israel S, Amit S, Israel A, Livneh A, Nir-Paz R, Korem M. The epidemiology and susceptibility of Candidemia in Jerusalem, Israel. Front Cell Infect Microbiol. 2019;9:352.
Zeng Z, Ding Y, Tian G, Yang K, Deng J, Li G, Liu J. A seven-year surveillance study of the epidemiology, antifungal susceptibility, risk factors and mortality of candidaemia among paediatric and adult inpatients in a tertiary teaching hospital in China. Antimicrob Resist Infect Control. 2020;9(1):133.
Acknowledgements
We thank Yanhan Li in the medical records room for guiding us in reviewing the electronic medical records. We have asked for EditorBar (www.editorbar.com) for its linguistic assistance during the preparation of this revised manuscript.
Funding
This work was supported by Supported by Sichuan Science and Technology Program (No. 2022YFQ0093, No. 2021YFS0329) and Southwest Medical University Industry-University Training Program (No. 22001). The funder had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
ZRZ and JBL designed the study and drafted the manuscript. YPL, CHG and YLY collected the data. ZRZ , YPL, YHD, MT and CHY analyzed the data; ZRZ and YPL wrote the paper. YPL, CHG and YLY are contributed equally to this work and share first authorship. All authors have read approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Clinical Research Ethics Committee of the Affiliated Hospital of Southwest Medical University (project no. KY2020043). This is a retrospective study. The need for informed consent was waived by the Clinical Research Ethics Committee of the Affiliated Hospital of Southwest Medical University. All experiments were performed with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Y., Gu, C., Yang, Y. et al. Epidemiology, antifungal susceptibility, risk factors, and mortality of persistent candidemia in adult patients in China: a 6-year multicenter retrospective study. BMC Infect Dis 23, 369 (2023). https://doi.org/10.1186/s12879-023-08241-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08241-9