
Abstract
Background
Previous studies reported that the incidence of intestinal spirochetosis was high in homosexual men, especially those with Human Immunodeficiency Virus infection. The aim of the present study was to clarify the clinicopathological features of intestinal spirochetosis in Japan with special reference to Human Immunodeficiency Virus infection status and species types.
Methods
A pathology database search for intestinal spirochetosis was performed at Tokyo Metropolitan Cancer and Infectious Disease Center Komagome Hospital between January 2008 and October 2011, and included 5265 consecutive colorectal biopsies from 4254 patients. After patient identification, a retrospective review of endoscopic records and clinical information was performed. All pathology slides were reviewed by two pathologists. The length of the spirochetes was measured using a digital microscope. Causative species were identified by polymerase chain reaction.
Results
Intestinal spirochetosis was diagnosed in 3 out of 55 Human Immunodeficiency Virus-positive patients (5.5%). The mean length of intestinal spirochetes was 8.5 μm (range 7–11). Brachyspira pilosicoli was detected by polymerase chain reaction in all 3 patients. Intestinal spirochetosis was also diagnosed in 73 out of 4199 Human Immunodeficiency Virus-negative patients (1.7%). The mean length of intestinal spirochetes was 3.5 μm (range 2–8). The species of intestinal spirochetosis was identified by polymerase chain reaction in 31 Human Immunodeficiency Virus-negative patients. Brachyspira aalborgi was detected in 24 cases (78%) and Brachyspira pilosicoli in 6 cases (19%). Both Brachyspira aalborgi and Brachyspira pilosicoli were detected in only one Human Immunodeficiency Virus-negative patient (3%). The mean length of Brachyspira aalborgi was 3.8 μm, while that of Brachyspira pilosicoli was 5.5 μm. The length of Brachyspira pilosicoli was significantly longer than that of Brachyspira aalborgi (p < 0.01). The lengths of intestinal spirochetes were significantly longer in Human Immunodeficiency Virus-positive patients than in Human Immunodeficiency Virus-negative patients (p < 0.05).
Conclusions
The incidence of intestinal spirochetosis was slightly higher in Human Immunodeficiency Virus-positive patients than in Human Immunodeficiency Virus-negative patients. However, no relationship was found between the Human Immunodeficiency Virus status and intestinal spirochetosis in Japan. Brachyspira pilosicoli infection may be more common in Human Immunodeficiency Virus-positive patients with intestinal spirochetosis than in Human Immunodeficiency Virus-negative patients with intestinal spirochetosis.
Similar content being viewed by others


Background
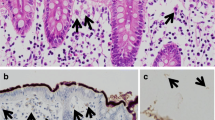
Intestinal spirochetosis (IS) is a condition in which colonic and appendiceal epithelial cells are colonized by one of two anaerobic spirochetes, either Brachyspira aalborgi, measuring 2 to 6 μm in length, or Brachyspira pilosicoli, measuring 4 to 20 μm in length (Figure 1) [1,2]. These two species may be zoonotic because they have previously been isolated from the feces of non-human primates and other animals [3]. However, it has yet to be determined whether IS is a pathogen or commensal inhabitant [4-6].

Microscopic appearance of intestinal spirochetosis. (H&E staining) ABrachyspira aalborgi. Basophilic fringes measuring 2 to 6 micrometers in length were observed on the surface epithelium. BBrachyspira pilosicoli. Basophilic fringes measuring 4 to 20 micrometers in length were observed on the surface epithelium.
Previous studies reported that the incidence of IS was high in homosexual men, especially those with Human Immunodeficiency Virus (HIV) [7-10]. Although IS is generally considered to be associated with immunocompromised states such as HIV infection, it has also been detected in patients with a normal immune status [5,11-13]. The incidence of IS in HIV-positive patients has not yet been reported in Japan. Furthermore, the prevalence of these species in HIV-positive patients remains unclear [11,13-15]. Therefore, the aim of the present study was to clarify the clinicopathological features of IS in Japan with special reference to HIV infection status and species types.
Methods
This study was approved by the Research Ethics Committees at the Tokyo Metropolitan Cancer and Infectious Disease Center Komagome Hospital, and performed according to its guidance. Informed consent was obtained from all participants. A pathology database search for IS was performed at the Tokyo Metropolitan Cancer and Infectious Disease Center Komagome Hospital between January 2008 and October 2011, and included 5265 consecutive colorectal biopsies from 4254 patients. Patients consisted of 2558 men and 1696 women, whose age ranged between 9 and 93 years with a mean age of 64 years. Fifty-five of these patients were HIV-positive (1.3%) and 4199 were HIV-negative (98.7%). After patient identification, a retrospective review of endoscopic records and clinical information was performed.
The database search identified 76 patients with IS. All pathology slides were collected and reviewed by two pathologists (YT and NF). All specimens were stained with hematoxylin and eosin and examined under X 400 magnification. IS was identified by characteristic basophilic fringes on the surface epithelium [13]. Immunostaining for spirochetosis was performed an antibody against Treponema pallidum (polyclonal, dilution 1:300; Concord CA, Biocare Medical) where necessary to confirm or refute the diagnosis. The lengths of spirochetes were measured using a digital microscope (Leica DMD 108).
Causative species were identified by PCR, which amplified the species-specific portion of the 16S ribosomal RNA gene. DNA from paraffin-embedded samples was extracted using NucleoSpin Tissue (MACHEREY-NAGEL, Duren, Germany). Pairs of primers were designed to detect the genes for 16S ribosome RNA (16S rRNA) and NADH oxidase (nox) in B. aalborgi and B. pilosicoli according to the method described by Mikosza et al. [16]. The integrity of paraffin-derived DNA was evaluated by PCR for D8S348. The sequence of primers and size of products are listed in Table 1.
All statistical analyses were performed using the JMP statistics software package (SAS; version 9.0.2). The relationship between IS and clinicopathological characteristics was assessed. Comparisons between two groups were analyzed with the Chi-square test. Differences were considered significant when the probability value was < 0.05.
Results
IS was detected in 76 out of 4254 patients (1.7%) by hematoxylin and eosin staining. Immunostaining for spirochetosis was performed to confirm this diagnosis in 8 cases. No cases were excluded by spirochetosis immunostaining. Patients with IS consisted of 58 men and 18 women, whose age ranged from 30 to 83 years with a mean age of 59.3 years. IS was diagnosed in 3 out of 55 HIV-positive patients (5.5%), and 73 out of 4199 HIV-negative patients (1.7%). A correlation was found between IS and sex (p < 0.01) and age (p < 0.01) (Table 2). No significant difference was found between the HIV status and IS (p = 0.09).
IS was identified by characteristic 2–11 -μm-thick basophilic fringes on the luminal surface of the epithelium. The mean lengths of IS were 8.5 μm in HIV-positive patients and 3.5 μm in HIV-negative patients. The length of IS was significantly longer in HIV-positive patients than in HIV-negative patients (p < 0.05).
The identification of species by PCR amplification was assessed in 76 cases. Products of the gene for 16S rRNA in B. aalborgi were detected in 24 cases. Products of the gene for 16S rRNA in B. pilosicoli were detected in 9 cases. Both products of the genes for B. aalborgi and B. pilosicoli were detected in 1 case. The integrity of paraffin-derived DNA was evaluated by PCR for D8S348 in 42 cases which were negative for B. aalborgi and B. pilosicoli. In 31 out of 42 cases, D8S348 was not amplified suggesting the quality of DNA was insufficient. In remaining 11 cases, DNA extracted from IS in infected human tissue samples may be too small in relative amount or too poor in quality. Another possibility is these cases may have contained other species of spirochetes that have yet to be characterized [17]. The length of IS was shown in Table 3. The mean length of B. aalborgi was 3.8 μm (range 2–4.5) and the mean length of B. pilosicoli was 5.5 μm (range 3.2-11). The length of IS was 2.5 μm in patients with B. aalborgi and B. pilosicoli. The length of B. pilosicoli was significantly longer than that of B. aalborgi (p < 0.01).
B. pilosicoli was detected in all 3 IS cases with HIV (100%). In HIV-negative patients, B. aalborgi was detected in 24 cases (78%) and B. pilosicoli was detected in 6 cases (19%). Both B. aalborgi and B. pilosicoli were detected in only one HIV-negative patient (3%). All 3 HIV-positive IS patients were male, not severely immunosuppressed (CD4 lymphocyte cells; 668/μL, 798/μL and 317/μL), had no other HIV-associated complications, showed no histological abnormalities other than IS, and had watery diarrhea. Most HIV-negative IS patients had no clinical symptoms. Forty-seven patients underwent a screening exam. Twelve patients underwent colonoscopy as a hemoccult-positive rectal examination. Two patients had hemorrhoids and one had ulcerative colitis. Eleven HIV-negative IS patients had clinical symptoms (15%); 6 had abdominal pain, 4 had diarrhea or loose stools, and 1 had abdominal pain and diarrhea. A correlation was found between the clinical symptoms and HIV status of IS patients (p < 0.01). The characteristics of IS patients with clinical symptoms were shown in Table 4. IS patients with clinical symptoms consisted of 10 men and 4 women, whose age ranged from 43 to 73 years with a mean age of 57.1 years. Endoscopically, tubular adenoma, or sessile serrated adenoma or adenocarcinoma was detected in 10 out of 14 cases, whereas no specific endoscopic findings were found in 4 out of 14 cases. The mean length of IS was 4.5 μm (range 2.5-11). B. pilosicoli was detected in all 3 HIV-positive patients. Each species was successfully identified in 6 out of 11 HIV-negative IS cases with clinical symptoms. B. aalborgi was detected in 3 cases and B. pilosicoli was detected in 2 cases. Both B. aalborgi and B. pilosicoli were detected in 1 case.
Discussion
The prevalence of IS was previously reported to be between 2 and 7% in Western countries and 11-34% in less developed countries [18,19]. Our study revealed that the incidence of IS in Japan was 1.7%, which was similar to that in Western countries. The prevalence of IS was previously reported to be approximately 54% in men who have sex with men (MSM) and HIV-positive patients [9,18,20]. On the other hand, Orenstein et al. identified four patients with IS among 82 HIV-positive patients [21]. Our study revealed that the incidence of IS was slightly higher in HIV-positive patients than in HIV-negative patients; however, no correlation was found between the HIV status and IS in Japan. Fifty-five HIV-positive and 4199 HIV-negative patients were evaluated in our study, which was one of the largest reported series of IS in HIV-positive and HIV-negative patients at a single institution.
Previous studies showed that the length of B. aalborgi was 2 to 6 μm and B. pilosicoli was 4 to 20 μm [1,2]. In patients in which the species was identified by PCR amplification, the length of B. aalborgi was 2 to 4.5 μm and B. pilosicoli was 2.5 to 11 μm. The length of B. pilosicoli was significantly longer than that of B. aalborgi (p < 0.01), which was consistent with the findings of previous studies. Furthermore, the length of IS in HIV-positive patients was significantly longer than that of IS in HIV-negative patients (p < 0.05).
B. aalborgi has been confirmed as the most prevalent species in Western countries and Japan, while B. pilosicoli is rare [6,13]. In the present study, B. pilosicoli was detected in all 3 HIV-positive patients. The results of the present study suggest that B. pilosicoli infections were more common in HIV-positive patients with IS while B. aalborgii infections may be more common in HIV-negative patients with IS in Japan. The prevalence of these species in HIV-positive patients has not yet been examined in detail [11,13-15]. To the best of our knowledge, this is the first study to show that B. pilosicoli infections may be more common in HIV-positive patients with IS based on one of the largest series composed of HIV-positive and HIV-negative patients examined at a single institution.
All 3 HIV-positive patients with IS in this study were male, less severely immunosuppressed, and had watery diarrhea. Anthony et al. reported that three HIV-positive IS patients were symptomatic with diarrhea [22]. A previous study demonstrated that IS caused chronic diarrhea in HIV-positive men who have sex with men, but were not severely immunosuppressed (CD4 lymphocyte cells >200/ μL) [20]. The clinicopathological findings of IS cases in our study were similar to these findings.
B. aalborgi is generally considered to be a non-pathogenic commensal, while B. pilosicoli is an opportunistic pathogen [23]. All three HIV-positive patients with B. pilosicoli in our study had watery diarrhea. In HIV-negative patients, B. pilosicoli was more commonly detected in patients with clinical symptoms (50%) than in patients without clinical symptoms (16%). Furthermore, the prevalence of B. pilosicoli was markedly higher in patients with clinical symptoms than in patients without clinical symptoms (p = 0.02). This result supports the pathogenic potential of B. pilosicoli. Since the number of patients was too small to clarify the clinical significance of B. pilosicoli infection, further investigations are required.
Conclusion
In this study, we revealed the clinicopathological features of IS in Japan. The incidence of IS was slightly higher in HIV-positive patients than in HIV-negative patients. However, no relationship was found between the HIV status and IS. Brachyspira pilosicoli infection may be more common in HIV-positive patients with IS than in HIV-negative patients with IS.
References
Smith JL. Colonic spirochetosis in animals and humans. J Food Prot. 2005;68(7):1525–34.
Takeuchi A, Jervis HR, Nakazawa H, Robinson DM. Spiral-shaped organisms on the surface colonic epithelium of the monkey and man. Am J Clin Nutr. 1974;27(11):1287–96.
Stephens CP, Hampson DJ. Intestinal spirochete infections of chickens: a review of disease associations, epidemiology and control. Anim Health Res Rev. 2001;2(1):83–91.
Esteve M, Salas A, Fernandez-Banares F, Lloreta J, Marine M, Gonzalez CI, et al. Intestinal spirochetosis and chronic watery diarrhea: clinical and histological response to treatment and long-term follow up. J Gastroenterol Hepatol. 2006;21(8):1326–33.
Carr NJ, Mahajan H, Tan KL, Sharma R. The histological features of intestinal spirochetosis in a series of 113 patients. Int J Surg Pathol. 2010;18(2):144–8.
Mikosza AS, Hampson DJ. Human intestinal spirochetosis: Brachyspira aalborgi and/or Brachyspira pilosicoli? Ani Health Res Rev. 2001;2(1):101–10.
Surawicz CM, Roberts PL, Rompalo A, Quinn TC, Holmes KK, Stamm WE. Intestinal spirochetosis in homosexual men. Am J Med. 1987;82(3 Spec No):587–92.
Trivett-Moore NL, Gilbert GL, Law CL, Trott DJ, Hampson DJ. Isolation of Serpulina pilosicoli from rectal biopsy specimens showing evidence of intestinal spirochetosis. J Clin Microbiol. 1998;36(1):261–5.
Fenoglio-Preiser CM, Noffsinger AE, Stemmermann GN, Lantz PE, Isaacson PG. Gastrointestinal Pathology an Atlas and Text Third Edition. Philadelphia: Lippincott Williams & Wilkins; 2007. p. 816.
Law CL, Grierson JM, Stevens SM. Rectal spirochaetosis in homosexual men: the association with sexual practices, HIV infection and enteric flora. Genitourin Med. 1994;70(1):26–9.
Koteish A, Kannangai R, Abraham SC, Torbenson M. Colonic spirochetosis in children and adults. Am J Clin Pathol. 2003;120(6):828–32.
Calderaro A, Bommezzadri S, Gorrini C, Piccolo G, Peruzzi S, Villanacci V, et al. Infective colitis associated with human intestinal spirochetosis. J Gastroenterol Hepatol. 2007;22(11):1772–9.
Tanahashi J, Daa T, Gamachi A, Kashima K, Kondoh Y, Yada N, et al. Human intestinal spirochetosis in Japan; its incidence, clinicopathologic features, and genotypic identification. Mod Pathol. 2008;21(2):76–84.
Mikosza AS, La T, de Boer WB, Hampson DJ. Comparative prevalences of Brachyspira aalborgi and Brachyspira (Serpulina) pilosicoli as etiologic agents of histologically identified intestinal spirochetosis in Australia. J Clin Microbiol. 2001;39(1):347–50.
Higashiyama M, Ogata S, Adachi Y, Nishiyama J, Ohara I, Okamura M, et al. Human intestinal spirochetosis accompanied by human immunodeficiency virus infection: a case report. Acta Med Okayama. 2009;63(4):217–21.
Mikosza AS, La T, Brooke CJ, Lindboe CF, Ward PB, Heine RG, et al. PCR amplification from fixed tissue indicates frequent involvement of Brachyspira aalborgi in human intestinal spirochetosis. J Clin Microbiol. 1999;37(6):2093–8.
Mikosza AS, Munshi MA, Hampson DJ. Analysis of genetic variation in Brachyspira aalborgi and related spirochaetes determined by partial sequencing of the 16S rRNA and NADH oxidase genes. J Med Microbiol. 2004;53(Pt 4):333–9.
Korner M, Gebbers JO. Clinical significance of human intestinal spirochetosis–a morphologic approach. Infection. 2003;31(5):341–9.
Christie JD. Intestinal spirochetes. Organisms in search of a disease? Am J Clin Pathol. 2003;120(6):820–1.
Ena J, Simon-Aylon A, Pasquau F. Intestinal spirochetosis as a cause of chronic diarrhoea in patients with HIV infection: case report and review of the literature. Int J STD AIDS. 2009;20(11):803–5.
Orenstein JM, Dieterich DT. The histopathology of 103 consecutive colonoscopy biopsies from 82 symptomatic patients with acquired immunodeficiency syndrome: original and look-back diagnoses. Arch Pathol Lab Med. 2001;125(8):1042–6.
Anthony NE, Blackwell J, Ahrens W, Lovell R, Scobey MW. Intestinal spirochetosis: an enigmatic disease. Dig Dis Sci. 2013;58(1):202–8.
Duhamel GE. Comparative pathology and pathogenesis of naturally acquired and experimentally induced colonic spirochetosis. Anim Health Res Rev. 2001;2(1):3–17.
Acknowledgements
The authors are grateful to staff of Tokyo Metropolitan Cancer and Infectious Disease Center Komagome Hospital for their unreserved help and facilitation of this study.
Presented at the 2012 American Society of Clinical Pathology Annual Meeting, October 31 to November 2, and was a finalist in the Best poster Submitted From Outside the U.S. Award Competition.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YT, MT, SH, NF, OK, KK, TH and KO. NF proposed the initial idea for the study. YT and NF reviewed all pathology slides. YT carried out the molecular genetic studies, participated in the extracting DNA from paraffin-embedded samples and identifying the species by PCR, and drafted the manuscript. KK recorded endoscopic reports and clinical information. YT and MT performed the statistical analysis. SH, OK, TH and KO conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscripts.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Tateishi, Y., Takahashi, M., Horiguchi, Si. et al. Clinicopathologic study of intestinal spirochetosis in Japan with special reference to human immunodeficiency virus infection status and species types: analysis of 5265 consecutive colorectal biopsies. BMC Infect Dis 15, 13 (2015). https://doi.org/10.1186/s12879-014-0736-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-014-0736-4