
Abstract
Background
Rat bite fever (RBF) is a rare systemic febrile illness transmitted by rats. Streptobacillus moniliformis is a pleomorphic Gram-negative bacillus which is the usual etiologic organism for rat bite fever in the United States.
Case presentation
Here we present a case of rat bite fever complicated by vertebral osteomyelitis and discitis. The patient revealed an exposure history of being bitten by pet rats. The patient’s symptoms dramatically improved with a six-week course of cephalexin therapy.
Conclusions
It is important to obtain a thorough zoonotic exposure history and maintain rat bite fever in the differential when considering potential causes of discitis and osteomyelitis.
Similar content being viewed by others


Background
Rat bite fever (RBF) is an uncommon systemic febrile illness transmitted by rats. Streptobacillus moniliformis is a pleomorphic Gram-negative bacillus which is the usual etiologic organism for RBF in the United States. Osteomyelitis and discitis have very rarely been reported in association with RBF.
Case presentation
A 55-year old male presented to an academic medical center in February 2020 with a six-week history of increasing midline back pain. He had a history of chronic mid- and lower back pain as the result of degenerative disc disease, however his pain had abruptly worsened in the 6 weeks prior to presentation. Pain was worsened with trying to sit up straight or walk. Pain was partially relieved with acetaminophen, ibuprofen, and oxycodone 5 mg tablets taken as needed. He reported no associated fevers, chills, or night sweats. He did not recall a febrile illness prior to the onset of symptoms. He did report anorexia and 15-pound weight loss in the last 6 weeks. His medical history included chronic obstructive pulmonary disease, chronic hepatitis C infection, hyperlipidemia, generalized anxiety disorder, and lumbar degenerative disc disease. His surgical history was notable for cervical spine laminectomy in the remote past. His social history was notable for heavy and ongoing tobacco use with a 60 pack-year smoking history. He denied alcohol or illicit drug use including intravenous drug use.
He was afebrile and hemodynamically stable on presentation. Physical exam revealed a gaunt Caucasian male in moderate distress due to pain. Poor dentition was noted. His cardiopulmonary examination was unremarkable. On spinal examination, no bony tenderness was elicited upon palpation of the thoracic and lumbar spine, however paraspinal tenderness was noted in the lumbar spine. Neurologic examination including strength and sensation of the lower extremities was intact. Babinski reflex was downward bilaterally.
MRI with and without gadolinium contrast revealed abnormal enhancement of the lower endplate of the L2 vertebral body as well as diffuse enhancement of the L3 vertebral body with irregularity of the upper endplate. This abnormal enhancement extended to the intervertebral disc. Findings were suggestive of discitis with osteomyelitis not excluded. Additionally, there was enhancement and thickening in the anterior epidural space measuring 2 mm × 4 mm which may represent epidural abscess or hematoma (Fig. 1). Laboratory evaluation including CBC with differential and comprehensive metabolic panel was unremarkable. Sedimentation rate was 36 mm/hr. and C-reactive protein was 30.1 mg/L. Blood cultures were sterile.

MR lumbar spine with contrast, T1WFS: There is abnormal enhancement of the lower endplate of L2 vertebral body and there is diffuse enhancement of most of L3 vertebral body with irregularity of the upper endplate. The abnormal enhancement slightly extends into the intervertebral disc. There is a thickening in the anterior epidural space and the central and right paracentral region at L2–3 level with a possibility of a tiny pocket of nonenhancement within the enhancing anterior epidural space measures about 2 × 4 mm which could represent a small epidural abscess or hematoma from the recent trauma
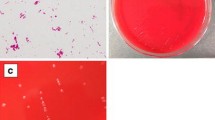
Based on initial results of clinical, laboratory, and radiographic evaluation, antibiotic therapy was withheld. CT-guided aspiration of the L2-L3 disc was performed for culture and histopathology. Gram stain revealed Gram variable rods. Histopathology revealed fibrocartilage with degenerative changes and acute inflammation suggestive of discitis (Fig. 2). He was seen in Infectious Diseases outpatient consultation, initially offered intravenous antibiotic therapy however patient requested oral antibiotic therapy for empiric treatment of discitis. He was started on treatment with cephalexin 1 g by mouth three times a day as well as linezolid 600 mg by mouth twice a day. (Initially, prior to the revelation of RBF infection, linezolid was chosen (in addition to cephalexin) because Gram stain revealed Gram-positive rods. The intention was to cover Corynebacterium spp. and coagulase-negative staphylococci, skin flora which tend to have resistance to beta-lactams but susceptibility to vancomycin or linezolid.) Cultures were sent to a reference laboratory, with growth noted on Mueller-Hinton media with 5% sheep blood. The organism was identified as Streptobacillus moniliformis by matrix-assisted laser desorption ionization time-of-flight mass spectroscopy (MALDI-TOF). On further history, it was revealed that patient had two pet rats and had sustained numerous bites in the last 1 year prior to symptom onset. In vitro susceptibility testing using broth microdilution revealed low MIC for penicillin (< 0.06 μg/ml), ampicillin (< 0.12 μg/ml), and ceftriaxone (< 0.06 μg/ml), with elevated MIC > 4 μg/mL for gentamicin. The patient’s symptoms dramatically improved with cephalexin so a decision was made not to switch to oral or IV penicillin. Linezolid was discontinued after 2 weeks once culture results were available. He completed 6 weeks of oral cephalexin therapy with dramatic improvement of back pain. The patient was offered TEE to evaluate for endocarditis. However, he declined to have the test done as this coincided with the onset of CoVID-19 pandemic.

H&E stain, vertebral disc fibroelastic cartilage infiltrated by acute inflammation, consistent with discitis
Discussion
Rat bite fever (RBF) caused by Streptobacillus moniliformis is transmitted to humans predominantly through rodent bites and scratches. S. moniliformis has been commonly detected in wild and pet rats [1]. A diverse array of animals has been implicated to harbor, or suffer from, S. moniliformis infections, such as gerbils, squirrels, turkeys, koalas, macaques, dogs, cats, weasels, and ferrets. However, more recent metagenomic data have suggested that streptobacilli in these other rodent species may in fact be separate species altogether [1]. Moreover, novel Streptobacillus species (S. hongkongensis, S. felis) have been recently described in clinical human and veterinary infections [2].
RBF has historically been a disease of poverty. While prior to 2007 only a small minority (5%) of RBF cases had known pet rat exposure, since 2010 most cases of RBF have been linked to pet rats [3, 4]. This trend is likely attributable to the increasingly popular practice in the United States of keeping rats as house pets [5]. The actual incidence of rat bite fever is unknown as it is not a mandatory reportable disease [4].
S. moniliformis is a pleomorphic, non-acid-fast, Gram-negative, facultative anaerobe bacillus which tends to grow in long intermittently-beaded filaments. Difficult to grow in culture, S. moniliformis requires specific growth and incubation conditions [3]. Definitive identification is made by MALDI-TOF [1]. In our case, the isolate was sent to ARUP reference laboratory (Salt Lake City, UT), and species identification was made using MALDI-TOF. It must be mentioned that commercial MALDI-TOF databases do not contain spectra of all Streptobacillus species and that it is plausible that MALDI-TOF may not be able to differentiate between S. moniliformis and other Streptobacillus species [1]. Many hospital laboratories do not have the capabilities for accurate detection of the organism, and therefore diagnosis may be delayed [4]. Exposure to rats may often not be clarified from patient history until after S. moniliformis is identified by laboratory testing.
A 2007 review of 65 RBF case reports showed that clinical symptoms are fever (92%), arthralgias (66%), and rash (61%). Nausea and vomiting (40%), headache (34%), and sore throat (17%) were also common. White blood cell count was on average 12.2 103/μL; only 5 patients demonstrated leukocytosis higher than 15 103/μL [3]. Interestingly, these common clinical manifestations were all absent in our patient. (WBC remained under 8 103/μL throughout the patient’s clinical course). It is possible that patient’s history of chronic hepatitis C infection may have blunted the patient’s adaptive and innate immune response to S. moniliformis infection and thereby led to the atypical clinical presentation.
Reported complications associated with RBF are extensive and include meningitis, mastoiditis, interstitial pneumonia, periarteritis nodosa, pancreatitis, pericarditis, myocarditis, hepatitis, prostatitis, septic arthritis, and abscess formation in various organs [4, 6]. Infective endocarditis due to RBF has a particularly poor outcome with mortality rates of 50% [4, 7].
The standard for treatment for S. monoliformis is penicillin G [4]. However, our patient was not switched to penicillin once RBF infection was revealed given his significant clinical improvement with cephalexin.
We performed a literature review for RBF cases with osteomyelitis or discitis. PubMed was searched for the following terms: Spirillum minus, Streptobacillus moniliformis, Haverhillia multiformis, rat bite fever, AND osteomyelitis, discitis. Our literature review uncovered associated with S. moniliformis, only 4 cases of osteomyelitis, 1 of possible osteomyelitis, and 4 of discitis, reported globally [6,7,8,9,10,11,12,13,14]. It is difficult to judge in our case whether the findings on MR imaging represent discitis or rather extension of infection from the L2-L3 endplate. Nonetheless, this is an unusual and rarely reported complication of RBF [13].
Table 1 summarizes nine cases of RBF associated with osteomyelitis or discitis, all reported from developed nations from 2008 through 2019. Ages ranged from 22-months to 80-years, with 4 females and 5 males. In only seven of the nine cases did the patient acknowledge direct exposure to rats. Four kept rats in their home for reasons including having house pets and a reptile food source. Affected joints included the cervical, thoracic, lumbar, sacral vertebrae and intervertebral discs, as well as hip, ankle, and sternoclavicular joints. Two cases required surgical debridement, while six resolved with antibiotic therapy alone (Table 1). A recent analysis of rat bite fever diagnosis in the United States reveals that the majority of encounters occur in persons aged 0–19 years [15]. Our case highlights the need to consider the diagnosis in older adults as well.
This case underscores the importance of obtaining a thorough zoonotic exposure history and maintaining a broad differential that includes RBF when considering potential causes of discitis and osteomyelitis.
Availability of data and materials
Not applicable.
Abbreviations
- RBF:
-
Rat bite fever
- MIC:
-
Minimum inhibitory concentration
- TEE:
-
Transesophageal echocardiography
- MALDI-TOF:
-
Matrix-assisted laser desorption/ionization
References
Eisenberg T, Ewers C, Rau J, Akimkin V, Nicklas W. Approved and novel strategies in diagnostics of rat bite fever and other Streptobacillus infections in humans and animals. Virulence. 2016;7(6):630–48 Cited 2021 Feb 28.
Eisenberg T, Nicklas W, Mauder N, Rau J, Contzen M, Semmler T, et al. Phenotypic and genotypic characteristics of members of the genus Streptobacillus. PLoS One. 2015;10(8) Cited 2021 Feb 28.
Elliott SP. Rat bite fever and Streptobacillus moniliformis. Clin Microbiol Rev. 2007;20(1):13–22. https://doi.org/10.1128/CMR.00016-06.
DuBray KA, Glaser CA. Streptobacillus moniliformis (rat-bite fever). In: Cherry J, Demmler-Harrison GJ, Kaplan SL, Steinbach WJ, Hotez PJ, editors. Feigin and Cherry’s textbook of pediatric infectious diseases. 8th ed. Philadelphia: Elsevier; 2019. Cited 2020 May 23.
Royer N. The history of fancy rats: American Fancy Rat & Mouse Association; 2015. Available from: https://www.afrma.org/historyrat.htm. Cited 2020 May 30
Abusalameh M, Mahankali-Rao P, Earl S. Discitis caused by rat bite fever in a rheumatoid arthritis patient on tocilizumab – first ever case. Rheumatology. 2018;57(6):1118–20 Cited 2020 May 30.
Pena MER, Jordão S, Simões MJ, Oleastro M, Neves I. A rare cause of vertebral osteomyelitis: the first case report of rat-bite fever in Portugal. Rev Soc Bras Med Trop. 2020;53. https://doi.org/10.1590/0037-8682-0328-2019.
Nei T, Sato A, Sonobe K, Miura Y, Takahashi K, Saito R. Streptobacillus moniliformis bacteremia in a rheumatoid arthritis patient without a rat bite: a case report. BMC Res Notes. 2015;8(1):694 Cited 2020 May 30.
Adizie T, Gayed M, Ravindran J. Rat bite fever causing septic arthritis and osteomyelitis in a young man. Rheumatology. 2014;53(suppl_1):i57.
Dubois D, Robin F, Bouvier D, Delmas J, Bonnet R, Lesens O, et al. Streptobacillus moniliformis as the causative agent in spondylodiscitis and psoas abscess after rooster scratches. J Clin Microbiol. 2008;46(8):2820–1. https://doi.org/10.1128/JCM.00744-08.
Akter R, Boland P, Daley P, Rahman P, Al Ghanim N. Rat bite fever resembling rheumatoid arthritis. Can J Infect Dis Med Microbiol. 2016;2016:7270413.
Sato R, Kuriyama A, Nasu M. Rat-bite fever complicated by vertebral osteomyelitis: a case report. J Infect Chemother. 2016;22(8):574–6. https://doi.org/10.1016/j.jiac.2016.01.023.
Flannery DD, Akinboyo I, Ty JM, Averill LW, Freedman A. Septic arthritis and concern for osteomyelitis in a child with rat bite fever. J Clin Microbiol. 2013;51(6):1987–9. https://doi.org/10.1128/JCM.03139-12.
Eisenberg T, Poignant S, Jouan Y, Fawzy A, Nicklas W, Ewers C, et al. Acute tetraplegia caused by rat bite fever in snake keeper and transmission of Streptobacillus moniliformis. Emerg Infect Dis. 2017;23:719–21 Centers for Disease Control and Prevention (CDC).
Kache PA, Person MK, Seeman SM, McQuiston JR, McCollum J, Traxler RM. Rat-bite fever in the United States: an analysis using multiple national data sources, 2001–2015. Open Forum Infect Dis. 2020;7(6):ofaa197.
Acknowledgements
We wish to acknowledge Stephanie Bryant, MD for providing the histology image.
Funding
The authors report no funding for this manuscript or its publication.
Author information
Authors and Affiliations
Contributions
S.H.A. and R.M. equally contributed to this manuscript. The author(s) read and approved the final manuscript.
Authors’ information
Rahul Mahapatra, DO is an Assistant Professor of Medicine at SUNY Upstate University Hospital. He specializes in Infectious Diseases.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Our case report does not meet criteria for required review by SUNY Upstate’s (our institution) IRB (https://www.upstateresearch.org/compliance/committees/institutional-review-board-irb/case-reports/).
Consent for publication
Written consent for publication was obtained from the patient. A copy of the written consent form can be made available for the editor to review under reasonable request.
Competing interests
The authors report no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Adams, S.H., Mahapatra, R. Rat bite fever with osteomyelitis and discitis: case report and literature review. BMC Infect Dis 21, 479 (2021). https://doi.org/10.1186/s12879-021-06172-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-021-06172-x