
Abstract
Background
Delafloxacin is a novel fluoroquinolone with broad antibacterial activity against pathogens causing acute bacterial skin and skin structure infections (ABSSSI). This network meta-analysis (NMA) was conducted to evaluate the relative efficacy of delafloxacin versus other comparators used for managing patients with ABSSSI.
Methods
A systematic literature review was conducted to identify randomised controlled trials (RCTs) evaluating adults (≥ 18 years) with ABSSSI, complicated SSSI (cSSSI), complicated skin and soft tissue infections (cSSTI) or severe cellulitis with pathogen of gram-positive, gram-negative, or mixed aetiology. OVID MEDLINE®, Embase, Epub Ahead of Print, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews were searched from inception through 12 April 2019. A feasibility assessment was conducted, followed by an NMA, which was run in a Bayesian framework. The interventions included in the NMA encompassed monotherapy or combination therapies of amoxicillin/clavulanate, ampicillin/sulbactam, ceftaroline, ceftobiprole, dalbavancin, daptomycin, delafloxacin, fusidic acid, iclaprim, linezolid, omadacycline, oxacillin + dicloxacillin, standard therapy, tedizolid, telavancin, tigecycline, vancomycin, vancomycin + aztreonam and vancomycin + linezolid.
Results
A feasibility assessment was performed and evidence networks were established for composite clinical response (n = 34 studies), early clinical response (n = 16 studies) and microbiological response (n = 14 studies) in the overall study population, composite clinical response (n = 4 studies) in obese subpopulation and for composite clinical response (n = 18 studies) and microbiological response (n = 14 studies) in patients with methicillin-resistant Staphylococcus aureus (MRSA) infection. Delafloxacin performed significantly better than fusidic acid, iclaprim, vancomycin, and ceftobiprole for composite clinical response. Delafloxacin was comparable to dalbavancin, daptomycin, fusidic acid, iclaprim, linezolid, omadacycline, tedizolid, vancomycin, vancomycin + aztreonam and vancomycin + linezolid in the analysis of early clinical response, whereas for microbiological response, delafloxacin was comparable to all interventions. In the obese subpopulation, the results favoured delafloxacin in comparison to vancomycin, whilst the results were comparable with other interventions among the MRSA subpopulation.
Conclusions
Delafloxacin is a promising new antibiotic for ABSSSI demonstrating greater improvement (composite clinical response) compared to ceftobiprole, fusidic acid, iclaprim, telavancin and vancomycin and comparable effectiveness versus standard of care for all outcomes considered in the study.
Similar content being viewed by others


Introduction
Complicated skin and soft tissue infections (cSSTI), or complicated skin and skin structure infections (cSSSI), represent a severe form of skin infections involving the skin and deeper soft tissues [1]. cSSSI have been associated with increasing morbidity, mortality and healthcare costs in recent decades [1, 2]. The overall incidence of SSTI in the United States (US) increased 40% from 2.4 million in 2000 to 3.3 million in 2012 [3]. In 2013, the US Food and Drug Administration (FDA) distinctly defined a subset of severe skin infections as acute bacterial skin and skin structure infections (ABSSSI) to facilitate the clinical development of drugs and evaluate efficacy of novel antibiotics through quantifiable variables such as lesion size and systemic signs of infections [4, 5]. According to the US FDA, ABSSSI include cellulitis, erysipelas, wound infections or major cutaneous abscesses with a minimum lesion surface area of 75 cm2, measured by erythema, oedema or induration [5, 6]. ABSSSI are caused most commonly by gram-positive bacteria such as Streptococcus pyogenes and Staphylococcus aureus, including methicillin-resistant S. aureus (MRSA) strains [5, 7, 8]. In 2018, epidemiological data from 30 participating countries in the European Antimicrobial Resistance Surveillance (EARS) network and European Centre for Disease prevention and Control (ECDC) estimated that MRSA accounted for 16.4% of all S. aureus isolates, with significant differences in national MRSA percentages ranging from 0% in Iceland to 43% in Romania [9]. The Centre for Disease Control and Prevention has recognised MRSA as a serious health threat to humans with an estimated 323,700 hospitalisations and 10,600 deaths across the US in 2017 [10]. Despite a decline in MRSA- related hospitalisations since 2005, MRSA accounts for significant morbidity and mortality in the US [11, 12].
Treatment approaches for ABSSSI according to the Infectious Disease Society of America (IDSA) practice guidelines include surgical drainage or debridement when appropriate, culture and susceptibility testing and appropriate empiric antibiotic therapy [6]. The increasing prevalence of MRSA in the past decade has altered the therapeutic approach to ABSSSI [6, 13]. The IDSA guidelines recommend vancomycin as the first-line agent for MRSA ABSSSI [6]. However, higher vancomycin doses often used to treat MRSA infections may lead to serious complications such as nephrotoxicity, ototoxicity and hypersensitivity reactions, which can be associated with prolonged hospitalisation and increased healthcare costs [14,15,16,17]. Other recommended antibiotics for MRSA include linezolid, daptomycin, ceftaroline and telavancin [6]. However, these antibiotics are ineffective against gram-negative bacteria, except ceftaroline which is effective against some gram-negative pathogens, excluding Pseudomonas aeruginosa and multi-drug resistant gram-negative bacteria [18]. Nafcillin, cefazolin and clindamycin may also be considered for ABSSSI caused by methicillin-sensitive S. aureus (MSSA) [6, 19]. The antimicrobial activity of recently approved antibiotics for the treatment of ABSSSI, namely, dalbavancin [20], oritavancin [21] and tedizolid [22] are also limited to strains of gram-positive pathogens, including MRSA. The global emergence of MRSA strains and other resistant pathogens in recent years has imposed a considerable challenge to its management, compelling a drive to develop safe and effective antibiotics for the treatment of ABSSSI, including MRSA-related infections [9, 23].
Obese patients with ABSSSIs are at a higher risk of treatment failure and have demonstrated slow recovery [24, 25] According to the World Health Organisation, globally 39% adults (≥ 18 years) were overweight, whilst about 13% of the world’s adult population was obese in 2016, making it a clinically important subpopulation of interest [26].
Delafloxacin, a novel fluoroquinolone with activity against a diverse range of gram-positive (S. aureus,[including MRSA] and Streptococcus pyogenes) and gram-negative bacteria (Pseudomonas aeruginosa, Escherichia coli and Klebsiella pneumoniae), was approved by the US FDA for ABSSSI in 2017 and by the European Medicines Agency in 2019 [27,28,29]. Delafloxacin is available in oral and intravenous (IV) forms, at a recommended dose of 300 mg IV or 450 mg orally once every 12 h [28]. The clinical efficacy of delafloxacin was explored in a large developmental programme that included two phase III clinical trials, demonstrating that delafloxacin was non-inferior to the combination of vancomycin plus aztreonam for the treatment of ABSSSI [30, 31]. Whilst the efficacy of delafloxacin in ABSSSI was assessed in comparison to vancomycin plus aztreonam, there are no randomised controlled trials (RCTs) available to assess the comparative effectiveness for other comparators used for the management of ABSSSI.
Two previous systematic literature reviews (SLRs) and meta-analyses investigating the safety and efficacy of delafloxacin for the treatment of ABSSSI in adult patients demonstrated similar clinical cure rates of delafloxacin versus comparators in the treatment of ABSSSI and MRSA ABSSSI’s [32, 33]. However, these studies included publications with ABSSSI populations only and as such, evaluated overall clinical cure or microbiological response for limited number of interventions (i.e. ceftobiprole, linezolid, tigecycline, and vancomycin/aztreonam) among the current standard of care for the treatment of ABSSSI. This network meta-analysis (NMA) aims to add to the existing knowledge on the performance of delafloxacin in terms of composite clinical response, microbiological response and early response versus the current standard of care, including obese patients (body mass index [BMI] ≥ 30 kg/m2) and patients with MRSA.
Methods
An SLR was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 to identify the clinical evidence from RCTs for delafloxacin versus standard of care in adult patients with ABSSSI, cSSSI, cSSTI or severe cellulitis [34].
Data sources and search strategy
OVID MEDLINE®, Embase, Epub Ahead of Print (In-process & other non-indexed citations), and Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews were searched for relevant RCTs with a prespecified search strategy. Additional searches were performed in the conference proceedings of European Society of Clinical Microbiology and Infectious Diseases, Infectious Diseases Week and World Antimicrobial Resistance Congress Europe from 2017 to 2019. The searches executed in the SLR were based on pre-defined patient population, intervention, comparators, outcome measures and study design criteria (Additional file 1: Appendix A). RCTs involving adult patients with ABSSSI, cSSSI, cSSTI or severe cellulitis, were selected for inclusion. The databases were systematically searched from inception through 12 April 2019.
Study selection and identification
All identified records were exported to Microsoft® Excel after removing duplicates in a reference management software. Abstract screening was conducted based on pre-defined eligibility criteria. Publications with uncertainty were reviewed by an independent second reviewer, and any disagreement was resolved either through “reconciliation” (discussion between the two reviewers) or through “arbitration” with a third independent reviewer where “majority view” determined the inclusion/exclusion. All records included at the end of this stage were retained for full text review, followed by data extraction and quality appraisal. A descriptive quality assessment of the included RCTs was performed using the Cochrane checklist as per the National Institute for Health and Care Excellence (NICE) technical support document (TSD) 2 for NMA of RCTs of RCTs (Additional file 1: Appendix B) [35, 36].
Feasibility assessment
The feasibility of conducting an NMA was examined by first assessing if a connected network of evidence could be established for each outcome of interest, based on the clinical evidence identified from the SLR. The studies included in the connected networks were further assessed for the presence and extent of between-study heterogeneity. To assess the comparability of study populations, a comparison of patients’ baseline characteristics (i.e. age, gender, BMI, race, MRSA/MSSA population, treatment duration, polymicrobial infections, and comorbidities) was conducted. Study design characteristics for all included RCTs (e.g. cross-over or open label) were assessed to identify potential sources of bias that could impact the outcomes of interest (Additional file 1: Appendix C).
Evidence synthesis assumptions
Assumptions on study outcomes
Due to the heterogeneity of outcome definitions, studies with similar outcome definitions at similar timepoints were grouped together, and any assumptions were validated by two clinical experts (Additional file 1: Appendix D).
The RCTs reporting clinical cure or success outcomes at the end of therapy, test of cure (TOC), post-therapy evaluation or follow-up were considered for the outcome ‘composite clinical response’ in the analysis. Wherever a study reported both clinical cure and clinical success, clinical success was considered as the efficacy outcome for analysis. ‘Early response’ was determined as either ≥ 20% lesion size reduction or early clinical response at 48–72 h. When a study reported both ≥ 20% lesion size reduction and early clinical response, ≥ 20% lesion size reduction was considered as the efficacy outcome for analysis. Documented eradication or presumed eradication of baseline pathogens was considered as ‘microbiological response’.
Assumptions on the study design and patient population
The potential bias due to any heterogeneity in study design and patient characteristics were also investigated and validated by a clinical expert. Populations and study design were deemed to be comparable and unlikely to have an impact on the NMA results. Variation in antibiotic dosing across trials was observed for delafloxacin, telavancin, iclaprim, vancomycin, omadacycline and dalbavancin, however as per the clinical expert opinion the variation in dosing schedules between studies was unlikely to influence the NMA results (Additional file 1: Appendix D). Doses were therefore pooled in the analysis after consultation with two clinical experts. For each study, outcome data from the ITT population were used in the analysis, whereas in the absence of the ITT population for a particular study, data from the population closest to the ITT was used instead (e.g., modified ITT). The analysis population from each RCT is presented in supplementary material Additional file 1: Appendix D.
Network meta-analysis
Bayesian NMA models were used to synthesise the results of included studies as per the NICE guidance [36]. The analyses were based on a burn-in of 80,000 iterations and a further sample of 20,000 iterations until convergence was achieved. The Monte Carlo error was captured, which reflects both the number of simulations and the degree of autocorrelation. This should be no more than 5% of the posterior standard deviation of the parameters of interest. Finally, visual inspection of trace/density plots was carried out. As suggested by the NICE Decision Support Unit TSD 2 a normal distribution with zero mean and variance equal to 104 was used for treatment effects and a uniform distribution with range zero to 5 for the between-trial standard deviation [36]. Vague (flat/uninformative) priors were used for all calculations. The analyses were conducted using JAGS (version 4.3.0) with RStudio (version 3.5.1) as the front end. The analyses consisted of binary outcomes. A binomial model with a logit link function was employed for all outcomes based on NICE guidance [36]. Both fixed effects and random effects models were run to test the model fit and assess heterogeneity. Given that the fixed effect models provided better fit than the random effect models in all analyses and the limited information to estimate between-study variance in the random effect models in some analyses, only results for the fixed effects models are discussed in the main body of the paper. Model fit statistics and results from the random effect models are presented in Additional file 1: Appendix E and Appendix F, respectively. Inconsistency, that is, the lack of agreement between direct and indirect evidence in an NMA, was assessed for each loop in the networks. Inconsistency was assessed by the inconsistency model, as described in the NICE Decision Support Unit TSD 4 [37].
For each outcome, an odds ratio (OR) was used to reflect the relative treatment effects between interventions. Forest plots were presented using the posterior median of OR for each pairwise treatment comparison. The 2.5th and 97.5th percentiles to capture the 95% credible interval (CrI) of corresponding ORs were also provided along with the posterior median. For all outcomes a median OR > 1 indicates favourable results for delafloxacin.
Results
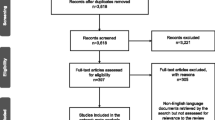
The SLR search identified 2212 studies after removing duplicates. Following the abstract screening, 1985 studies were excluded as they did not meet the eligibility criteria and 227 publications were assessed for full text review. Out of these, 48 primary studies from 79 publications were considered for the NMA feasibility assessment. Nine primary studies were excluded as they did not form a connection in the networks. Two oritavancin phase III RCTs were excluded from the NMA, as the study population in these two studies included a lower proportion of elderly and obese patients than the pivotal RCT on delafloxacin [38, 39]. Overall, 37 primary RCTs were included in the NMA following full text screening and feasibility assessment (Fig. 1). The results of the quality assessment for included RCTs suggested an overall low or moderate risk of bias. A high risk of bias was observed in terms of blinding for seven open label RCTs [40,41,42,43,44,45,46]. Evidence networks were established for the overall study population (outcomes: composite clinical response, early clinical response, and microbiological response), patients with obesity (outcome: composite clinical response) and patients with MRSA (outcomes: composite clinical response and microbiological response). The evidence network for patients with obesity (outcomes: early clinical response and microbiological response) and patients with MRSA (outcome: early clinical response) could not be established due to the limited number of studies reporting outcomes for these subgroups.

PRISMA flow chart. NMA network metanalysis, SLR systematic literature review
An assessment of the degree of between-study heterogeneity was conducted and was validated with two clinical experts by examining differences across studies eligible for inclusion in the NMA. Potential effect modifiers were generally similar across the included studies, and where variability across studies was noted (e.g., proportion of MSSA patients, proportion of MRSA patients, mean treatment duration, proportion of patients with comorbidities), they were further discussed and validated with clinical experts. The potential sources of heterogeneity are presented in Additional file 1: Appendix C. The outcome of the feasibility was that the studies were generally comparable with a low risk of bias from treatment effect modifiers. Based on feedback from the two clinical experts, and given that no considerable evidence of heterogeneity was found (as evidenced from the better fit of the fixed effect models over the random effect models), two sensitivity analyses were also conducted to assess the impact of the populations considered and three ‘outlier studies’ identified. The first sensitivity analysis included only studies which reported outcomes in the ITT (or mITT) population, and the second removed three studies (Wilcox et al. 2009 [42], Sharpe et al. 2005 [46] and Pushker et al. [47]) from the evidence networks, which were deemed to potentially introduce bias due to their small sample sizes and differences in baseline patient characteristics compared to the other included studies.
Inconsistency was tested in the evidence networks for “all patients: composite clinical response” and “all patients: microbiological response”, as these two networks had closed loops (between delafloxacin, vancomycin, vancomycin + aztreonam, ceftaroline and tigecycline in the first network and between delafloxacin, vancomycin, vancomycin + aztreonam, ceftaroline in the second). No evidence of inconsistency in either network was found. Results from the inconsistency assessment are presented in Additional file 1: Appendix G.
Across the 37 RCTs in the evidence networks, efficacy outcomes were included from 18 interventions, of which vancomycin and linezolid were the most common interventions (Additional file 1: Appendix D). Two studies considered the use of either an anti-staphylococcal penicillin (including activity against MRSA) or vancomycin as ‘Standard therapy’ (ST) [48, 49].
All patients
Composite clinical response
The network of evidence for composite clinical response consisted of 34 studies, reporting estimates for 18 interventions (Fig. 2). The results were in favour of delafloxacin in comparison to ceftobiprole, fusidic acid, iclaprim and vancomycin. Results for amoxicillin/clavulanate, ampicillin/sulbactam, ceftaroline fosamil, dalbavancin, daptomycin, delafloxacin, linezolid, omadacycline, oxacillin + dicloxacillin, ST (i.e. anti-staphylococcal penicillin or vancomycin), tedizolid, telavancin, tigecycline, vancomycin + aztreonam and vancomycin + linezolid were comparable to delafloxacin. The forest plot of median ORs and associated 95% CrIs for delafloxacin versus all comparators is presented in Fig. 3.

Network of evidence for all patients: composite clinical response. ASAC ampicillin/sulbactam or amoxicillin/clavulanate, CEF ceftaroline, CEFT ceftobiprole, DAL dalbavancin, DAP daptomycin, DEL delafloxacin, FUS fusidic acid, ICL iclaprim, LIN linezolid, OD oxacillin + dicloxacillin, OMA omadacycline, ST standard therapy, TED tedizolid, TEL telavancin, TIG tigecycline, VA vancomycin + aztreonam, VAN vancomycin, VL vancomycin + linezolid

Forest plot for all patients: composite clinical response. ASAC ampicillin/sulbactam or amoxicillin/clavulanate, CEF ceftaroline, CEFT ceftobiprole, DAL dalbavancin, DAP daptomycin, DEL delafloxacin, FUS fusidic acid, ICL iclaprim, LIN linezolid, OD oxacillin + dicloxacillin, OMA omadacycline, ST standard therapy, TED tedizolid, TEL telavancin, TIG tigecycline, VA vancomycin + aztreonam, VAN vancomycin, VL vancomycin + linezolid
Early clinical response
In terms of early clinical response, delafloxacin was comparable to dalbavancin, daptomycin, fusidic acid, iclaprim, linezolid, omadacycline, tedizolid, vancomycin, vancomycin + aztreonam and vancomycin + linezolid. The network of evidence and the forest plot of median ORs and associated 95% CrIs for early clinical response are presented in Additional file 1: Appendix H and Fig. 4, respectively.

Forest plot for all patients: early clinical response. DAL dalbavancin, DAP daptomycin, DEL delafloxacin, FUS fusidic acid, ICL iclaprim, LIN linezolid, OMA omadacycline, TED tedizolid, VA vancomycin + aztreonam, VAN vancomycin, VL vancomycin + linezolid
Microbiological response
For microbiological response, delafloxacin was comparable to all interventions i.e. ampicillin/sulbactam, amoxicillin/clavulanate, ceftaroline, ceftobiprole, dalbavancin, linezolid, oxacillin + dicloxacillin, tigecycline, vancomycin + aztreonam, and vancomycin. The median ORs and associated 95% CrIs for microbiological response are presented in Fig. 5 and the network of evidence is presented in Additional file 1: Appendix I.

Forest plot for all patients: microbiological response. ASAC ampicillin/sulbactam or amoxicillin/clavulanate, CEF ceftaroline fosamil, CEFT ceftobiprole, DAL dalbavancin, DEL delafloxacin, LIN linezolid, OD oxacillin + dicloxacillin, TIG tigecycline, VA vancomycin + aztreonam, VAN vancomycin
Obese patients (BMI ≥ 30 kg/m2)
Composite clinical response
Results for composite clinical response in obese patients favoured delafloxacin in comparison to vancomycin. However, the results for delafloxacin, linezolid and vancomycin + aztreonam were comparable. The forest plot of median ORs and associated 95% CrIs in obese patients is presented in Fig. 6, and the network of evidence is presented in Additional file 1: Appendix J.

Forest plot for obese subpopulation: composite clinical response. DEL delafloxacin, Lin linezolid, VA vancomycin + aztreonam, VAN vancomycin
Additional subgroup: patients with MRSA infection
The network of evidence for patients with MRSA infection consisted of 18 studies, reporting estimates for ten interventions. For composite clinical response, delafloxacin was found to be comparable to all interventions in the network, namely, ampicillin/sulbactam, amoxicillin/clavulanate, ceftobiprole, ceftaroline, linezolid, omadacycline, tigecycline, vancomycin + aztreonam and vancomycin (Additional file 1: Appendix K). Similarly, for microbiological response, delafloxacin was found to be comparable to ceftaroline, dalbavancin, linezolid, tedizolid, tigecycline, vancomycin + aztreonam and vancomycin (Additional file 1: Appendix L).
Sensitivity analyses
Sensitivity analyses for ITT/mITT population
Evidence networks were established for the overall population for composite clinical response and early clinical response. Delafloxacin was superior in terms of composite clinical response in comparisons with fusidic acid, iclaprim, vancomycin, and ceftobiprole, whilst with other active comparators results were comparable with delafloxacin. In early clinical response the results were comparable for delafloxacin versus fusidic acid, vancomycin, iclaprim, omadacycline, linezolid, tedizolid, and vancomycin + aztreonam.
Sensitivity analyses after removing outlier studies
Evidence networks were established for the overall population for composite clinical response and microbiological response. For composite clinical response, in comparisons of delafloxacin with fusidic acid, iclaprim, vancomycin, ceftobiprole, and telavancin, the results favoured delafloxacin. For the comparisons of delafloxacin with the remaining treatments, the results were comparable between delafloxacin and the comparator treatments.
For microbiological response, the results were comparable for delafloxacin versus ampicillin + sulbactam or amoxycillin + clavulanate, ceftobiprole, dalbavancin, linezolid, oxacillin + dicloxacillin, tigecycline, vancomycin, ceftaroline and vancomycin + aztreonam.
Discussion
Delafloxacin is a fluoroquinolone with broad spectrum activity against gram-positive pathogens, including MRSA and many gram-negative pathogens [30, 50]. This NMA included RCTs involving adult patients with ABSSSI, cSSSI, cSSTI or severe cellulitis and comprehensively evaluated the relative clinical efficacy of delafloxacin versus interventions used to treat patients with complicated and ABSSSI. In comparison to previously published NMAs, this NMA included a broader range of infections such as ABSSSI, cSSSIs, cSSTI or severe cellulitis, together with a wider array of interventions [32, 33].
The NMA found that, for composite clinical response in the overall patient population, the results were in favour of delafloxacin when compared to ceftobiprole, fusidic acid, iclaprim, and vancomycin. For early clinical response, the results were comparable for delafloxacin versus dalbavancin, daptomycin, fusidic acid, iclaprim, linezolid, omadacycline, tedizolid, vancomycin, vancomycin + aztreonam and vancomycin + linezolid. For microbiological response, delafloxacin showed comparable effectiveness with ampicillin/sulbactam, amoxicillin/clavulanate, ceftaroline, ceftobiprole, dalbavancin, linezolid, oxacillin + dicloxacillin, tigecycline, vancomycin + aztreonam, and vancomycin. The relative clinical efficacy of delafloxacin versus other treatments in obese patients demonstrated consistency with the results of composite clinical response in the overall population, as delafloxacin showed greater improvement in comparison to vancomycin, and comparable results with linezolid and vancomycin + aztreonam. Furthermore, delafloxacin showed comparable results with other included interventions in terms of composite clinical and microbiological response for MRSA patients. The sensitivity analysis including only trials reporting outcomes for the ITT/mITT populations and removing the three outlier studies identified by clinical experts were comparable to the base case analysis.
Across all analysed populations, particularly for the MRSA subpopulation, median OR estimates for several treatment comparisons were associated with considerable uncertainty, depicted by wide CrIs. This uncertainty can be attributed to the availability of data from a limited number of studies and heterogeneity in study populations. Therefore, robust conclusions cannot be derived for the MRSA subgroup analysis. It should be noted that as majority of the identified studies were not carried out exclusively in the MRSA population, these studies were not specifically designed or powered to detect differences in the subgroups. Furthermore, the proportion of patients with MRSA also varied across RCTs, which reflects the inherent heterogeneity between the included trials.
Our findings are consistent with a previous NMA involving four RCTs by Lan et al., in which delafloxacin exhibited clinical cure rate similar to other comparator drugs (OR: 1.05; 95% CI: 0.87 to 1.27; I2 = 16%) in the treatment of ABSSSI [32]. Although, Lan et al. included an adult population with ABSSSI that was limited to delafloxacin RCTs, thereby comparing delafloxacin to just four comparators i.e. tigecycline, vancomycin, linezolid and vancomycin + aztreonam [32]. In another NMA which included ten RCTs, the indirect comparison of delafloxacin showed similar efficacy in terms of clinical cure with ceftaroline (OR: 0.82; 95% CrI: 0.39 to 1.8), ceftobiprole (OR: 0.79; 95% CrI: 0.32 to 1.9) and tigecycline (OR: 1.0: 95% CrI: 0.45 to 2.2) [33]. However, the analysis was restricted to the MRSA ABSSSI population and compared the efficacy of delafloxacin with just ceftaroline, ceftobiprole and tigecycline [33].
The present NMA encompassed 37 RCTs which included adult patients with a wide range of severe skin and skin structure infections. It evaluated the comparative effectiveness of delafloxacin versus 18 interventions in terms of composite clinical response, early clinical response and microbiological response. This NMA also evaluated the efficacy of delafloxacin with relevant comparators for obese patients, which to our knowledge has not been evaluated in previously published NMAs [32, 33]. In the present NMA, an assessment of the risk of bias was undertaken for each identified RCT and the variability across studies was validated by the clinical expert.
This study is subject to the limitations inherent to all NMAs in terms of heterogeneity of included studies [51]. The included RCTs were conducted in populations that were categorised by different definitions of infections (ABSSSI, cSSSI, cSSTI, severe cellulitis) and outcomes. This could lead to potential bias in the results. However, the assessment of inconsistency in the NMA did not suggest any discrepancy in the evidence. In addition, the studies included in the NMA were published over a time span extending two decades (2000–2019). A number of the included studies were conducted before the publication of the FDA guidance for the design of RCTs to evaluate drugs for ABSSSI [5], justifying the variability in the definition of infections. The RCTs assessing ceftaroline [52,53,54] and one of the RCTs assessing delafloxacin [55] considered patients with cSSSI whereas three RCTs for delafloxacin included patients with ABSSSI [30, 31, 56]. Moreover, different dosing regimens were used in RCTs assessing ceftaroline, dalbavancin, daptomycin, delafloxacin, linezolid, omadacycline, and telavancin. To facilitate the NMA, different doses of treatments were pooled for each study. However, the clinical expert validated that the treatment doses and infection subtypes across RCTs were comparable, therefore, these differences are unlikely to introduce bias in the results.
This study provides substantial indirect evidence for the comparative efficacy of delafloxacin versus a broad range of comparators for the management of ABSSSI. Further research is warranted for the comparative efficacy of delafloxacin involving RCTs powered to detect differences in populations with obesity and MRSA infections.
Conclusion
The results of this NMA substantiate that delafloxacin is an effective new antibiotic for ABSSSI. Delafloxacin demonstrated improved composite clinical response versus ceftobiprole, fusidic acid, iclaprim and vancomycin in base case analysis, and with telavancin in the scenario analysis. For the remaining comparators in composite clinical response, in addition to all interventions included in the early response and microbiological response analysis, delafloxacin was equivalent. The results favoured delafloxacin in comparison to vancomycin for composite clinical response in obese patients. Finally, the NMA showed that delafloxacin has comparable efficacy to all interventions in the MRSA subgroup. Delafloxacin, with a broad spectrum activity against MRSA and gram-negative bacteria, is a promising addition to the standard of care for patients with ABSSSI.
Availability of data and materials
All data sets are provided in Additional file 1
Abbreviations
- ABSSSI:
-
Acute bacterial skin and skin structure infections
- BMI:
-
Body mass index
- Crl:
-
Credible interval
- cSSSI:
-
Complicated skin and skin structure infections
- cSSTI:
-
Complicated skin and soft tissue infections
- EARS:
-
European Antimicrobial Resistance Surveillance
- ECDC:
-
European Centre for Disease prevention and Control
- FDA:
-
Food and Drug Administration
- IDSA:
-
Infectious Disease Society of America
- IV:
-
Intravenous
- ITT:
-
Intention-to-treat
- MRSA:
-
Methicillin-resistant Staphylococcus aureus
- MSSA:
-
Methicillin-sensitive Staphylococcus aureus
- NICE:
-
National Institute for Health and Care Excellence
- NMA:
-
Network meta-analysis
- OR:
-
Odds ratio
- RCT:
-
Randomised controlled trials
- SLR:
-
Systematic literature reviews
- SSSI:
-
Skin and skin structure infections
- ST:
-
Standard therapy
- TOC:
-
Test of cure
- US:
-
United States
References
Dryden MS. Complicated skin and soft tissue infection. J Antimicrob Chemother. 2010;65(suppl_3):iii35–44. https://doi.org/10.1093/jac/dkq302.
Miller LG, Eisenberg DF, Liu H, Chang C-L, Wang Y, Luthra R, et al. Incidence of skin and soft tissue infections in ambulatory and inpatient settings, 2005–2010. BMC Infect Dis. 2015;15(1):362. https://doi.org/10.1186/s12879-015-1071-0.
Lee GC, Boyd NK, Lawson KA, Frei CR. Incidence and cost of skin and soft tissue infections in the United States. Value Health. 2015;18(3):A245. https://doi.org/10.1016/j.jval.2015.03.1424.
Pollack CV Jr, Amin A, Ford WT Jr, Finley R, Kaye KS, Nguyen HH, et al. Acute bacterial skin and skin structure infections (ABSSSI): practice guidelines for management and care transitions in the emergency department and hospital. J Emerg Med. 2015;48(4):508–19. https://doi.org/10.1016/j.jemermed.2014.12.001.
USFDA. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER)Guidance for Industry. Acute Bacterial Skin and Skin Structure Infections: Developing Drugs for Treatment 2013, https://www.fda.gov/files/drugs/published/Acute-Bacterial-Skin-and-Skin-Structure-Infections---Developing-Drugs-for-Treatment.pdf. Accessed 19 Aug 2020.
Stevens DL, Bisno AL, Chambers HF, Dellinger EP, Goldstein EJ, Gorbach SL, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10-52. https://doi.org/10.1093/cid/ciu444.
Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603. https://doi.org/10.1128/CMR.00134-14.
Livermore DM, Mushtaq S, Warner M, James D, Kearns A, Woodford N. Pathogens of skin and skin-structure infections in the UK and their susceptibility to antibiotics, including ceftaroline. J Antimicrob Chemother. 2015;70(10):2844–53. https://doi.org/10.1093/jac/dkv179.
ECDC. European Centre for Disease Prevention and Control (ECDC); Annual report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) 2018, https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2018. Accessed 9 Aug 2020.
CDC. Centre for Disease Control and Prevention; Antibiotic Resistance Threats Report, https://www.cdc.gov/drugresistance/biggest-threats.html (2019).
Klein EY, Mojica N, Jiang W, Cosgrove SE, Septimus E, Morgan DJ, et al. Trends in methicillin-resistant Staphylococcus aureus hospitalizations in the United States, 2010–2014. Clin Infect Dis. 2017;65(11):1921–3. https://doi.org/10.1093/cid/cix640.
Kourtis AP, Hatfield K, Baggs J, Mu Y, See I, Epson E, et al. Vital signs: epidemiology and recent trends in methicillin-resistant and in methicillin-susceptible Staphylococcus aureus bloodstream infections - United States. MMWR Morb Mortal Wkly Rep. 2019;68(9):214–9. https://doi.org/10.15585/mmwr.mm6809e1.
Golan Y. Current treatment options for acute skin and skin-structure infections. Clin Infect Dis. 2019;68(Suppl 3):S206–12. https://doi.org/10.1093/cid/ciz004.
Jeffres MN. The whole price of vancomycin: toxicities, troughs, and time. Drugs. 2017;77(11):1143–54. https://doi.org/10.1007/s40265-017-0764-7.
Forouzesh A, Moise PA, Sakoulas G. Vancomycin ototoxicity: a reevaluation in an era of increasing doses. Antimicrob Agents Chemother. 2009;53(2):483–6. https://doi.org/10.1128/AAC.01088-08.
Kupstaite R, Baranauskaite A, Pileckyte M, Sveikata A, Kadusevicius E, Muckiene G. Severe vancomycin-induced anaphylactic reaction. Medicina (Kaunas). 2010;46(1):30–3.
Alvarez-Arango S, Yerneni S, Tang O, Zhou L, Mancini CM, Blackley SV, et al. Vancomycin hypersensitivity reactions documented in electronic health records. J Allergy Clin Immunol Pract. 2021;9(2):906–12. https://doi.org/10.1016/j.jaip.2020.09.027.
Frampton JE. Ceftaroline fosamil: a review of its use in the treatment of complicated skin and soft tissue infections and community-acquired pneumonia. Drugs. 2013;73(10):1067–94. https://doi.org/10.1007/s40265-013-0075-6.
Russo A, Concia E, Cristini F, De Rosa FG, Esposito S, Menichetti F, et al. Current and future trends in antibiotic therapy of acute bacterial skin and skin-structure infections. Clin Microbiol Infect. 2016;22(Suppl 2):S27-36. https://doi.org/10.1016/s1198-743x(16)30095-7.
Allergan. USA, Inc, DALVANCE (dalbavancin) Prescribing information 2018, https://media.allergan.com/actavis/actavis/media/allergan-pdf-documents/product-prescribing/Dalvance_Final_PI_10_2018.pdf. Accessed 05 Oct 2020.
EMA. Orbactiv; EPAR; Summary of Product Characteristics; European Medicines Agency, https://www.ema.europa.eu/en/documents/overview/orbactiv-epar-summary-public_en.pdf (2015).
MSD. Merck Sharp & Dohme Corp, SIVEXTRO (tedizolid phosphate) https://www.merck.com/product/usa/pi_circulars/s/sivextro/sivextro_pi.pdf. Accessed 05 Oct 2020.
WHO. World Health Organization, Antimicrobial resistance: global report on surveillance 2014, https://www.who.int/antimicrobial-resistance/publications/surveillancereport/en/. Accessed 05 Oct 2020.
Ayyagari R, Revol C, Tang W, Faust E, Tuttle EG. Association of Obesity with 30-day readmission rates among patients Hospitalized with Acute Bacterial Skin and Skin-Structure Infections (ABSSSI). Value in Health. 2015;18(3):A186. https://doi.org/10.1016/j.jval.2015.03.1073.
Pulido-Cejudo A, Guzmán-Gutierrez M, Jalife-Montaño A, Ortiz-Covarrubias A, Martínez-Ordaz JL, Noyola-Villalobos HF, et al. Management of acute bacterial skin and skin structure infections with a focus on patients at high risk of treatment failure. Therap Adv Infect Dis. 2017;4(5):143–61. https://doi.org/10.1177/2049936117723228.
WHO. Obesity and overweight; World Health Organization, https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (2016).
Jorgensen SCJ, Mercuro NJ, Davis SL, Rybak MJ. Delafloxacin: place in therapy and review of microbiologic, clinical and pharmacologic properties. Infect Dis Ther. 2018;7(2):197–217. https://doi.org/10.1007/s40121-018-0198-x.
Lodise TP, Fan W, Sulham KA. Economic impact of oritavancin for the treatment of acute bacterial skin and skin structure infections in the emergency department or observation setting: cost savings associated with avoidable hospitalizations. Clin Ther. 2016;38(1):136–48. https://doi.org/10.1016/j.clinthera.2015.11.014.
EMA. European Medicines Agency; Quofenix (delafloxacin), https://www.ema.europa.eu/en/documents/overview/quofenix-epar-medicine-overview_en.pdf. Accessed 05 Oct 2020.
O’Riordan W, McManus A, Teras J, Poromanski I, Cruz-Saldariagga M, Quintas M, et al. A comparison of the efficacy and safety of intravenous followed by oral delafloxacin with vancomycin plus aztreonam for the treatment of acute bacterial skin and skin structure infections: a phase 3, multinational, double-blind. Randomized Study. Clin Infect Dis. 2018;67(5):657–66. https://doi.org/10.1093/cid/ciy165.
Pullman J, Gardovskis J, Farley B, Sun E, Quintas M, Lawrence L, et al. Efficacy and safety of delafloxacin compared with vancomycin plus aztreonam for acute bacterial skin and skin structure infections: a Phase 3, double-blind, randomized study. J Antimicrob Chemother. 2017;72(12):3471–80. https://doi.org/10.1093/jac/dkx329.
Lan SH, Lai CC, Lu LC, Chang SP, Huang HT. Efficacy and safety of delafloxacin in the treatment of acute bacterial skin and skin structure infections: a systematic review and meta-analysis of randomized controlled trials. Infect Drug Resist. 2019;12:1415–23. https://doi.org/10.2147/idr.S202160.
Alhifany AA, Bifari N, Alatawi Y, Ullah Malik S, Almangour T. 465. Comparative efficacy of double vs. single antibiotic regimens for the empiric treatment of MRSA-induced acute bacterial skin and skin structure infection. Open Forum Infect Dis. 2019;6(2):S227–8. https://doi.org/10.1093/ofid/ofz360.538.
Julian PT Higgins SG. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.02011.
Higgins JPT AD. Assessing risk of bias in included studies, In: Higgins JPT, Green S, eds. Cochrane handbook for systematic reviews of interventions. Chichester (UK): Wiley; 2008.
Sofia Dias NJW, Alex J Sutton, and AE Ades. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials2014.
Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE Decision Support Unit Technical Support Documents. NICE DSU Technical Support Document 4: Inconsistency in Networks of Evidence Based on Randomised Controlled Trials. London: National Institute for Health and Care Excellence (NICE) Copyright © 2014 National Institute for Health and Clinical Excellence, unless otherwise stated. All rights reserved.; 2014.
Corey GR, Kabler H, Mehra P, Gupta S, Overcash JS, Porwal A, et al. Single-Dose Oritavancin in the Treatment of Acute Bacterial Skin Infections. 2014;370(23):2180–90. https://doi.org/10.1056/NEJMoa1310422.
Corey GR, Good S, Jiang H, Moeck G, Wikler M, Green S, et al. Single-dose oritavancin versus 7–10 days of vancomycin in the treatment of gram-positive acute bacterial skin and skin structure infections: the SOLO II noninferiority study. Clin Infect Dis. 2015;60(2):254–62. https://doi.org/10.1093/cid/ciu778.
Matthews P, Alpert M, Rahav G, Rill D, Zito E, Gardiner D, et al. A randomized trial of tigecycline versus ampicillin-sulbactam or amoxicillin-clavulanate for the treatment of complicated skin and skin structure infections. BMC Infect Dis. 2012;12:297. https://doi.org/10.1186/1471-2334-12-297.
Noel GJ, Draper MP, Hait H, Tanaka SK, Arbeit RD. A randomized, evaluator-blind, phase 2 study comparing the safety and efficacy of omadacycline to those of linezolid for treatment of complicated skin and skin structure infections. Antimicrob Agents Chemother. 2012;56(11):5650–4. https://doi.org/10.1128/aac.00948-12.
Wilcox MH, Tack KJ, Bouza E, Herr DL, Ruf BR, Ijzerman MM, et al. Complicated skin and skin-structure infections and catheter-related bloodstream infections: noninferiority of linezolid in a phase 3 study. Clin Infect Dis. 2009;48(2):203–12. https://doi.org/10.1086/595686.
Weigelt J, Itani K, Stevens D, Lau W, Dryden M, Knirsch C. Linezolid versus vancomycin in treatment of complicated skin and soft tissue infections. Antimicrob Agents Chemother. 2005;49(6):2260–6. https://doi.org/10.1128/aac.49.6.2260-2266.2005.
Itani KM, Dryden MS, Bhattacharyya H, Kunkel MJ, Baruch AM, Weigelt JA. Efficacy and safety of linezolid versus vancomycin for the treatment of complicated skin and soft-tissue infections proven to be caused by methicillin-resistant Staphylococcus aureus. Am J Surg. 2010;199(6):804–16. https://doi.org/10.1016/j.amjsurg.2009.08.045.
Kauf TL, McKinnon P, Corey GR, Bedolla J, Riska PF, Sims M, et al. An open-label, pragmatic, randomized controlled clinical trial to evaluate the comparative effectiveness of daptomycin versus vancomycin for the treatment of complicated skin and skin structure infection. BMC Infect Dis. 2015;15:503. https://doi.org/10.1186/s12879-015-1261-9.
Sharpe JN, Shively EH, Polk HC Jr. Clinical and economic outcomes of oral linezolid versus intravenous vancomycin in the treatment of MRSA-complicated, lower-extremity skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus. Am J Surg. 2005;189(4):425–8. https://doi.org/10.1016/j.amjsurg.2005.01.011.
Pushker N, Tejwani LK, Bajaj MS, Khurana S, Velpandian T, Chandra M. Role of oral corticosteroids in orbital cellulitis. Am J Ophthalmol. 2013;156(1):178-83.e1. https://doi.org/10.1016/j.ajo.2013.01.031.
Stryjewski ME, O’Riordan WD, Lau WK, Pien FD, Dunbar LM, Vallee M, et al. Telavancin versus standard therapy for treatment of complicated skin and soft-tissue infections due to gram-positive bacteria. Clin Infect Dis. 2005;40(11):1601–7. https://doi.org/10.1086/429914.
Stryjewski ME, Chu VH, O’Riordan WD, Warren BL, Dunbar LM, Young DM, et al. Telavancin versus standard therapy for treatment of complicated skin and skin structure infections caused by gram-positive bacteria: FAST 2 study. Antimicrob Agents Chemother. 2006;50(3):862–7. https://doi.org/10.1128/aac.50.3.862-867.2006.
McCurdy S, Lawrence L, Quintas M, Woosley L, Flamm R, Tseng C, et al. In vitro activity of delafloxacin and microbiological response against fluoroquinolone-susceptible and nonsusceptible staphylococcus aureus isolates from two phase 3 studies of acute bacterial skin and skin structure infections. Antimicrob Agents Chemother. 2017;61:9. https://doi.org/10.1128/aac.00772-17.
Cipriani A, Higgins JPT, Geddes JR, Salanti G. Conceptual and technical challenges in network meta-analysis. Ann Intern Med. 2013;159(2):130–7. https://doi.org/10.7326/0003-4819-159-2-201307160-00008.
Corey GR, Wilcox MH, Talbot GH, Thye D, Friedland D, Baculik T. CANVAS 1: the first Phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J Antimicrob Chemother. 2010;65(Suppl 4):41–51. https://doi.org/10.1093/jac/dkq254.
Wilcox MH, Corey GR, Talbot GH, Thye D, Friedland D, Baculik T. CANVAS 2: the second Phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J Antimicrob Chemother. 2010;65(Suppl 4):iv53–65. https://doi.org/10.1093/jac/dkq255.
Talbot GH, Thye D, Das A, Ge Y. Phase 2 study of ceftaroline versus standard therapy in treatment of complicated skin and skin structure infections. Antimicrob Agents Chemother. 2007;51(10):3612–6. https://doi.org/10.1128/aac.00590-07.
O’Riordan W, Mehra P, Manos P, Kingsley J, Lawrence L, Cammarata S. A randomized phase 2 study comparing two doses of delafloxacin with tigecycline in adults with complicated skin and skin-structure infections. Int J Infect Dis. 2015;30:67–73. https://doi.org/10.1016/j.ijid.2014.10.009.
Kingsley J, Mehra P, Lawrence LE, Henry E, Duffy E, Cammarata SK, et al. A randomized, double-blind, Phase 2 study to evaluate subjective and objective outcomes in patients with acute bacterial skin and skin structure infections treated with delafloxacin, linezolid or vancomycin. J Antimicrob Chemother. 2016;71(3):821–9. https://doi.org/10.1093/jac/dkv411.
Acknowledgements
The authors would like to thank Paranjoy Saharia and Vibha Dhamija from IQVIA for their medical writing and editing support.
Funding
Funding for this study was provided by Menarini I.F.R.
Author information
Authors and Affiliations
Contributions
All authors (EF, TM, YJ, IV, MV, DZ, DN) were involved in the design of the work as well as the analysis and interpretation of the data. EF, TM and YJ conducted the study analysis and validation. All authors (EF, TM, YJ, IV, MV, DZ, DN) reviewed and revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval and patient consent was not required as the study is a meta-analysis based on published studies.
Consent for publication
All authors have given their consent to publishing this work.
Competing interests
MV, IV and DZ are full time employees of Menarini group. YJ, EF and TM received consulting fees from Menarini. DN supported the study as the clinical expert and received personal fee from Menarini for his support in the present study. DN has also received honoraria from Menarini outside the submitted work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Appendices.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Vlachaki, I., Vacchelli, M., Zinzi, D. et al. Comparative efficacy of delafloxacin for complicated and acute bacterial skin and skin structure infections: results from a network meta-analysis. BMC Infect Dis 21, 1036 (2021). https://doi.org/10.1186/s12879-021-06736-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-021-06736-x