
Abstract
Background
War-wounded civilians in Middle East countries are at risk of post-traumatic osteomyelitis (PTO). We aimed to describe and compare the bacterial etiology and proportion of first-line antibiotics resistant bacteria (FLAR) among PTO cases in civilians from Syria, Iraq and Yemen admitted to the reconstructive surgical program of Médecins Sans Frontières (MSF) in Amman, Jordan, and to identify risk factors for developing PTO with FLAR bacteria.
Methods
We retrospectively analyzed the laboratory database of the MSF program. Inclusion criteria were: patients from Iraq, Yemen or Syria, admitted to the Amman MSF program between October 2006 and December 2016, with at least one bone biopsy sample culture result. Only bone samples taken during first orthopedic surgery were included in the analysis. To assess factors associated with FLAR infection, logistic regression was used to estimate odds ratio (ORs) and 95% confidence intervals (CI).
Results
558 (76.7%) among 727 patients included had ≥1 positive culture results. 318 were from Iraq, 140 from Syria and 100 from Yemen. Median time since injury was 19 months [IQR 8–40]. Among the 732 different bacterial isolates, we identified 228 Enterobacteriaceae (31.5%), 193 Staphylococcus aureus (26.3%), 99 Pseudomonas aeruginosa (13.5%), and 21 Acinetobacter baumanii (2.8%). Three hundred and sixty four isolates were FLAR: 86.2% of Enterobacteriaceae, 53.4% of Pseudomonas aeruginosa, 60.5% of S. aureus and 45% of Acinetobacter baumannii. There was no difference in bacterial etiology or proportion of FLAR according to the country of origin. In multivariate analysis, a FLAR infection was associated with an infection of the lower extremity, with a time since the injury ≤12 months compared with time > 30 months and with more than 3 previous surgeries.
Conclusions
Enterobacteriaceae were frequently involved in PTO in war wounded civilians from Iraq, Yemen and Syria between 2006 and 2016. Proportion of FLAR was high, particularly among Enterobacteriaceae, regardless of country of origin.
Similar content being viewed by others


Background
Post-traumatic and diabetes mellitus-related infections are the most frequent causes of osteomyelitis [1, 2]. Two retrospective studies found a rate of post-traumatic osteomyelitis (PTO) after limb fracture of 2.5 and 1.5%, but incidence of PTO depends on the host condition and on the severity of injury; it is much higher after open fractures [3, 4]. The gold standard for diagnosis of PTO is culture of bone biopsy, as deep wound tissue culture lacks sensitivity and specificity [5]. The most frequent causative pathogen is Staphylococcus aureus, involved in 36.2 to 57.0% of cases [2, 4,5,6]. Management of PTO is complex and combines initial aggressive debridement, prolonged antibiotic therapy and often reconstruction of bone or soft tissue defects [7].
Since 2003, Middle Eastern countries have experienced many conflicts, leaving thousands of civilians injured particularly in Iraq and more recently in Syria and Yemen. The majority of injuries involves extremities and is caused by bomb blasts and ballistic trauma. Due to the damage to connective tissues with open fractures, contamination with environmental debris and difficult access to timely optimal surgical care, PTO is a frequent complication of injuries in the context of conflict. This has been previously documented in the reconstructive surgical program set up by Médecins Sans Frontières (MSF) in Amman. Among 1353 war-wounded civilians with bone injury admitted to the program (where bone culture are taken routinely on initial surgery), 63.5% had positive bone cultures. This included patients without any clinical or radiological signs of osteomyelitis (76/167 patients, 46%) [8]. PTO, particularly in this context, may be due to commensal flora or environmental contamination at the time of injury, but may also be due to bacteria transmitted during hospitalization [9]. The spread of multi-drug resistant bacteria (MDR), usually described as organism non-susceptible to at least one agent in 3 or more antimicrobial classes [10], is a concern worldwide [11]. In the Middle East region, high rates of fecal colonization with Extended-Spectrum Beta-lactamase-Producing Enterobacteriaceae (ESBL-PE) has been reported in the community [12, 13], and particularly in war-wounded and refugees: 69% of 24 Syrian war-wounded children at first admission [14] and 35.1% of 134 adult refugees in four Swiss centers [15]. A high proportion of MDR has also been reported in community-acquired infections, with up to 49.4% of Escherichia coli isolated from urine specimens taken from outpatients and hospitalized patients in a recent meta-analysis in Iran [16, 17].
Our primary objective was to describe and compare the bacterial etiology and proportion of first-line antibiotics resistant bacteria among PTO in war-wounded civilians from Syria, Iraq and Yemen admitted to the reconstructive surgical program of MSF in Amman, Jordan, in the period October 2006–December 2016. Our second objective was to identify risk factors for an infection with FLAR bacteria.
Methods
Study population and microbiological analysis
In October 2006, MSF set up a surgical program in Amman, Jordan, to respond to the needs of war-wounded Iraqi civilians. As conflict expanded to neighboring countries, the program admitted patients from Yemen (since 2010) and Syria (since 2011). Patients had undergone one or multiple previous surgeries in their countries of origin, and entered the MSF program for different conditions including non-union, mal-union, chronic osteomyelitis or amputation stumps needing revision. They were referred for surgical management, and to access physiotherapy and psychological counseling. During orthopedic surgery, the surgeon collected 3 to 5 samples of bone or deep soft tissue and placed them in separate sterile containers. Antibiotic treatment was supposed to stop at least 2 weeks before the surgery. Up to August 2015, each sample was labeled and stored at 4–8 °C before being sent, within 3 h of collection, to laboratories outside the program. After this date, the cultures were carried out in the laboratory set up by MSF within the program. Bacterial culturing and identification followed the European Society of Clinical Microbiology and Infectious Diseases recommendations [18]. Antibiotic susceptibility was determined using Kirby Bauer disk diffusion, as recommended by the European Committee on Antimicrobial Susceptibility Testing [19].
Study design and eligibility criteria
We conducted a retrospective analysis of the laboratory database entered in WHONET, software developed as shareware by the World Health Organization [20]. The inclusion criteria were: civilian patients with bone injury admitted in the Amman MSF program for orthopedic surgery between October 2006 and December 2016, of Iraqi, Syrian or Yemeni nationality, with bone tissue samples collected at time of surgery. Only bone samples taken during first surgery in the Amman MSF program were included in the analysis. We excluded soft tissue samples. Cases of PTO, defined as war-wounded patients with at least one positive bone tissue culture, were described and compared according to country of origin. If the same organism was isolated many times during the same episode of osteomyelitis, it was taken into account only once in the analysis.
Data and statistical analysis
Based on the therapeutic guidelines currently used in the hospital, we defined a first-line antibiotics resistant bacteria (FLAR) as any of the following: i) Enterobacteriaceae resistant to third-generation cephalosporins (3GC, ceftriaxone or cefotaxime or ceftazidime), ii) Pseudomonas aeruginosa resistant to ceftazidime, iii) Acinetobacter baumannii resistant to carbapenems (imipenem or meropenem), or iv) Staphylococcus aureus resistant to oxacillin or to cefoxitin (methicillin-resistant S. aureus, MRSA).
Socio-demographic data of participants were described using percentages for qualitative variables and medians with Inter-Quartile Ranges [IQRs] for quantitative variables. We compared the bacterial etiology and drug resistance proportions according to country of origin using the Chi-square test or Fisher’s exact test. Means of the 3 groups were compared using the ANOVA test.
We described the evolution of the proportion of FLAR (among Enterobacteriaceae and S. aureus) over the time from January 2007 to December 2016 and cases were grouped into five periods of 2 years.
To assess factors associated with infection by FLAR bacteria, logistic regression was used to estimate odds ratio (ORs) and 95% confidence intervals (CI). Variables associated with FLAR infection with p-value < 0.2 in bivariate analysis were selected for inclusion in the multivariate model. Then, a back-step selection procedure was used to keep variables with a p-value < 0.05. Age and sex were left in the final model. Missing values were imputed with the median for quantitative variables and the mode for categorical variables.
Patients with missing values for main explicative variables were compared with other patients for the main demographic and clinical characteristics.
Analyses were done using R software.
Ethics approval and consent to participate
This research fulfilled the criteria set by the Médecins Sans Frontières Ethics Review Board (MSF ERB) for review exemption as a retrospective analysis of routinely collected and anonymized data. The need for MSF ERB submission was deemed unnecessary according to MSF ERB policy.
Results
A total of 727 patients were included, among whom 558 (76.7%) had one or more positive bone tissue cultures. Median age was 31 years and median time between injury and positive bone sample culture was 19 months [IQR 8–40]. Iraqi patients were older, with a longer delay since injury, with a greater number of previous surgeries before entering the program and with a more frequent polymicrobial infection (Table 1).
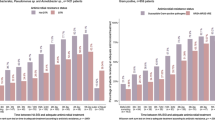
Among the 558 cases of PTO, 450 were monomicrobial and 108 were polymicrobial. A total of 732 different bacterial isolates were identified. Staphylococcus aureus was the most frequently isolated bacteria (n = 193, 26.3%), followed by coagulase-negative Staphylococcus (n = 130, 17.7%), Escherichia coli (n = 126, 17.2%), Pseudomonas aeruginosa (n = 99, 13.5%), Klebsiella pneumoniae (n = 50, 6.8%) and Acinetobacter baumanii (n = 21, 2.8%). Enterobacteriaceae (Escherichia coli, Enterobacter cloacae, Klebsiella spp., Morganella morganii and Proteus spp.) represented 31.5% of all isolates (n = 229) and were cultured in 200 (35.8%) cases of PTO. The proportion of S. aureus was higher in patients from Yemen (34.3%) compared to patients from Syria (25.7%) and from Iraq (24.2%), but this difference was not statistically significant (p = 0.08) (Fig. 1). Bone sample cultures of the lower extremities were more frequently positive for Enterobacteriaceae (38.5%) compared to upper extremities (20.2%, p = 0.003).

Percentage of micro-organism among total isolates from bone biopsies in war-wounded civilians according to country of origin, 2006–2016. *coagulase negative Staphylococcus
According to our definition, 364 isolates were considered as FLAR. Overall, the proportion of resistance to 3GC among Enterobacteriaceae was 86.2% (89.7% among E. coli and 87.7% among K. pneumoniae). Nine isolates (5 E. coli, 2 K. pneumoniae, 1 E. cloacae and 1 P. mirabilis) were also resistant to imipenems (4.3% of all Enterobacteriaceae with susceptibility test results available). The proportion of MRSA among S. aureus was 60.5%. The proportion of P. aeruginosa isolates resistant to ceftazidime was 53.4 and 45% of A. baumannii isolates were carbapenem-resistant. The proportion of MRSA was not significantly different between Iraq (66.6%), Syria (52.2%) and Yemen (54.5%, p = 0.17). There was also no difference in the proportion of FLAR among Enterobacteriaceae and P. aeruginosa by country (Table 2).
While the proportion of 3GC-resistant Enterobacteriaceae remained consistently above 80% since 2007, there was a decreasing trend in the proportion of MRSA over the period, from more than 80% in 2007–2008 to less than 60% since 2011 (Fig. 2). Eight among the 9 Enterobacteriaceae resistant to carbapenems were isolated after 2011.

Trends of methicillin-resistant Staphylococcus aureus and third-generation cephalosporin resistant Enterobacteriaceae from war-related osteomyelitis in civilians from Iraq, Syria and Yemen. *methicillin-resistant Staphylococcus aureus, ** Enterobacteriaceae resistant to 3rd-generation cephalosporin
Concerning resistance to other antibiotics of interest, 58.5% of Enterobacteriaceae and 50.0% of P. aeruginosa were resistant to ciprofloxacin, 44.3 and 41.8% of S. aureus were resistant to rifampin and to ciprofloxacin respectively (Table 3). These proportions were significantly (p < 0.01) higher among FLAR than non-FLAR isolates: 63.3% of 3GC-resistant Enterobacteriaceae were also resistant to ciprofloxacin (versus 24.0% in non-FLAR Enterobacteriaceae) as well as 66% of ceftazidime-resistant P. aeruginosa (vs 34.2% in non-FLAR P. aeruginosa); 66.6% of MRSA were resistant to rifampin (vs 17.1% in non-MRSA) and 59.0% were resistant to ciprofloxacin (vs 16.2%).
FLAR infection was diagnosed in 303 (55.2%) cases. In multivariate analysis, after adjustment for age and sex, FLAR infection was associated with an infection with the lower extremity (p = 0.001), with a time since the injury ≤12 months compared with > 30 months (p = 0.004), and with more than three previous surgeries (p = 0.002) [Additional file 1]. One hundred and thirty two (23.6%) patients had missing values for the number of previous surgeries, 103 (18.4%) had missing values for the site of infection and 92 (16.4%) had also missing values for the time since injury. Compared to other patients, patients with missing values were not different in terms of sex (86% male among patients with missing values vs 90.1%, p = 0.12), their mean age (31.2 years vs 33 years, p = 0.15) and the percentage with FLAR infection (53.6% vs 55%, p = 0.9). However, patients with missing data were more frequently from Iraq (81.6% vs 49%, p = 0.005).
Discussion
PTO in war-wounded patients is a frequent and difficult to treat infection that can have serious functional consequences and even be life-threatening. We report on the bacterial etiology of PTO and the antibiotic resistance of isolates from civilians at the time they were referred from Iraq, Yemen and Syria by analyzing results of bone biopsy cultures. As expected, S. aureus was the most frequent pathogen isolated. However, we also found a high proportion of Gram-negative organisms and a predominance of Enterobacteriaceae. Our results, based here on gold standard specimen for diagnosis of PTO, is similar to that already reported in case series of osteomyelitis in war-wounded patients [21,22,23]. In other contexts, the proportion of Enterobacteriaceae in PTO is variable. This group of bacteria was involved in 2.8% of 142 PTO in one American trauma center [6], but in 35.5% of cases in another recent study in China where patients, like those in the Amman MSF program, were frequently suffering from open fracture and/or soft tissue damage following direct trauma [4]. P. aeruginosa was frequent in our study (13.5% of isolates); this is worrisome for PTO patients in Amman given the fact that infections with P. aeruginosa have been found to be associated with increased risk of recurrence of osteomyelitis [3, 6].
Over the 10 year period, half of the isolates were FLAR. Resistance to 3GC among Enterobacteriaceae was particularly high. This resistance is commonly associated with production of Extended-Spectrum Beta-lactamase and less frequently with AmpC cephalosporinases [24]; however we cannot specify the mechanism due to the absence of reliable information in our database. These results are in line with previous reports of infections in war-wounded in the Eastern Mediterranean and Middle East regions: 100% of 9 Enterobacteriaceae isolates from wounds in the combatants in the Libyan uprising in 2011 were resistant to 3GC [25]; 20 (69%) of 29 g-negative bacteria isolated in 2015 from wound (mostly with deep wound swabs) in refugees from Syria in Jordan were MDR [26]. In a study reporting results of blood culture in patients referred in a regional referral burn care center supported by MSF in Iraq in 2009, 8 (61.5%) of 13 Enterobacteriaceae were EBLS-PE and 12 (54.5%) of 22 P. aeruginosa were resistant to ceftazidime [27]. Results are similar in children: among 24 Syrian war-wounded children, admitted mostly for osteomyelitis and surgical site infection, 66% were infected with ESBL-PE [28]. Carbapenem resistance was quite rare in our series, but emerged from 2012 and is expected to increase given the global dissemination of carbapenemase-producing Enterobacteriaceae [29]. In our study, 60.5% of S. aureus isolated were resistant to oxacillin. Although we observed a slight decline over the study period, this proportion is higher than that reported in recent series of PTO in Brazil (35.5%) and in China (35.9%) [3, 4]. Resistance to other drugs of interest frequently used for osteomyelitis was also common in our patients. The percentage of resistance to fluoroquinolone, the cornerstone of treatment of bone and joint infections involving gram-negative pathogens, and particularly of prosthetic joint infections [30], was higher than 50% in Enterobacteriaceae and P. aeruginosa. The percentage of resistance to rifampin and to fluoroquinolone was higher than 40% in S. aureus isolates. These drugs are commonly used is osteomyelitis and are recommended as first-line oral treatment for Staphylococcus spp. prosthetic joint infections [31]. Due to the high rates of resistance, treatment of PTO is complex in the MSF program in Amman and requires strong antibiotic stewardship procedures as well as second-line antibiotics, often in prolonged intravenous regimens.
The origin of FLAR bacteria isolated from bone sample cultures in these patients in the MSF program is unclear. Intra-hospital transmission of MDR is common and may occur from patient-to-patient, via healthcare workers, or from the environment [32], particularly in the context of conflict with resulting instability and disorganization of health care structures [9]. But it may also be related to colonization prior to injury; the frequent carriage of MDR in the healthy population [12,13,14,15] and the high prevalence of MDR in different community-acquired infections in the Middle East region [16, 17] support this hypothesis. Our analysis found a higher number of previous surgeries to be an independent risk factor for FLAR infection. This finding has already been reported in the previous study from the MSF program in Amman [21]. However, we also found a shorter time since injury to be an independent risk factor, which seems paradoxical with the hypothesis of nosocomial transmission as the origin of FLAR. This may potentially be due to reverse causality; if it is hypothesized that pre-injury colonization with FLAR is the origin of subsequent FLAR bone infection, the initial infection would likely to be inefficiently controlled with first-line antibiotic therapy and would therefore require a higher number of surgical interventions and an earlier referral to our program. Alternatively, a survival bias could exist: patients with wound-related infections caused by FLAR may have poorer early outcome with earlier and more frequent fatal sepsis complications or requirement for amputation compared with those with infection caused by non-FLAR.
The main limitation of our study is related to the laboratory origin of the database and therefore the lack of clinical or radiological data, yet useful for the diagnosis of osteomyelitis, especially when potential contaminant like coagulase-negative Staphylococcus are isolated. However we limited this by analyzing only cultures from bone specimens, and not including deep soft tissue samples. Our risk factor analysis should be interpreted with caution given the number of missing values, but the association between number of previous surgeries and infection with MDR has been already reported [23]. Patients with missing data were more frequently from Iraq and we found that the time since injury was significantly longer in patients from Iraq. This could result in selection bias and an overestimation of the association between FLAR infection and shorter time since injury.
Conclusions
Over 10 years, Enterobacteriaceae were frequently involved in more than 500 PTO in war-wounded civilians from Iraq, Syria and Yemen admitted to the reconstructive surgical program of MSF in Amman. Resistance to first-line antibiotics was frequent among S. aureus and Enterobacteriaceae, regardless of country of origin. Treatment of PTO in the Middle East war context is a challenge given the limited choice of effective antibiotics, the frequent large soft tissue damage and, more globally, the disorganization of health care systems. A high-quality laboratory, a skilled surgical team, a robust antibiotic stewardship and effective infection prevention and control practices are the cornerstones for adequate management.
Abbreviations
- 3GC:
-
Third-generation cephalosporin
- CI:
-
Confidence interval
- ESBL-PE:
-
Extended-Spectrum Beta-lactamase-Producing Enterobacteriaceae
- FLAR:
-
First-line antibiotics resistant bacteria
- IQR:
-
Interquartile range
- MDR:
-
Multi-drug resistant bacteria
- MRSA:
-
Methicillin-resistant Staphylococcus aureus
- MSF:
-
Médecins Sans Frontières
- OR:
-
Odd ratio
- PTO:
-
Post-traumatic osteomyelitis
References
Kremers HM, Nwojo ME, Ransom JE, Wood-Wentz CM, Melton LJ 3rd, Huddleston PM 3rd. Trends in the epidemiology of osteomyelitis: a population-based study, 1969 to 2009. J Bone Joint Surg Am. 2015;97:837–45.
Jiang N, Ma YF, Jiang Y, Zhao XQ, Xie GP, Hu YJ, et al. Clinical characteristics and treatment of extremity chronic osteomyelitis in southern China: a retrospective analysis of 394 consecutive patients. Medicine. 2015;94:e187424.
Jorge LS, Chueire AG, Silva Fucuta P, Machado MN, Oliveira MGL, Nakazone MA, et al. Predisposing factors for recurrence of chronic posttraumatic osteomyelitis: a retrospective observational cohort study from a tertiary referral Center in Brazil. Patient Saf Surg. 2017;11:17.
Peng J, Ren Y, He WZ, Li Z, Yang J, Liu Y, et al. Epidemiological, clinical and microbiological characteristics of patients with post-traumatic osteomyelitis of limb fractures in Southwest China: a hospital-based study. J Bone Joint Infect. 2017;2:149–53.
Chadayammuri V, Herbert B, Hao J, Mavrogenis A, Quispe JC, Kim JW, et al. Diagnostic accuracy of various modalities relative to open bone biopsy for detection of long bone posttraumatic osteomyelitis. Eur J Orthop Surg Traumatol. 2017;27:871–5.
Chadayammuri V, Herbert B, Hao J, Mavrogenis A, Quispe JC, Kim JW, et al. Factors associated with adverse postoperative outcomes in patients with long bone post-traumatic osteomyelitis. Eur J Orthop Surg Traumatol. 2017;27:877–82.
Geurts J, Hohnen A, Vranken T, Moh P. Treatment strategies for chronic osteomyelitis in low- and middle-income countries: systematic review. Tropical Med Int Health. 2017;9:1054–62.
Hérard P, Boillot F, Fakhri RM. Bone cultures from war-wounded civilians in the Middle East: a surgical prospective. Int Orthop. 2017;41:1291–4.
Sahli ZT, Bizri AR, Abu-Sittah GS. Microbiology and risk factors associated with war-related wound infections in the Middle East. Epidemiol Infect. 2016;144:2848–57.
Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:268–81.
Karanika S, Karantanos T, Arvanitis M, Grigoras C, Mylonakis E. Fecal colonization with Extended-Spectrum Beta-lactamase-producing Enterobacteriaceae and risk factors among healthy individuals: a systematic review and Metaanalysis. Clin Infect Dis. 2016;63:310–8.
Hijazi SM, Fawzi MA, Ali FM, Abd El Galil KH. Prevalence and characterization of Extended-Spectrum Beta-lactamases producing Enterobacteriaceae in healthy children and associated risk factors. Ann Clin Microbiol Antimicrob. 2016;15:3.
Hijazi SM, Fawzi MA, Ali FM, Abd El Galil KH. Multidrug-resistant ESBL-producing Enterobacteriaceae and associated risk factors in community infants in Lebanon. J Infect Dev Ctries. 2016;9:947–55.
Peretz A, Labay K, Zonis Z, Glikman D. Disengagement does not apply to Bacteria: a high carriage rate of antibiotic-resistant pathogens among Syrian civilians treated in Israeli hospitals. Clin Infect Dis. 2014;59:753–4.
Piso RJ, Käch R, Pop R, Zillig D, Schibli U, Bassetti S, et al. A cross-sectional study of colonization rates with Methicillin-Resistant Staphylococcus Aureus (MRSA) and Extended-Spectrum Beta-Lactamase (ESBL) and carbapenemase-producing Enterobacteriaceae in four Swiss refugee Centres. PLoS One. 2017;12:e0170251.
Hadifar S, Moghoofei M, Nematollahi S, Ramazanzadeh R, Sedighi M, Salehi-Abargouei A, et al. Epidemiology of multidrug resistant Uropathogenic Escherichia Coli in Iran: a systematic review and meta-analysis. Jpn J Infect Dis. 2017;1:19–25.
Hamouche E, Sarkis DK. Evolution of susceptibility to antibiotics of Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter baumanii, in a University Hospital Center of Beirut between 2005 and 2009. Pathol Biol. 2012;60:e15–20.
European Society of Clinical Microbiology and Infectious Diseases (ESCMID). Manual of Microbiology. https://www.escmid.org/escmid_publications/manual_of_microbiology/. Accessed 10 Apr 2018.
European Committee on Antimicrobial Susceptibility Testing (EUCAST). Guidance documents. http://www.eucast.org/guidance_documents/. Accessed 10 Apr 2018.
O’Brien TF, Eskildsen MA, Stelling JM. Using internet discussion of antimicrobial susceptibility databases for continuous quality improvement of the testing and management of antimicrobial resistance. Clin Infect Dis. 2001;33(Suppl 3):118–23.
Johnson EN, Burns TC, Hayda RA, Hospenthal DR, Murray CK. Infectious complications of open type III tibial fractures among combat casualties. Clin Infect Dis. 2007;45:409–15.
Yun HC, Branstetter JG, Murray CK. Osteomyelitis in military personnel wounded in Iraq and Afghanistan. J Trauma. 2008;64(Suppl 2):163–8.
Murphy RA, Ronat JB, Fakhri RM, Herard P, Blackwell N, Abgrall S, et al. Multidrug-resistant chronic osteomyelitis complicating war injury in Iraqi civilians. J Trauma. 2011;71:252–4.
Roer L, Hansen F, Christen M, Knudsen JD, Hansen DS, Wang M, et al. WGS-based surveillance of third-generation cephalosporin-resistant Escherichia Coli from bloodstream infections in Denmark. J Antimicrob Chemother. 2017;72:1922–9.
Franka EA, Shembesh MK, Zaied AA, El-Turki E, Zorgani A, Elahmer OR, et al. Multidrug resistant Bacteria in wounds of combatants of the Libyan uprising. J Infect. 2012;65:279–81.
Abbara A, Al-Harbat N, Karah N, Abo-Yahya B, El-Amin W, Hatcher J, et al. Antimicrobial drug resistance among refugees from Syria, Jordan. Emerg Infect Dis. 2017;23:885–6.
Ronat JB, Kakol J, Khoury MN, Berthelot M, Yun O, Brown V, et al. Highly drug-resistant pathogens implicated in burn-associated bacteremia in an Iraqi burn care unit. PLoS One. 2014;9:e101017.
Kassem DF, Hoffmann Y, Shahar N, Ocampo S, Salomon L, Zonis Z, et al. Multidrug-resistant pathogens in hospitalized Syrian children. Emerg Infect Dis. 2017;23:166–8.
Logan LK, Weinstein RA. The epidemiology of Carbapenem-resistant Enterobacteriaceae: the impact and evolution of a global menace. J Infect Dis. 2017;215(Suppl 1):28–36.
Rodríguez-Pardo D, Pigrau C, Lora-Tamayo J, Soriano A, del Toro MD, Cobo J, et al. Gram-negative prosthetic joint infection: outcome of debridement, antibiotics and implant retention approach. A large multicentre study. Clin Microbiol Infect. 2014;20:911–9.
Osmon DR, Berbari EF, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis. 2013;56:e1–25.
Birgand G, Zahar JR, Lucet JC. Insight into the complex epidemiology of multidrug-resistant Enterobacteriaceae. Clin Infect Dis. 2018;66:494–9.
Acknowledgments
The authors are grateful to Justine Michel and Conor Browman, all the staff of the reconstructive surgical program of Médecins Sans Frontières in Amman, Jordan, who contributed to the collection of the data and to Clair Mills, medical director, operational center Paris Médecins Sans Frontières, for her critical reviewing of the manuscript.
Funding
This study was supported by Médecins Sans Frontières. Epicentre receives core funding from Médecins Sans Frontières. Authors from Médecins Sans Frontières were involved in the conception of the study, in the acquisition and interpretation of the data and in the revision of the manuscript.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
FF, CL, J-BR, RK and NM conceived and designed the study. NH and R-MF contributed to the acquisition of data. FF, CL and CS analyzed and interpreted the data. FF and CL wrote the final report. All authors were involved in revising the manuscript, approved the final version and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research fulfilled the criteria set by the Médecins Sans Frontières Ethics Review Board (MSF ERB) for review exemption as a retrospective analysis of routinely collected and anonymized data. The need for MSF ERB submission was deemed unnecessary according to MSF ERB policy.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Factors associated with first-line antibiotics resistant bacteria infection in war-related post-traumatic osteomyelitis from Iraq, Syria and Yemen, 2006–2016. (DOCX 33 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Fily, F., Ronat, JB., Malou, N. et al. Post-traumatic osteomyelitis in Middle East war-wounded civilians: resistance to first-line antibiotics in selected bacteria over the decade 2006–2016. BMC Infect Dis 19, 103 (2019). https://doi.org/10.1186/s12879-019-3741-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-019-3741-9