
Abstract
Background
Chlorhexidine gluconate (CHG) bathing of hospitalized patients may have benefit in reducing hospital-acquired bloodstream infections (HABSIs). However, the magnitude of effect, implementation fidelity, and patient-centered outcomes are unclear. In this meta-analysis, we examined the effect of CHG bathing on prevention of HABSIs and assessed fidelity to implementation of this behavioral intervention.
Methods
We undertook a meta-analysis by searching Medline, EMBASE, CINAHL, Scopus, and Cochrane’s CENTRAL registry from database inception through January 4, 2019 without language restrictions. We included randomized controlled trials, cluster randomized trials and quasi-experimental studies that evaluated the effect of CHG bathing versus a non-CHG comparator for prevention of HABSIs in any adult healthcare setting. Studies of pediatric patients, of pre-surgical CHG use, or without a non-CHG comparison arm were excluded. Outcomes of this study were HABSIs, patient-centered outcomes, such as patient comfort during the bath, and implementation fidelity assessed through five elements: adherence, exposure or dose, quality of the delivery, participant responsiveness, and program differentiation. Three authors independently extracted data and assessed study quality; a random-effects model was used.
Results
We included 26 studies with 861,546 patient-days and 5259 HABSIs. CHG bathing markedly reduced the risk of HABSIs (IRR = 0.59, 95% confidence interval [CI]: 0.52–0.68). The effect of CHG bathing was consistent within subgroups: randomized (0.67, 95% CI: 0.53–0.85) vs. non-randomized studies (0.54, 95% CI: 0.44–0.65), bundled (0.66, 95% CI: 0.62–0.70) vs. non-bundled interventions (0.51, 95% CI: 0.39–0.68), CHG impregnated wipes (0.63, 95% CI: 0.55–0.73) vs. CHG solution (0.41, 95% CI: 0.26–0.64), and intensive care unit (ICU) (0.58, 95% CI: 0.49–0.68) vs. non-ICU settings (0.56, 95% CI: 0.38–0.83). Only three studies reported all five measures of fidelity, and ten studies did not report any patient-centered outcomes.
Conclusions
Patient bathing with CHG significantly reduced the incidence of HABSIs in both ICU and non-ICU settings. Many studies did not report fidelity to the intervention or patient-centered outcomes. For sustainability and replicability essential for effective implementation, fidelity assessment that goes beyond whether a patient received an intervention or not should be standard practice particularly for complex behavioral interventions such as CHG bathing.
Trial registration
Study registration with PROSPERO CRD42015032523.
Similar content being viewed by others


Background
Hospital-acquired bloodstream infections (HABSIs) are associated with increased morbidity, mortality, length of hospital stay, and costs [1, 2]. Central line-associated bloodstream infections (CLABSIs) account for the vast majority of HABSIs [3]. In the past decade, a number of interventions have led to an overall decline in CLABSI rates in intensive care units (ICUs). These include catheter insertion bundles or checklists [4], disinfection of hubs and needleless connectors [5], and use of chlorhexidine gluconate (CHG) impregnated dressings [6]. More recently, bathing of patients with CHG has received attention as a novel strategy to prevent HABSIs, both CLABSIs and non-CLABSIs [7]. Bathing with CHG may reduce the risk of HABSI by lowering microbial burden on the patient’s skin and the hands of healthcare workers [8,9,10].
Although some studies have shown the efficacy of CHG bathing in reducing HABSIs, particularly in the ICU, there is considerable variation in the implementation of this behavioral intervention, especially ensuring intervention fidelity. Failure to ensure fidelity to this intervention due to the possible suboptimal compliance with daily CHG bathing can potentially lead to decreased susceptibility of bacteria to CHG and eventual development of resistance [11].
In addition, CHG studies have not addressed patient-centered outcomes [12]; these outcomes are particularly relevant for CHG bathing where the patient may be an active participant. Examples include patient comfort during bathing and CHG-related adverse events, such as skin irritation and dryness, which may affect patient acceptance of the intervention [13,14,15].
Current infection prevention literature lacks meta-analyses/systematic reviews assessing intervention fidelity and patient-centered outcomes among patients receiving CHG bathing. Given several studies on CHG bathing and its potential for reducing HABSIs, we undertook a systematic review and meta-analysis to examine 1) the magnitude of effect of CHG bathing in different settings, 2) fidelity to the intervention, and 3) patient-centered outcomes.
Methods
We conducted this systematic review and meta-analysis in conformity with PRISMA and MOOSE guidelines and registered the protocol with the PROSPERO: CRD42015032523 [16, 17].
Data sources and search strategy
With the assistance of a reference librarian (CMB), we conducted a search for CHG and hospital-acquired infection human studies published through January 4, 2019 without date or language restrictions. We searched Medline (via Ovid), EMBASE, CINAHL, Scopus, and Cochrane’s CENTRAL registry. We used controlled vocabulary or MeSH (Medical Subject Heading) terms in addition to keywords, including “Baths,” “Chlorhexidine,” “Disinfection,” “Soaps,” “Anti-Infective Agents,” “Treatment Outcome,” “Disinfectants,” “Cross Infection,” “Drug Resistance,” “Catheter-Related Infections,” and “Bacteria.” Additional records were identified by reviewing reference lists of included articles.
Study selection
Inclusion and exclusion criteria
Three authors (JCO, JSM, and PKG) assessed eligibility for inclusion of studies in this meta-analysis. Disagreements regarding study inclusion were resolved through discussion. We included randomized controlled trials (RCT), cluster randomized trials (CRT), and quasi-experimental studies that evaluated the effect of CHG bathing versus a non-CHG comparator for prevention of HABSIs in any adult healthcare setting. Studies that compared post-intervention rates with historical controls and review papers were excluded. We also excluded studies of pediatric patients, those that studied pre-surgical CHG use, and those without a non-CHG comparison arm.
Data extraction and quality assessment
Two authors (JCO and JSM) independently extracted the data. The following variables were abstracted: first author and year of publication, study design, country, setting, intervention, comparator, study duration, method used to assess fidelity, fidelity components (adherence, exposure or dose, quality of the delivery, participant responsiveness, and program differentiation), patient-centered outcomes assessed in the study, demographics, patient-days at risk, number of HABSIs in the intervention and comparator groups, and intervention bundling (i.e., CHG bathing combined with other interventions). In these bundled interventions, CHG bathing was the prominent component of the bundle, and we performed subgroup analyses comparing bundled vs. non-bundled interventions.
We assessed the quality of studies using a modified version of the Cochrane’s Risk of Bias tool [18]. The domains assessed were subject allocation (e.g., randomized vs. non-randomized), completeness of outcome data, method of outcome assessment (blinded or not), diagnostic criteria for bloodstream infection, and other sources of bias, such as exclusion of certain study subjects during the analysis and information bias during data collection. We qualitatively scored studies as “high” or “low” risk of bias in each of these domains. Three authors (JCO, JSM, and PKG) independently reviewed and assessed each study, and differences in assessments were reconciled via discussion. Reporting and publication bias was assessed using a funnel plot and Egger’s test.
Outcomes
The primary clinical outcome of interest was the incidence of HABSIs. The incidence rate ratio (IRR) of HABSIs was calculated as the ratio between the incidence rate (i.e., the number of bloodstream infections identified per 1000 patient-days) among patients treated with CHG vs. that of patients in the control group, or the ratio of the incidence rate of bloodstream infections before and after implementation of CHG bathing. We collected data on causative microorganisms of reported HABSIs and categorized the organisms as fungi (mainly yeasts), gram-negative bacteria, coagulase-negative staphylococci (CoNS), and gram-positive bacteria other than CoNS. We treated CoNS as a separate category as it is a common contaminant [19].
We also assessed intervention fidelity. Fidelity is defined as “the demonstration that an experimental manipulation is conducted as planned” [20]. Dane and Schneider’s proposed five components of fidelity, including adherence, exposure or dose, quality of the delivery, participant responsiveness, and program differentiation, were assessed [21].
Adherence
Adherence measures the extent to which the implemented program elements align with the intervention as outlined in the protocol and can be assessed by identifying the primary components of a given intervention. For CHG bathing, this is whether bathing actually occurs and could have been assessed through direct observations of bathing, assessment of CHG purchase, or usage data.
Exposure or dose
This measures how much of the program content actually reaches the intended participants (i.e., healthcare workers conducting the CHG baths). For example, program content can include the number of CHG training sessions including their duration and frequency that are completed by healthcare workers prior to implementing CHG use. Exposure does not refer to how much CHG a patient was exposed to during the bath, which is assessed by both adherence and quality of delivery.
Quality of the delivery
This assesses the processes and content of an intervention. For CHG bathing, quality of the delivery can be assessed by conducting direct observations of the process to assess if all the bathing steps are followed.
Participant responsiveness
Measuring how engaged participants are in a CHG intervention and their perceptions of the intervention involves obtaining feedback from providers administering baths and patients receiving the baths through surveys or interviews.
Program differentiation
This assesses the specific ways by which researchers carried out interventions and any unique characteristics. For example, studies should unambiguously report how unit leadership was engaged, if audits were conducted, or how feedback was provided to staff conducting CHG baths. In addition, studies need to clearly state the CHG product used and in what concentration.
In addition, we examined whether studies assessed or reported patient-centered outcomes. These may include major barriers to bathing, such as patient comfort during the bath, adverse events related to CHG and CHG’s lack of a fragrant scent which has especially been associated with patient refusal of CHG baths [13,14,15]. These outcomes can be passively reported by patients or actively elicited. The patient-centered outcomes we assessed in this study included 1) patient discomfort; 2) smell of the CHG soap and whether this was acceptable to patients; 3) patient education about CHG bathing and 4) adverse events related to CHG bathing, such as skin rashes, skin dryness and pruritus. These were generated through several collaborative discussions with a panel of seven patients at our institution, all of whom have experience with healthcare-associated infections (HAIs) and CHG bathing.
Statistical methods
The effect of CHG bathing was calculated as the IRR for each study using a continuity correction. The DerSimonian and Laird method was used to obtain estimates of the average intervention effect and the heterogeneity of intervention effects across studies using a random-effects model [22]. We evaluated heterogeneity of the IRR across studies using the I2 statistic [23]. As a robustness check, we also estimated the parameters of the random-effects logistic regression model via maximum likelihood. We calculated infection risk using patient-days at risk or venous catheter-days as the denominator depending on whichever the study provided with a preference for catheter-days if both were provided and the outcome was limited to patients with venous access devices. We decided to combine studies that used patient-days at risk and those that used venous catheter-days at risk as the denominator because conducting the analyses separately did not make a difference in terms of the CHG effect. Moreover, the use of patient days in some studies would bias the results towards the null. One study did not report person-time data (patient-days at risk or venous catheter-days) and was omitted from the analysis using person-time as the denominator [24]. To assess the effect of excluding this study, we also conducted a separate analysis using number of patients as the denominator for those studies that reported this information. We conducted subgroup analyses that were defined a priori for the following groups: RCT or CRT vs. non-randomized studies, bundled vs. non-bundled interventions, CHG wipes vs. CHG solution, and ICU vs. non-ICU setting.
We performed statistical analyses using the command “METAN,” with the cc option in Stata software, version 14.0 (Stata Corp. College Station, Texas) and PROC GLIMMIX in SAS 9.4 (SAS Institute Inc., Cary, North Carolina).
Results
The search yielded 788 articles of which 179 were duplicates and were excluded. We screened 609 articles. We excluded 420 studies after title and abstract review leaving 189 articles for full article review, after which 163 were excluded. This left 26 articles for the meta-analysis (Fig. 1).

Study selection flow diagram adapted from the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)
Eighteen studies were non-randomized, and we classified them as quasi-experimental studies; eight were RCTs or CRTs. Most were single-center studies (n = 19). Nineteen were conducted in the ICU; the remaining seven were conducted in various settings, such as general medical wards, burns unit, geriatric chronic care units, and long-term acute care hospitals.
The most commonly used product for bathing was the non-rinse 2% CHG wipe (18/27) [8, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41]. All but two studies obtained wipes from Sage Product LLC, Cary, IL. For the two studies that did not use Sage cloths, one study used a similar cloth product manufactured by G70 Antisepsis, Mexico City, Mexico [37], and the other used 2% CHG cloths produced by their local pharmacy department [27]. Five studies used a 4% CHG liquid solution with rinsing [24, 42,43,44,45]. Two studies used a 2% CHG solution that was locally made. In one study, the 2% CHG solution was prepared by diluting Bactoshield chlorhexidine 4% Surgical Scrub (STERIS, Mentor, OH) [46]. The other study prepared 2% CHG solution by diluting bulk 4% CHG (Betasept; Purdue Pharma) 1:2 with tap water [47]. Another study used a 0.9% CHG solution in sterile water [48]. Nine studies used bundled interventions [24, 25, 28, 33, 35, 37, 43, 45, 48] incorporating other infection control interventions, such as reinforcement of hand hygiene during the study period, intranasal decolonization with mupirocin, and universal gloving and gowning by healthcare providers. The extent and timing of implementation of these interventions relative to CHG bathing were not described in detail in any of the studies. Details of characteristics of included studies are presented in Additional file 1: Table S1.
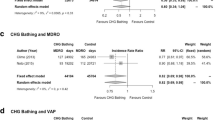
There were 5259 HABSIs and 861,546 patient-days. Overall, the incidence rate of HABSI per 1000 patient days was 4.4 (95% confidence interval [CI]: 4.2–4.6) in the CHG group and 7.5 (95% CI: 7.3–7.8) in the comparator group. Figure 2 summarizes the effect of CHG bathing on HABSI. Sixteen studies made a distinction between CLABSI and other bloodstream infections. Among these studies, 75% of HABSI in the CHG group and 71% in the comparator group were CLABSIs. There was moderate heterogeneity in the effect of CHG bathing across studies (τ2 = 0.17; I2 = 50.3%, p = 0.002) [23]. The random-effects IRR for CHG bathing was 0.59 (95% CI: 0.52–0.68); in other words, the incidence rate of HABSIs was reduced by approximately 40% (95% CI: 32–48%).

Forest plot showing that chlorhexidine bathing reduced the incidence of hospital acquired bloodstream infections; the dotted line indicates the mean estimated relative risk
The effect of CHG bathing was consistent within subgroups: randomized (0.67, 95% CI: 0.53–0.85) vs. non-randomized studies (0.54, 95% CI: 0.44–0.65), bundled (0.66, 95% CI: 0.62–0.70) vs. non-bundled interventions (0.51, 95% CI: 0.39–0.68), CHG impregnated wipes (0.63, 95% CI: 0.55–0.73) vs. CHG solution (0.41, 95% CI: 0.26–0.64), and ICU (0.58, 95% CI: 0.49–0.68) vs. non-ICU settings (0.56, 95% CI: 0.38–0.83) (Additional file 2: Figures S1-S4). A meta-regression analysis to examine differences between these subgroups showed that the stratified estimates did not significantly differ between subgroups (Additional file 3: Table S3).
Analysis using number of patients as the denominator for a subset of studies that provided this data did not change our findings (IRR = 0.59, 95% CI: 0.51–0.68, I2 = 60.5%, p < 0.001).
Only three studies reported all five measures of fidelity [34, 35, 37]. Twelve percent (3/26) of the studies reported four measures of fidelity, 15% (4/26) reported three measures, 27% (7/26) reported two measures, and 35% (9/26) reported one fidelity measure. The most frequently missed fidelity measures were participant responsiveness (21/26) and exposure or dose (17/26), while program differentiation was not missed by any study. Most studies (16/26, 62%) did not report how fidelity was assessed, and those that did reported measures used to assess adherence, quality of the delivery, and participant responsiveness (Additional file 4: Table S2).
Ten studies did not report any patient-centered outcomes. The remaining 16 studies described monitoring of adverse events to CHG as reported by patients and/or from medical records. Of these 16, eight studies reported data on adverse events, such as skin rashes, skin dryness, and pruritus [28, 31, 32, 35, 38, 43, 46, 47].
The risk of bias for each of the studies is reported in Additional file 1: Table S1. Overall, most of the studies were appraised as being at low risk of bias in the majority of the five domains. The main sources of potential bias came from allocation (pre-post designs), presence of potentially confounding interventions such as mupirocin nasal decolonization and non-standard definitions for infection. Two studies did not provide their definition for bloodstream infection [34, 47]. Although visual inspection of the funnel plot (Fig. 3) suggested the presence of publication bias, the Egger’s test did not show evidence of publication bias (Egger’s test, p = 0.80).

Funnel plot to assess publication bias
Microbiology—HABSI causative organisms
Twenty-three studies (85%) reported data on the causative organisms of HABSIs. Beneficial impact of CHG on gram-positive bacteria other than CoNS was reported in ten (43%) studies; impact of CHG on CoNS in eight (35%) studies; impact of CHG on gram-negative bacteria in eight (35%) studies; and beneficial impact of CHG on fungi (Candida species) in five (22%) of the studies.
Discussion
We found that CHG bathing of patients is associated with a consistent, clinically important, and statistically significant reduction in the risk of HABSIs. This effect was consistent across study settings, study designs, whether the intervention was bundled or not, and whether a no-rinse approach (i.e., CHG-impregnated wipes) or CHG solution requiring rinsing was used. The finding that the effect of CHG was present even with the rinsing approach was interesting because the literature suggests that rinsing results in lower levels of CHG on the skin [49, 50]. However, a certain amount of CHG remains even with rinsing, and this might account for the observed effect with rinsing [51].
There is considerable variation in the implementation of CHG bathing. Most CHG intervention studies included in our analysis failed to report measures of fidelity. Given the complexity of effectively implementing a behavioral intervention in healthcare settings, a systematic, careful assessment of fidelity is essential. The three studies that reported all fidelity components heavily engaged their frontline staff in rolling out the intervention and conducted direct observations of the bathing process [34, 35, 37]. Involvement of frontline staff in CHG bathing rollout has been shown to be important in ensuring success and sustainability of CHG bathing [14]. Many studies tended to report adherence and quality of the delivery fidelity measures. Although these are necessary for ensuring that the intervention is performed at a given facility, they are not sufficient for replication of the studies in other settings. Therefore, reporting adherence and quality of the delivery alone without the other three fidelity measures (i.e., exposure or dose, participant responsiveness and program differentiation) limits the generalizability of study findings.
As an increasing number of institutions adopt CHG bathing as an important horizontal pathogen-independent infection prevention strategy, standardization is an essential step. As most studies were not RCTs, thus precluding a robust assessment of causality, future research should focus on understanding and reporting factors that facilitate or impede high-fidelity implementation.
Our study has implications for clinical practice. Our results show that CHG bathing should be considered for adoption by institutions as part of a comprehensive HABSI reduction strategy that includes careful monitoring of adherence to the bathing protocol.
Our study extends the findings of previous reviews. Unlike other previous reviews [52,53,54,55,56,57], including two conducted by our group [6, 7], this analysis includes a rigorous assessment of implementation as well as patient-centered factors. We found that many studies did not report assessment of any patient outcomes, and those that did only reported adverse events, such as skin rashes, skin dryness, and pruritus. CHG bathing interventions should incorporate comprehensive assessment of patient-centered outcomes, such as patient comfort during the bath and perceptions regarding the smell and feel of the chosen product in addition to adverse cutaneous effects – all of these factors have been reported to affect patient acceptance of CHG bathing [14]. This is especially important in light of the recent FDA advisory on the risk of rare allergic skin reactions to CHG [58].
Our study also showed that CHG bathing impacted all microorganisms responsible for HABSIs as expected from the broad-spectrum nature of CHG [59]. One of the very few negative ICU studies that did not show an effect of CHG bathing had serious limitations [39]. The study was a single-center unblinded study that used a composite endpoint of all HAIs rather than HABSIs for which there is a high biological plausibility for CHG’s role in preventing infections.
Although not assessed in our study, CHG cost is an important factor that warrants mention. CHG bathing can lead to substantial cost savings for institutions in which it is implemented. A cost analysis by Holder & Zellinger et al. showed that implementing CHG bathing in all ICUs of 93-ICU-bed hospital would save the hospital $1.56 million per year [34]. Dixon and Carver showed implementing CHG bathing in a nine-bed surgical ICU compared to ordinary soap and water was associated with $728,820 in cost savings over a 17-month intervention period. [30]. These studies suggest that considering the potentially prevented HAIs, the use of CHG is associated with cost savings.
Another important consideration before implementing CHG is the potential of development of bacterial resistance to CHG. Examination of current literature indicates that the evidence for the development of resistance to CHG has been mixed. An eight-year prospective study of MRSA in a surgical ICU showed a trend towards increasing prevalence of the resistance gene qacA/B [60]. Another ICU study showed that 2 and 7% of MRSA isolates were qacA/B and smr positive, respectively [61]. Using published data from clinical isolates and comparing their CHG minimum inhibitory concentrations with epidemiological cut-off values, Kampf showed CHG resistance by certain bacteria but not others [11]. On the other hand, a multicenter cluster randomized ICU study did not show CHG resistance [29]. Therefore, there is still clinical equipoise regarding bacterial resistance to CHG.
Our study has limitations. As this meta-analysis focused on adult patients by design, its findings may not be applicable to pediatric populations. There was a high degree of heterogeneity in the studies included in our analysis. We observed that heterogeneity came mainly from studies that were non-bundled rather than from bundled ones. In contrast to our findings, previous studies have shown that bundled interventions have a greater effect on the incidence of CLABSIs than non-bundled interventions [62, 63]. The heterogeneity observed with regard to non-bundled interventions and the fact that our study pooled all HABSIs could explain this difference. Infection control “care bundles,” such as the Institute for Healthcare Improvement Central Line Bundle [64], have clearly defined bundle components and are more likely to be implemented in a similar fashion across facilities. A high degree of compliance is needed for bundled interventions to be effective [65]. For CHG studies (both bundled and non-bundled), there is likely to be variation in CHG bathing processes, products used, and populations under study. We employed a random-effects model and explored potential causes of heterogeneity in depth. In some studies, CHG bathing was instituted as a quality improvement intervention in combination with other concurrent interventions, such as screening for resistant bacteria [24, 32, 42] or reinforcement of hand hygiene practices [37, 43,44,45]. The independent impact of these concurrent interventions cannot be accounted for in our meta-analysis. Another limitation is that the included studies defined CLABSIs differently and most did not provide information on the site of origin. Only a few studies reported bloodstream as a source of the HABSI, in which case data for bloodstream was extracted. In addition, we could not rank interventions based on their fidelity measurements, because no published studies examined which of the five elements are most important. Some are more likely to influence study replicability (dose, differentiation, quality), while others are more likely to influence intervention sustainability (participant responsiveness, adherence) [20, 66]. Regardless, interventions should aim at incorporating all five, and future research should examine the importance of each element individually.
Conclusion
We found that patient bathing with CHG significantly reduced the incidence of HABSIs in both ICU and non-ICU settings. However, the strength of evidence for non-ICU use was lower. As a horizontal infection prevention strategy that covers a broad spectrum of pathogens, CHG bathing is an effective, relatively low-cost intervention that should be implemented with high fidelity to achieve maximum impact. For sustainability and replicability essential for effective implementation, fidelity assessment that goes beyond whether a patient received an intervention or not should be standard practice particularly for complex behavioral interventions such as CHG bathing.
Abbreviations
- CHG:
-
Chlorhexidine gluconate
- CI:
-
Confidence interval
- CLABSI:
-
Central line-associated bloodstream infections
- CoNS:
-
Coagulase-negative staphylococci
- CRT:
-
Cluster randomized trials
- FDA:
-
Food and Drug Administration
- HABSIs:
-
Hospital-acquired bloodstream infections
- HAIs:
-
Healthcare-associated infections
- ICU:
-
Intensive care unit
- IRR:
-
Incidence rate ratio
- RCT:
-
Randomized controlled trials
References
Stevens V, Geiger K, Concannon C, Nelson RE, Brown J, Dumyati G. Inpatient costs, mortality and 30-day re-admission in patients with central-line-associated bloodstream infections. Clin Microbiol Infect. 2014;20(5):O318–24.
Cassini A, Plachouras D, Eckmanns T, Abu Sin M, Blank HP, Ducomble T, et al. Burden of six healthcare-associated infections on European population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med. 2016;13(10):e1002150.
Raad I, Hanna H, Maki D. Intravascular catheter-related infections: advances in diagnosis, prevention, and management. Lancet Infect Dis. 2007;7(10):645–57.
DePalo VA, McNicoll L, Cornell M, Rocha JM, Adams L, Pronovost PJ. The Rhode Island ICU collaborative: a model for reducing central line-associated bloodstream infection and ventilator-associated pneumonia statewide. Qual Saf Health Care. 2010;19(6):555–61.
Simmons S, Bryson C, Porter S. “Scrub the hub”: cleaning duration and reduction in bacterial load on central venous catheters. Crit Care Nurs Q. 2011;34(1):31–5.
Safdar N, O'Horo JC, Ghufran A, Bearden A, Didier ME, Chateau D, Maki DG. Chlorhexidine-impregnated dressing for prevention of catheter-related bloodstream infection: a meta-analysis. Crit Care Med. 2014;42(7):1703–13.
O'Horo JC, Silva GL, Munoz-Price LS, Safdar N. The efficacy of daily bathing with chlorhexidine for reducing healthcare-associated bloodstream infections: a meta-analysis. Infect Control Hosp Epidemiol. 2012;33(3):257–67.
Bleasdale SC, Trick WE, Gonzalez IM, Lyles RD, Hayden MK, Weinstein RA. Effectiveness of chlorhexidine bathing to reduce catheter-associated bloodstream infections in medical intensive care unit patients. Arch Intern Med. 2007;167(19):2073–9.
Cassir N, Papazian L, Fournier PE, Raoult D, La Scola B. Insights into bacterial colonization of intensive care patients’ skin: the effect of chlorhexidine daily bathing. Eur J Clin Microbiol Infect Dis. 2015;34(5):999–1004.
Vernon MO, Hayden MK, Trick WE, Hayes RA, Blom DW, Weinstein RA, et al. Chlorhexidine gluconate to cleanse patients in a medical intensive care unit: the effectiveness of source control to reduce the bioburden of vancomycin-resistant enterococci. Arch Intern Med. 2006;166(3):306–12.
Kampf G. Acquired resistance to chlorhexidine – is it time to establish an ‘antiseptic stewardship’ initiative. J Hosp Infect. 2016;94(3):213–27.
Frank L, Basch E, Selby JV. Institute P-COR. The PCORI perspective on patient-centered outcomes research. JAMA. 2014;312(15):1513–4.
Hines AG, Nuss S, Rupp ME, Lyden E, Tyner K, Hewlett A. Chlorhexidine bathing of hospitalized patients: beliefs and practices of nurses and patient care technicians, and potential barriers to compliance. Infect Control Hosp Epidemiol. 2015;36(8):993–4.
Musuuza JS, Roberts TJ, Carayon P, Safdar N. Assessing the sustainability of daily chlorhexidine bathing in the intensive care unit of a Veteran’s hospital by examining nurses’ perspectives and experiences. BMC Infect Dis. 2017;17(1):75.
Caya T, Musuuza J, Yanke E, Schmitz M, Anderson B, Carayon P, et al. Using a systems engineering initiative for patient safety to evaluate a hospital-wide daily chlorhexidine bathing intervention. J Nurs Care Qual. 2015;30(4):337–44.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–41.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clin Microbiol Rev. 2014;27(4):870–926.
Dumas JE, Lynch AM, Laughlin JE, Phillips Smith E, Prinz RJ. Promoting intervention fidelity. Conceptual issues, methods, and preliminary results from the EARLY ALLIANCE prevention trial. Am J Prev Med. 2001;20(1 Suppl):38–47.
Dane AV, Schneider BH. Program integrity in primary and early secondary prevention: are implementation effects out of control? Clin Psychol Rev. 1998;18(1):23–45.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Willis GC, Ooi ST, Foo ML, Ong PL, Tan BBC, Li D, et al. The effect of daily chlorhexidine baths on nosocomial meticillin-resistant Staphylococcus aureus infection in MRSA-colonized patients admitted to general wards. Int J Infect Control. 2015;11(4):1–7.
Abboud CS, de Souza EE, Zandonadi EC, Borges LS, Miglioli L, Monaco FC, et al. Carbapenem-resistant Enterobacteriaceae on a cardiac surgery intensive care unit: successful measures for infection control. J Hosp Infect. 2016;94(1):60–4.
Amirov CM, Binns MA, Jacob LE, Candon HL. Impact of chlorhexidine bathing on methicillin-resistant Staphylococcus aureus incidence in an endemic chronic care setting: a randomized controlled trial. Am J Infect Control. 2017;45(3):298–300.
Boonyasiri A, Thaisiam P, Permpikul C, Judaeng T, Suiwongsa B, Apiradeewajeset N, et al. Effectiveness of chlorhexidine wipes for the prevention of multidrug-resistant bacterial colonization and hospital-acquired infections in intensive care unit patients: a randomized trial in Thailand. Infect Control Hosp Epidemiol. 2016;37(3):245–53.
Cassir N, Thomas G, Hraiech S, Brunet J, Fournier PE, La Scola B, et al. Chlorhexidine daily bathing: impact on health care-associated infections caused by gram-negative bacteria. Am J Infect Control. 2015;43(6):640–3.
Climo MW, Yokoe DS, Warren DK, Perl TM, Bolon M, Herwaldt LA, et al. Effect of daily chlorhexidine bathing on hospital-acquired infection. N Engl J Med. 2013;368(6):533–42.
Dixon JM, Carver RL. Daily chlorohexidine gluconate bathing with impregnated cloths results in statistically significant reduction in central line-associated bloodstream infections. Am J Infect Control. 2010;38(10):817–21.
Duszynska W, Adamik B, Lentka-Bera K, Kulpa K, Nieckula-Schwarz A, Litwin A, et al. Effect of universal chlorhexidine decolonisation on the infection rate in intensive care patients. Anaesthesiol Intensive Ther. 2017;49(1):28–33.
Evans HL, Dellit TH, Chan J, Nathens AB, Maier RV, Cuschieri J, et al. Effect of chlorhexidine whole-body bathing on hospital-acquired infections among trauma patients. Arch Surg. 2010;145(3):240–6.
Hayden MK, Lin MY, Lolans K, Weiner S, Blom D, Moore NM, et al. Prevention of colonization and infection by Klebsiella pneumoniae carbapenemase-producing enterobacteriaceae in long-term acute-care hospitals. Clin Infect Dis. 2015;60(8):1153–61.
Holder C, Zellinger M. Daily bathing with chlorhexidine in the ICU to prevent central line--associated bloodstream infections. J Clin Outcomes Manag. 2009;16(11):509–13.
Huang SS, Septimus E, Kleinman K, Moody J, Hickok J, Avery TR, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368(24):2255–65.
Kassakian SZ, Mermel LA, Jefferson JA, Parenteau SL, Machan JT. Impact of chlorhexidine bathing on hospital-acquired infections among general medical patients. Infect Control Hosp Epidemiol. 2011;32(3):238–43.
Martínez-Reséndez MF, Garza-González E, Mendoza-Olazaran S, Herrera-Guerra A, Rodríguez-López JM, Pérez-Rodriguez E, et al. Impact of daily chlorhexidine baths and hand hygiene compliance on nosocomial infection rates in critically ill patients. Am J Infect Control. 2014;42(7):713–7.
Montecalvo MA, McKenna D, Yarrish R, Mack L, Maguire G, Haas J, et al. Chlorhexidine bathing to reduce central venous catheter-associated bloodstream infection: impact and sustainability. Am J Med. 2012;125(5):505–11.
Noto MJ, Domenico HJ, Byrne DW, Talbot T, Rice TW, Bernard GR, et al. Chlorhexidine bathing and health care-associated infections: a randomized clinical trial. JAMA. 2015;313(4):369–78.
Popovich KJ, Hota B, Hayes R, Weinstein RA, Hayden MK. Effectiveness of routine patient cleansing with chlorhexidine gluconate for infection prevention in the medical intensive care unit. Infect Control Hosp Epidemiol. 2009;30(10):959–63.
Popovich KJ, Hota B, Hayes R, Weinstein RA, Hayden MK. Daily skin cleansing with chlorhexidine did not reduce the rate of central-line associated bloodstream infection in a surgical intensive care unit. Intensive Care Med. 2010;36(5):854–8.
Borer A, Gilad J, Porat N, Megrelesvilli R, Saidel-Odes L, Peled N, et al. Impact of 4% chlorhexidine whole-body washing on multidrug-resistant Acinetobacter baumannii skin colonisation among patients in a medical intensive care unit. J Hosp Infect. 2007;67(2):149–55.
Camus C, Bellissant E, Sebille V, Perrotin D, Garo B, Legras A, et al. Prevention of acquired infections in intubated patients with the combination of two decontamination regimens. Crit Care Med. 2005;33(2):307–14.
Climo MW, Sepkowitz KA, Zuccotti G, Fraser VJ, Warren DK, Perl TM, et al. The effect of daily bathing with chlorhexidine on the acquisition of methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, and healthcare-associated bloodstream infections: results of a quasi-experimental multicenter trial. Crit Care Med. 2009;37(6):1858–65.
Gould IM, MacKenzie FM, MacLennan G, Pacitti D, Watson EJ, Noble DW. Topical antimicrobials in combination with admission screening and barrier precautions to control endemic methicillin-resistant Staphylococcus aureus in an intensive care unit. Int J Antimicrob Agents. 2007;29(5):536–43.
Swan JT, Ashton CM, Bui LN, Pham VP, Shirkey BA, Blackshear JE, et al. Effect of chlorhexidine bathing every other day on prevention of hospital-acquired infections in the surgical ICU: a single-center, randomized controlled trial. Crit Care Med. 2016;44(10):1822–32.
Munoz-Price LS, Hota B, Stemer A, Weinstein RA. Prevention of bloodstream infections by use of daily chlorhexidine baths for patients at a long-term acute care hospital. Infect Control Hosp Epidemiol. 2009;30(11):1031–5.
Popp JA, Layon AJ, Nappo R, Richards WT, Mozingo DW. Hospital-acquired infections and thermally injured patients: chlorhexidine gluconate baths work. Am J Infect Control. 2014;42(2):129–32.
Edmiston CE, Seabrook GR, Johnson CP, Paulson DS, Beausoleil CM. Comparative of a new and innovative 2% chlorhexidine gluconate-impregnated cloth with 4% chlorhexidine gluconate as topical antiseptic for preparation of the skin prior to surgery. Am J Infect Control. 2007;35(2):89–96.
Edmiston CE, Krepel CJ, Seabrook GR, Lewis BD, Brown KR, Towne JB. Preoperative shower revisited: can high topical antiseptic levels be achieved on the skin surface before surgical admission? J Am Coll Surg. 2008;207(2):233–9.
Rhee Y, Palmer LJ, Okamoto K, Gemunden S, Hammouda K, Kemble SK, et al. Differential effects of chlorhexidine skin cleansing methods on residual chlorhexidine skin concentrations and bacterial recovery. Infect Control Hosp Epidemiol. 2018;39(4):405–11.
Frost SA, Alogso MC, Metcalfe L, Lynch JM, Hunt L, Sanghavi R, et al. Chlorhexidine bathing and health care-associated infections among adult intensive care patients: a systematic review and meta-analysis. Crit Care. 2016;20(1):379.
Afonso E, Blot K, Blot S. Prevention of hospital-acquired bloodstream infections through chlorhexidine gluconate-impregnated washcloth bathing in intensive care units: a systematic review and meta-analysis of randomised crossover trials. Euro Surveill. 2016;21(46). https://doi.org/10.2807/1560-7917.ES.2016.21.46.30400.
Chen W, Cao Q, Li S, Li H, Zhang W. Impact of daily bathing with chlorhexidine gluconate on ventilator associated pneumonia in intensive care units: a meta-analysis. J Thorac Dis. 2015;7(4):746–53.
Choi EY, Park DA, Kim HJ, Park J. Efficacy of chlorhexidine bathing for reducing healthcare associated bloodstream infections: a meta-analysis. Ann Intensive Care. 2015;5(1):31.
Kim HY, Lee WK, Na S, Roh YH, Shin CS, Kim J. The effects of chlorhexidine gluconate bathing on health care-associated infection in intensive care units: a meta-analysis. J Crit Care. 2016;32:126–37.
Frost SA, Hou YC, Lombardo L, Metcalfe L, Lynch JM, Hunt L, et al. Evidence for the effectiveness of chlorhexidine bathing and health care-associated infections among adult intensive care patients: a trial sequential meta-analysis. BMC Infect Dis. 2018;18(1):679.
U.S Food and Drug Administration. FDA drug safety communication: FDA warns about rare but serious allergic reactions with the skin antiseptic chlorhexidine gluconate. 2017. https://www.fda.gov/Drugs/DrugSafety/ucm530975.htm. Accessed 9 Apr 2019.
Milstone AM, Passaretti CL, Perl TM. Chlorhexidine: expanding the armamentarium for infection control and prevention. Clin Infect Dis. 2008;46(2):274–81.
Warren DK, Prager M, Munigala S, Wallace MA, Kennedy CR, Bommarito KM, et al. Prevalence of qacA/B genes and mupirocin resistance among methicillin-resistant Staphylococcus aureus (MRSA) isolates in the setting of chlorhexidine bathing without mupirocin. Infect Control Hosp Epidemiol. 2016;37(5):590–7.
Longtin J, Seah C, Siebert K, McGeer A, Simor A, Longtin Y, et al. Distribution of antiseptic resistance genes qacA, qacB, and smr in methicillin-resistant Staphylococcus aureus isolated in Toronto, Canada, from 2005 to 2009. Antimicrob Agents Chemother. 2011;55(6):2999–3001.
Blot K, Bergs J, Vogelaers D, Blot S, Vandijck D. Prevention of central line–associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis. Clin Infect Dis. 2014;59(1):96–105.
Ista E, van der Hoven B, Kornelisse RF, van der Starre C, Vos MC, Boersma E, et al. Effectiveness of insertion and maintenance bundles to prevent central-line-associated bloodstream infections in critically ill patients of all ages: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(6):724–34.
Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The 100,000 lives campaign: setting a goal and a deadline for improving health care quality. JAMA. 2006;295(3):324–7.
Furuya EY, Dick A, Perencevich EN, Pogorzelska M, Goldmann D, Stone PW. Central line bundle implementation in US intensive care units and impact on bloodstream infections. PLoS One. 2011;6(1):e15452.
Henggeler SW, Melton GB, Brondino MJ, Scherer DG, Hanley JH. Multisystemic therapy with violent and chronic juvenile offenders and their families: the role of treatment fidelity in successful dissemination. J Consult Clin Psychol. 1997;65(5):821–33.
Acknowledgements
Not applicable.
Funding
This work was supported by from the Agency for Healthcare Research and Quality [R18HS024039] and the United States Veterans Affairs (VA) National Center for Patient Safety Center of Inquiry. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality or those of the U.S. Department of Veterans Affairs or the United States Government. The funding sources did not have any role in the study design, collection, analysis, and interpretation of data or in writing of the manuscript.
Availability of data and materials
All data used in analysis of this manuscript is freely available by contacting the corresponding author.
Author information
Authors and Affiliations
Contributions
NS obtained funding and conceptualised the study. JSM conducted statistical analysis and wrote first draft. REG provided statistical expertise during data analysis. JCO, JSM, and PKG conduced screening of studies and bias assessment. JSM, JCO, and NS wrote the manuscript. CMB drafted strategy and methodology, and conducted searches for studies. JSM conducted patient peer discussions, and MAK coordinated patient peer activities and served as a liaison between study team and patient peers. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable (review of published literature).
Consent for publication
Not applicable.
Competing interests
Investigators will receive only normal scholarly gains from taking part in this study. The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Table S1. Characteristics of included studies. (DOCX 57 kb)
Additional file 2:
Figure S1. Effect of chlorhexidine gluconate bathing comparing Randomized vs. non-randomized studies. Figure S2. Effect of chlorhexidine gluconate bathing comparing bundled vs. non-bundled interventions. Figure S3. Effect of chlorhexidine gluconate bathing comparing 2% chlorhexidine impregnated wipes vs. 4% CHG solution. Figure S4. Effect of chlorhexidine gluconate bathing comparing intensive care unit (ICU) vs. non-ICU settings. (PDF 164 kb)
Additional file 3:
Table S3. Meta-regression analysis showed that the stratified estimates did not significantly differ between subgroups. (DOCX 14 kb)
Additional file 4:
Table S2. Fidelity assessment. (DOCX 47 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Musuuza, J.S., Guru, P.K., O’Horo, J.C. et al. The impact of chlorhexidine bathing on hospital-acquired bloodstream infections: a systematic review and meta-analysis. BMC Infect Dis 19, 416 (2019). https://doi.org/10.1186/s12879-019-4002-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-019-4002-7