
Abstract
Background
Research on the relationship between disclosure of HIV status to male sexual partners (HIV disclosure) and quality of life (QOL) revealed complex and even contradictory results. The impact of HIV disclosure on various domains of QOL and the mediation effect between them are unclear. The purposes of this study were to explore the impact of HIV disclosure on QOL among men who have sex with men (MSM), and whether HIV treatment self-efficacy mediated these relationships.
Methods
The data came from a baseline survey on the design of a randomized control trial conducted in Shandong, China. A total of 579 MSM patients were included. SPSS 24.0 was used to conduct independent samples t test, one-way analysis of variance and nonparametric tests and the PROCESS macro was used to conduct mediation analysis.
Results
Among 579 participants, 16.06% disclosed their HIV infection status to their male sexual partners. The effect of HIV disclosure on QOL was mediated by treatment self-efficacy. Self-efficacy played partial mediating role in social relationships, meaning that HIV disclosure had both direct and indirect effects on this factor. In the overall QOL and domains of physical, psychological, independence, and environment, HIV disclosure had an indirect effect only through self-efficacy and no significant effect on the spirituality domain.
Conclusions
The results emphasize the importance of HIV disclosure and self-efficacy on the QOL of MSM patients and suggest that health care providers should assist MSM patients in deciding whether to disclose their HIV status during daily medical services.
Similar content being viewed by others


Background
Acquired immune deficiency syndrome (AIDS) is an infectious disease caused by Human immunodeficiency virus (HIV), which poses great challenges to global public health [1]. Antiretroviral therapy (ART) has shown great efficacy in viral suppression, immune function recovery and HIV/AIDS-related mortality reduction, transforming AIDS from a fatal disease into a manageable chronic disease [2]. With the extension of life expectancy for people living with HIV (PLWH), quality of life (QOL) has become an important topic for PLWH. The Joint United Nations Programme on HIV/AIDS (UNAIDS) considered the QOL to be the ‘fourth 90’ target of HIV/AIDS testing and prevention; that is, 90% of PLWH with viral load suppression remain in a healthy state [3]. In China, the risk of HIV infection among men who have sex with men (MSM) is growing rapidly, and MSM with HIV/AIDS still have many problems in the physical, psychological and social domains [4,5,6]. Improving the QOL of MSM patients has become one of the primary goals of patients and their medical service providers.
Among MSM patients, disclosure of HIV status to male sexual partners (“HIV disclosure” hereafter) was the first step to establishing a supportive relationship with sexual partners. HIV disclosure also played an important role in HIV prevention, which could minimize stigmatization and discrimination against PLWH [7, 8]. Current studies have indicated that HIV disclosure can reduce the occurrence of high-risk sexual behaviours, such as unprotected anal intercourse (UAI) behaviours and multiple sexual partners, thus decreasing the risk of HIV transmission [9, 10]. A previous review demonstrated that HIV disclosure of MSM could not only reduce the transmission of HIV from patients to negative partners but also decrease the risk of repeated infection due to reinfection with other viruses in MSM patients [11]. Mathematical models showed that disclosure of HIV status to sexual partners can reduce the risk of HIV transmission by approximately 40% [12, 13]. In addition, HIV disclosure was linked to less mortality among HIV-infected individuals on ART and could help MSM patients improve their ART adherence [14]. Good adherence of those who disclosed HIV infection status was found to be 1.6 times that of those who did not [15, 16]. In addition to preventing HIV transmission and promoting treatment adherence, HIV disclosure was also related to many positive results, such as increasing social support, reducing psychological distress, and improving happiness [17,18,19]. However, MSM faced many challenges in disclosing their HIV serostatus to their male partners. Although HIV disclosure was important for MSM to obtain social support, potential risks such as loss of financial support, breakdown of partnership, abuse or fear of discrimination prevented them from disclosing [20, 21]. There was a difference between regions and countries in terms of HIV disclosure [22, 23].
The relationship between the disclosure of HIV status and QOL revealed complex and even contradictory results [24,25,26]. For example, some studies found that MSM patients who were hiding their HIV status were related to poor QOL [25, 26], but others showed that disclosure was related to poor physical and mental health [24]. This difference might be related to the various disclosure methods, regions and cultural backgrounds. Although it has been showed that there is a specific correlation between disclosure and QOL, the path of the role of disclosure and the impact on the specific areas of QOL have not been fully explained.
Self-efficacy, as first proposed by Bandura, refers to a person’s confidence in their ability to complete a specific behaviour [27]. According to social cognitive theory (SCT) [27, 28], self-efficacy is a promoting factor to take action and one of the four core determinants of health promotion [27, 28]. People with higher self-efficacy are more likely to engage in health promotion behaviours. Several studies [29, 30] showed that self-efficacy had an important effect on QOL, indicating that improving HIV treatment self-efficacy was essential to promote QOL in patients with HIV/AIDS. PLWH with high self-efficacy might have more optimistic attitudes and more positive coping strategies, resulting in higher QOL scores in various domains [30]. Moreover, some studies found a negative correlation between disclosure and HIV treatment self-efficacy due to a lack of economic, emotional or psychological support and poor coping skills in partners [7, 20]. Some researchers began to explore the impact of self-efficacy as a mediator of the QOL of MSM patients. Although existing studies have demonstrated that self-efficacy was related to HIV disclosure and QOL, few studies on the mediation role of self-efficacy in the relationship between HIV disclosure and QOL in various domains have been conducted [31, 32].
MSM with HIV/AIDS face the double stigma of having sex with males and their HIV infection status. Compared with promoting disclosure to the general population, disclosing HIV serostatus to male sexual partners was considered a promising behaviour index, which could be changed through behavioural intervention. In this way, we could prevent HIV transmission, improve the QOL of MSM patients and promote a good outcome [33, 34]. Therefore, we conducted this study to explore whether HIV disclosure among MSM patients had an impact on QOL and its various domains, and whether HIV treatment self-efficacy played a mediating role.
Methods
Study sites and participants
This study was a secondary analysis of baseline data from a randomized controlled study conducted from October to December 2020 in a hospital in Jinan, Shandong Province, China [35]. The hospital included more than 2000 PLWH, accounting for more than 90% of the PLWH in the city. Among the subjects, MSM patients accounted for approximately 80%. The inclusion criteria for the baseline survey were as follows: (1) 18 years old and above; (2) male sex birth and has had anal sex; (3) HIV-positive; (4) has provided informed consent and volunteered to participate in the study. The exclusion criteria were as follows: (1) inability to complete the survey due to health problems (e.g., mental illness) and (2) inability provide written informed consent.
The original sample size (586) was decided based on the design of a randomized control trial. The sample size for this study was calculated according to the cross-sectional survey formula [36]. The World Health Organization Quality of Life for the HIV-abbreviated version (WHOQOL-HIV BREF) scale is a multidimensional scale, and the mean score of each domain was considered to calculate the sample size. According to previous studies [37], the mean score of MSM with HIV/AIDS in each domain of the QOL was estimated to be 15, the standard deviation was 4, and the relative error was 0.5 [37]. The minimum sample size required was 246, and the existing sample size met the needs of the current research.
Data collection
MSM with HIV/AIDS were recruited by convenience sampling. The trained medical staff in the hospital referred the research subjects who met the inclusion criteria to the staff of this study. The staff explained the purpose and content of the study to MSM patients who met the inclusion criteria, and distributed paper questionnaires in a relatively closed and independent space of the hospital after obtaining informed consent. After the participants finished the questionnaire, the staff examined and verified the questionnaire on site. Each participant received a compensation of 50 RMB (approximately 7.47 USD). The research protocol was approved by the Ethical Review Committee of the School of Public Health at Shandong University (ethical code: 20190210).
Measures
Socio-demographic characteristics
We collected the socio-demographic characteristics of the participants, including their age, place of residence (1 = urban, 2 = county, 3 = rural areas), job status (1 = stable job or 0 = unstable job), education level (1 = primary school and below, 2 = middle school, 3 = high school or technical school, or 4 = college degree and above) and monthly disposable income (1 = 1500 RMB and below, 2 = 1501–3000 RMB, 3 = 3001–5000 RMB, 4 = 5001–8000 RMB, or 5 = 8001 RMB and above). The response “1500 RMB and below” means very poor, “1500–3000” means low income, “3000–5000” means average income, “5000–8000” means good income, and “8001 RMB and above” means high income.
HIV disclosure
We used one question to assess the HIV disclosure status to the male sexual partner of the participants, i.e., “do you inform your male sexual partner of your HIV-positive status?” We dichotomized the responses into “1 = Disclosure” or “0 = Nondisclosure”.
HIV treatment self-efficacy
HIV treatment self-efficacy was measured using the revised Chinese version of the AIDS self-efficacy scale (HIV-ASES) [38, 39]. A 10-point Likert scale was used to express patient confidence in their ability to achieve each adherence behaviour. The scale contained 12 items, and its response ranged from 1 = “No confidence at all” to 10 = “Completely confident”, and the total score was between 0 and 120. The higher scores reflected better self-efficacy of MSM patients to HIV treatment adherence. The Cronbach’s alpha coefficient was 0.955 for the scale in this study.
Quality of life
It is a multidimensional concept. The Chinese version of the World Health Organization Quality of Life for HIV-abbreviated version (WHOQOL-HIV BREF) scale was used to assess the QOL of MSM patients, which was developed by the WHOQOL-HIV BREF scale in accordance with the Chinese cultural background [40, 41]. The scale contained 31 items that were divided into six domains: physical, psychological, social relationships, independence, environment and spirituality. Each item in each domain had the same weight. The response was a 5-level Likert scale ranging from 1 = “Highly disagree” to 5 = “Highly agree”. The score range of each domain was 4 to 20 and the total score range was 24–120. A higher score indicated a better QOL. The scale had good reliability and validity. The Cronbach’s alpha coefficient was 0.920, and its various domains of Cronbach’s alpha coefficients ranged from 0.586 to 0.821 in this study. Previous studies revealed that the Chinese WHOQOL-HIV BREF scale can be used to measure the QOL of MSM patients in China and to conduct cross-cultural comparative research on QOL [41].
Statistical analysis
All the data were entered into EpiData 3.1 software by two researchers and tested for consistency. We assessed the normal distribution of continuous variables. Means and standard deviations (\(\overline{x }\) ± s) or medians (interquartile range, IQR) were used to describe continuous data, and frequencies (percentages) were estimated for categorical variables. We conducted independent-sample t test, one-way analysis of variance (ANOVA) and Kruskal–Wallis H tests to assess the differences in QOL and the self-efficacy scores among groups with different socio-demographic characteristics. The variables with P < 0.10 in univariate analysis were used as covariates [42].
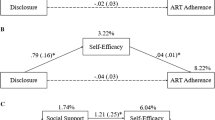
The mediation analyses were examined using the PROCESS macro for SPSS developed by Hayes (2013) and conducted among every different QOL domain [43]. We constructed mediation analysis models with HIV disclosure as the independent variable (X), HIV treatment self-efficacy as the mediator (M) and QOL and its various domains as the dependent variables (Y). The predictive effect of HIV disclosure on self-efficacy was set as a, the predictive effect of self-efficacy on QOL was set as b, the total effect of HIV disclosure on QOL was set as c, and the direct effect after controlling the mediator was c′ (Fig. 1). The bias-corrected nonparametric percentile bootstrap method was used to test the statistical significance of indirect effects based on 5000 resamples. The indirect effects were considered significant if the estimates of the bootstrapped 95% confidence interval (95% CI) did not include zero [44]. All the statistical analyses were performed using SPSS version 24.0 and two-tailed P < 0.05 was considered statistically significant.

Diagram of mediation effect models of HIV disclosure, self-efficacy and QOL. The variables in the dotted box are the various domains of quality of life. *P < 0.05, **P < 0.001
Results
Socio-demographic characteristics
A total of 586 MSM with HIV/AIDS were recruited in this study, and 7 participants were excluded due to the large number of logical errors and missing values in their questionnaires. Therefore, a total of 579 participants were included in the analysis. As shown in Table 1, the median age of MSM patients was 33 (28–39), and the age range was wide (age range, 18–82 years). A total of 87.22% of the respondents were 18–44 years old. In addition, 70.98% of them had a stable job, and 61.66% had a college degree or above. Only 4.66% of participants had little disposable income (< 1500RMB), and 16.06% of them disclosed their HIV infection status to their male sexual partners. In all participants, the QOL score was 87.91 ± 12.73, including 14.08 ± 2.75 in the social relationships domain, 14.92 ± 2.49 in the physical domain, 13.88 ± 2.67 in the psychological, 16.84 ± 2.12 in the independence domain, 13.62 ± 2.67 in the environment domain and 14.56 ± 3.55 in the spirituality domain. The median HIV treatment self-efficacy score was 120.00 (116.00–120.00).The QOL scores of MSM who disclosed were higher than those who did not disclose (t = − 1.972, P < 0.05). In addition, the impacts of having a stable job, the education level, and the monthly disposable income on QOL were statistically significant (t = − 4.473, P < 0.001; H = 7.855, P < 0.001; H = 11.397, P < 0.001). In six domains of QOL, the scores of MSM patients with stable jobs and high monthly disposable income in all domains of QOL were higher than those without (P < 0.05) (as shown in Additional file 1: Table S1).
Mediation model analysis
HIV disclosure had a positive effect on self-efficacy, and self-efficacy was then associated with overall QOL and its physical, psychological, independence and environmental domains (P < 0.05). However, the effects of HIV disclosure were not significant in these domains after considering self-efficacy.
In the social relationships domain, HIV disclosure significantly predicted HIV treatment self-efficacy (a1 = 3.609, P = 0.035) and HIV treatment self-efficacy, which in turn was associated with better QOL in the social relationships domain (b1 = 0.021, P = 0.004). After the mediator was included, HIV disclosure still had a positive effect on social relationships (\({c}^{^{\prime}}\)1 = 0.634, P = 0.035), which indicated that self-efficacy was not the only path between HIV disclosure and the social relationships of MSM patients and played a partial mediation role (Table 2).
In addition, there were no significant effects of HIV disclosure and self-efficacy in the spirituality domain of QOL (\({c}^{^{\prime}}\)6 = 0.400, P = 0.088; b6 = 0.010, P = 0.093). Detailed multivariable analysis results for each domain of QOL were provided in Additional file 1: Tables S2–S7.
Mediation effects testing
The bias-corrected nonparametric percentile bootstrap method was conducted to assess the mediation effects with 5000 resamples. As shown in Table 3, the indirect effects through self-efficacy were all statistically significant (95% CI did not include zero) on the overall QOL and its various domains, which means that self-efficacy was the potential mechanism for explaining the relationship between HIV disclosure and QOL. The mediation effect accounts for 10.70% of the total effect on the domain of social relationships. However, the confidence interval of the mediation effect in the spirituality domain was very close to 0, and the regression coefficient was not statistically significant. It was believed that the mediation effect was very weak and can be ignored. The diagram of the mediation effect model was shown in Fig. 1.
Discussion
In this study we explored the mediating role of HIV treatment self-efficacy between HIV disclosure and QOL among MSM with HIV/AIDS. The findings demonstrated that HIV disclosure was positively associated with self-efficacy, which was related to a better QOL, including the physical, psychological, social relationships, independence and environment domains. The mediation analyses indicated that self-efficacy played an important role in the relationship between HIV disclosure and QOL [25, 45,46,47]. Consistent with the results of a meta-analysis, the proportion of individuals disclosing their HIV infection status to sexual partners was very low (12–53%) and varied according to personal and situational factors [48]. For most MSM patients, it is a great challenge to disclose their HIV infection status. Our study showed that only 16.06% of participants disclosed their HIV infection status to their male sexual partners. Disclosure of HIV infection status is clearly related to reducing HIV transmission, promoting treatment adherence and promting good health [8]. In this study, the QOL scores and its domains of participants with HIV disclosure were higher than those who did not disclose. Although the differences in some domains were not statistically significant, it also showed that HIV disclosure has a positive impact on most domains of QOL. Unlike the general disclosure of previous studies, HIV disclosure makes it easier to obtain understanding, emotional support and positive response. It will increase MSM patients’ belief in fighting disease, improve their self-efficacy, help them actively seek medical treatment strategies, and reduce the probability of missing drugs or hindering their access to medical services [49, 50]. In addition, disclosure behaviour is a positive and reinforcing experience that helps patients accept their disease condition. The encouragement of male sexual partners is combined with their own expectations, which enhances their treatment motivation and confidence. Improving self-efficacy in turn can reduce the expected pressure and promote mental health while improving social relationships. This finding is aligned with the results that the positive rate of depression and other negative results of those who refuse to disclose their HIV status were higher than those who disclose their HIV status [51]. HIV disclosure is an important contributing factor to mental health. Moreover, disclosure behaviour is affected by the surroundings but also affects the surrounding people and environment. We found that disclosure was an important predictor in domains of good social relationships and environment, which was consistent with previous results [26]. We found that disclosure did not have a significant impact on the spirituality domain, either as a direct effect or an indirect effect, which was consistent with a previous study [6].
Our study revealed the mediation mechanism that explained the impact of HIV disclosure on the QOL of MSM with HIV/AIDS. The results showed that self-efficacy was an important mediator that was related to the overall QOL and its physical, psychological, social relationships, independence and environment domains. Self-efficacy was considered to be the key determinant of health promotion behaviour based on social cognitive theory (SCT) [52]. As noted in the study by Jiang, MSM patients with higher self-efficacy were usually more able to accept the reality of the illness and their own health status, had a better mentality and positively sought medical treatment [30]. Therefore, self-efficacy can not only improve their physical health and enhance their autonomy but also enable them to access a good psychological state by reducing anxiety and depression. Previous studies in China also have shown that self-efficacy can help MSM patients make use of various resources to manage disease conditions and reduce the negative impact on their health [31, 53]. Self-efficacy has been shown to be a predictor of health behaviours, such as promoting treatment adherence, and it plays an important role in improving the QOL of MSM patients [54].
This study has some limitations. First, it was a cross-sectional study, which limited the ability to infer the causal and temporal relationships between variables. Future studies should use longitudinal and intervention designs to validate our findings and explore the long-term outcomes of disclosure. Second, the participants were recruited through convenience sampling, which may not fully represent all MSM patients, and selection bias cannot be excluded. Third, self-report measurement may induce social desirability bias, and future research must evaluate the research variables more objectively. Despite these limitations, our results increase the current understanding of the potential path of HIV on QOL and its impact on various domains in MSM patients.
Conclusions
MSM living with HIV/AIDS who disclosed their HIV status to male sexual partners were more likely to have a good QOL. This study showed that HIV disclosure not only had a positive direct effect on the social relationships domain of QOL but also had an indirect impact on it through self-efficacy. In the overall QOL, physical, psychological, independence and environment domains, it only had an indirect impact through self-efficacy. The results emphasized the importance of HIV disclosure for QOL among MSM patients and suggested that health care providers should assist MSM infected persons in deciding whether to disclose their HIV infectious status during daily medical services. In addition, it is not enough to promote disclosure to male sexual partners but also to increase the intervention related to HIV treatment self-efficacy, such as cognitive behavioural interventions [55], to improve the health-related quality of life of MSM with HIV/AIDS.
Availability of data and materials
The datasets generated during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
Abbreviations
- AIDS:
-
Acquired immune deficiency syndrome
- HIV:
-
Human immunodeficiency virus
- ART:
-
Antiretroviral therapy
- PLWH:
-
People living with HIV
- QOL:
-
Quality of life
- MSM:
-
Men who have sex with men
- UAI:
-
Unprotected anal intercourse
- SCT:
-
Social cognitive theory
- HIV-ASES:
-
AIDS self-efficacy scale
- WHOQOL-HIV BREF:
-
World Health Organization Quality of Life for HIV-abbreviated version
- IQR:
-
Interquartile range
- ANOVA:
-
One-way analysis of variance
- CI:
-
Confidence interval
References
Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M,et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–22.
Li X, Huang L, Wang H, Fennie KP, He G, Williams AB. Stigma mediates the relationship between self-efficacy, medication adherence, and quality of life among people living with HIV/AIDS in China. AIDS Patient Care STDS. 2011;25(11):665–71.
Webster P. UNAIDS survey aligns with so-called fourth 90 for HIV/AIDS. The Lancet. 2019;393(10187):2188.
Sun S, Budge S, Shen W, Xu G, Liu M, Feng S. Minority stress and health: a grounded theory exploration among men who have sex with men in China and implications for health research and interventions. Soc Sci Med. 2020;252:112917.
Liu J, Qu B, Hu B, Jiang N, Wang D. The quality of life of men who have sex with men in China: reliability and validity testing of the SF-36 questionnaire. PLoS ONE. 2013;8(12):e83362.
Chen D, Wang M, Duan L, Chen X, Zhang Q, Li X. Quality of life among older Chinese people living with HIV/AIDS: a cross-sectional study in Hunan. Trans R Soc Trop Med Hyg. 2021;116(3):213–21.
Mengwai K, Madiba S, Modjadji P. Low disclosure rates to sexual partners and unsafe sexual practices of youth recently diagnosed with HIV; Implications for HIV prevention interventions in South Africa. Healthcare (Basel). 2020;8(3):253.
Bhagwanjee A, Govender K, Akintola O, Petersen I, George G, Johnstone L, et al. Patterns of disclosure and antiretroviral treatment adherence in a South African mining workplace programme and implications for HIV prevention. Afr J AIDS Res. 2011;10(Suppl 1):357–68.
Grov C, Rendina HJ, Moody RL, Ventuneac A, Parsons JT. HIV serosorting, status disclosure, and strategic positioning among highly sexually active gay and bisexual men. AIDS Patient Care STDS. 2015;29(10):559–68.
Serovich JM, Reed SJ, O’Connell AA, Laschober TC. Relationship between serostatus disclosure and categories of HIV transmission risk in men who have sex with men living with HIV. Int J STD AIDS. 2018;29(8):744–50.
Redd AD, Quinn TC, Tobian AA. Frequency and implications of HIV superinfection. Lancet Infect Dis. 2013;13(7):622–8.
O’Connell AA, Reed SJ, Serovich JA. The efficacy of serostatus disclosure for HIV transmission risk reduction. AIDS Behav. 2015;19(2):283–90.
Pinkerton SD, Galletly CL. Reducing HIV transmission risk by increasing serostatus disclosure: a mathematical modeling analysis. AIDS Behav. 2007;11(5):698–705.
Holmes CB, Sikazwe I, Sikombe K, Eshun-Wilson I, Czaicki N, Beres LK, et al. Estimated mortality on HIV treatment among active patients and patients lost to follow-up in 4 provinces of Zambia: findings from a multistage sampling-based survey. PLoS Med. 2018;15(1):e1002489.
Yonah G, Fredrick F, Leyna G. HIV serostatus disclosure among people living with HIV/AIDS in Mwanza, Tanzania. AIDS Res Ther. 2014;11(1):5.
Dessie G, Wagnew F, Mulugeta H, Amare D, Jara D, Leshargie CT, et al. The effect of disclosure on adherence to antiretroviral therapy among adults living with HIV in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2019;19(1):528.
Gabbidon K, Chenneville T, Peless T, Sheared-Evans S. Self-Disclosure of HIV status among youth living with HIV: a global systematic review. AIDS Behav. 2020;24(1):114–41.
Chaudoir SR, Fisher JD, Simoni JM. Understanding HIV disclosure: a review and application of the Disclosure Processes Model. Soc Sci Med. 2011;72(10):1618–29.
Daskalopoulou M, Lampe FC, Sherr L, Phillips AN, Johnson MA, Gilson R, et al. Non-disclosure of HIV status and associations with psychological factors, ART non-adherence, and viral load non-suppression among people living with HIV in the UK. AIDS Behav. 2017;21(1):184–95.
Dessalegn NG, Hailemichael RG, Shewa-Amare A, Sawleshwarkar S, Lodebo B, Amberbir A, et al. HIV Disclosure: HIV-positive status disclosure to sexual partners among individuals receiving HIV care in Addis Ababa, Ethiopia. PLoS ONE. 2019;14(2):e0211967.
Medley A, Garcia-Moreno C, McGill S, Maman S. Rates, barriers and outcomes of HIV serostatus disclosure among women in developing countries: implications for prevention of mother-to-child transmission programmes. Bull World Health Organ. 2004;82(4):299–307.
Marcus U, Schink SB, Sherriff N, Jones AM, Gios L, Folch C, et al. HIV serostatus knowledge and serostatus disclosure with the most recent anal intercourse partner in a European MSM sample recruited in 13 cities: results from the Sialon-II study. BMC Infect Dis. 2017;17(1):730.
Yin Y, Yang H, Xie X, Wang H, Nie A, Chen H. Status and associated characteristics of HIV disclosure among people living with HIV/AIDS in Liangshan, China: a cross-sectional study. Medicine (Baltimore). 2019;98(31):e16681.
Préau M, Marcellin F, Carrieri MP, Lert F, Obadia Y, Spire B. Health-related quality of life in French people living with HIV in 2003: results from the national ANRS-EN12-VESPA Study. AIDS. 2007;21(Suppl 1):S19-27.
Algaralleh A, Altwalbeh D, Al-Tarawneh F. Health-related quality of life among persons living with HIV/AIDS in Jordan: an exploratory study. HIV AIDS (Auckl). 2020;12:897–907.
Nyongesa MK, Mwangi P, Wanjala SW, Mutua AM, Koot HM, Cuijpers P, et al. Correlates of health-related quality of life among adults receiving combination antiretroviral therapy in coastal Kenya. Health Qual Life Outcomes. 2020;18(1):169.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31(2):143–64.
Lamb KM, Nogg KA, Safren SA, Blashill AJ. Mechanism of change in cognitive behavioral therapy for body image and self-care on ART adherence among sexual minority men living with HIV. AIDS Behav. 2018;22(8):2711–7.
Jiang T, Zhou X, Wang H, Luo M, Pan X, Ma Q, et al. Psychosocial factors associated with quality of life in young men who have sex with men living with HIV/AIDS in Zhejiang, China. Int J Environ Res Public Health. 2019;16(15):2667.
Zhou G, Li X, Qiao S, Shen Z, Zhou Y. HIV symptom management self-efficacy mediates the relationship of internalized stigma and quality of life among people living with HIV in China. J Health Psychol. 2020;25(3):311–21.
Chen WT, Shiu C, Yang JP, Li CR, Wang K, Zhang L, et al. Substance use, anxiety, and self-management efficacy in HIV-positive individuals: a mediation analysis. J Subst Use. 2018;23(4):408–14.
Overstreet NM, Earnshaw VA, Kalichman SC, Quinn DM. Internalized stigma and HIV status disclosure among HIV-positive black men who have sex with men. AIDS Care. 2013;25(4):466–71.
Johnson WD, Hedges LV, Ramirez G, Semaan S, Norman LR, Sogolow E, et al. HIV prevention research for men who have sex with men: a systematic review and meta-analysis. J Acquir Immune Defic Syndr. 2002;30(Suppl 1):S118–29.
Jiao K, Wang C, Liao M, Ma J, Kang D, Tang W, et al. A differentiated digital intervention to improve antiretroviral therapy adherence among men who have sex with men living with HIV in China: a randomized controlled trial. BMC Med. 2022;20(1):341.
Rodríguez Del Águila M, González-Ramírez A. Sample size calculation. Allergol Immunopathol (Madr). 2014;42(5):485–92.
Ferreira AC, Teixeira AL, Silveira MF, Carneiro M. Quality of life predictors for people living with HIV/AIDS in an impoverished region of Brazil. Rev Soc Bras Med Trop. 2018;51(6):743–51.
Johnson MO, Neilands TB, Dilworth SE, Morin SF, Remien RH, Chesney MA. The role of self-efficacy in HIV treatment adherence: validation of the HIV Treatment Adherence Self-Efficacy Scale (HIV-ASES). J Behav Med. 2007;30(5):359–70.
Sun L, Yang SM, Wu H, Chen B, Wang CJ, Li XF. Reliability and validity of the Chinese version of the HIV Treatment Adherence Self-Efficacy Scale in mainland China. Int J STD AIDS. 2017;28(8):829–37.
WHOQOL HIV Group. Initial steps to developing the World Health Organization’s Quality of Life Instrument (WHOQOL) module for international assessment in HIV/AIDS. AIDS Care. 2003;15(3):347–57.
Zhu Y, Liu J, Qu B. Psychometric properties of the Chinese version of the WHOQOL-HIV BREF to assess quality of life among people living with HIV/AIDS: a cross-sectional study. BMJ Open. 2017;7(8):e016382.
Shrestha R, Altice FL, Copenhaver MM. HIV-related stigma, motivation to adhere to antiretroviral therapy, and medication adherence among HIV-positive methadone-maintained patients. J Acquir Immune Defic Syndr. 2019;80(2):166–73.
Bolin JH, Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. J Educ Meas. 2014;51(3):335–7.
Zhao X, Lynch JG, Chen Q. Reconsidering Baron and Kenny: myths and truths about mediation analysis. J Consum Res. 2010;37(2):197–206.
Belay YB, Ali EE, Sander B, Gebretekle GB. Health-related quality of life of patients with HIV/AIDS at a tertiary care teaching hospital in Ethiopia. Health Qual Life Outcomes. 2021;19(1):24.
Chen JP, Han MM, Liao ZJ, Dai ZZ, Liu L, Chen H, et al. HIV-related behaviors, social support and health-related quality of life among men who have sex with men and women (MSMW): a cross-sectional study in Chongqing, China. PLoS ONE. 2015;10(2):e0118651.
Li J, Wu C, Suo C, Zhou H, Lu T, Lu L, et al. Health status and associated factors of HIV-infected patients in Kunming, China. Qual Life Res. 2020;29(10):2661–8.
Cao W, Wong HM, Chang C, Agudile EP, Ekström AM. Behavioral interventions promoting HIV serostatus disclosure to sex partners among HIV-positive men who have sex with men: a systematic review. Int J Public Health. 2019;64(7):985–98.
Perlson J, Scholl J, Mayer KH, O’Cleirigh C, Batchelder AW. To disclose, not disclose, or conceal: a qualitative study of HIV-positive men with multiple concealable stigmatized identities. AIDS Patient Care STDS. 2021;35(2):47–55.
Lim JM, Tan RKJ, Chan JKW. “Do I need to or do I want to?” A typology of HIV status disclosure among gay, bisexual, and other men who have sex with men. AIDS Care. 2020;32(sup2):142–7.
Yu Y, Luo D, Chen X, Huang Z, Wang M, Xiao S. Medication adherence to antiretroviral therapy among newly treated people living with HIV. BMC Public Health. 2018;18(1):825.
Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44(9):1175–84.
Huang L, Li L, Zhang Y, Li H, Li X, Wang H. Self-efficacy, medication adherence, and quality of life among people living with HIV in Hunan Province of China: a questionnaire survey. J Assoc Nurses AIDS Care. 2013;24(2):145–53.
Emlet CA, Fredriksen-Goldsen KI, Kim HJ. Risk and protective factors associated with health-related quality of life among older gay and bisexual men living with HIV disease. Gerontologist. 2013;53(6):963–72.
Spence AB, Michel K, Wang C, Dutton MA, Lee K, Merenstein D, et al. Viral suppression is associated with HIV treatment self-efficacy in a cohort of women in Washington, DC. AIDS Patient Care STDS. 2021;35(3):75–83.
Acknowledgements
The authors thank the medical staffs of Jinan Infectious Disease Hospital in Shandong Province who assisted in patient recruitment and data collection. The authors also thank all the subjects for their participation and cooperation.
Funding
This work received support from the National Key Research and Development Program of China (2017YFE0103800).
Author information
Authors and Affiliations
Contributions
WJ conceptualized the study, conducted the data analysis and completed the writing of the manuscript. KJ conducted the data collation and assisted the writing of the manuscript. ML, CW and DK guided the data collection and analysis. YL assisted in data analysis and revision of the manuscript. KJ, JM, YY, YL, CC, JM, XY, WJ, YC, LW, and ZZ conducted the material preparation, data collection, data entry and management. WM and XW guided and assisted the study design, data analysis and the revision of the manuscript. All authors participated in critical revisions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the principles of the Declaration of Helsinki. The study was approved by the Ethics Committee of the School of Public Health of Shandong University (20190210). The informed consent of all individuals involved in the study has been obtained.
Consent for publication
Participants consented to the publication of their de-identified data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Table S1. Socio-demographic characteristics and relationships with QOL and its various domains a (n = 579). Table S2. Multivariable analyses with HIV treatment self-efficacy and overall QOL as outcomes. Table S3. Multivariable analyses with HIV treatment self-efficacy and physical as outcomes. Table S4. Multivariable analyses with HIV treatment self-efficacy and psychological as outcomes. Table S5. Multivariable analyses with HIV treatment self-efficacy and independence as outcomes. Table S6. Multivariable analyses with HIV treatment self-efficacy and environment as outcomes. Table S7. Multivariable analyses with HIV treatment self-efficacy and spirituality as outcomes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jia, W., Jiao, K., Ma, J. et al. HIV infection disclosure, treatment self-efficacy and quality of life in HIV-infected MSM receiving antiretroviral therapy. BMC Infect Dis 22, 937 (2022). https://doi.org/10.1186/s12879-022-07932-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07932-z