
Abstract
Background
This study investigated the molecular characteristics of azithromycin-resistant Streptococcus pneumoniae in Taiwan.
Methods
A total of 486 non-duplicate isolates of azithromycin-resistant S. pneumoniae recovered from various clinical sources of patients treated at 22 different hospitals in Taiwan from 2006 to 2010. The presence of erm(B) and mef(A) genes using duplex PCR, multilocus sequence typing (MLST), and pulsed-field gel electrophoresis of these isolates were studied.
Results
Of the isolates tested, 59% carried the erm(B) gene, 22% carried the mef(A) gene, and 19% carried both genes. The prevalence of isolates carrying the erm(B) and mef(A) genes increased from 10% (11/110) in 2006 to 25% (15/60) in 2010 (p-value = 0.0136). The majority of isolates carrying both erm(B) and mef(A) genes belonged to serotypes 19 F (64%) followed by 19 F A (24%). Of these isolates, 33% were sequence type 320 (ST320), 32% were ST236, and 12% were ST271.
Conclusions
The increase in incidence of mef(A)/erm(B)-positive azithromycin-resistant S. pneumoniae isolates during the study period was primarily due to serotypes 19 F and 19A and ST236 and ST320.
Similar content being viewed by others

Background
Streptococcus pneumoniae is a leading cause of bacterial pneumonia, meningitis, and sepsis worldwide. Since 1965, many cases of infections due to drug-resistant S. pneumoniae have been reported [1]. The emergence of antimicrobial resistance is correlated with selective pressure from the use, often inappropriate, of antimicrobial agents and results in increased mortality, morbidity, and health care costs [2]. Antibacterial resistance in S. pneumoniae is increasing, affecting principally β-lactams and macrolides (azithromycin, erythromycin, or clarithromycin) with prevalence ranging between 1% and 90% depending on the geographical area [3]. Fluoroquinolone resistance has also been reported in countries with high levels of antibacterial resistance and consumption [3].
Macrolide resistance in S. pneumoniae is most often mediated by two mechanisms: target-site modification encoded by the erm(B) gene and active drug efflux mediated by a membrane efflux pump encoded by mef-class genes [4]. Song et al. reported the erm(B) gene was found in >50% of pneumococcal isolates either alone or in combination with mef(A) among S. pneumoniae isolates from 10 Asian countries during 1998–2001 [5]. In Finland and Germany, the most frequent macrolide resistance determinant carried was the mef gene [6],[7]. Macrolide resistance among pneumococcal isolates in Alaska recovered from 1986–2010 was also reported to be predominantly mediated by mef genes and this has not changed significantly over time [8]. However, the authors of the study reported a significant increase in the proportion of isolates that possess both erm(B) and mef(A), primarily among serotype 19A isolates.
Bowers et al. reported that of 592 clinical pneumococcal isolates collected in Arizona from 1999 to 2008, all isolates carrying the erythromycin-resistant genes mef(E) and erm(B) were multidrug-resistant clonal lineages of Taiwan 19 F-14 and most were multilocus sequence type (ST) 320 [9]. In China, recent studies have shown that erythromycin-resistant isolates commonly carry both genes and that the majority of isolates belong to ST271, ST320, ST236, with clonal complex 271 (CC271) being the most frequently isolated CC [10]-[12]. In 2005, two predominant macrolide-resistant S. pneumoniae CCs, namely CC271 and CC15, were identified in New South Wales, Australia [13]. Recently, Tsai et al. reported the prevalence of serotype 19A pneumococcal isolates increased significantly in Taiwan from 2006 to 2010 and that more than 90% of the isolates were non-susceptible to azithromycin [14]. In the current study, we investigated the molecular characteristics of azithromycin-resistant S. pneumoniae recovered from various clinical sources of patients who were treated at 22 different hospitals in Taiwan from 2006 to 2010.
Methods
Bacterial isolates
A total of 530 consecutive and non-duplicate pneumococcal isolates were collected from various clinical specimens of patients treated at 22 different hospitals in Taiwan during a 3-month period per year, with a maximum number of isolates per year of 10 during 2006–2008 and 5 during 2009–2010 [14]. Among these isolates, 486 were not susceptible to azithromycin [14]. These pneumococcal isolates were collected as part of the Tigecycline In Vitro Surveillance in Taiwan (TIST) study, a nationwide, multicenter, prospective surveillance study conducted in 12 regional hospitals (500–1000 beds) and 10 medical centers (1200–3000 beds) (eight in northern, four in central, six in southern and two in eastern Taiwan) from January 2006 to December 2010 [15], Pneumococcal isolates were identified at each hospital and the identification was confirmed by the central laboratory at the National Taiwan University Hospital [15]. Serotype determination by a latex agglutination method and antimicrobial susceptibility testing by the broth microdilution method were performed as described previously [14]. Isolates were collected as part of standard patient care and no ethical approval required for your use.
Detection of erm(B) and mef(A) genes
The detection of erm(B) and mef(A) was performed by duplex PCR as previously described [5],[16].
Pulsed-field gel electrophoresis (PFGE) analysis
PFGE analysis of isolates was performed as described previously [17],[18]. The Dice coefficient of similarity was calculated and the unweighted pair group method with arithmetic averages (UPGMA) was used for cluster analysis. Isolates with coefficients of similarity ≥80% were considered to be the same cluster [18].
Multilocus sequence typing (MLST)
MLST was performed as described previously [19]. Allele profiles and sequence types were determined using the MLST database (http://spneumoniae.mlst.net/).
Statistical analysis
Statistical analyses were conducted using GraphPad Prism V5.0 (GraphPad Software, San Diego, CA, USA).
Results
Prevalence of isolates carrying the erm(B) and mef(A)genes
Among the 486 isolates, 59% carried the erm(B) gene, 22% carried the mef(A) gene, and 19% carried both genes (Table 1). The prevalence of isolates carrying the erm(B) gene did not differ significantly from year to year (p-value = 0.2436) (Table 1); the prevalence of isolates carrying the mef(A) gene declined significantly from 30% in 2006 to 5% in 2010 (p-value = 0.0001); and the prevalence of isolates carrying both genes increased significantly from 10% in 2006 to 25% in 2010 (p-value = 0.0136) (Table 1). There were no obvious geographic differences with respect to the distribution of isolates carrying erm(B), mef(A), or both genes (data not shown).
Serotype and sequence type of isolates carrying both erm(B) and mef(A) genes
All isolates of serotype 3 and 15B carried only erm(B) (Table 2). The majority of the other main serotypes also carried only the erm(B) gene, namely serotype 23 F (73%), 14 (87%), 23A (86%), and 6B (54%) (Table 2). Among serotype 19 F isolates, 13% carried the erm(B) gene, 36% carried the mef(A) gene, and 52% carried both genes. The majority of serotype 19A isolates carried both erm(B) and mef(A) genes (61%) (Table 2). Of 91 these isolates carried both genes, 58 (64%) of isolates were belong to serotype 19 F, followed by 19A (22/91; 24%).
The distribution of isolates harboring erm(B) and mef(A) genes by sequence type was 33% for ST320, 32% for ST236, 12% for ST271, 8% for ST81, 2% for ST283 and ST8525, and 11% for other sequence types (Table 3). The majority of ST236 (28/29) and ST271 (10/11) clones belonged to serotype 19 F. Isolates of clone ST320 mainly belonged to serotype 19 F (16/30) and serotype 19A (13/30) (Table 3). Seven isolates of clone ST81 were identified as belonging to serotype 23 F (n = 2), 23A (n = 1) and 6A (n = 4). Based on the results of MLST allelic profiling, the ST236 and ST81 clones were identified as reference strain of PMEN global clone Taiwan19F-14 and reference strain of PMEN global clone Spain23F-1 respectively (Table 3). ST320 and ST271 clones were identified as a double-locus variant (DLV) and a single-locus variant (SLV) of the worldwide-established Taiwan19F-14 (ST236) clone respectively.
Clusters of isolates carrying both erm(B) and mef(A)genes
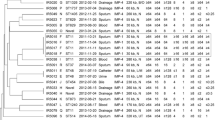
We constructed a phylogenetic tree based on PFGE profiles and found no specific clustering for the strains of serotype 19 F and 19A or for the three major sequence types (ST320, ST271, and ST236) (Figure 1). In this study, the isolates carrying both erm(B) and mef(A) were stratified into eight clusters (Cluster I to VIII) by PFGE (Figure 1 and Table 4). Clusters III, IV, V, and VII corresponded to the isolates with serotype 19 F (Table 4). Isolates belonging to the same cluster can have different serotypes and STs. Furthermore, several isolates with the same ST also exhibited different serotypes and pulsotypes. The majority of isolates of serotype 19A were in cluster VI (13/24, 54%). ST320 clone isolates belonged to cluster VI (13/24, 54%), cluster II (9/16, 56%), and cluster I (2/4, 50%). Meanwhile, isolates of clone ST236 were frequently clustered in cluster V (9/9, 100%) and III (6/7, 86%) (Table 4). The majority of ST81 clone isolates were clustered in cluster VIII (4/5, 80%).

A phylogenetic tree analysis based on pulsed-field gel electrophoresis profiles with Sma I among isolates of azithromycin-resistant Streptococcus pneumoniae carrying both erm(B)/mef(A) genes.
Discussion
Azithromycin is the most commonly used macrolide in the treatment of community-acquired pneumonia and other respiratory tract infections in Taiwan. The rate of susceptibility to azithromycin remained stationary from 2006 to 2010 in Taiwan, although the numbers of isolates randomly collected in 2009 and 2010 were lower than in 2006 to 2008 [14]. In Taiwan, PCV-7 vaccination was introduced in October 2005 and PCV-13 was introduced in July 2010. Nevertheless, some studies have shown that changes in antimicrobial susceptibility before and after implementation of the PCV-7 vaccine were not associated with serotypes [14]. Our finding of increase in the rate of azithromycin-resistant S. pneumoniae isolates carrying the erm(B) and mef(A) genes from from 10% in 2006 to 25% in 2010 after the introduction of the pneumococcal conjugate vaccine in Taiwan. These findings are in line with a previously published report on the PROTEKT US surveillance study from 10% in 2000 1 to 16% in 2003 [21], the study in Alaska from 0% in 1986 to 21% in 2010 [8], and the study in Canada from 3% in 1998 to 19% in 2008 [22].
In this study, the majority of azithromycin-resistant isolates carrying both mef(A) and erm(B) genes was serotype 19 F (58/91; 64%), followed by19A (22/91; 24%) and is similar to a previous published report in Korea, 57% of carried both genes were serotype 19 F (44/77, 57%), followed by 19A (21/77, 30%)7.5%) [23]. However, the study in Alaska showed 79% of isolates carrying both genes was serotype 19A (15/19), followed by 19 F (3/19; 16%) [8].
We investigated further via MLST and PFGE all isolates carried both the erm(B) and mef(A), and identified 33% of these to be of ST320, followed by ST236 (32%), ST271 (12%), and other STs (23%). Previously, it was reported in Taiwan that the CCs related to Spain23F-1, Taiwan19F-14, and Taiwan23F-15 were responsible for the spread of isolates with high-beta-lactam resistance [24],[25]. Recently, the S. pneumoniae serotype 19A ST320 clone, derived from an international Taiwan19F-14 (ST236) clone, has become prevalent in many countries, including Taiwan [25]. In Arizona, the isolates carrying both mef(E)/erm(B)-positive genes are multidrug-resistant clonal lineages of Taiwan19F-14 [9].
In the last two decades, PFGE and MLST have become the main genotyping methods for assessing the genetic diversity of isolates [26]. Although both methods are time- and labor-consuming, they are useful for studying the local and global epidemiology of S. pneumoniae. In the present study, discrepancies of typing results by these two methods occurred. Since pneumococci are capable of undergoing capsular switching and are recognized as one of the most recombinogenic bacteria, additional typing methods, i.e. multiple-locus variable number tandem repeat analysis and MILST, have been developed recently to offer better discrimination in S. pneumoniae isolates [26].
Conclusions
The increase in incidence of mef(A)- and erm(B)-positive azithromycin-resistant S. pneumoniae isolates during the study period was primarily due to serotypes 19 F and 19A and ST236 and ST320.
Abbreviations
- MLST:
-
Multilocus sequence typing
- TIST:
-
Tigecycline In Vitro Surveillance in Taiwan
- PCR:
-
Polymerase chain reaction
- ST:
-
Sequence type
- CC:
-
Clonal complex
- PFGE:
-
Pulsed-field gel electrophoresis
- UPGMA:
-
Unweighted pair group method with arithmetic averages
- PMEN:
-
Pneumococcal molecular epidemiology network
- DLV:
-
Double-locus variant
- SLV:
-
Single-locus variant
References
Hansman D, Bullen MM: A resistant pneumococcus. Lancet. 1967, 290: 264-265. 10.1016/S0140-6736(67)92346-X.
Li CF, Liu MF, Shi ZY, Hsueh PR, Liao CH, Jang TN, Tsao SM, Kung HC, Hsu GJ, Cheng YJ, Lin HC, Liu YC, Chuang YC, Wang LS, Chen CM: Changing trends in antimicrobial susceptibility of Streptococcus pneumoniae isolates in Taiwan, 2006–2007. J Microbiol Immunol Infect. 2012, 45: 305-310. 10.1016/j.jmii.2011.12.012.
Van Bambeke F, Reinert RR, Appelbaum PC, Tulkens PM, Peetermans WE: Multidrug-resistant Streptococcus pneumoniae infections: current and future therapeutic options. Drugs. 2007, 67: 2355-2382. 10.2165/00003495-200767160-00005.
Klugman KP, Lonks JR: Hidden epidemic of macrolide-resistant pneumococci. Emerg Infect Dis. 2005, 11: 802-807. 10.3201/eid1106.050147.
Song JH, Chang HH, Suh JY, Ko KS, Jung SI, Oh WS, Peck KR, Lee NY, Yang Y, Chongthaleong A, Aswapokee N, Chiu CH, Lalitha MK, Perera J, Yee TT, Kumararasinghe G, Jamal F, Kamarulazaman A, Parasakthi N, Van PH, So T, Ng TK, ANSORP Study Group: Macrolide resistance and genotypic characterization of Streptococcus pneumoniae in Asian countries: a study of the Asian Network for Surveillance of Resistant Pathogens (ANSORP). J Antimicrob Chemother. 2004, 53: 457-463. 10.1093/jac/dkh118.
Bley C, van der Linden M, Reinert RR: mef(A) is the predominant macrolide resistance determinant in Streptococcus pneumoniae and Streptococcus pyogenes in Germany. Int J Antimicrob Agents. 2011, 37: 425-431. 10.1016/j.ijantimicag.2011.01.019.
Siira L, Rantala M, Jalava J, Hakanen AJ, Huovinen P, Kaijalainen T, Lyytikäinen O, Virolainen A: Temporal trends of antimicrobial resistance and clonality of invasive Streptococcus pneumoniae isolates in Finland, 2002 to 2006. Antimicrob Agents Chemother. 2009, 53: 2066-2073. 10.1128/AAC.01464-08.
Rudolph K, Bulkow L, Bruce M, Zulz T, Reasonover A, Harker-Jones M, Hurlburt D, Hennessy T: Molecular resistance mechanisms of macrolide-resistant invasive Streptococcus pneumoniae isolates from Alaska, 1986 to 2010. Antimicrob Agents Chemother. 2013, 57: 5415-5422. 10.1128/AAC.00319-13.
Bowers JR, Driebe EM, Nibecker JL, Wojack BR, Sarovich DS, Wong AH, Brzoska PM, Hubert N, Knadler A, Watson LM, Wagner DM, Furtado MR, Saubolle M, Engelthaler DM, Keim PS: Dominance of multidrug resistant CC271 clones in macrolide-resistant Streptococcus pneumoniae in Arizona. BMC Microbiol. 2012, 12: 12-10.1186/1471-2180-12-12.
Li Y, Tomita H, Lv Y, Liu J, Xue F, Zheng B, Ike Y: Molecular characterization of erm(B)- and mef(E)-mediated erythromycin-resistant Streptococcus pneumoniae in China and complete DNA sequence of Tn2010. J Appl Microbiol. 2011, 110: 254-265. 10.1111/j.1365-2672.2010.04875.x.
Zhao C, Zhang F, Chu Y, Liu Y, Cao B, Chen M, Yu Y, Liao K, Zhang L, Sun Z, Hu B, Lei J, Hu Z, Zhang X, Wang H: Phenotypic and genotypic characteristic of invasive pneumococcal isolates from both children and adult patients from a multicenter surveillance in China 2005–2011. PLoS ONE 2013, 8.
Zhou L, Ma X, Gao W, Yao KH, Shen AD, Yu SJ, Yang YH: Molecular characteristics of erythromycin-resistant Streptococcus pneumoniae from pediatric patients younger than five years in Beijing, 2010. BMC Microbiol. 2012, 12: 228-10.1186/1471-2180-12-228.
Xu X, Cai L, Xiao M, Kong F, Oftadeh S, Zhou F, Gilbert GL: Distribution of serotypes, genotypes, and resistance determinants among macrolide-resistant Streptococcus pneumoniae isolates. Antimicrob Agents Chemother. 2010, 54: 1152-1159. 10.1128/AAC.01268-09.
Tsai HY, Chen YH, Liao CH, Lu PL, Huang CH, Lu CT, Chuang YC, Tsao SM, Chen YS, Liu YC, Chen WY, Jang TN, Lin HC, Chen CM, Shi ZY, Pan SC, Yang JL, Kung HC, Liu CE, Cheng YJ, Liu JW, Sun W, Wang LS, Ko WC, Yu KW, Chiang PC, Lee MH, Lee CM, Hsu GJ, Hsueh PR: Trends in the antimicrobial susceptibilities and serotypes of Streptococcus pneumoniae: results from the Tigecycline In Vitro Surveillance in Taiwan (TIST) study, 2006–2010. Int J Antimicrob Agents. 2013, 42: 312-316. 10.1016/j.ijantimicag.2013.05.013.
Chen YH, Lu PL, Huang CH, Liao CH, Lu CT, Chuang YC, Tsao SM, Chen YS, Liu YC, Chen WY, Jang TN, Lin HC, Chen CM, Shi ZY, Pan SC, Yang JL, Kung HC, Liu CE, Cheng YJ, Liu JW, Sun W, Wang LS, Ko WC, Yu KW, Chiang PC, Lee MH, Lee CM, Hsu GJ, Hsueh PR: Trends in the susceptibility of clinically important resistant bacteria to tigecycline: results from the Tigecycline In Vitro Surveillance in Taiwan study, 2006 to 2010. Antimicrob Agents Chemother. 2012, 56: 1452-1457. 10.1128/AAC.06053-11.
Ko KS, Song JH: Evolution of erythromycin-resistant Streptococcus pneumoniae from Asian countries that contains erm(B) and mef(A) genes. J Infect Dis. 2004, 190: 739-747. 10.1086/422156.
Hsueh PR, Teng LJ, Lee LN, Yang PC, Ho SW, Luh KT: Dissemination of high-level penicillin-, extended-spectrum cephalosporin-, and erythromycin-resistant Streptococcus pneumoniae clones in Taiwan. J Clin Microbiol. 1999, 37: 221-224.
Lefevre JC, Faucon G, Sicard AM, Gasc AM: DNA fingerprinting of Streptococcus pneumoniae strains by pulsed-field gel electrophoresis. J Clin Microbiol. 1993, 31: 2724-2728.
Enright MC, Spratt BG: A multilocus sequence typing scheme for Streptococcus pneumoniae: identification of clones associated with serious invasive disease. Microbiol Read Engl. 1998, 144 (Pt 11): 3049-3060. 10.1099/00221287-144-11-3049.
Mavroidi A, Paraskakis I, Pangalis A, Kirikou E, Charisiadou A, Athanasiou T, Tassios PT, Tzouvelekis LS: Spread of the Streptococcus pneumoniae Taiwan19F-14 clone among children in Greece. Clin Microbiol Infect. 2007, 13: 1213-1216. 10.1111/j.1469-0691.2007.01837.x.
Farrell DJ, Jenkins SG, Brown SD, Patel M, Lavin BS, Klugman KP: Emergence and spread of Streptococcus pneumoniae with erm(B) and mef(A) resistance. Emerg Infect Dis. 2005, 11: 851-858. 10.3201/eid1106.050222.
Wierzbowski AK, Karlowsky JA, Adam HJ, Nichol KA, Hoban DJ, Zhanel GG, Canadian Antimicrobial Resistance Alliance (CARA): Evolution and molecular characterization of macrolide-resistant Streptococcus pneumoniae in Canada between 1998 and 2008. J Antimicrob Chemother. 2014, 69: 59-66. 10.1093/jac/dkt332.
Bae S, Lee K: Distribution of capsular serotypes and macrolide resistance mechanisms among macrolide-resistant Streptococcus pneumoniae isolates in Korea. Diagn Microbiol Infect Dis. 2009, 63: 213-216. 10.1016/j.diagmicrobio.2008.10.002.
Ardanuy C, Rolo D, Fenoll A, Tarrago D, Calatayud L, Liñares J: Emergence of a multidrug-resistant clone (ST320) among invasive serotype 19A pneumococci in Spain. J Antimicrob Chemother. 2009, 64: 507-510. 10.1093/jac/dkp210.
Hsieh YC, Lin TL, Chang KY, Huang YC, Chen CJ, Lin TY, Wang JT: Expansion and evolution of Streptococcus pneumoniae serotype 19A ST320 clone as compared to its ancestral clone, Taiwan19F-14 (ST236). J Infect Dis. 2013, 208: 203-210. 10.1093/infdis/jit145.
Elberse KEM, Nunes S, Sá-Leão R, van der Heide HGJ, Schouls LM: Multiple-locus variable number tandem repeat analysis for Streptococcus pneumoniae: comparison with PFGE and MLST. PLoS One. 2011, 6: e19668-10.1371/journal.pone.0019668.
Acknowledgements
The TIST study team included Hsih-Yeh Tsai, Yen-Hsu Chen, Chun-Hsing Liao, Po-Liang Lu, Cheng-Hua Huang, Chin-Te Lu, Yin-Ching Chuang, Shih-Ming Tsao, Yao-Shen Chen, Yung-Ching Liu, Wei-Yu Chen, Tsrang-Neng Jang, Hsiu-Chen Lin, Chih-Ming Chen, Zhi-Yuan Shi, Sung-Ching Pan, Jia-Ling Yang, Hsiang-Chi Kung, Chun-Eng Liu, Yu-Jen Cheng, Jien-Wei Liu, Wu Sun, Lih-Shinn Wang, Wen-Chien Ko, Kwok-Woon Yu, Ping-Cherng Chiang, Ming-Hsun Lee, Chun-Ming Lee, Gwo-Jong Hsu, and Po-Ren Hsueh.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interest. This search was supported by a fellowship grant from the International Society of Chemotherapy Infection and Cancer (ISC).
Authors’ contributions
DS draft the manuscript; DS, YTH, and PRH analyze the data; CHL and WHS collect the data; PRH complete the manuscript. All authors read and approval the final manuscript before submission.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

{kind=link}
Cite this article
Safari, D., Kuo, LC., Huang, YT. et al. Increase in the rate of azithromycin-resistant Streptococcus pneumoniae isolates carrying the erm(B) and mef(A) genes in Taiwan, 2006–2010. BMC Infect Dis 14, 704 (2014). https://doi.org/10.1186/s12879-014-0704-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-014-0704-z