
Abstract
Background
Recurrence continues to place significant burden on patients and tuberculosis programmes worldwide, and previous studies have rarely provided analysis in negative recurrence cases. We characterized the epidemiological features of recurrent pulmonary tuberculosis (PTB) patients, estimated its probability associated with different bacteriology results and risk factors.
Methods
Using 2005–2018 provincial surveillance data from Henan, China, where the permanent population approximately were 100 million, we described the epidemiological and bacteriological features of recurrent PTB. The Kaplan–Meier method and Cox proportional hazard models, respectively, were used to estimate probability of recurrent PTB and risk factors.
Results
A total of 7143 (1.5%) PTB patients had recurrence, and of 21.1% were bacteriological positive on both laboratory tests (positive–positive), and of 34.9% were negative–negative. Compared with bacteriological negative recurrent PTB at first episodes, the bacteriological positive cases were more male (81.70% vs 72.79%; P < 0.001), higher mortality risk (1.78% vs 0.92%; P = 0.003), lower proportion of cured or completed treatment (82.81% vs 84.97%; P = 0.022), and longer time from onset to end-of-treatment. The probability of recurrence was higher in bacteriological positive cases than those in bacteriological negative cases (0.5% vs 0.4% at 20 months; P < 0.05).
Conclusions
Based on patient’s epidemiological characteristics and bacteriological type, it was necessary to actively enact measures to control their recurrent.
Similar content being viewed by others

Background
Recurrence of tuberculosis (TB) is defined as patients who have previously been treated for TB, and were declared cured or treatment completed at the end of their most recent course of treatment, and now are diagnosed with a recurrent episode of TB (either a endogenous reactivation of a previous infection or a new episode of TB caused by reinfection) [1]. According to WHO global estimates, approximately 430,000 previously treated patients experienced bacteriologically confirmed or clinically diagnosed recurrence in 2015, representing 7% of all notified TB cases [2]. In detail, approximately 5% of patients with drug-susceptible tuberculosis have a recurrence after 6 months of first-line therapy, and approximately 20% of patients have a recurrence after 4 months of short-course therapy, even when regimens include a fluoroquinolone [3]. Therefore, recurrence has become the core stumbling block to achieve WHO’s target of eradicating TB in 2035.
In China, extensive studies have been published on TB recurrence; however, most of these studies have focused on pathogens of bacteriological positive cases caused by exogenous reinfection or endogenous relapse as well as the relationship between recurrence and drug resistance [4,5,6]. However, these studies have rarely provided analysis in negative recurrence cases, which consists of 35.4% of the total recurrence of TB in a previous study [7] and unlike the bacteriological positive cases, most of them are lack of timely diagnosis and treatment. Therefore, it is worthwhile to conduct a comprehensive study on this topic to elucidate the factors that may be associated with the different features of bacteriological positive and negative recurrence cases.
Henan, with approximately 100 million residents, is one of the most populous provinces in China [8], and the number of new cases is about 60,000 each year and accounts for almost 10% of the national TB patients of China mainland [9]. In this retrospective study, we describe the epidemiological features of all recurrent pulmonary tuberculosis (PTB) cases from 2005 to 2008 in Henan province, estimate the recurrence probability of bacteriological positive and negative cases, and explore the risk factors of recurrent PTB.
Methods
Data sources
The information of PTB cases from January 1, 2005 to December 31, 2018, which were reported to the Tuberculosis Information Management System (TBIMS) as the national TB surveillance system within 24 h after diagnosis [10], were collected and included basic demographics, time of illness onset and diagnosis, laboratory outcomes, supervisor mode, and treatment outcomes.
Case definitions
Based on WHO guideline, clinical-diagnosed PTB patients [1] and bacteriologically-confirmed patients were defined respectively. We defined clinical-diagnosed PTB as bacteriological negative PTB, clinical diagnosis was based on TB-specialized chest imaging, supplemented by epidemiological investigation, clinical manifestation (coughing, expectoration ≥ 2 weeks, or hemoptysis), or results of an immunology test (tuberculin skin test and/or interferon gamma release assay), and effective experimental treatment using antituberculosis drugs for 2 months. Bacteriological positive PTB was based on laboratory evidence (sputum smear, culture and Genxpert) of infection with Mycobacterium tuberculosis (M.TB). Both were defined as PTB patients in our study.
We identified patients with at least two episodes of PTB reported in the TBIMS by matching records using any of the following screening criteria: (1) having highly similar patient names; (2) having highly similar patient names and home addresses; (3) having highly similar patient names, home addresses, and birth dates. We considered patients to have recurrent TB if they experienced at least two independent episodes of TB. An independent episode was defined as a case wherein a patient who was previously diagnosed with PTB and received anti-tuberculosis treatment was declared cured at the end of the course or completion of treatment but was subsequently diagnosed with PTB again. Additionally, patients with at least two independent episodes of recurrent laboratory-confirmed PTB were classified into this group. We also excluded the following PTB patients: (1) not cured; (2) treatment was not completed at the end of their most recent course of treatment.
Because of the retrospective study design, there was no active follow-up for all of the cases. We defined the passive follow-up time as the time after the end of the initial tuberculosis treatment until an event (recurrence) or the censored date (December 31, 2018). To aid comparison with other published studies, we also looked at the proportion of recurrence among a subset of all pulmonary cases, bacteriologically confirmed pulmonary cases who completed treatment.
Data analysis
Descriptive analyses of recurrent PTB cases were performed using a descriptive method to analyze continuous variables and categorical variables. The Kaplan–Meier method was used to estimate the recurrence curve of PTB. The probability of first and second recurrences of PTB were both calculated. Subgroups of interest were compared using the log rank test. The risk factors associated were explored using Cox proportional hazard models. Only the first episode of recurrence was included in the Cox models. Unadjusted hazard ratios (HRs) and adjusted HRs (aHRs) were estimated from a univariable analysis and multivariable analysis, respectively.
All statistical analyses were performed with R (version 3.3.0). All statistical tests were two-sided with a significance level of p < 0.05.
Results
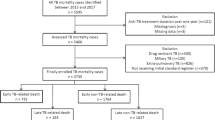
From 2005 to 2018, a total of 976,526 PTB episodes occurring in Henan province were reported to the TBIMS. Excluding single TB episodes, extrapulmonary tuberculosis, and non-independent episodes, 7143 patients (having 14,717 [1.5%] episodes) were identified as having recurrent PTB. Among all PTB and bacteriological confirmed PTB cases, who completed treatment for the first episode, the proportion of recurrence was 1.8% and 2.2% respectively. Among the 7143 recurrent patients, 94.3% (6739) of these patients had two episodes and 5.7% had more than two episodes: 379 (5.3%) patients had three episodes and 25 (0.4%) had at least four episodes. Bacteriological results revealed that 21.1% of patients with recurrence tested bacteriological positive on both laboratory tests, 34.9% tested bacteriological negative on both tests, 23.4% tested bacteriological positive on the first test and bacteriological negative on the second, and 13.6% tested bacteriological negative on the first test and bacteriological positive on the second (Fig. 1; Additional file 1: Fig. S1).

Flowchart showing screening and analysis of patients with recurrent PTB from the national TB surveillance database in Henan province, China from 2005 to 2018
Demographic characteristics
The overall male to female ratio was 3.4:1. The median age at primary onset of all patients with recurrent PTB was 54 years (interquartile range [IQR]: 40–64), which was higher than that of non-recurrent cases (48 [IQR: 28–63]). In addition, the median ages of patients with one recurrence, two recurrences, and three or more recurrences were 57 (IQR: 42–67), 59 (IQR: 48–68), and 63 (IQR: 54–68), respectively. 50.7% of recurrent cases received enhanced supervision, 49.2% received a directly observed treatment short course chemotherapy (DOTS), and 0.1% performed self-medication. Additionally, the proportion of death in recurrent cases was higher than that in non-recurrent cases, and the proportions of death with one recurrence, two recurrences and three recurrences were 1.4%, 1.9%, and 4.0%, respectively (Table 1). Compared with bacteriological negative recurrent PTB at first episodes, bacteriological positive cases had higher proportion of male patients (81.70% vs 72.79%; p < 0.001) and DOTS management mode (99.08% vs 5.45%; p < 0.001). And higher levels of mortality risk (1.78% vs 0.92%; p = 0.003), lower proportion of cured or treatment completed patients (82.81% vs 84.97%; p = 0.022), and longer time from onset to course end were also observed for bacteriological positive recurrent PTB at first episodes (Table 2).
Probability of recurrence
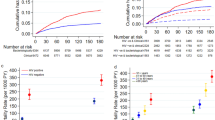
The median times from the completion of first episode to recurrent tuberculosis were 17.6 months (IQR: 8.3–33.9), 17.6 months (IQR: 8.3–32.5), and 17.5 months (IQR: 8.3–35.5) for all pulmonary cases, bacteriological negative cases, and bacteriological positive cases, respectively (p = 0.121). Figure 2 depicted the probabilities of the recurrences of the three types of TB cases. Specifically, after the primary episode of PTB (Fig. 2A, B), the recurrences of all PTB and bacteriological positive PTB were similar along with the probabilities of 0.4%, 0.6%, and 0.7% at 20, 40, and 60 months, respectively, and then remained stable after 60 months. The recurrence probabilities of bacteriological negative cases were slightly lower than the positive cases (p < 0.05), but still showed an increasing trend.

The probability of PTB recurrence after primary PTB diagnosis in Henan province, China from 2005 to 2018. A Probability of recurrence in primary PTB patients. B Probability of recurrence in primary PTB patients with bacteriological positive and negative cases. C Probability of recurrence after first recurrence. D Probability of recurrence after first recurrence with bacteriological positive and negative cases
Compared to the first scenario, during the median time of 15.7 (IQR: 7.5–24.4) months after the second PTB episode in patients with recurrence, the recurrence probabilities were much higher regardless of the types of PTB cases (Fig. 2C, D). All PTB and bacteriological positive cases shared similar probabilities of 3.6%, 5.2%, and 5.6% at 20, 40, and 60 months, respectively. And bacteriological negative PTB had significantly lower probabilities at the same time point. After 62 months, all probabilities kept stable like that in the first scenario.
Risk factors associated with recurrence
Compared to female, males had higher risk of recurrence with aHRs of 1.29 (95% CI 1.22–1.36). Patients with older age had higher risk of recurrence, compared to the 0–14 years group (reference group), the aHR was 2.32 (95% CI 1.49–3.62) for patients aged 45–59 years, and was 2.07 (95% CI 1.32–3.22) for subjects aged ≥ 60 years (p < 0.001). Bacteriological positive cases also exhibited consistently higher risk of recurrence, and the aHRs was 1.27 (95% CI 1.21–1.33) comparing to the negative cases. A longer time from illness onset to cure was associated with greater risk of recurrence, compared to the group of cases with time from illness onset to cure < 6 months (reference group), the aHR was 7.01 (95% CI 5.43–9.04) for cases with time from illness onset to cure between 6 and 12 months, and was 8.32 (95% CI 6.34–10.93) for cases with time from illness onset to cure > 12 months (p < 0·001) (Table 3).
We then assessed the multivariate analysis of hazard ratios of characteristics of bacteriological positive cases and bacteriological negative cases, respectively. In the multivariate analysis, bacteriological negative patients aged 45–59 years and ≥ 60 years were at high risk for recurrence (aHR: 1.92 [1.19–3.07]; aHR: 1.92 [1.20–3.08]) but bacteriological positive patients only had a higher risk on those aged 45–59 years (aHR: 5.09 [1.27–20.44]). There were no other significant differences in risk factors between the two groups (Table 4).
Discussion
The findings from this study showed the overall proportion of recurrent tuberculosis to be 1.5%. The hazard of recurrent tuberculosis was significantly higher for tuberculosis patients who were male, older age, bacteriological positive cases, and with a longer time from illness onset to cure. Notably, bacteriological positive recurrence cases had higher mortality risk (1.78% vs 0.92%; p = 0.003) and lower cure or treatment completement rate (82.81% vs 84.97%; p = 0.022) than bacteriological negative cases.
A WHO report estimated that 6.8% of TB cases recurred worldwide in 2019 [11], and recurrence occurs not only in high TB incidence countries, but also in low countries [12,13,14]. A retrospective study of surveillance data and clinical records in Finland showed 0.6% of TB cases were recurrent from 1995 to 2013 [15], and 1.3% of TB cases were recurrent in Barcelona from 2003 to 2006 [12], and the proportion of recurrent cases between 4.2 and 5.7% in the United States during 1993–2010 [16]. In addition, 5.3% of successfully treated bacteriologically confirmed cases had a recurrence in Shanghai [5], China, and 6.8% in Beijing [6]. In comparison, 2.2% of bacteriological confirmed PTB cases who completed treatment recurred in Henan province from 2005 to 2018. Shanghai and Beijing had more comprehensive PTB case detection, treatment and management strategies, compared with the area of Henan, which helped find more PTB and recurrent patients. For example, the administrative department of Shanghai required all pulmonary tuberculosis patients to test sputum culture, and the pathogenic positive rate to be above 50% [17], and extended free tuberculosis treatment to all migrants [18] (free treatment was not available outside individuals’ originally registered residence in Henan). Of course, differences in enrollment patients, the criteria for defining cases as recurrent TB, and the length of the study varied between studies and limit the comparisons.
In this study, we found male gender and older age were related to recurrence, which were in line with some previous reports [19,20,21,22]. We also observed that more proportion of men had bacteriological positive PTB recurrent PTB at first episodes (81.70% vs 72.79%), because men tended to have radiographic abnormalities, positive results on smear microscopy, and culture positivity compared with women [23,24,25]. The time from illness onset to cure within 6 months was associated with a lower risk of recurrence than that for the period beyond 6 months. The aHR also increased with prolongation of treatment time. This demonstrates that longer treatment periods are associated with a higher chance of recurrence and could be due to the treatment noncompliance [22]. Compared with bacteriological negative PTB cases, bacteriological positive PTB cases were more likely to recur. We found that patients with bacteriological positive results had a longer treatment period and some researches showed that bacteriology-negative PTB can be treated for a shorter duration [26]. During the longer treatment period, because of factors such as adverse reactions, cost and stigma [27], there was a lower treatment completion or cure rate on bacteriological positive patients (82.81% vs 84.97%). Furthermore, incomplete or irregular treatment could increase disease recurrence [22]. The health system needs to pay attention to the case management of recurrent patients to ensure patients finish the treatment or take the drugs irregularly, having a benefit impact on reducing recurrence. In addition, bacteriologically positive PTB presented with more symptoms and were more likely to have cavitary lesions than patients with bacteriologically negative PTB [28]. Cavitation on radiology was the risk factor for tuberculosis recurrence [29], which may make bacteriologically confirmed PTB more likely to recur.
More intriguingly, our study specifically evaluated the recurrence of bacteriological negative cases though it had a lower mortality risk than bacteriological positive recurrence cases as previously reported (0.92% vs. 1.78%) but with a more complicated diagnosis criteria. Even if not bacteriological confirmed, such bacteriology-negative PTB may be hindered in routine clinical practice and with high likelihood of progression to transmissible bacteriology-positive disease if left untreated or treated inappropriately [30]. Recent studies suggested the detection from the perspective of immunology mechanisms including the T cell dysfunction and the transitional changes in interferon (IFN)-γ responses [31], as well as the alterations of MTB-specific IgG profiles [32]. These suggest a potential exploration of immunological biomarkers for the detection of bacteriology-negative PTB cases, which may help increase its detection rate in clinical setting and further reduce the recurrence of PTB.
This study has several limitations. First, although most of the clinically diagnosed PTB were caused by M.TB, Non-tuberculosis mycobacteria (NTM) infection cannot be ruled out, because the symptom, image feature and treatment scheme of NTM infection are almost the same as that of M.TB infection. Second, we did not obtain M.TB and blood samples; therefore, we were unable to distinguish between recurrent cases due to reactivation and those due to re-infection, or to investigate their respective risk factors. Third, we were limited to the information routinely collected in the TBIMS, which at the time did not include potentially important variables such as underlying medical conditions, drug resistance status, and clinical symptoms. Further implementation of clinical and treatment characteristics of recurrent TB stratified by bacteriology results will provide more information to understand recurrence. In addition, due to the lack of patient identification numbers, there may be some misclassification of recurrence cases, which caused an underestimation of the proportion of recurrences. And we do not get the national recurrent data, and there is no literature to report the epidemiological characteristics of recurrent cases in China in the national scale, therefore, we cannot compare it with the national recurrent level.
Conclusions
In conclusion, our study provides a detailed overview of the epidemiology of PTB recurrence from 100 million residents in China. Our findings suggest although bacteriological positive cases had higher risk of recurrence than bacteriological negative cases, and bacteriological positive recurrence cases had higher mortality risk, it was not neglected the clinical diagnosis PTB recurrence cases. It was necessary for the increase of recurrent cases to actively targeted interventions to control based on its epidemiological characteristics.
Availability of data and materials
The data comes from the Henan Provincial Center for Disease Control and Prevention. If you want data, you can contact Guolong Zhang. The email is 1296190445@qq.com.
References
WHO. Definitions and reporting framework for tuberculosis—2013 revision. WHO 2013 (2020 update). https://apps.who.int/iris/bitstream/handle/10665/79199/9789241505345_eng.pdf?sequence=1&isAllowed=y.
Romanowski K, Balshaw RF, Benedetti A, et al. Predicting tuberculosis relapse in patients treated with the standard 6-month regimen: an individual patient data meta-analysis. Thorax. 2019;74(3):291–7.
Colangeli R, Jedrey H, Kim S, et al. Bacteriological factors that predict relapse after tuberculosis therapy. N Engl J Med. 2018;379(9):823–33.
Zong Z, Huo F, Shi J, et al. Relapse versus reinfection of recurrent tuberculosis patients in a national tuberculosis specialized hospital in Beijing, China. Front Microbiol. 2018;9:1858.
Shen X, Yang C, Wu J, et al. Recurrent tuberculosis in an urban area in China: relapse or exogenous reinfection? Tuberculosis. 2017;103:97.
Liu Y, Zhang X, Yu J, et al. Tuberculosis relapse is more common than reinfection in Beijing, China. Infect Dis. 2020;52(12):858–65.
Crofts JP, Andrews NJ, Barker RD, et al. Risk factors for recurrent tuberculosis in England and Wales, 1998–2005. Thorax. 2010;65(4):310–4.
Henan Provincial Bureau of Statistics. Communique of the seventh national population census of Henan province. http://www.ha.stats.gov.cn/2021/05-14/2145057.html.
Jiang H, Zhang G, Yin J, et al. Assessment of Strategies and Epidemiological Characteristics of Tuberculosis in Henan Province, China: Observational Study. JMIR public health and surveillance 2021;7(1): e24830.
Jiang H, Liu M, Zhang Y, et al. Changes in Incidence and Epidemiological Characteristics of Pulmonary Tuberculosis in Mainland China, 2005-2016. JAMA Network Open. 2021; 4(4): e215302.
World Health Organization. Global tuberculosis report 2020. World Health Organization. 2020. https://apps.who.int/iris/handle/10665/336069.
Millet JP, Shaw E, Orcau A, et al. Tuberculosis recurrence after completion treatment in a European city: reinfection or relapse? PLoS ONE. 2013;8(6): e64898.
Panjabi R, Comstock GW, Golub JE. Recurrent tuberculosis and its risk factors: adequately treated patients are still at high risk. Int J Tuberc Lung Dis. 2007;11(8):828–37.
Dobler CC, Crawford AB, Jelfs PJ, et al. Recurrence of tuberculosis in a low-incidence setting. Eur Respir J. 2009;33(1):160–7.
Korhonen V, Soini H, Vasankari T, et al. Recurrent tuberculosis in Finland 1995–2013: a clinical and epidemiological cohort study. BMC Infect Dis. 2017;17(1):721.
Kim L, Moonan PK, Yelk Woodruff RS, et al. Epidemiology of recurrent tuberculosis in the United States, 1993–2010. Int J Tuberc Lung Dis. 2013;17(3):357–60.
General Office of Shanghai Municipal Government. Tuberculosis prevention and control plan of Shanghai in the 13th five-year plan period. http://wsjkw.sh.gov.cn/zdjb-zcwj/20191014/0012-65415.html.
Yang C, Lu L, Warren JL, et al. Internal migration and transmission dynamics of tuberculosis in Shanghai, China: an epidemiological, spatial, genomic analysis. Lancet Infect Dis. 2018;18(7):788–95.
Kim L, Moonan PK, Heilig CM, et al. Factors associated with recurrent tuberculosis more than 12 months after treatment completion. Int J Tuberc Lung Dis. 2016;20:49–56.
Pettit AC, Kaltenbach LA, Maruri F, et al. Chronic lung disease and HIV infection are risk factors for recurrent tuberculosis in a low-incidence setting. Int J Tuberc Lung Dis. 2011;15(7):906–11.
Datiko DG, Lindtjorn B. Tuberculosis recurrence in smear-positive patients cured under DOTS in southern Ethiopia: retrospective cohort study. BMC Public Health. 2009;9(1):1–5.
Picon PD, Bassanesi SL, Caramori ML, et al. Risk factors for recurrence of tuberculosis. J Bras Pneumol. 2007;33(5):572–8.
Austin JF, Dick JM, Zwarenstein M. Gender disparity amongst TB suspects and new TB patients according to data recorded at the South African institute of medical research laboratory for the Western Cape Region of South Africa. Int J Tuberc Lung Dis. 2004;8(4):435–9.
Boum Y II, Atwine D, Orikiriza P, et al. Male gender is independently associated with pulmonary tuberculosis among sputum and non-sputum producers people with presumptive tuberculosis in Southwestern Uganda. BMC Infect Dis. 2014;14:638.
Lawson L, Lawson JO, Olajide I, et al. Sex differences in the clinical presentation of urban Nigerian patients with pulmonary tuberculosis. West Afr J Med. 2008;27(2):82–6.
Blumberg HM, Burman WJ, Chaisson RE, et al. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003;167(4):603–62.
Munro SA, Lewin SA, Smith HJ, et al. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7): e238.
Nguyen MV, Jenny-Avital ER, Burger S, et al. Clinical and radiographic manifestations of sputum culture-negative pulmonary tuberculosis. PLoS ONE. 2015;10(10): e0140003.
Sonnenberg P, Murray J, Glynn JR, et al. HIV-1 and recurrence, relapse, and reinfection of tuberculosis after cure: a cohort study in South African mineworkers. Lancet. 2001;358(9294):1687–93.
Achkar JM, Jenny-Avital ER. Incipient and subclinical tuberculosis: defining early disease states in the context of host immune response. J Infect Dis. 2011;204(suppl 4):S1179–86.
Caminero JA, Pena MJ, Campos-Herrero MI, et al. Exogenous reinfection with tuberculosis on a European island with a moderate incidence of disease. Am J Respir Crit Care Med. 2001;163:717–20.
Lu LL, Smith MT, Yu KKQ, et al. IFN-gamma-independent immune markers of Mycobacterium tuberculosis exposure. Nat Med. 2019;25(6):977–87.
Acknowledgements
Not applicable.
Funding
This study was funded by grants from the National Key Research and Development Program (2018YFC2000300); National Natural Science Foundation of China (U1903118); Beijing Natural Science Foundation (No. Z200001); Natural Science Foundation of China (No. 11971478); Public Health & Disease Control and Prevention, fund for building World-Class Universities (Disciplines) of Renmin University of China.
Author information
Authors and Affiliations
Contributions
WL, GZ and WX conceived, designed and supervised the study. YY and JX collected the data. CC, LZ, CZ, and JJ cleaned the data. HJ, JY and FL analyzed the data. HJ wrote the drafts of the manuscript. HJ, WL and XG interpreted the findings. WL and GZ commented on and revised the drafts of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Data of this study is from the China Tuberculosis Information Management System (TBIMS) Tuberculosis is one of the legal infectious diseases in China, based on the law of the People’s Republic of China on prevention and control of infectious diseases, all cases of PTB need to be reported through the National Notifiable Infectious Disease Surveillance System, and TBIMS is part of this system. As a part of continuing public health, the collection of data from TB cases was exempted from institutional review board assessment by the National Health Commission of the People’s Republic of China. Moreover, although the data of this study were not anonymous, all methods in this study were carried out in accordance with relevant guidelines and regulations in the declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
All authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Flow chart of showing screening of tuberculosis cases with completed treatment or cured.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jiang, H., Yin, J., Liu, F. et al. Epidemiology of recurrent pulmonary tuberculosis by bacteriological features of 100 million residents in China. BMC Infect Dis 22, 638 (2022). https://doi.org/10.1186/s12879-022-07622-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07622-w