
Abstract
Background
Coronavirus disease once thought to be a respiratory infection is now recognised as a multi-system disease affecting the respiratory, cardiovascular, gastrointestinal, neurological, immune, and hematopoietic systems. An emerging body of evidence suggests the persistence of COVID-19 symptoms of varying patterns among some survivors. This study aimed to describe persistent symptoms in COVID-19 survivors and investigate possible risk factors for these persistent symptoms.
Methods
The study used a retrospective study design. The study population comprised of discharged COVID-19 patients. Demographic information, days since discharge, comorbidities, and persistent COVID-19 like symptoms were assessed in patients attending the COVID-19 outpatient clinic in Lagos State. Statistical analysis was done using STATA 15.0 software (StataCorp Texas) with significance placed at p-value < 0.05.
Results
A total of 274 patients were enrolled in the study. A majority were within the age group > 35 to ≤49 years (38.3%), and male (66.1%). More than one-third (40.9%) had persistent COVID-19 symptoms after discharge, and 19.7% had more than three persistent COVID-like symptoms. The most persistent COVID-like symptoms experienced were easy fatigability (12.8%), headaches (12.8%), and chest pain (9.8%). Symptomatic COVID-19 disease with moderate severity compared to mild severity was a predictor of persistent COVID-like symptoms after discharge (p < 0.05).
Conclusion
Findings from this study suggests that patients who recovered from COVID-19 disease may still experience COVID-19 like symptoms, particularly fatigue and headaches. Therefore, careful monitoring should be in place after discharge to help mitigate the effects of these symptoms and improve the quality of life of COVID-19 survivors.
Similar content being viewed by others


Background
COVID-19 is currently spreading rapidly with increasing incidence across most countries of the world [1]. Nigeria, the most populous African country, has recorded 42,208 confirmed cases since the index case in February 2020, and 19,004 recovered cases from the infection as of July 30th 2020 [2]. Lagos, the most populous State in Nigeria, and the epicentre of coronavirus disease 2019 (COVID-19) in Nigeria has recorded 14,954 cases and 192 deaths [2]. However, these figures could be much higher as they are subject to challenges of limited testing capacities which many countries, including Nigeria, currently face amidst potential asymptomatic infections.
The spectrum of clinical presentation of COVID-19 ranges from the asymptomatic, to symptomatic with varying levels of severity depending on age, comorbid conditions, and basal metabolic index [3, 4]. If symptomatic, COVID-19 patients may present with fever, dry cough, anosmia, fatigue as common symptoms, amongst others. Less common symptoms include aches and pains, sore throat, nausea, vomiting and diarrhoea, conjunctivitis, headache, and a skin rash or discolouration of fingers or toes [3, 5,6,7]. Associated shortness of breath and difficulty in breathing indicate severe disease [3, 4]. While most infected people develop mild to moderate illness and recover without requiring hospitalisation, others become sick enough to be hospitalised. Few succumb to the disease as a result of severe irreversible respiratory compromise, the lungs being the most severely affected body organ [8]. Emerging pathologic evidence suggests increased coagulability of many victims’ blood as autopsy findings reveal blood clots in the lungs [9].
Typically, COVID-19 symptoms manifest in individuals for 14 days from onset of symptoms, after which, symptoms expectedly subside or resolve completely, and infectiousness abates [8, 10]. An emerging body of evidence, however, suggests the persistence of post-infection clinical symptoms of varying consistencies and durations among some survivors [11,12,13,14,15,16].
In this study, we describe persistent symptoms in patients who had recovered from COVID-19. Our objectives were to highlight associations between socio-demographic characteristics and comorbidities with persistent symptoms in COVID-19 survivors. Findings from our study may provide additional evidence to guide public health measures and policies, as well as build on the current knowledge of the long-term effects of COVID-19.
Methods
Study design
A retrospective study using de-identified data of cases from the Lagos State COVID-19 outpatient clinic seen between April and June 2020.
Study setting
On April 27th 2020, the Lagos State COVID-19 incident command established a COVID-19 outpatient clinic for all COVID-19 survivors discharged from the six isolation facilities being run in the State. Patients were referred to the Outpatient clinic two weeks after discharge from COVID-19 isolation facilities. Discharge from the isolation facilities between March and May 2020 was based on the World Health Organization (WHO) criteria: Three days after resolution of symptoms and/or Two negative RT-PCR SARS-CoV-2 results, at least 24 h apart. The term ‘survivor’ (as used throughout the paper) is used to describe patients who met the above criteria before discharge from isolation and treatment facilities in Lagos State, Nigeria.
Data collection
A thorough clinical history and physical assessment was conducted for all patients at the outpatient clinic. Information was obtained on the presence or absence of COVID-19 symptoms, general symptoms, and the nature of symptoms if any. This information was reconciled with prior demographic information and medical history for each patient and entered in the outpatient database. The term ‘Persistent symptoms’ (as used throughout the paper) was used to describe patients’ self-reported COVID-19 like symptoms reported during clinical review and physical assessment at the Post COVID-19 clinic. Information on the presence or absence of persistent symptoms before COVID-19 infection was confirmed before the diagnosis of persistent COVID-19 symptoms to rule out potential confounding comorbidities or concurrent infections. Participants were also grouped based on the severity at the time of initial COVID-19 diagnosis using the WHO criteria [17]: Mild- Symptomatic patients with no evidence of viral pneumonia or hypoxia; Moderate – SpO2 > 90%; fever, cough, dyspnea, fast breathing (clinical signs of pneumonia) but no signs of severe pneumonia; Severe - SpO2 < 90%; Adolescent or adult with clinical signs of pneumonia (fever, cough, dyspnea, fast breathing); severe respiratory distress; Asymptomatic- No symptoms.
Statistical analysis
Demographic information, medical history and persistence of symptoms were analysed using descriptive statistics. Univariable and multivariable logistic regression models were used to investigate the association between demographic information, comorbidities and the presence or absence of persistent COVID-19 symptoms. P values of < 0.05 were considered significant, and tests were 2- tailed. Statistical analysis was done using STATA 15.0 software (StataCorp LLC Lakeway Drive, College Station, Texas).
Ethics
Ethical approval was obtained from the Lagos State University Teaching Hospital Health Research Ethics Committee. Approval number: LREC/06/10/1345.
Results
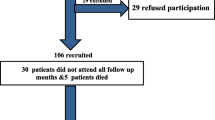
A total number of 274 COVID-19 survivors were assessed in this study. The mean age of respondents was 41.8 years (SD ± 11.8) with a range of 10 to 83 years. Majority of respondents were male (66.1%) and aged between 36 and 49 years (38.3%). The median number of days after discharge with COVID-19 like symptoms was 15 days (IQR 14–17 days) (Table 1). Among the study participants, a majority (50.7%) had a mild form of the disease at the initial time of COVID-19 diagnosis (Table 1).
Clinical characteristics
More than two-thirds (78.5%) of the study population had no underlying comorbid condition (Table 1). Among respondents with underlying comorbidities (n = 52), the most common comorbidities were hypertension (72.9%) and diabetes (15.3%), respectively (Table 1). Over half (59.1%) of the study population had no persistent COVID-19 symptoms. Among respondents with persistent symptoms (n = 112), a majority (48.2%) had three or more persistent COVID-like symptoms (Table 1). Of all cases reviewed (n = 274), the most common symptoms were easy fatigability (12.8%), headache (12.8%), chest pain (9.8%), and insomnia (9.8%) (Table 2).
Association between the presence of persistent symptoms and demographic and medical history among symptomatic COVID-19 cases
Table 3 demonstrates there was no association between age, sex, a history of hypertension, diabetes or multiple comorbidities with the presence of persistent COVID-19 like symptoms among symptomatic COVID-19 cases (n = 253) on univariable logistic regression models. However, participants with moderate disease severity at the time of initial COVID-19 diagnosis had increased odds of persistent COVID-19 symptoms compared to the participants with mild disease severity (OR: 2.17; 95 CI: 1.30, 3.64; p: 0.003). After adjusting for age, sex, number and type of comorbidities (hypertension and diabetes), moderate disease severity at the time of initial COVID-19 diagnosis remained significantly associated with higher odds of persistent COVID-19 like symptoms (aOR: 2.03; 95% CI: 1.19, 3.47; p: 0.009) (Table 3).
Discussion
This study assessed the pattern of COVID-19 like symptoms and their association with demographic factors and comorbidities in a cohort of 274 survivors followed up at a COVID-19 outpatient clinic in Lagos State, Nigeria. About four out of ten survivors remained symptomatic for atleast two weeks after discharge, with the majority of them presenting with more than three symptoms. Easy fatigability, headache, chest pain and insomnia were the most common symptoms. Further, there was a significant association between severity of COVID-19 disease at initial diagnosis with the presence of persistent COVID-19 like symptoms after hospitalisation. Our findings align with reports on COVID-19 symptoms in survivors based on recent studies from the United States, the United Kingdom, and Italy [11, 12, 14, 15].
The most common symptom manifested by survivors in our study was easy fatigability. Carfi et al. [11] also reported easy fatigability in a review of COVID-19 survivors, likewise, Tenforde et al. in a review of cases in the United States [12]. Also, a COVID-symptom study app in the United Kingdom which tracks patients for weeks and months has reported similar symptoms, as in this study [13]. From other peer-reviewed studies and this study, easy fatigability was a consistently identified symptom in COVID-19 survivors [11,12,13,14,15]. Further, several studies have identified chronic pain and psychological distress (anxiety, depression, and post-traumatic stress) in COVID-19 survivors [18,19,20,21]. This underscores the importance of channelling resources to the long-term follow-up and care of COVID-19 survivors to support their return to a normal state of health. Recently the quality of life and rehabilitation of COVID-19 survivors after discharge has generated research interests [11, 22,23,24,25]. Our study identified neurologic symptoms in 39.1% of the COVID-19 survivors reviewed, symptoms such as headaches, insomnia, and attention deficits. These symptoms can potentially preclude a safe and effective return of survivors to usual life. More studies are needed to assess predictors of persistent symptoms, as well as the quality of life in COVID-19 survivors in Nigeria and globally.
Based on our findings, there was no significant association between demographic factors and comorbidities such as hypertension or diabetes and the presence of persistent symptoms in COVID-19 survivors. However, a prior study reported the presence of more than three underlying medical conditions as significant factors in predicting a delayed return to the normal state of health 14–21 days after testing [12], which is contrary to our study where two or more comorbidities was not significantly associated with persistent COVID-19 like symptoms. Further, participants that were symptomatic, with moderately severe forms of COVID-19 disease, at the time of initial diagnosis had higher odds of persistent COVID-19 like symptoms after discharge compared to participants that were mildly symptomatic at the time of initial diagnosis. The relationship between COVID-19 severity and increased odds of persistent symptoms may be explained by the immune response to the SARS-CoV-2 virus which stimulates the production of cytokines and other inflammatory mediators, with higher concentrations found in those with a more severe clinical form [3, 26,27,28]. The multi-systemic inflammatory response to the virus may also be responsible for persistent COVID-19 symptoms in survivors [28,29,30,31].
Persistent COVID-19 symptoms- ‘long COVID’- have been reported to have similarities with other syndromes such as myalgic encephalomyelitis, or chronic fatigue syndrome which occur after viral infections [3, 11, 14] However, the exact pathophysiology of ‘long COVID’ is not yet understood. Probable mechanisms described in the literature include vascular inflammation, detected using 2-deoxy-2-[18F] Fluoro-D-glucose [30], hyper-inflammation from cytokines storm which alters the immune response function, or endothelial dysfunction caused by the action of the SARS-CoV-2 on ACE2 receptors [30, 31]. These mechanisms all support the evidence that COVID-19 is primarily a multi-systemic disease, with varied manifestations [32]. Further, to better understand the entity ‘long COVID’, it is important to distinguish between symptoms from persistent chronic inflammation, and symptoms which may arise as sequelae of organ damage (pulmonary fibrosis and subsequently cough), and other persistent symptoms from factors such as hospital-stay and social isolation (nutritional anaemia, weight loss, muscle wasting) [16].
Of interest is the potential effect of the public health messaging on rapid recovery from COVID-19. While a majority of COVID survivors with mild cases may recover rapidly in about two weeks [26], our evidence suggests that a significant number experience long-term symptoms. The unintended effect of messaging on rapid recovery can be psychosocial, as survivors could begin to worry about their normalcy when experiencing delayed physical or mental recovery. Therefore, effective strategies are needed to accurately coin messaging on COVID-19 recovery and educate survivors to ease the return to their usual way of life.
The current study has limitations. For example, the study depended on self-reported persistent COVID-19 symptoms. However, the diagnosis was carefully made to avoid potential confounders such as symptoms which had been present before SARS-COV-2 infection, concurrent infection from other viral agents, and underlying comorbidities. In addition, the sample population was relatively small, and the retrospective design, as well as the convenient sampling method, may not be generalisable to the over 40,000 confirmed cases of COVID-19 in the country [2]. Further, some self-reported symptoms might be associated with standard therapeutic agents administered to the patients during isolation or treatment in Lagos State [33]. For example, diarrhoea associated with lopinavir/ ritonavir, which was administered as the standard of care between April and May 2020 in Lagos State. However, this association is unlikely because patients presented at the COVID-19 follow-up clinic 14 days or more after therapy and discharge, and effects would have subsided.
Conclusion
In conclusion, this study presents early evidence to support the emerging literature on the persistent manifestation of clinical symptoms among survivors of COVID-19 disease in Lagos State, Nigeria. In the cases reviewed, most survivors with persistent symptoms had more than two self-reported symptoms. Easy fatigability, headaches, chest pain and insomnia, were the most common symptoms. As interest and calls for a review of the current evidence of symptoms in survivors emerge [13, 34], further research is needed to identify factors associated with persistent COVID-19 like symptoms in survivors- termed ‘long COVID’ [34]. Evidence from these studies can guide policies and interventions aimed at improving the quality of life of survivors and return to usual health.
Availability of data and materials
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- ACE2:
-
Angiotensin-Converting Enzyme- 2
- aOR:
-
Adjusted odds ratio
- COVID-19:
-
Coronavirus disease 2019
- DM:
-
Diabetes Mellitus
- HTN:
-
Hypertension
- OR:
-
Odds ratio
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- SpO2:
-
Oxygen saturation
- WHO:
-
World Health Organization
References
COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available at: https://coronavirus.jhu.edu/map.html Accessed 30 July 2020.
Nigeria Center for Disease Control. Available at: http://covid19.ncdc.gov.ng/ Last updated July 30th 2020. Accessed 30 July 2020.
Escandón K, Rasmussen AL, Bogoch I, Murray EJ, Escandón K, Kindrachuk J. COVID-19 and false dichotomies — A nuanced review of the evidence regarding public health, COVID-19 symptomatology, SARS-CoV-2 transmission, masks, and reinfection. OSF Preprints; 2020. https://doi.org/10.31219/osf.io/k2d84.
Cevik M, Kuppalli K, Kindrachuk J, Peiris M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ. 2020;371:m3862.
Grant MC, Geoghegan L, Arbyn M, Mohammed Z, McGuinness L, Clarke EL, et al. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): a systematic review and meta-analysis of 148 studies from 9 countries. PLoS One. 2020;15(6):e0234765. https://doi.org/10.1371/journal.pone.0234765.
Abayomi A, Odukoya O, Osibogun A, Wright O, Adebayo B, Balogun M, et al. Presenting symptoms and predictors of poor outcomes among 2,184 patients with COVID-19 in Lagos state. Int J Infect Dis. 2020;102:226–32. https://doi.org/10.1016/j.ijid.2020.10.024.
Bowale A, Abayomi A, Idris J, Omilabu S, Abdus-Salam I, Adebayo B, et al. Clinical presentation, case management and outcomes for the first 32 COVID-19 patients in Nigeria. Pan Afr Med J. 2020;35(2):24. https://doi.org/10.11604/pamj.supp.2020.35.2.23262.
Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020 Apr 7;323(13):1239–42. https://doi.org/10.1001/jama.2020.2648.
Terpos E, Ntanasis-Stathopoulos I, Elalamy I, Kastritis E, Sergentanis TN, Politou M, et al. Hematological findings, and complications of COVID-19. Am J Hematol. 2020;95:834–47. https://doi.org/10.1002/ajh.25829.
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N Engl J Med. 2020;382(13):1199–207.
Carfì A, Bernabei R, Landi F. For the Gemelli against COVID-19 post-acute care study group. Persistent symptoms in patients after acute COVID-19. JAMA. 2020;324(6):603–5.
Tenforde MW, Kim SS, Lindsell CJ, Rose EB, Shapiro NI, Files CD, et al. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network — United States, march–June 2020. Morb Mortal Wkly Rep. 2020;69(30):993–8.
How long does COVID last? COVID symptom study. Available at: https://covid.joinzoe.com/post/covid-long-term. Accessed 8 Aug 2020.
Davido B, Seang S, Tubiana R, de Truchis P. Post–COVID-19 chronic symptoms: a postinfectious entity? Clin Microbiol Infect. 2020;26(11):1448–9. https://doi.org/10.1016/j.cmi.2020.07.028.
Halpin SJ, McIvor C, Whyatt G, Adams A, Harvey O, McLean L, et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: a cross-sectional evaluation. J Med Virol. 2020:1–10. https://doi.org/10.1002/jmv.26368.
Garg P, Arora U, Kumar A, Wig N. The "post-COVID" syndrome: how deep is the damage? J Med Virol. 2020:1–2. https://doi.org/10.1002/jmv.26465.
World Health Organisation. Clinical management of COVID-19 interim guidance. COVID-19: Clinical care. [Published online May 27th 2020]. Available from: https://www.who.int/publications/i/item/clinical-management-of-covid-19 Accessed 3 Nov 2020.
Cai X, Hu X, Otte EI, Wang J, An Y, Li Z, et al. Psychological distress and its correlates among COVID-19 survivors during early convalescence across age groups. Am J Geriatr Psychiatry. 2020;28(10):1030–9. https://doi.org/10.1016/j.jagp.2020.07.003.
Gennaro Mazza M, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, et al. Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain Behav Immun. 2020;89:594–600. https://doi.org/10.1016/j.bbi.2020.07.037.
Kemp HI, Corner E, Colvin LA. Chronic pain following COVID-19: implications for rehabilitation. Br J Anaesth. 2020;125(4):436–40. https://doi.org/10.1016/j.bja.2020.05.021.
Olufadewa II, Adesina MA, Oladokun B, Baru A, Oladele RI, TO I, et al. “I Was Scared I Might Die Alone”: A Qualitative Study on the Physiological and Psychological Experience of COVID-19 Survivors and the Quality of Care Received at Health Facilities. Int J Travel Med Glob Health. 2020;8(2):51–7.
Klok FA, Boon GJAM, Barco S, Endres M, Geelhoed JJM, Knauss S, et al. The post-COVID-19 functional status scale: a tool to measure functional status over time after COVID-19. Eur Respir J. 2020;56(1):2001494. https://doi.org/10.1183/13993003.01494-2020.
Sheehy LM. Considerations for Postacute rehabilitation for survivors of COVID-19. JMIR Public Health Surveill. 2020;6(2):e19462.
Schellhorn P, Klingel K, Burgstahler C. Return to sports after COVID-19 infection. Eur Heart J. 2020:ehaa448. https://doi.org/10.1093/eurheartj/ehaa448.
Korupolu R, Francisco GE, Levin H, Needham DM. Rehabilitation of critically ill COVID-19 survivors. J Int Soc Phys Rehabil Med. 2020;3(2):45.
Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf#:~:text=Using%20available%20preliminary%20data%2C,severe%20or%20critical%20disease. Accessed 19 Oct 2020.
Kuppalli K, Rasmussen AL. A glimpse into the eye of the COVID-19 cytokine storm. EBioMedicine. 2020;55:102789. https://doi.org/10.1016/j.ebiom.2020.102789.
Moore JB, June CH. Cytokine release syndrome in severe COVID-19. Science. 2020;368(6490):473–4. https://doi.org/10.1126/science.abb8925.
Liu J, Li S, Liu J, Liang B, Wang X, Wang H, et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020;55:102763.
Sollini M, Ciccarelli M, Cecconi M, Aghemo A, Morelli P, Gelardi F, et al. Vasculitis changes in COVID-19 survivors with persistent symptoms: an [18F]FDG-PET/CT study. Eur J Nucl Med Mol Imaging. 2020. https://doi.org/10.1007/s00259-020-05084-3.
Libby P, Lüscher T. COVID-19 is, in the end, an endothelial disease. Eur Heart J Eur Heart J. 2020;41:3038–44.
Temgoua MN, Endomba FT, Nkeck JR, Kenfack GU, Tochie JN, Essouma M. Coronavirus disease 2019 (COVID-19) as a multi-systemic disease and its impact in low- and middle-income countries (LMICs). SN Compr Clin Med. 2020;2:1377–87.
Nigeria Centre for Disease Control. National Interim Guidelines for Clinical Management of COVID-19. [Published online March 14th 2020]. Available from: https://reliefweb.int/report/nigeria/national-interim-guidelines-clinical-management-covid-19 Accessed 6 July 2020.
Mahase E. Covid-19:what do we know about "longcovid"? BMJ. 2020;370:m2815. https://doi.org/10.1136/bmj.m2815.
Acknowledgements
The authors would like to acknowledge the role of Mr. Babajide Sanwo-Olu, the Governor of Lagos State and Dr. Kadiri Hamza the Deputy Governor of Lagos State for providing leadership through the Incident Command System established to respond to the COVID-19 outbreak. The staff of the Lagos State, Directorate for Planning, Research and Statistics at the Ministry of Health, as well as the staff of the Post-COVID outpatient clinic at Mainland Hospital Yaba, Lagos State, Nigeria, were also supportive.
Dataset disclosures
The authors will like to confirm that, to the best of our knowledge, this cohort of patients have not been reported in any other submission on the subject of post-discharge clinical features of COVID-19 (or other phrase reflecting the subject of the study), by us or anyone else. However, some of the patients might have been included in a prior study reviewing the clinical symptoms on the admission and management of the first 32 cases of COVID-19 in Lagos State [7], as well as a subsequent study under peer-review, assessing factors associated with symptomatic presentation and increased length of hospitalisation in a cohort of 632 COVID-19 patients in Lagos State.
Funding
This work was supported by funding from the Lagos State Government. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
BO, OAE, and KW conceptualised the article. BO, OAE, and KW conducted the data analysis. BO, OAE, KW and AO1 drafted the article. BT, IA, AO2, and AA contributed significantly to the conception and design of the study. OA1, OA2 and AF, contributed significantly to the acquisition and interpretation of the data. AB and OO contributed significantly to the conception of the study and acquisition of the data. All authors approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Lagos State University Teaching Hospital Health Research Ethics Committee. Approval number: LREC/06/10/1345. Written consent was obtained from participants, and the study was conducted according to the principles set by the Declaration of Helsinki.
Consent for publication
Not Applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Osikomaiya, B., Erinoso, O., Wright, K.O. et al. ‘Long COVID’: persistent COVID-19 symptoms in survivors managed in Lagos State, Nigeria. BMC Infect Dis 21, 304 (2021). https://doi.org/10.1186/s12879-020-05716-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-020-05716-x