
Abstract
Background
Bacteraemia is a common cause of morbidity and mortality in patients admitted to hospital. The aim of this study is to analyse the results of a two-year programme for the early optimisation of antibiotic treatment in patients admitted to the Costa del Sol Hospital (Marbella. Spain).
Methods
A prospective two-year cohort study was conducted, evaluating all episodes of bacteraemia at the Costa del Sol Hospital. Epidemiological and microbiological characteristics, any modification of the initial antibiotic treatment, prognostic risk stratification, early mortality related to the episode of bacteraemia, and mortality after the seventh day, were included in the analysis.
Results
Seven hundred seventy-three episodes of bacteraemia were treated, 61.6% males and 38.4% females. The mean age was 65.2 years. The condition was most commonly acquired in the community (41.4%). The bacteraemia was most frequently urological in nature (30.5%), and E coli was the microorganism most frequently isolated (31.6%). In 51.1% of the episodes, a modification was made to optimise the treatment. In the first week, 8.2% died from bacteraemia, and 4.5% had died when they were located. The highest rates of death were associated with older patients, nosocomial acquisition, no source, McCabe score rapidly fatal, Charlson index ≥3, Pitt index ≥3 and treatment remained unmodified.
Conclusion
The existence of bacteraemia control programmes and teams composed of clinicians who are experienced in the treatment of infectious diseases, can improve the disease outcome by enabling more severe episodes of bacteraemia to be recognised and their empirical treatment optimised.
Similar content being viewed by others

Background
Bacteraemia is a major cause of morbidity and mortality in patients admitted to hospital [1,2,3]. Many of the deaths caused by this infectious process take place in the first few hours following the onset of bacteraemia. For this reason, it is crucial to implement measures for diagnosis and treatment as soon as possible [4].It is also particularly important to identify the subgroup of patients who are most likely to present a poor prognosis and therefore suffer greater mortality. Recent studies have reported a higher incidence of mortality among patients who receive inappropriate empirical therapy in the initial hours of bacteraemia [5].
The aim of this study is to describe the results achieved by a multidisciplinary early intervention programme for patients with bacteraemia, and its impact on attributable mortality during the first 7 days. In additions, we aimed to determine risk factors for 7 day mortality.
Methods
The Costa del Sol Hospital (HCS) is a general hospital of specialities that forms part of the public health system in Andalusia (southern Spain). It has 350 beds and functions as a referral hospital for 396,012 inhabitants of the Western Costa del Sol (Málaga province). The software used is HP Doctor, an operating system that enables administrators to work with a single computerised medical record.
Since 2008, the HCS has employed a multidisciplinary programme for early intervention in patients with positive blood cultures (except the ICU and the paediatrics department), staffed by clinicians from the infectious disease and microbiology groups [6, 7]. Positive blood cultures are notified at an early stage by the microbiology service group, at a joint meeting with experts in the treatment of infectious diseases. Subsequently, a systematic search is conducted to identify hospitalised patients with bacteraemia and the doctor treating them. The same process is used to locate patients who have been sent home from the emergency department, via an action protocol based on clinical status and treatment recommended at the moment of discharge [8]. With these data available, an interview is held with the physician responsible (in the case of hospitalised patients), to assess the outlook for the optimisation of antibiotic treatment, taking into account the antimicrobial spectrum, the drug dose and Pk/Pd parameters.
The first action taken by the bacteraemia control team is based on the results of the Gram stain of blood cultures, facilitated by the team’s microbiologist. The second stage of the procedure is applied after the definitive identification of the microorganism producing the bacteraemia and of its sensitivity profile. At this point, the empirical treatment is confirmed or assessed according to the microbiological results. In addition, a recommendation is made regarding the duration of antibiotic treatment. The outcome of the intervention, after an interview with the doctor responsible for follow up, is transcribed onto a non-binding clinical report included in the patient’s computerised medical history.
A prospective cohort study was conducted to evaluate the results of an early intervention programme developed by the HCS Infectious Diseases and Microbiology group for patients aged 14 years and older with bacteraemia. The following variables were analysed: age, sex, microbiological isolates, source of infection acquisition, source of origin and evolution of condition in response to the modified antimicrobial treatment. The condition was considered to be of community origin in patients with no previous hospitalisation or contact with health care services; or nosocomial, in accordance with CDC criteria or treatment-related, under the definition proposed by Friedman [9]. The prognosis of the underlying disease was defined using the criteria of McCabe and Jackson, with the following classifications: rapidly fatal (RF), ultimately fatal (UF) or nonfatal (NF). Mortality was predicted using Charlson’s index of comorbidity [10] and Pitt’s index of bacteraemia [11].
True bacteraemia was defined as the isolation of one or more clinically-apparent bacteria or fungi in the blood cultures [12]. The presence of coagulase-negative Staphylococcus (ECN), Streptococcus viridans, Corynebacterium spp., Propionibacterium spp. or Bacillus spp. in just one blood culture bottle was considered to result from contamination. Polymicrobial bacteraemias were not excluded. The patients were not included in more than one occasion.
Statistical analysis
A descriptive analysis was performed, with measures of central tendency and dispersion for the quantitative variables and of frequency distribution for the qualitative ones, together with 95% confidence intervals for the outcome variables. Taking as the variable for the comparison of subgroups the presence or absence of mortality at the conclusion of the study, a bivariate analysis was performed using the chi-square test for qualitative independent variables (or Fisher’s exact test if fewer than five observations were expected), and Student’s t test for quantitative independent variables (or the Mann-Whitney U test in the case of non-normal distribution, which was checked by the Kolmogorov-Smirnov test). Finally, three multivariate logistic regression models were constructed, taking as the outcome variable the mortality at the conclusion of the study, and including the independent variables by forward stepwise selection, including the relative risk with the corresponding 95% CI. In each multivariate model, each of the comorbidity indicators to be evaluated was introduced independently. In all analyses, the limit of statistical significance was established at p < 0.05.
Results
“Analysis of the entire cohort”
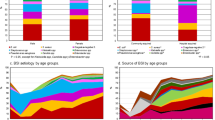
Over a period of 2 years, 773 episodes of bacteraemia aged 14 years or more were evaluated. Characteristics of patients and infection are presented in Table 1. The gender distribution was 476 males (61.6%) and 297 females (38.4%). The mean age of the patients was 65.2 years (SD 16.7). Infection acquisition took place in the community in 320 episodes (41.4%), was healthcare-associated in 280 (36.2%) and was nosocomial in 173 (22.4%). The severity of comorbidities was determined by the McCabe index (NF: 43.7% UF: 41.2%, RF: 15.2%) and the Charlson index (≤2: 54.8%; >2: 45.2%). The severity of bacteraemia was determined by the Pitt index (≤2: 83.3%; >2: 16.7%). Although 45% of the patients had a significantly high Charlson comorbidity index >2, only a relatively small proportion (16.7%) of the patients with bacteraemia had an increased prognosis of mortality in 30 days (Pitt index ≥3).
The main source of origin of the bacteraemia were urological (n = 217; 30.5%), abdominal (n = 160; 20.7%). The rest of the sources are in Table 1. The most frequently isolated microorganisms were E. coli (246 episodes; 31.6%), Klebsiella sp. (59 episodes; 7.6%), Enterobacter sp. (22 episodes; 2.8%), Proteus mirabilis (20 episodes; 2.6%), Pseudomonas aeruginosa (27 episodes; 3.5%), Staphylococcus coagulase-negative (172 episodes; 22.3%), Staphylococcus aureus (65 episodes; 52 (6.7%) of which were MSSA and 13 (1.7%) were MRSA), Enterococcus faecalis (19 episodes; 2.5%), Enterococcus faecium (9 episodes; 1.2%), anaerobes (17 episodes; 2.3%), and Candida sp. (10 episodes; 1.3%). Enterobacteriaceae producing extended spectrum beta-lactamase originated 37 episodes (4.8%). The cases provoked by coagulase-negative Staphylococcus were related to health care in patients with central or tunnelled catheters or haemodialysis. Only 4 episodes of bacteraemia were polymicrobial and they have been included in the section of others (table n° 1).
Of the 773 episodes of bacteraemia, 21 were excluded from the analysis of mortality because the patient was transferred to another centre, and so 752 were finally evaluated. Of these 111 died (14.7%; 95% CI: 12.2–17.4). Thirty-four patients (4.5%) had died before they were located. In the first week of hospitalization, 62 patients (8.2%) died with the cause of death attributed to bacteraemia. During the first 30 days, another 49 patients (6.5%) died for reasons not directly attributable to bacteraemia after the first week. Six hundred forty-one patients (85.2%) survived more than 30 days.
Regarding modifications to the antimicrobial treatment applied in these episodes of bacteraemia, in 350 cases (45.3%) there was no such modification, in 27 cases (3.6%) the treatment duration was extended and in 396 (51.1%) a modification was made to optimise the treatment. In the 51,1% of cases, the antimicrobial spectrum was enlarged due to the inadequate empirical treatment by switching to other drugs (see Table 1).
The bivariate analysis revealed significant differences (p < 0.001) between mortality attributable to bacteraemia and age (the differences were greater for older patients), the McCabe index with ultimately fatal (UF) and rapidly fatal (RF) disease, the Charlson and Pitt index score ≥ 3, the absence of a source of origin and the non-modification of treatment. There were no statistically significant differences regarding gender distribution, microorganism isolated or place of infection acquisition, although nosocomial acquisition presented a higher percentage (18%; 30 patients) than community-acquired infection (13.2%; 41 patients) and healthcare-associated infection (14.6%; 40 patients) (see Table 2).
Each of the multivariate logistic regression models, differentiated by the comorbidity adjustment applied, includes the increased risk of mortality as an associated variable. The model incorporating McCabe category RF is associated with a greater adjusted risk of death at 7 days (RR 7.616, 95%CI: 3.81–15.221) (Table 3). In the Pitt-adjusted multivariate model (Table 4) for category ≥3, the RR is 7.014 (95%CI: 4.345–11.321), compared with RR = 2.678 (95%CI: 1.706–4.204) for category ≥3 on the model with Charlson adjustment (Table 5). In the three multivariate models, age, absence of a source of infection and the non-modification of treatment are all risk factors for greater mortality, while the model in which comorbidity is adjusted by the Charlson index also includes the presence of nosocomial infection.
“Analysis of patients discharged from the emergency department”
Ninety patients were located at home. Of these 90, the median age was 67 years, and they comprised 54 males (60%) and 36 females. Infection acquisition took place in the community in 51 cases (56.6%) and the microorganism that was most frequently involved was Escherichia coli, with 31 cases (34.4%). The median score on both the Charlson index and the Pitt index of bacteraemia was 1. Thirty-eight cases (42.2%) required hospitalisation. A Pitt index >1 and treatment modification were the variables most frequently associated with the need for hospital admission. One patient (1.2%) died and 6 (6.6%) could not be located.
Discussion
Bacteraemia remains a significant cause of morbidity and mortality in hospitalised patients, despite recent advances in diagnosis and treatment strategies [13, 14]. The recognition of episodes of bacteraemia according to criteria of severity and early treatment optimisation can facilitate actions to improve final outcomes. The administration of inappropriate antibiotic therapy is an independent predictor of mortality in patients with bacteraemia and sepsis [5]. The existence of multidisciplinary teams, composed of experts in the field of infectious diseases, together with pharmacists and microbiologists, enables a comprehensive approach to be taken to antibiotic treatment, producing not only better and earlier diagnosis but also enhancing outcomes in terms of Pk/Pd. The incorporation of pharmaceutical experts can also lend added value to the recommendations made by the bacteraemia control team [15]. Several reports have been issued on the reductions achieved in the mortality of certain infectious diseases when the treatment strategy is directed by experts in this field [16].
This paper describes the results obtained from the application, over 2 years, of a multidisciplinary programme for patients with bacteraemia, at a general hospital of specialities in Andalusia (Spain). Of the 773 episodes considered, 40% were community-acquired; the most frequent source of infection was urological and the microorganism producing the bacteraemia was E coli in 30.6% of cases, which is in accordance with previous reports [17].
Fewer than 5% of patients died within 24 h, before the bacteraemia control team was able to intervene. A further 8.2% of the patients died within the first 7 days of hospital admission, due to the bacteraemia episode. In 51.1% of the episodes, the treatment was modified in order to optimise its antimicrobial impact.
Older patients, the nosocomial acquisition of bacteraemia and the absence of identifiable source of infection are all associated with increased patient mortality. These findings are consistent with previous research in the field. Thus, a multicentre study, conducted in Andalusia (Spain), reported that mortality at days 14 and 28, in elderly patients, was associated with severe forms of infection and with inadequate empirical treatment [18]. Another study reported higher mortality in bacteraemia cases of nosocomial origin, possibly interacting with resistant organisms and in conjunction with inadequate treatment [19]. The greater mortality of patients with no identifiable source of infection is probably accounted for by the increased difficulty this causes in establishing appropriate empirical treatment and by the impossibility of acting on or removing an initial source of bacteraemia. Recently, Mansur et al. [20] reported increased mortality among critically-ill patients with primary bacteraemia versus those with bacteraemia of respiratory or abdominal origin. Patients with bacteraemia of unknown origin presented a higher SOFA score than those with a respiratory or abdominal source of infection.
Patients with high scores on the risk stratification indices for mortality prediction, such as McCabe RF (RR: 7.616), Pitt’s bacteraemia index ≥3 (RR: 7.019) and Charlson’s comorbidity index ≥3 (RR: 2.68), were more liable to suffer early mortality (in the first 7 days), as reported elsewhere [21]. Both the presence of comorbidity or chronic debilitating disease, as measured by the Charlson index, and the presentation of severe forms of infection, often with haemodynamic instability, may account for the higher mortality recorded [22].
The main limitation of the present study is that, although it was prospective, we did not know the incidence of mortality before the bacteraemia control team began its work, since our hospital classifies cases by disease process, and the study cases were coded as sepsis, not bacteraemia. For this reason, our results cannot be compared with previous data. Nevertheless, they can be compared with those from general hospitals of specialities that attend patients with the same profile of complexity. The continuing application of the early care programme for patients with bacteraemia will enable a long-term assessment to be made of outcomes, and may reduce morbidity and mortality among these patients.
We believe that early intervention in patients with a strong probability of presenting bacteraemia, based on multidisciplinary programmes integrated into routine clinical practice, would enable clinicians to stratify the severity of the process and facilitate rapid optimisation of empirical antimicrobial therapy in the initial response and focused treatment thereafter. This set of actions could reduce morbidity and mortality in patients with bacteraemia. Additionally, early intervention programmes for patients with bacteraemia would enable the recovery of patients who have been discharged from the emergency department and who require treatment modification or even hospitalisation [8].
Conclusions
Our program of identification and early action on patients with bacteraemia allowed the localization of both hospitalized patients and those who discharged from the Emergency Department, who had a higher risk of unfavorable outcome based on the McCabe and Charlson comorbidities indexes and Pitt bacteraemia index. The bacteraemia control team optimized antimicrobial treatment in slightly more than half of the cases, being this a favourable influence in the final mortality of the patients.
Abbreviations
- 95% CI:
-
95% confidence interval
- CDC:
-
Center for diseases control
- HCS:
-
Costa del Sol Hospital
- ICU:
-
Intensive care unit
- NF:
-
Nonfatal
- RF:
-
Rapidly fatal
- RR:
-
Relative risk
- SD:
-
Standard deviation
- SOFA score:
-
Sequential organ failure assessment score
- UF:
-
Ultimately fatal
References
Weinstein MP, Towns ML, Quartery SM, et al. The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis. 1997;24:584–602.
Wisplinghoff H, Bischoff T, Tallent SM, et al. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39:309–17.
Rodríguez-Creixems M, Alcalá L, Muñoz P, et al. Bloodstream infections. Evolution and trends in the microbiology workload, incidence and etiology, 1985–2006. Medicine. 2008;87:234–49.
Yokota PKO, Marra AR, Martino MDV, et al. Impact of appropriate antimicrobial therapy for patients with severe sepsis and septic shock – a quality improvement study. PLoS One. 2014;9(11):e104475. doi:10.1371/journal.pone.0104475.
Retamar P, Portillo MM, López-Prieto MD, Rodríguez-López F, et al. Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis. Antimicrob Agents Chemother. 2012;56(1):472–8.
Del Arco A, Tortajada B, de la Torre J. Olalla et al. results of a counselling programme in antibiotic treatment in a secondary hospital. Rev Esp Quimioter. 2011;24(2):96–8.
Del Arco A, Tortajada B, de la Torre J, Olalla J. The impact of an antimicrobial stewardship programme on the use of antimicrobials and the evolution of drug resistance. Eur J Clin Microbiol Infect Dis. 2015;34(2):247–51.
Del Arco-Jiménez A, Olalla-Sierra J, de la Torre-Lima J, Prada-Pardal JL, et al. Results of an early intervention program for patients with bacteremia discharged from the emergency department. Med Clin (Barc). 2014;142(3):107–10.
Friedman ND, Kaye KS, Stout JE, McGarry SA, Trivette SL, Briggs JP, et al. Health care-associated bloodstream infections. Ann Intern Med. 2002;137:791–7.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Cisneros-Herreros JM, Cobo-Reinoso J, Pujol-Rojo M, Rodríguez-Baño J, Salavert-Lletí M. Guía para el diagnóstico y tratamiento del paciente con bacteriemia. Guía de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica. Enferm Infecc Microbiol Clin. 2007;25:111–30.
Bryan CS. Clinical implications of positive blood cultures. Clin Microbiol Rev. 1989;2:329–53.
Sanz Carabaña P, Ramos Martínez A, Asensio Vegas A, García Navarro MJ. Mortality and prognostic factors in patients admitted with community-acquired bacteremia. An Med Interna. 2006;23(2):66–72.
Rodríguez-Baño J, López-Prieto MD, Portillo MM, Retamar P, et al. Epidemiology and clinical features of community-acquired, healthcare-associated and nosocomial bloodstream infections in tertiary-care and community hospitals. Clin Microbiol Infect. 2010;16:1408–13.
Tsukamoto H, Higashi T, Nakamura T, Yano R. Clinical effect of a multidisciplinary team approach to the initial treatment of patients with hospital-acquired bloodstream infections at a Japanese university hospital. Am J Infect Control. 2014;42(9):970–5.
Jenkins TC, Price CS, Sabel AL, Mehler PS, Burman WJ. Impact of routine infectious diseases service consultation on the evaluation, management, and outcomes of Staphylococcus Aureus bacteremia. Clin Infect Dis. 2008;46:1000–8.
Cisneros-Herreros JM, Sánchez-González M, Prados-Blanco MT, Llanos-Rodríguez C. Blood cultures in the emergency department. Enferm Infecc Microbiol Clin. 2005;23(3):135–9.
Retamar P, López-Prieto MD, Rodríguez-López F, de Cueto M. Predictors of early mortality in very elderly patients with bacteremia: a prospective multicenter cohort. Int J Infect Dis. 2014;26:83–7.
Peralta G, Lamelo M, Alvarez-García P, Velasco M. Impact of empirical treatment in extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella spp. bacteremia. A multicentric cohort study. BMC Infect Dis. 2012;12:245.
Mansur A, Klee Y, Popov AF, Erlenwein J, et al. Primary bacteraemia is associated with a higher mortality risk compared with pulmonary and intra-abdominal infections in patients with sepsis: a prospective observational cohort study. BMJ Open. 2015;5(1):e006616. doi:10.1136/bmjopen-2014-006616.
Rhee JY, Kwon KT, Ki HK, Shin SY, et al. Scoring systems for prediction of mortality in patients with intensive care unit-acquired sepsis: a comparison of the Pitt bacteremia score and the acute physiology and chronic health evaluation II scoring systems. Shock. 2009;31(2):146–50.
Mylotte JM, Kahler L, McCann C. Community-acquired bacteremia at a teaching versus a nonteaching hospital: impact of acute severity of illness on 30-day mortality. Am J Infect Control. 2001;29:13–9.
Acknowledgments
To the Costa del Sol Sanitary Agency for the economic support to publish the present paper.
Funding
None.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and supplementary information files.
Authors’ contributions
AA designed the study and drafted the manuscript. AA, JO, JT, AB, JLP and JGA have been involved in revising critically the manuscript. FR participated in data analysis. NMQ and FFS contributed to data acquisition and critical manuscript revision. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The Costa del Sol Research Ethics Committee has evaluated the study “Results of an early intervention program for patients with bacteraemia. Analysis of prognostic factors and mortality” with low ethical load, not specifying the request of informed consent to the patient; being in any case a study from the perspective of clinical practice. All data compiled in this project were recorded anonymously, in strict accordance with the Biomedical Research law currently in force in Spain (Act 14/2007 of 3 July), data protection laws in force at national level (Law 41/2002 of 14 November, Law 15/1999 of 15 December) and adhering at all times to the Declaration of Helsinki.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
del Arco, A., Olalla, J., de la Torre, J. et al. Results of an early intervention programme for patients with bacteraemia: analysis of prognostic factors and mortality. BMC Infect Dis 17, 360 (2017). https://doi.org/10.1186/s12879-017-2458-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-017-2458-x