
Abstract
Background
The goal of tuberculosis elimination put forward in the End TB Strategy prioritizes diagnosis and treatment of incipient and subclinical TB, recently defined by key stakeholders as “asymptomatic, early pre-clinical disease during which pathology evolves”. Regarded as indicative of a high risk of TB progression, considerable efforts have been made to identify these cases through exploration of biomarkers. The present study aimed to evaluate simple scoring systems for TB exposure as screening tools for subclinical TB, the only identifiable of the incipient and subclinical disease states, in a contact investigation (CI) setting of low HIV-prevalence.
Methods
Nested within a large prospective study in household contacts (HHCs) of smear positive pulmonary TB cases in South-India conducted 2010–2012, we assessed 1) the association between the Tuberculosis Contact Score (TCS) and the Infectivity Score, with established tools for Mycobacterium tuberculosis (Mtb) infection, corrected for established TB risk factors, and 2) the capability of the TB exposure scores to identify subclinical TB defined by Mtb-culture positivity in sputum or gastric aspirate (subjects < 5 years) specimen.
Results
Of 525 HHCs, 29 were Mtb-culture positive and 96.6% of these asymptomatic. The TCS and the Infectivity Score associated with positive Tuberculin Skin Test and QuantiFeron TB-Gold In-tube assay (QFT) results in multivariate analyses (TCS: ORTST 1.16, 95% CI: 1.01, 1.33; ORQFT 1.33 95% CI: 1.16, 1.51. Infectivity Score: ORTST 1.39, 95% CI: 1.10, 1.76; ORQFT 1.41 95% CI: 1.16, 1.71). The Infectivity Score showed a moderate capability to identify subclinical TB (AUC of 0.61, 95% CI: 0.52, 0.70).
Conclusions
Although our results did not identify an easily applicable screening tool for subclinical TB, the present study indicates that focusing on TB-related symptoms in CI settings may be of limited value for early identification of HHCs with high risk for TB progression.
Similar content being viewed by others


Background
Globally, tuberculosis (TB) caused by Mycobacterium tuberculosis (Mtb) is the largest killer among infectious diseases, causing an estimated 1.2 million deaths in 2018 [1]. Despite declining TB incidence achieved through considerable joint efforts since the Stop TB Initiative [2], the TB epidemic will represent a great challenge for years to come: the estimated number of new TB cases was 10.0 million in 2018 [1]. Traditionally, treatment of cases has been the cornerstone of epidemiological control [2, 3]. In most high-endemic countries, case detection relies on patients seeking health-care because of symptoms, but this strategy leaves 40% of estimated TB cases undiagnosed [4]. In order to reduce the TB prevalence further, The End TB Strategy included in the Sustainable developmental goals, emphasizes early diagnosis of cases [5] including incipient TB defined as “asymptomatic, early pre-clinical disease during which pathology evolves, such as mycobacterial replication or the inflammatory response. Radiological abnormalities or positive microbiological tests may or may not be present. This state may either evolve and lead to symptomatic clinical TB or regress and remain asymptomatic” [6]. Meeting this ambitious goal will require systematic screening of contacts and high risk groups for TB disease and subsequent preventive or full-length TB treatment where adequate [5].
Being recently exposed, Mtb-infected household contacts (HHCs) have increased risk of TB progression and are therefore defined a target population for active case-finding as part of contact investigations (CIs) [7]. The World Health Organization (WHO) strongly recommends CIs by health staff visiting households following diagnosis of all smear positive pulmonary TB cases. In low-middle income countries (LMICs) with TB incidence ≥100 per 100,000 population, CIs include evaluation for active TB in persons of all ages with symptoms. If active TB is excluded, preventive treatment should be given to children aged < 5 years and persons living with HIV (PLHIV) [8]. Although suggested as a possible strategy to eliminate TB [9,10,11], giving preventive treatment to all Mtb-infected subjects is not practical in LMICs with moderate-high TB incidence as health systems are already overwhelmed. Although the Tuberculin Skin Test (TST) and/or interferon-gamma release assays (IGRAs) give evidence of Mtb-infection, these tests have poor predictive value for future TB [12, 13] reducing their relevance in the identification of incipient and subclinical TB [14]. These disease states represent early TB disease with high risk of TB progression and are likely to contribute to continued transmission [6, 14]. Therefore, the World Health Organization (WHO) and other stakeholders are strongly encouraging and facilitating the development of novel tests capable of identifying incipient and subclinical TB [6, 15]. CI represents a reasonable well-established framework for identification of these TB cases which would have a large impact on the TB epidemic [9, 16] subsequently increasing national incentives to adhere to programmatic CIs [8]. Although the scientific community are making progress in identifying host biomarker-based risk signatures for TB progression [17,18,19], validation and approval according to defined target product profiles [6, 15] will still take time.
Notably, risk factors for incipient/subclinical and active TB can be assumed to be similar [14, 20,21,22]. The risk of Mtb-infection and disease progression is generally accepted to be strongly affected by the degree of exposure [23, 24]. Therefore, a scoring system has been developed to quantify TB-exposure in HHCs when evaluating the performance of the TST and IGRAs in pediatric and adult populations [24,25,26,27]. The Tuberculosis Contact Score (TCS) contains multiple subscores (Infectivity Score, Duration of Contact Score, Type of Exposure Score and Duration of Symptoms Score) and, as opposed to TST and IGRAs, does not require repeated visits and laboratory facilities. Sputum smear grade alone has also been found to associate with TST [28, 29] and QFT positivity [30, 31]. We therefore hypothesized that TB-exposure scores could serve as screening tools for incipient/subclinical TB. Verification of incipient TB according to the recent consensus definition by Kik et al., is indeed challenging [6]. Inspired by Drain et al. who denotes subclinical TB as a categorical state between incipient and clinical TB where cases can be identified by microbiological or radiological evidence [14], we considered laboratory confirmation a more robust evidence of ongoing Mtb-replication than chest X-ray changes. We therefore defined subclinical TB by growth of Mtb in respiratory (or gastric aspirate for children aged > 5 years) specimens from recently exposed HHCs and argue that we hereby identify the subjects with the highest bacterial burden suggestive of risk of transmission and progression to overt disease. Patient-reported symptoms are highly variable in previous Asian studies even in definite TB cases [32], and were therefore not included in our definition.
Thus, in the context of a prospective study of HHCs of adult pulmonary TB index cases in South India, our primary aim was to evaluate the potential of the TB exposure scores TCS and the Infectivity Score (a TCS subscore), as screening tools for subclinical TB. We first assessed the association between the TB exposure scores for identifying Mtb-infection (TST and Quantiferon) and subclinical TB while correcting for established TB risk factors. We then evaluated the capability of the TB exposure scores to identify individual contacts and/or families with ≥1 subclinical TB case.
Methods
Study population
The present study was a cross-sectional study nested within a large prospective household contact (HHC) study conducted in Palamaner Taluk, Andhra Pradesh, India (3.200°N, 72.7500°E, altitude 683 m) in the period 2010–2012. The bacillus Calmette-Guérin vaccine (BCG) coverage in the area was > 90% in all populations < 2 years except for the muslim minority (81.4%) [33]. The HIV prevalence in tested pregnant women in the area was 1–2% [34]. Index cases were recruited through the RNTCP (Revised National TB Control Program) when diagnosed with smear positive pulmonary TB (PTB). Both index cases and household contacts were enrolled in the HHC study: eligible PTB cases were smear positive subjects aged > 18 years. Eligible contacts were persons living ≥75% of the time in the same household as the index case and sharing the same kitchen [35]. Contacts with previous PTB or already on TB treatment/prophylaxis were excluded. Written informed consent was given by all adults. Children aged 7–18 years gave their assents followed by parental consent whereas parental consent alone was given for children aged < 7 years.
Tuberculosis contact investigation
According to the study protocol, all participating contacts were offered a comprehensive evaluation at baseline. This included an interview on socioeconomic conditions, medical history, TB-symptoms and clinical examinations including weight, TST, the QuantiFeron TB-Gold In-tube assay (QFT), two sputa (gastric aspirates for children ≤5 years) harvested on two consecutive days, for smear and culture, and chest X-rays (anterior view for all, lateral view added on selected children < 5 years). First, a blood sample was drawn for the QFT that was interpreted according to the manufacturer’s instructions (a positive test was defined as ≥0.35 IU/ml). Then trained staff performed a TST by injecting 2 TU Purified Protein Derivate (PPD, SPAN Diagnostics Ltd., Surat, India) intra-dermally on the volar part of the left arm. The following induration was read after 48-96 h (~ 80% evaluated within 72 h, the remaining within 96 h) and defined positive if ≥10 mm. The TST was repeated after 1–4 weeks in HHCs with an induration < 5 mm (n = 54), and the baseline TST result defined as the larger of the two tests. The chest X-rays were interpreted as either “normal”, “abnormal, not TB” or “abnormal TB”, first by a medical officer in the field, later by a radiologist whose interpretation was preferred if discrepancy. Sputum/gastric samples were evaluated by smear microscopy for acid-fast bacilli (AFB) and cultured on both liquid (BACTEC MGIT 960™ [Becton and Dickinson, USA]) and solid (Lowenstein-Jensen) media. Identification of Mtb was done using the GenoType MTBC test kit (HAIN kit). All HHC participants were offered HIV-testing and pre-test counselling at baseline.
TB exposure scores: the tuberculosis contact score and the infectivity score
The Tuberculosis Contact Score (TCS) was based on previously published scores when assessing children [24] and adults [26], and modified to include HHCs of all ages. Relationship score was excluded as data were judged unreliable (Table 1).
The TCS was based on interview (three questions) and sputum evaluation of the index cases assuming the gradient of exposure to be a composite function of: 1) the infectivity of the index case represented by the sputum smear grade, graded 0–6 (Infectivity Score), 2) closeness to the index case during sleep, graded 0–4 (Type of Exposure Score), 3) the time (hours per day) spent with the index case, graded 0–4 (Duration of Contact Score), and 4) duration of the index case’s symptoms before first visit to the doctor, graded 0–4 (Duration of Symptoms Score). The TCS is a sum of all subscores (max score 18); the higher the score, the greater the exposure and risk of Mtb-infection and disease.
Categorization and definition of household contacts (HHCs) according to Mtb-infection status and subclinical TB
For analysis, HHCs were categorized according to their Mtb-infection status at baseline defined by 1) TST and QFT results (both tests required: TST and QFT negative; TST or QFT positive; TST and QFT positive) or 2) subclinical TB defined by positive Mtb-culture in sputum or gastric aspirate (subjects < 5 years) specimen. Although being asymptomatic is the key in the suggested definition for subclinical TB, broad reports from similar CI settings in Asia suggest that 40–79% of active TB cases do not report symptoms [32] highlighting the disease continuum and difficulty in drawing a strict line between subclinical and active TB. After all, finding all these cases must be the goal of CIs. In accordance with the suggested subclinical TB definition [14] and the study aim of finding a screening tool applicable in the field, categorization of subclinical TB was done irrespective of chest X-ray results.
Statistical analysis
Categorical variables were reported as percentages. Continuous variables were summarized by mean and standard deviation or median and interquartile range, as appropriate. TST (mm) and QFT (IU/ml) results were analyzed both as continuous variables and as categorical variables dichotomized around their cut-offs (TST ≥10 mm) and (QFT ≥0.35 IU/ml). Distribution of clinical characteristics between HHCs categorized according to Mtb-infection status was assessed with Chi-square test and one-way analysis of variance (ANOVA) (Tukey “Honest Significant Difference” method for post-hoc comparisons), where appropriate. Associations between the independent variables TCS and established risk factors for TB (age, gender, BCG-scar, diabetes, smoking, indoor pollution, crowding) and the dependent variables 1) TST and QFT results, and 2) subclinical TB, were evaluated by univariate logistic regression, and multivariate logistic regression adjusted for previously listed risk factors for TB. Since assessment of body weight is different in subjects aged ≥15 years (Body Mass Index, BMI) and < 15 years (Body Mass Index Z-score, BMIZ), BMI and BMIZ were only entered in the models evaluating this variable, which were then stratified for age. All other listed TB risk factors were entered in the BMI/BMIZ models. Similar models were fitted to the Infectivity Score. Unadjusted, predictive capabilities of TCS, the Infectivity Score, TST, and QFT for the individual contacts and/or families with ≥1 contact Mtb culture positive at baseline, were assessed using receiver operating characteristic (ROC) curves and area under curve (AUC). A significance level of p < 0.05 was used. IBM SPSS Software, version 25 and R Core Team, 2018.
Results
Characterization of the study population
A total of 525 household contacts (HHCs) were recruited from 176 index cases in the study area accounting for 94.3% of all eligible households. Index cases reported a median of 20 days (IQR: [15, 30] days) from onset of symptoms to first doctor visit, and a median of 6 days (IQR: [3, 20] days) from doctor visit to diagnosis. At inclusion, 93 index cases (57%) had started treatment. In these subjects, the median time from diagnosis to initiation of treatment was 2 days (IQR: [2, 4] days), and a median of 2 days of treatment was given at the time of CI (IQR: [1, 2] days). Baseline investigations were completed in 490 (93%) HHCs, in a median of 4 days (IQR: [3, 5] days) in the 436 (83%) HHCs with only one TST, and a median of 17.5 days (IQR: [15.0, 19.25]) in the 54 (10%) HHC with repeated TST. Adequate specimen for Mtb culture were harvested in 493 (93.9%) HHCs. Of these, 488 (99%) (and all 38 children < 5 years) had two samples harvested on two consecutive days.
Males accounted for 40.5% of the study cohort, and 63% of the study cohort were aged > 14 years. BCG scar was recorded in 221 (51.5%). All the 312 (60.4%) HHCs that agreed to HIV-testing were HIV negative. Houses were small with a mean of 4.25 (St.dev 2.04) subjects per room. Indoor pollution can be assumed high as 75% used wood and agricultural residue for fuel. In addition, 118 (24.8%) were/had been smokers for ≥6 months. The distribution of gender, age, TB risk factors and clinical parameters within the Mtb-infection categories are given in Table 2.
Among the 29 subclinical TB cases, one (5.5%) had symptoms, one had a positive smear and “abnormal TB” chest X-rays, one had “abnormal TB” and one “abnormal, not TB” chest X-ray.
Association between TB exposure scores and Mtb-infection in HHCs
Although the association between TCS and TST/QFT is established in other cohorts [24,25,26,27], we first investigated the strength of this association in the present Indian cohort corrected for established risk factors for TB. The TCS and the Infectivity Score was associated with positive TST and QFT both in univariate and in multivariate analysis (Table 3).
In the multivariate models, the likelihood for a positive TST increased by 16% (95% CI: 1–33%) per unit increase in the TCS and by 39% (95% CI: 10–76%) per unit increase in the Infectivity Score, whereas the likelihood for a positive QFT increased 33% (95% CI: 16–51%) per unit TCS and 41% (95% CI: 16–71%) per unit increase of the Infectivity Score. Surprisingly, LPG fuel, indicative of higher SES and less indoor pollution, was significantly associated with a positive TST in multivariate analysis (TCS model: OR 2.05, 95% CI: 1.07, 3.93. Infectivity Score model: OR 1.96, 95% CI: 1.02, 3.76). Notably, the association was not present when analyses were limited to HHCs ≥15 years regardless of BMI being included in analyses. No other known TB risk factors associated with TST or QFT result.
Association between TB exposure scores and subclinical TB in HHCs
There was no association between the TCS or the Infectivity Score and subclinical TB (Table 4).
Of TB risk factors, only crowding was associated with subclinical TB (TCS multivariate model: OR 0.72, 95%CI: 0.54, 0.95. Infectivity Score multivariate model: OR 0.71, 95% CI: 0.53, 0.95). This negative association was unexpected as crowding normally increases TB risk [36]. Notably, crowding was not significant in the BMI model, suggesting interaction between BMI and crowding. To explore this, the interaction BMI/crowding was entered in the model resulting in no significant association for crowding alone.
The capacity of TB exposure scores to identify subclinical TB
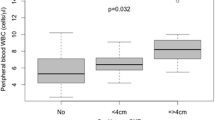
Finally, we assessed the capability of the TB exposure scores to identify individual contacts and/or families with ≥1 contact with subclinical TB. For comparison, the same analyses were performed for TST and QFT at baseline CI. As our aim was to evaluate the potential of the TB exposure scores as robust screening tools, no adjustments were made. The TCS and the established immunological tools, TST and QFT, all had AUC values close to 0.5 indicating no capability to identify individual HHCs and/or families with ≥1 HHC with Mtb-positive cultures (data not shown). Interestingly, the simpler Infectivity Score showed moderate capability to identify individual contacts (AUC of 0.61, 95% CI: 0.52, 0.70) but marginal capability to identify families with ≥1 contact with growth of Mtb-positive sputum cultures (AUC of 0.58, 95% CI: 0.48, 0.68) (Fig. 1).

The capability of the Infectivity Score to identify individual household contacts (HHCs) with growth of Mtb in sputum cultures (A) and families with ≥1 HHCs (B)
Discussion
To our knowledge, the present study is the first to assess the Tuberculosis Contact Score (TCS) and the Infectivity Score as screening tools for subclinical TB in a CI setting. Currently, no tools are available for this purpose. Even with promising host biomarker-based risk signatures for TB progression [17,18,19], validation in various populations as well as translation to a point-of-care test format, will take time [6, 15]. Therefore, the present study was motivated by our hope that simple scoring systems, previously proven to reflect TB exposure, a well-established risk factor for TB, could fill some of this gap. Being independent of laboratory and X-ray facilities, the TCS or the Infectivity Score can easily be applied as a screening tool resulting in more targeted CIs either by sorting out low-risk families/subjects where no CI could be justified, or identify high-risk families/subjects warranting referral for further TB investigations. Regrettably, the TCS could not reliably identify individual subjects or families with subclinical TB. The Infectivity Score performed better with a significant capacity to identify subjects and families with subclinical TB with an AUC of 0.61 and 0.58 respectively. This is however, not good enough for a screening test [37] to identify low-risk (“rule-out”) or high-risk (“rule-in”) families/subjects, underlining the need for continued search for host biomarkers for this screening purpose. Nevertheless, the present study adds an important aspect for CIs. Notably, the strong recommendations for CI for active case finding in all households of sputum positive TB index patients [8, 38] focus on symptomatic HHCs. The present study, one of very few studies from India where sputum samples for both smear and culture were collected from all HHCs regardless of signs and symptoms of disease, provides clear evidence that the majority of HHCs with replicating Mtb in respiratory specimen were asymptomatic. The discrepancy between symptoms, X-ray findings and Mtb-culture results is remarkable, and illustrates the challenge of early identification of cases based on patient-reported symptoms. Among the 525 HHCs, 29 met our definition of subclinical TB (5.5%), but only 1 of the Mtb-culture positive participants had symptoms qualifying for a co-prevalent case (0.2%). Of 525 HHCs, 13 (2.7%) reported symptoms, but only one of the symptomatic HHCs (8.3%) had Mtb-positive cultures. Therefore, in a regular CI setting where microbiological sampling is, at best, done only in symptomatic subjects [5], 28 of 29 (96.6%) subclinical cases would remain undetected. The frequency of Mtb-culture positivity of 5.5% HHCs in the present study, is remarkably high compared to the reported 0.23% of Mtb-culture positivity in symptomatic Indian patients (passive case-finding) [39, 40], but comparable to another Indian Study (4.3%) [41]. We do though, acknowledge that our definition of subclinical TB that relied on Mtb-culture results only, and not on chest X-ray findings as suggested by Drain et al. [14], might have underestimated the number of subclinical TB cases. Interestingly, only 2 (6.9%) had X-ray changes suggestive of TB and none of these had symptoms. The same picture was observed for HHCs within the other Mtb-infection categories with X-ray changes suggestive of TB: Of 3 TST−/QFT- subjects none had symptoms, of 6 TST+ or QFT+ one had symptoms, and of 3 TST+/QFT+ none had symptoms. Therefore, we argue that our Mtb-culture based definition of subclinical TB is the most objective and robust tool for identification of subjects with high-risk for progressive disease and transmission [42,43,44,45]. We acknowledge though, that the relevance of Mtb-replication and transient excretion in the early phase of Mtb-infection reported in children [46], that probably also occurs in adults, could be questioned, as successful containment and spontaneous recovery can be expected in an unknown proportion of subjects [14].
The window of HHC enrollment following TB index case identification could influence the number of HHCs with ongoing Mtb-replication verified by positive cultures. The present study succeeded in rapid inclusion of HHCs illustrated by 42.6% of TB index cases not yet on treatment at inclusion. The delay to diagnosis for the index cases was higher in our study (mean 20 days) than in other Indian studies (mean 6–16 days) [47,48,49], but lower than in LMICs other than Sub-Saharan Africa (median 27 days) [50]. Furthermore, the majority of included HHCs had baseline investigations efficiently completed within a median of 4 days (83%), and all completed within 40 days.
Of further relevance is the vulnerability for Mtb-infection and subclinical TB in our population for which the presence of TB risk factors in the study population could be indicative: Despite a high reported BCG-coverage [33], only 51.1% of all HHCs in our study had a BCG scar compared to > 80% in a semi-urban population in Delhi [41]. Interestingly, scar rates of only 47.5% were reported in newborns with low birthweight [51]. A prospective cohort study conducted (2006–2008) in the same study area reported a birthweight of ≤2500 g in 29% of 4382 neonates [52] which taken together suggests an explanation for the low BCG scar rate in the present study.
Surprisingly, and despite the fact that we for the first time confirmed a clear association between the TB exposure scores and TST/QFT in an Indian HHC population, neither the TB exposure scores or other well-established TB risk factors had a clear association with subclinical TB in multivariate analysis. There are multiple possible explanations: Although high TB exposure outside the household is the most evident, this seems unlikely given the Indian TB incidence about 180 per 100,000 in the study period [4]. It may be possible that the moderate size of our study cohort means that it is not entirely comparable with findings from large epidemiological studies [21, 22, 36]. Furthermore, it is possible that the considerable crowding (mean of 4.25 persons per room) have affected negatively the performance of the TCS by causing less differentiated exposure of the HHCs to the index case. Crowding might also decrease the association observed in large-scale studies between smoking and TB disease due to passive smoking. The size of the households in the present study (median of 5) was similar to another HHC study in rural Indian [53]. Semi-urban and urban Indian families tend to be smaller [41, 54], but congested living is common in both rural and urban areas [41] with 96.8% of families in the present study living in 1–2 rooms. Interestingly, multivariate analyses revealed a possible interaction between BMI and crowding that could confound the results. Notably, children aged < 15 could not be included in multivariate analyses assessing BMI as BMI is an invalid measurement in this age group. For HHCs aged ≥15 years, HHCs with and without subclinical TB had a mean BMI of 18.7 (St.dev 2.13) and 19.6 (St.dev 3.25) respectively. This was considerably lower than the BMI in two large Peruvian HHC Study cohorts (mean BMI 25.2 and 25.6). Interestingly, the dose-response log-linear relationship between BMI and TB incidence reported in a meta-analysis, was less certain at BMI < 18.5 and > 30 [21].
The strengths of the present study are inclusion of HHCs of all ages, detailed sociodemographic data, a thorough work-up of most contacts with TST, QFT, sputum or gastric aspirate samples for both smear and cultures, combined with data on the TCS and Infectivity Score for all HHCs. A major weakness is the lack of 18–24 months follow-up data in accordance with current consensus definition for incipient TB [6]. Another limitation is due to the 18% missing data in the study. The missing data may be the reason that some associations may not have been detected. Moreover, as the missingness pattern is at least partly attributable to missing not at random mechanisms (e.g., different types of non-responders) there is a risk of bias in the reported associations.
Conclusions
Although our results were disappointing with regard to our hope of identifying an easily applicable screening tool for subclinical TB, the present study provides relevant information to CIs as framework for identification and early treatment of subclinical TB required to achieve the ambitious goal of the End TB Strategy [5]. Findings in our cohort indicate that focusing on TB-related symptoms is of little value in identifying HHCs with replicating Mtb in respiratory specimens, as this strategy would have left 96.6% of HHCs with Mtb-positive cultures unidentified. Although other studies support more targeted identification of subjects with high TB risk based on other TB risk assessment-based framework [21, 22, 36], it is questionable whether exploring and validating eventual new TB risk scores offers a viable alternative to host biomarker-based screening tools for subclinical TB, which are strongly needed to reach the ambitious goal of TB elimination.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to ongoing work on immune readouts in the same cohort but are available from the corresponding author on reasonable request.
Abbreviations
- ANOVA:
-
Analysis of variance
- AUC:
-
Area under curve
- BCG:
-
Bacillus calmette-guérin vaccine
- BMI:
-
Body mass index
- BMIZ:
-
Body mass index Z-score
- CI:
-
Contact investigation
- HHC:
-
Household contact
- HIV:
-
Human immunodeficiency virus
- IGRA:
-
Interferon-gamma release assay
- IQR:
-
Interquartile range
- LMICs:
-
Low-middle income countries
- Mtb :
-
Mycobacterium tuberculosis
- OR:
-
Odds ratio
- PLHIV:
-
People living with human immunodeficiency virus
- PPD:
-
Purified protein derivate
- PTB:
-
Pulmonary tuberculosis
- QFT:
-
Quantiferon TB-gold In-tube assay
- RNTCP:
-
Revised national TB control program
- ROC:
-
Receiver operating characteristic
- TB:
-
Tuberculosis
- TCS:
-
Tuberculosis contact score
- TST:
-
Tuberculin skin test
- WHO:
-
World health organization
References
WHO. Global tuberculosis report 2019. Geneva: World Health Organization; 2019. Contract No.: ISBN 978-92-4-156571-4
WHO. The Global Plan to Stop TB 2006–2015. 2006.
WHO. WHO Tuberculosis Programme. In: Framework for Effective Tuberculosis Control; 1994.
WHO. Global tuberculosis report 2018. Geneva: World Health Organization; 2018. Report No.: ISBN 978-92-4-156564-6
WHO. In: Organization WH, editor. The End TB Strategy. Global strategy and targets for tuberculosis prevention, care and control after 2015. Geneva: World Health Organization; 2014.
Kik SV, Schumacher S, Cirillo DM, Churchyard G, Boehme C, Goletti D, et al. An evaluation framework for new tests that predict progression from tuberculosis infection to clinical disease. Eur Respir J. 2018;52(4), 1800946.
Fox GJ, Barry SE, Britton WJ, Marks GB. Contact investigation for tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2013;41(1):140–56.
WHO. Recommendations for investigating contacts of persons with infectious TB in low- and middle-income countries. Geneva: World Health Organization; 2012.
Abu-Raddad LJ, Sabatelli L, Achterberg JT, Sugimoto JD, Longini IM Jr, Dye C, et al. Epidemiological benefits of more-effective tuberculosis vaccines, drugs, and diagnostics. Proc Natl Acad Sci U S A. 2009;106(33):13980–5.
Dye C, Glaziou P, Floyd K, Raviglione M. Prospects for Tuberculosis Elimination. Annu Rev Public Health. 2012;34(1):271–86.
Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent mycobacterium tuberculosis infection. N Engl J Med. 2015;372(22):2127–35.
Diel R, Loddenkemper R, Nienhaus A. Predictive value of interferon-gamma release assays and tuberculin skin testing for progression from latent TB infection to disease state: a meta-analysis. Chest. 2012;142(1):63–75.
Rangaka MX, Wilkinson KA, Glynn JR, Ling D, Menzies D, Mwansa-Kambafwile J, et al. Predictive value of interferon-gamma release assays for incident active tuberculosis: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(1):45–55.
Drain PK, Bajema KL, Dowdy D, Dheda K, Naidoo K, Schumacher SG, et al. Incipient and Subclinical Tuberculosis: a Clinical Review of Early Stages and Progression of Infection. Clin Microbiol Rev. 2018;31(4).
Kik SV, Denkinger CM, Casenghi M, Vadnais C, Pai M. Tuberculosis diagnostics: which target product profiles should be prioritised? Eur Respir J; 2014.
Houben RM, Dodd PJ. The global burden of latent tuberculosis infection: a re-estimation using mathematical Modelling. PLoS Med. 2016;13(10):e1002152.
Zak DE, Penn-Nicholson A, Scriba TJ, Thompson E, Suliman S, Amon LM, et al. A blood RNA signature for tuberculosis disease risk: a prospective cohort study. Lancet. 2016.
Petruccioli E, Scriba TJ, Petrone L, Hatherill M, Cirillo DM, Joosten SA, et al. Correlates of tuberculosis risk: predictive biomarkers for progression to active tuberculosis. Eur Respir J. 2016;48(6):1751–63.
Fletcher HA. Systems approaches to correlates of protection and progression to TB disease. Semin Immunol. 2018;39:81–7.
Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. WHO's new end TB strategy. Lancet. 2015;385(9979):1799–801.
Lonnroth K, Williams BG, Cegielski P, Dye C. A consistent log-linear relationship between tuberculosis incidence and body mass index. Int J Epidemiol. 2010;39(1):149–55.
Saunders MJ, Wingfield T, Tovar MA, Baldwin MR, Datta S, Zevallos K, et al. A score to predict and stratify risk of tuberculosis in adult contacts of tuberculosis index cases: a prospective derivation and external validation cohort study. Lancet Infect Dis. 2017;17(11):1190–9.
Mandalakas AM, Kirchner HL, Lombard C, Walzl G, Grewal HM, Gie RP, et al. Well-quantified tuberculosis exposure is a reliable surrogate measure of tuberculosis infection. Int J Tuberc Lung Dis. 2012;16(8):1033–9.
Hesseling AC, Mandalakas AM, Kirchner HL, Chegou NN, Marais BJ, Stanley K, et al. Highly discordant T cell responses in individuals with recent exposure to household tuberculosis. Thorax. 2009;64(10):840–6.
Perez-Porcuna TM, Pereira-da-Silva HD, Ascaso C, Malheiro A, Buhrer S, Martinez-Espinosa F, et al. Prevalence and diagnosis of latent tuberculosis infection in Young children in the absence of a gold standard. PLoS One. 2016;11(10):e0164181.
Shams H, Weis SE, Klucar P, Lalvani A, Moonan PK, Pogoda JM, et al. Enzyme-linked immunospot and tuberculin skin testing to detect latent tuberculosis infection. Am J Respir Crit Care Med. 2005;172(9):1161–8.
Tieu HV, Suntarattiwong P, Puthanakit T, Chotpitayasunondh T, Chokephaibulkit K, Sirivichayakul S, et al. Comparing interferon-gamma release assays to tuberculin skin test in Thai children with tuberculosis exposure. PLoS One. 2014;9(8):e105003.
Shaw JB, Wynn-Williams N. Infectivity of pulmonary tuberculosis in relation to sputum status. Am Rev Tuberc. 1954;69(5):724–32.
Espinal MA, Perez EN, Baez J, Henriquez L, Fernandez K, Lopez M, et al. Infectiousness of mycobacterium tuberculosis in HIV-1-infected patients with tuberculosis: a prospective study. Lancet. 2000;355(9200):275–80.
Mutsvangwa J, Millington KA, Chaka K, Mavhudzi T, Cheung YB, Mason PR, et al. Identifying recent mycobacterium tuberculosis transmission in the setting of high HIV and TB burden. Thorax. 2010;65(4):315–20.
Shanaube K, Hargreaves J, Fielding K, Schaap A, Lawrence KA, Hensen B, et al. Risk factors associated with positive QuantiFERON-TB gold in-tube and tuberculin skin tests results in Zambia and South Africa. PLoS One. 2011;6(4):e18206.
Onozaki I, Law I, Sismanidis C, Zignol M, Glaziou P, Floyd K. National tuberculosis prevalence surveys in Asia, 1990-2012: an overview of results and lessons learned. Trop Med Int Health : TM IH. 2015;20(9):1128–45.
International Institute for Population Sciences (IIPS) and Macro International. National Family Health Survey (NFHS-3), India, 2005-06: Andhra Pradesh. Mumbai: IIPS; 2008.
NACO. Annual HIV Sentinel Surveillance. Country Report 2008-2009. Government of India: Government of India; 2011 [Available from: http://www.naco.gov.in/sites/default/files/HIV%20Sentinel%20Surveillance%20India%20Country%20Report%2C%202008-09.pdf. Accessed 16 Dec 2019.
Go I. Concepts and definitions: Government of India CoId; 2001.
Lonnroth K, Raviglione M. Global epidemiology of tuberculosis: prospects for control. Semin Respir Crit Care Med. 2008;29(5):481–91.
WHO. High-priority target product profiles for new tuberculosis diagnostics: report of a consensus meeting. Geneva: World Health Organization; 2014. Report No.: WHO_HTM_TB_2014.18
WHO. In: Organization WH, editor. Guidelines on the management of latent tuberculosis infection. Geneva: World Health Organization; 2015.
WHO. Global tuberculosis report 2013. Geneva, World Health Organization; 2013. Report No.: ISBN 9789241564656
Government of India CTD. TB India 2014. Revised National TB Control Programme. Annual Status Report. In: Welfare MoHaF, editor. www.tbcindia.nic.in: Government of India; 2014. Accessed 16 Dec 2019.
Singh J, Sankar MM, Kumar S, Gopinath K, Singh N, Mani K, et al. Incidence and prevalence of tuberculosis among household contacts of pulmonary tuberculosis patients in a peri-urban population of South Delhi. India PLoS One. 2013;8(7):e69730.
Young DB, Gideon HP, Wilkinson RJ. Eliminating latent tuberculosis. Trends Microbiol. 2009;17(5):183–8.
Barry CE III, Boshoff HI, Dartois V, Dick T, Ehrt S, Flynn J, et al. The spectrum of latent tuberculosis: rethinking the biology and intervention strategies. Nat Rev Microbiol. 2009;7(12):845–55.
Lawn SD, Zumla AI. Tuberculosis Lancet. 2011;378(9785):57–72.
Fennelly KP, Jones-Lopez EC. Quantity and quality of inhaled dose predicts immunopathology in tuberculosis. Front Immunol. 2015;6:313.
Marais BJ, Gie RP, Schaaf HS, Beyers N, Donald PR, Starke JR. Childhood pulmonary tuberculosis: old wisdom and new challenges. Am J Respir Crit Care Med. 2006;173(10):1078–90.
Pradhan A, Kielmann K, Gupte H, Bamne A, Porter JD, Rangan S. What 'outliers' tell us about missed opportunities for tuberculosis control: a cross-sectional study of patients in Mumbai. India BMC Public Health. 2010;10:263.
Tamhane A, Ambe G, Vermund SH, Kohler CL, Karande A, Sathiakumar N. Pulmonary tuberculosis in Mumbai, India: factors responsible for patient and treatment delays. Int J Prev Med. 2012;3(8):569–80.
Behera BK, Jain RB, Gupta KB, Goel MK. Extent of delay in diagnosis in new smear positive patients of pulmonary tuberculosis attending tertiary care hospital. Int J Prev Med. 2013;4(12):1480–5.
Getnet F, Demissie M, Assefa N, Mengistie B, Worku A. Delay in diagnosis of pulmonary tuberculosis in low-and middle-income settings: systematic review and meta-analysis. BMC Pulm Med. 2017;17(1):202.
Kaur S, Faridi MM, Agarwal KN. BCG vaccination reaction in low birth weight infants. Indian J Med Res. 2002;116:64–9.
Jenum S, Sumithra S, Nelson J, Christian R, Anneke CH, Vicky C, et al. Incidence of tuberculosis and the influence of surveillance strategy on tuberculosis case-finding and all-cause mortality: a cluster randomised trial in Indian neonates vaccinated with BCG. BMJ open respiratory research. 2018;5(1):e000304.
Khaparde K, Jethani P, Dewan PK, Nair SA, Deshpande MR, Satyanarayana S, et al. Evaluation of TB case finding through systematic contact investigation, Chhattisgarh. India Tuberculosis research and treatment. 2015;2015:670167.
Nair D, Rajshekhar N, Klinton JS, Watson B, Velayutham B, Tripathy JP, et al. Household contact screening and yield of tuberculosis cases-a clinic based study in Chennai. South India PLoS One. 2016;11(9):e0162090.
Acknowledgements
Larry Geiter, Sean Bennett, Lew Barker, and Robert Walker, previously at Aeras, and John Kenneth (late) previously at St. Johns’ Research Institute, Bangalore, India, and the TB Trials Study Group (Doherty TM, Grewal HMS, Hesseling AC, Jacob A, Jahnsen F, D’ Souza G, Kurpad AV, Lau E, Lindtjorn B, Macaden R, Vaz M.). Study physicians, field and lab workers in the Palamaner Study Field Site and at St. Johns’ Research Institute, India.
Funding
This work was supported by the Research Council of Norway [grants 179342 and 192534]; the University of Bergen (Norway); Aeras (USA) and St. John’s Research Institute (India). The funding sources had no role in the design of this study and did not have any role during its execution, analyses, interpretation of the data, or decision to submit results and writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Implementation and coordination of the HHC study: JN, MV, HMSG; Study aim and design: HMSG, SJ; Data analyses: GKB, SS, CR, SJ. Figures: CR; Wrote the manuscript: GKB, SJ; Interpretation of data: GKB, CR, SJ, ACH, TMD, HMSG; Approved and contributed to the manuscript: all authors. Agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work: GKB, SS, JN, CR, ACH, TMD, HMSG, MV, SJ.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional ethical review board of the St John’s National Academy of Health Sciences, Bangalore, an independent Ethics Committee contracted by Aeras, USA, and the Ministry of Health Screening Committee, Government of India (No. 5/8/9/60/2006-ECD-I dt. 10.11.2006). Participants (parents/caretakers) gave written consent for enrolment. Also, ethical approval was obtained (Ref no: 2018/1614 D) from the Regional Committee for Medical and Health Research Ethics, Western-Norway (REK Vest).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bekken, G.K., Ritz, C., Selvam, S. et al. Identification of subclinical tuberculosis in household contacts using exposure scores and contact investigations. BMC Infect Dis 20, 96 (2020). https://doi.org/10.1186/s12879-020-4800-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-020-4800-y