
Abstract
Background
Health care associated transmission of Mycobacterium tuberculosis (TB) is well described. A previous survey of infection control (IC) practices at clinical research sites in low and middle income countries (LMIC) funded by the National Institute of Allergy and Infectious Diseases (NIAID) conducting HIV research identified issues with respiratory IC practices. A guideline for TB IC based on international recommendations was developed and promulgated. This paper reports on adherence to the guideline at sites conducting or planning to conduct TB studies with the intention of supporting improvement.
Methods
A survey was developed that assessed IC activities in three domains: facility level measures, administrative control measures and environmental measures. An external site monitor visited each site in 2013–2014, to complete the audit. A central review committee evaluated the site-level survey and results were tabulated. Fisher’s exact test was performed to determine whether there were significant differences in practices at sites that had IC officers versus sites that did not have IC officers. Significance was assessed at p</=.05
Results
Seven of thirty-three sites surveyed (22 %) had all the evaluated tuberculosis IC (TB IC) elements in place. Sixty-one percent of sites had an IC officer tasked with developing and maintaining TB IC standard operating procedures. Twenty-two (71 %) sites promptly identified and segregated individuals with TB symptoms. Thirty (93 %) sites had a separate waiting area for patients, and 26 (81 %) collected sputum within a specific well-ventilated area that was separate from the general waiting area. Sites with an IC officer were more likely to have standard operating procedures covering TB IC practices (p = 0.02) and monitor those policies (p = 0.02) and perform regular surveillance of healthcare workers (p = 0.02). The presence of an IC officer had a positive impact on performance in most of the TB IC domains surveyed including having adequate ventilation (p = 0.02) and a separate area for sputum collection (p = 0.02)
Conclusions
Specific and targeted support of TB IC activities in the clinical research environment is needed and is likely to have a positive and sustained impact on preventing the transmission of TB to both health care workers and vulnerable HIV-infected research participants.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Time and attention to infection control (IC) activities improves patient and staff infection rates [1, 2] and reduces costs associated with health care [3]. In resource limited settings, the contribution of health care associated infections to patient morbidity may be underestimated and significant [4]. Health care associated transmission of Mycobacterium tuberculosis (TB) is well described in both patients and health care workers and outbreaks of tuberculosis including extensively drug resistant TB (XDR TB) have been linked to the health care environment in several resource limited settings [5, 6]. Prevention of health care associated TB transmission, therefore, is an urgent IC need in resource-limited settings.
Recommendations regarding facilities level management activities, administrative, and environmental IC measures and personal protection practices [7–9] have been developed by several agencies including the World Health Organization (WHO) and the US Centers for Disease Control (CDC). In the United States, regulations require an “active program for the prevention, control, and investigation of infections and communicable diseases” [10], and wide implementation of a variety of IC practices in the last 20 years has resulted in a substantial decrease in health care associated transmission of TB [7]. In resource limited settings, there are no regulatory requirements, and uptake of guidance has been incomplete. Adherence to international guidelines has been evaluated in several settings and compliance with the full complement of recommendations is rare. In particular the presence of a written IC plan, staff and patient education, segregation of patients with symptoms and yearly evaluation of health care workers are uncommonly found [11–13]. Two recent studies in South Africa assessed the impact of health care worker education about IC principles and the results are worrisome [14, 15]. Although a higher level of training was associated with better knowledge of TB IC, this knowledge did not always translate into better TB IC (IC) practice [14]. Importantly, among health care workers (HCW) the rates of smear positive TB were higher than in the general population and the audit cycle (standard setting, evaluation of practice and outcomes and re-audit) had no impact on rates of incident TB in this group. A general review of IC practices including respiratory and hand hygiene, IC organizational structure and blood safety at NIAID funded clinical research sites was conducted in 2011 and 2012 [16]. Several important issues were identified at the sites in low and middle income countries, the most urgent of which was the need for a network policy for TB IC. A guideline for TB IC was developed based on existing international recommendations and promulgated early in 2012. External monitors were then sent to all sites to assess adherence to the guideline. This paper reports on uptake of these recommendations at clinical sites conducting or planning to conduct TB-related ACTG clinical trials with the objective of improving participant and staff safety.
Methods
Thirty-three NIAID-funded clinical research sites located in LMIC in the AIDS Clinical Trials Group (ACTG) and the International Maternal, Pediatric, Adolescent AIDS Clinical Trials Network (IMPAACT) networks signaled their intention to participate in clinical trials involving TB. These sites were given the ACTG TB IC guideline, and a survey was developed to assess adherence to the ACTG guideline [Additional file 1]. This survey tool was piloted at five representative clinical trial sites and refined to improve the ease of its administration for both the monitor and the site staff as well as to address minor technical and scientific issues. The sites were then monitored by an objective external monitoring organization (PPD) to assess adherence to the guideline using the survey. The external monitoring organization visited each site and directly observed IC practice between February 2013 and December 2014 and documented adherence to the ACTG guideline using the survey tool. The results of each site survey were reviewed by an ACTG committee in real time, and feedback was given to each site in order to improve practice.
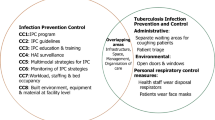
Notionally the survey was divided into three key components of TB IC practice: facility level measures, administrative control measures and environmental control measures (see Table 1). Facilities level activities that were evaluated included whether an air flow assessment for clinic areas had been performed, whether patients with symptoms and cough were identified and separated, and whether sputum collection was separate from the patient care areas and collected in an appropriate facility. Waiting areas were evaluated for crowding and ventilation. The presence of policies for annual TB surveillance of health care workers (HCW) and policies for HIV Post-Exposure Prophylaxis (PEP) and Isoniazid Preventive Therapy (IPT) were noted as well as quality management practices for regular assessment of adherence to written policies and standard operating procedures. External monitors assessed whether personal protective equipment (PPE) including N95 masks or equivalent were available and fit tested. Policies for hand hygiene and appropriate instruction were recorded as present or absent.
Two reviewers (CG and GT) summarized and tabulated the information, percentages of positive responses were recorded and a yes/no assessment to open ended questions was provided. The answers to the elements in the assessment tool provided a measure of adherence to the ACTG IC guideline. A Fisher’s exact test was performed to determine whether there were significant differences in practices at sites that had IC officers versus sites that did not have IC officers. Significance was assessed at p</=.05
No ethical review was required as this was not research involving human subjects.
Results
Thirty one of thirty-three sites had complete responses to the IC survey. Seven sites (22 %) had all the surveyed elements already in place.
Facilities level control
Sixty-one percent of sites had an IC officer tasked with developing and maintaining SOPs. Just over half the sites had SOPs in place for the major IC domains, and 81 % (25/31) of these performed and documented regular audits of their SOPs. Health care workers were required to have annual screening for tuberculosis at 61 % (19/31) of sites. Screening could consist of any of a symptom screen, a CXR or a tuberculin skin test.
Administrative
Most sites had some TB IC administrative support. Seventy-one percent of sites promptly identified individuals with TB symptoms and segregated them.
Environmental
Ninety-three percent of sites (28/30) had a separate waiting area for patients, and collected sputum in a specific area (81 %) that was separate from the general area and well ventilated as judged by the auditor. Sites were likely to promote cough hygiene by having signs posted, available disposable handkerchiefs, and disposable masks for patients (81 % of sites). There was adequate ventilation with measurement of airflow in the waiting areas, examination rooms and specimen collection areas at 81 % of sites. Personal protective equipment was commonly present (97 %), including N95 masks and respirators (87 %), but masks were not commonly fit tested (43 %–13/30 sites).
The sites with an IC officer in general performed significantly better in most but not all of the domains surveyed (see Table 2). Specifically, sites with an IC officer were more likely to have standard operating procedures for important IC practices (p = 0.02; 95 % confidence intervals 9.0 %, 71.5 %) and to monitor adherence to these practices (p = 0.02; 6.2–63.9 %) were more likely to perform surveillance of health care workers (p = 0.02; 8.8–72.5 %). These sites were also more likely to have adequate ventilation (p = 0.02; 5.9– 64.2 %) and separate areas for sputum collection (p = 0.02; 6.0– 64.3 %).
Discussion
The results of our study provide an assessment tool for continuing improvement in the area of TB IC in the clinical research setting. The clinical research environment provides an opportunity to model and evaluate best practices for clinical care. Typically the patient volume is less than in the clinical care setting and there are rigorous standards for good clinical practice with which all members of the research team are required to be certified. Indeed, many have argued that the research environment should be held to the highest achievable standard of clinical care [17] which may differ from local standard of care. Nevertheless, we identified important gaps in TB IC knowledge and areas for improvement of IC practices. Most of the NIAID Division of AIDS (DAIDS) sponsored clinical sites had some basic TB elements for IC practices in place and a few sites had all the important elements in place. The most important finding was that when a trained IC officer was present, the facility was more likely to have SOPs in place for the major TB IC domains, to segregate sputum collection from the general study participant areas, and to provide annual surveillance of health care workers for TB infection. The TB IC survey was used to make site-specific recommendations in real time for improvement of TB infection prevention practices and capacity building. For example, standardized instructions were developed for assessing airflow and inexpensive equipment for its measurement were sourced. Having the elements in place did not imply that the practices were the best available, but they provided a framework in which improvement could occur. For example, having a policy of yearly screening of health care workers already in place, means that the specifics of the screening can then be evaluated as a next step.
The effect of specific IC activities is difficult to measure but evaluation of adherence to specific recommendations will be a helpful next step. Despite appropriate TB IC training, it still may be difficult to prevent health care associated transmission of TB. The administrative component of IC practice such as the presence of an IC practitioner, policies and procedures for handling patients and staff members with infections and documentation of those procedures, has been demonstrated to lead to improved outcomes in resource rich environments [18, 19]. A review of the effect of IC interventions in low and middle income countries concluded that administrative controls have the potential to reduce new TB infections in health care workers [6]. There also may be an incremental benefit to engineered solutions such as the use of mechanical ventilation and ultraviolet (UV) lights to limit TB infectiousness [6]. In resource-limited settings high clinical burden, shortages of the materiel required for universal precautions (eg PPE), minimal support from health care management for these activities and minimal or no regulatory requirements for compliance to IC procedures make adhering to IC recommendations difficult. High staff turnover provides an additional challenge. The effect of a specific single intervention, is therefore harder to prove and is less well studied
Health care workers may be an important link in the transmission cycle of TB in clinical research settings: the risk to clinic staff for TB acquisition may be considerable and staff with active TB may put other vulnerable patients at risk. The prevalence of TB infection and disease is high in health care workers compared to the general population [6, 20]. Latent TB infection is common and in a prospective study, HCW experienced incident latent TB infection almost five times more than a control population [20]. A recent meta-analysis found that in high TB prevalence countries, 81 % of active TB disease cases in health care workers was attributable to exposure in their work environment [21]. When active surveillance of health care workers is undertaken, undiagnosed pulmonary disease is not uncommon, and of those with active pulmonary TB multidrug resistant strains comprise an important component [22–24]. Rates of admission to hospital for TB were evaluated in Kwa Zulu-Natal and the estimated incidence of MDR TB hospitalization for HCW was more than five times that of the non-health care worker population and HCW represented a significant proportion of the XDR cases [25]. Universal screening for TB at the workplace, undifferentiated by HIV status is now recommended by the WHO [26] although few resource limited countries undertake regular screening [6, 27] of any type.
Evaluation of adherence to specific recommendations will be a helpful next step at the DAIDS funded clinical research sites. Documentation of adherence to SOPs and other surveillance activities will identify other gaps at a site level and continued surveillance of the aggregate performance will provide important information that will allow for the deployment of targeted resources. Biologically relevant surrogate markers for assessing the success of IC measures remain elusive in the outpatient environment, although a decrease in new cases of TB infection and disease in HCW has been proposed as a measurement of TB IC success [15, 27–31]. Quantification on a population level of TB burden using various methodologies including Xpert probe frequency is a novel technique that may provide additional information [32].
Conclusions
In our study the presence of an IC practitioner was more likely to be associated with the availability of basic elements of IC practice, however this was less influential on overall TB specific IC practices than we expected. It may be that the role and job description of the IC officer needs to be standardized and ownership of the principles by the entire site staff may be required. Some experts have argued that the implementation of administrative level controls such as the identification and isolation of individuals with cough and the provision of preventive and care services for health care workers should be prioritized [6, 11], however the contribution of each component of an effective IC program has not been evaluated and it may be that the presence of managerial support of resources including commitment to the establishment, implementation and monitoring of IC policies is critical. Our study lends credence to this notion, and suggests that support of an individual specifically tasked with IC activities may improve the overall quality of care at and reduce nosocomial transmission of infections to HCW and trial participants. Regular TB surveillance of health care workers, site study personnel and research participants is clearly an important component of IC practice in resource limited settings and may provide an outcome measure of IC activities. Inculcating a best practices culture of infection prevention and continuous quality improvement will help ensure that all site personnel adhere to and benefit from basic IC principles. A research agenda for TB IC in areas of high prevalence is critically needed in order to prioritize efforts and to focus attention on this acute need.
Abbreviations
ACTG, AIDS Clinical Trials Group; CDC, centers for disease control; CXR, chest radiograph; DAIDS, NIAID Division of AIDS; HCW, Health Care Workers; HIV, Human Immunodeficiency Virus; IC, infection control; IMPAACT, International Maternal Pediatric, Adolescent AIDS Clinical Trials Network; IPT, isoniazid prevention therapy; LMIC, low and middle income countries; NIAID, National Institute of Allergy and Infectious Diseases; PEP, post-exposure prophylaxis; PPE, personal protective equipment; SOP, standard operating procedure; TB, Mycobacterium tuberculosis; UV, ultraviolet; WHO, World Health Organization
References
Klevens RM, Edwards JR, Richards Jr CL, Horan TC, Gaynes RP, Pollock DA, et al. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep (Washington, DC: 1974). 2007;122(2):160–6.
Dixon RE. Control of health-care-associated infections, 1961–2011. Morbidity and mortality weekly report. Surveill Summ (Washington, DC: 2002). 2011;60 Suppl 4:58–63.
Swensen SJ, Dilling JA, Mc Carty PM, Bolton JW, Harper Jr CM. The business case for health-care quality improvement. J Patient Saf. 2013;9(1):44–52. doi:10.1097/PTS.0b013e3182753e33.
Allegranzi B, Bagheri Nejad S, Combescure C, Graafmans W, Attar H, Donaldson L, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377(9761):228–41. doi:10.1016/S0140-6736(10)61458-4.
Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, Lalloo U, et al. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet. 2006;368(9547):1575–80. doi:10.1016/s0140-6736(06)69573-1.
Menzies D, Joshi R, Pai M. Risk of tuberculosis infection and disease associated with work in health care settings. Int J Tuberc Lung Dis. 2007;11(6):593–605.
Jensen PA, Lambert LA, Iademarco MF, Ridzon R. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Recommendations and Reports. 2005;54(Rr-17):1–141.
WHO. WHO Guidelines Approved by the Guidelines Review Committee. WHO Policy on TB Infection Control in Health-Care Facilities, Congregate Settings and Households. Geneva: World Health Organization Copyright (c) World Health Organization 2009; 2009.
CDC. TB Infection Control M&E Tool for Clinical Sites. MMWR. 2010. http://www.cdc.gov/globalaids/resources/pmtct-care/docs/focused-monitoring-tool.pdf. Accessed 23 Nov 2014.
Title 42 - Public HealthVolume: 5Title: Section 482.42 - Condition of participation: Infection control. 42 CFR 482.42 - Condition of participation: Infection control. 2011.
Reid MJ, Saito S, Nash D, Scardigli A, Casalini C, Howard AA. Implementation of tuberculosis infection control measures at HIV care and treatment sites in sub-Saharan Africa. Int J Tuberc Lung Dis. 2012;16(12):1605–12. doi:10.5588/ijtld.12.0033.
Kuyinu YA, Mohammed AS, Adeyeye OO, Odugbemi BA, Goodman OO, Odusanya OO. Tuberculosis infection control measures in health care facilities offering tb services in Ikeja local government area, Lagos, South West Nigeria. BMC Infect Dis. 2016;16:126. doi:10.1186/s12879-016-1453-y.
Dokubo EK, Odume B, Lipke V, Muianga C, Onu E, Olutola A, et al. Building and Strengthening Infection Control Strategies to Prevent Tuberculosis - Nigeria, 2015. MMWR Morb Mortal Wkly Rep. 2016;65(10):263–6. doi:10.15585/mmwr.mm6510a3.
Farley JE, Tudor C, Mphahlele M, Franz K, Perrin NA, Dorman S, et al. A national infection control evaluation of drug-resistant tuberculosis hospitals in South Africa. Int J Tuberc Lung Dis. 2012;16(1):82–9. doi:10.5588/ijtld.10.0791.
Claassens MM, van Schalkwyk C, du Toit E, Roest E, Lombard CJ, Enarson DA, et al. Tuberculosis in healthcare workers and infection control measures at primary healthcare facilities in South Africa. PLoS One. 2013;8(10), e76272. doi:10.1371/journal.pone.0076272.
Godfrey C, Villa C, Dawson L, Swindells S, Schouten JT. Controlling healthcare-associated infections in the international research setting. J Acquir Immune Defic Syndr. 2013;62(4):e115–8. doi:10.1097/QAI.0b013e3182845b95.
Hyder AA, Dawson L. Defining standard of care in the developing world: the intersection of international research ethics and health systems analysis. Dev World Bioeth. 2005;5(2):142–52. doi:10.1111/j.1471-8847.2005.00109.x.
Sydnor ER, Perl TM. Hospital epidemiology and infection control in acute-care settings. Clin Microbiol Rev. 2011;24(1):141–73. doi:10.1128/cmr.00027-10.
Finch R. Current challenges in antimicrobial resistance and healthcare-associated infections: role and organization of ARHAI. J Antimicrob Chemother. 2012;67 Suppl 1:i3–10. doi:10.1093/jac/dks204.
McCarthy KM, Scott LE, Gous N, Tellie M, Venter WDF, Stevens WS, et al. High incidence of latent tuberculous infection among South African health workers: an urgent call for action. Int J Tuberc Lung Dis. 2015;19(6):647–53. doi:10.5588/ijtld.14.0759.
Baussano I, Nunn P, Williams B, Pivetta E, Bugiani M, Scano F. Tuberculosis among health care workers. Emerg Infect Dis. 2011;17(3):488–94. doi:10.3201/eid1703.100947.
Misquita D et al. Saving those who save lives! Integrated approach to surveillance of TB among Health Care Workers in a TB hospital in Mumbai. 45th World Congress on Lung Health of the International Union against Tuberculosis and Lung Disease; Nov 2014. Tuber Lung Dis. 2014;122(2):160–6.
Matsebula M et al. TB Screening for Health Care workers in Swaziland. 45th World Congress on Lung Health of the International Union against Tuberculosis and Lung Disease; Barcelona. Tuber Lung Dis. 2014;122(2):160–6.
Nunes G et al. Analysis of Occupational Tuberculosis in the Brazilian National Recording System 2007–2011. 45th World Congress on Lung Health of the International Union against Tuberculosis and Lung Disease; Barcelona. Tuber Lung Dis. 2014;122(2):160–6.
O'Donnell MR, Jarand J, Loveday M, Padayatchi N, Zelnick J, Werner L, et al. High incidence of hospital admissions with multidrug-resistant and extensively drug-resistant tuberculosis among South African health care workers. Ann Intern Med. 2010;153(8):516–22. doi:10.7326/0003-4819-153-8-201010190-00008.
Buregyeya E, Nuwaha F, Wanyenze RK, Mitchell EM, Criel B, Verver S, et al. Utilization of HIV and tuberculosis services by health care workers in Uganda: implications for occupational health policies and implementation. PLoS One. 2012;7(10), e46069. doi:10.1371/journal.pone.0046069.
Joshi R, Reingold AL, Menzies D, Pai M. Tuberculosis among health-care workers in low- and middle-income countries: a systematic review. PLoS Med. 2006;3(12), e494. doi:10.1371/journal.pmed.0030494.
van Rie A, McCarthy K, Scott L, Dow A, Venter WD, Stevens WS. Prevalence, risk factors and risk perception of tuberculosis infection among medical students and healthcare workers in Johannesburg, South Africa. S Afr Med J. 2013;103(11):853–7. doi:10.7196/samj.7092.
Mirtskhulava V, Whitaker JA, Kipiani M, Harris DA, Tabagari N, Owen-Smith AA et al. Determinants of Tuberculosis Infection Control-Related Behaviors Among Healthcare Workers in the Country of Georgia. Infect Control Hosp Epidemiol. 2015:1–7. doi:10.1017/ice.2015.5
Whitaker JA, Mirtskhulava V, Kipiani M, Harris DA, Tabagari N, Kempker RR, et al. Prevalence and incidence of latent tuberculosis infection in georgian healthcare workers. PLoS One. 2013;8(3):e58202. doi:10.1371/journal.pone.0058202.
Jones López E, Ellner J. Tuberculosis infection among HCWs. Int J Tuberc Lung Dis. 2005;9(6):591.
Scott LE CB, Van Rie A, Gous N, Molapo S, Erasmus L, Stevens W. Exploring the Value of the Xpert MTB/RIF Probe Frequencies and Cycle Threshold Data for Surveillance Purposes. Seattle: CROI; 2012.
Acknowledgements
This paper was written by CCG and GT in their capacity as NIH employees, but the views expressed in this paper do not necessarily represent those of the NIH.
Members of the HANC TBDLWG: Debra Benator MD, Constance Benson MD, Robert Coombs MD, PhD, FRCPC, Peggy Coulter MDE MT, Janice Darden MS, Anne Marie Demers MD, FRCPC, Joan Dragavon MLM, Constance Ducar, Kathleen Eisenach PhD, Carrie Frye, Morgan Gapara, Catherine Godfrey, Amy James Loftis, Vandana Kulkarni MS, Christopher Lane, Daniella Livnat, Annie Luetkemeyer MD, Peter Meewes, Beverly Metchock, Kurt, Michael M.Ed MT (ASCP), Mark Nicol Ph.D, Savita Pahwa MD, Anne Purfield Ph.D, Jeffrey Schouten, MD, JD, Lesley Scott PhD, Dave Shugarts, Donna Smith, Wendy Stevens MBBch, MMed (Haem), FCPath (Haem), Susan Swindells MBBS, Gail Tauscher BSN, Nicole Tobin MD, Frances Whalen MPH, MT (ASCP), Sharon Williams BS Carolyn Yanovich.
Funding
The project described was supported by Award Number UM1-AI-068636; UM1-AI-106701 from the National Institute of Allergy and Infectious Diseases and supported by National Institute of Mental Health (NIMH), National Institute of Dental and Craniofacial Research (NIDCR). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Allergy and Infectious Diseases or the National Institutes of Health.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article and its Additional file.
Authors’ contributions
All authors (CG,GT,SH,MA,LS,JTS,AL,CB,RC,SS) contributed to the design of the survey tool and performed real time analysis of results. CG and GT collated and tabulated the results. SH performed the statistical analysis, CG conceived and made the first draft of the manuscript, all authors contributed edited and approved the final manuscript (CG,GT,SH,MA,LS,JTS,AL,CB,RC,SS).
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
No ethics approval or consent was required as this was not human subject research.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional file
Additional file 1:
Clinical site tuberculosis (TB) infection control checklist. (PDF 405 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Godfrey, C., Tauscher, G., Hunsberger, S. et al. A survey of tuberculosis infection control practices at the NIH/NIAID/DAIDS-supported clinical trial sites in low and middle income countries. BMC Infect Dis 16, 269 (2016). https://doi.org/10.1186/s12879-016-1579-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-016-1579-y