
Abstract
This study investigated the moderating effect of financial strain or social support on depressive symptoms among older people living alone in Taiwan. Data were collected from the “Taiwan Longitudinal Study on Aging (TLSA),” which included 1513 participants aged 65 and over, among them, 153 (10.1%) were living alone, while 1360 (89.9%) were living with others. Measurement tools included the Depression scale (CES-D), financial stress scale, social support scale, ADL scale, IADL scale, and stress scale, with Cronbach’s α coefficients were 0.85, 0.78, 0.67, 0.91, 0.90, and 0.70 respectively. Hierarchical multiple regression was used to examine the moderator effect. The findings revealed that (1) Financial strain was found to moderate the relationship between living alone and depressive symptoms, acting as a promotive moderator among older men living alone. For older women, financial stress does not moderate the relationship between living alone and depressive symptoms. However, financial strain was also identified as a significant factor associated with depressive symptoms among older women living alone. (2) Social support does not moderate effect on the relationship between living alone and depressive symptoms in older men or older women. These results underscore the importance of considering financial stress in mental health policy development by government agencies. It is imperative to address the unique challenges faced by older individuals living alone, particularly in relation to financial strain, in order to promote their mental well-being.
Similar content being viewed by others


Introduction
In Taiwan, individuals aged 65 and above constitute nearly 20% of the older people [1]. In 2017, approximately 8.97% (288,734) of older non-institutionalized individuals lived alone, with a higher likelihood of living alone observed among older women (10.7%) compared to men (6.9%) in Taiwan [2]. A significant factor contributing to women’s tendency to live alone is their longer lifespan [3]. Moreover, older men, those without living partners, and those lacking male offspring are also more inclined to live alone in Taiwan. Older men often prefer to reside primarily with their sons, and in cases where they do not have sons, they opt for solitary living instead of cohabiting with their married daughters in Chinese culture [4,5,6].
Recent research suggests that living alone is associated with higher levels of depressive symptoms among older individuals [7,8,9]. A prevalence rate of 21% (Geriatric Depression Score of five or more) has been reported [8]. Older people living alone are particularly vulnerable to depression. However, gender emerges as a significant risk factor for depressive symptoms among older individuals living alone [10]. Specifically, older men living alone exhibit significantly more severe depressive symptoms than older women [11, 12]. Conversely, Chou et al. (2006) [4] emphasized that living alone results in higher levels of depressive symptoms for older women but not for older men. Another analysis revealed that older women living alone are more susceptible to depression than the general older population [13]. The study demonstrated that older women living alone had a higher prevalence of depressive symptoms than men (74% vs. 45%), and older women exhibited a 1.6-fold greater prevalence of depressive symptoms than men in Taiwan [10]. As suggested by Compas et al. (1993) [14], men deliberately mitigate their depressive mood by exerting a sense of control over their surrounding environment.
Moreover, older individuals who live alone are more likely to report feelings of depression. They also become physically frail due to aging, and the decline in activity and independence may influence depressive symptoms [13]. Other risk factors associated with the prevalence of depressive symptoms include a higher level of financial strain, low financial satisfaction, dissatisfaction with income, receiving less social support, gender, lower education attainment, poorer perceived health, hospitalization, more impairment in activities of daily living (ADL) or instrumental activities of daily living(IADL), and stressful life events [4, 8, 15]. The risk factors for depressive symptoms in older men living alone include educational level, self-rated health status, and social support in Taiwan [10]. Identifying certain significant factors, including social support and health indicators, can affect and explain the link between living alone and depressive symptoms among Chinese older women [4]. Additionally, the lack of social support as a risk factor also highlights the issue of women living alone in Taiwan [10].
In individuals living alone, depressive symptoms are often associated with financial strain in later life. Numerous research analyses have revealed that older people living alone, particularly those experiencing higher levels of financial strain, report more depressive symptoms [12, 16, 17]. In Taiwan, a higher percentage of older people living alone are without a job and lack income [5]. According to traditional Chinese values, older individuals may feel a sense of pride and gratitude if their adult children can provide financial support. They may even consider this financial support as an achievement in their lives, reflecting successful child-rearing [16]. As such, Chinese older people often rely heavily on financial support from their adult children or children-in-law [5, 16]. Children are identified as the primary source of financial support and assistance for issues, followed by relatives and spouses [18]. Financial strain is consistently identified as a strong predictor of deteriorating mental health among older individuals [19]. Moreover, older individuals with low incomes who live alone often experience depressive symptoms [12, 19,20,21,22], whereas those whose primary source of income is their adult children are more likely to report a lower level of depressive symptoms compared to those who are not receive such support [16].
Furthermore, the amount of social support received by older individuals who live alone is also correlated with depressive symptoms. Higher levels of social support, along with awareness of receiving such support and willingness to accept assistance, may decrease the risk of experiencing depressive symptoms [23]. In comparison to the older respondents living with others, older individuals living alone often report smaller social networks comprised of relatives, and receive less social support [4, 5, 18]. Living alone is associated with reduced levels of social support among older individuals in Taiwan [5]. Cohen & Wills (1985) [24] and Kivett et al. (2000) [25] have also concurred that family members primarily provide most social support. Children are identified as the primary source of social support and assistance for issues, followed by relatives and spouses among the aged population [18]. Lack of social support is prevalent among older individuals live alone in Taiwan [5]. At a broader level, it can be suggested that a dearth of positive social support leads to negative psychological states such as depressive symptoms [24]. Both males and females among the older population who have limited social support exhibit a significantly higher occurrence rate of depressive symptoms [10].
Living alone in later life is not inherently a strong risk factor for psychological distress [26]. Dean et al. (1992) [11] also reported that while living alone is unlikely to directly lead to depression, this arrangement does contribute independently, as well as in combination with other psychosocial problems, to increased depressive symptomatology. Conversely, Hughes & Gove suggested that living alone increases the risk of experiencing depressive symptoms, especially when accompanied by other issues such as lack of social support, which is often associated with advanced age [27]. However, social support can moderate the association between living alone and depressive symptoms among older individuals [28]. Nonetheless, when older people experience a decline in social connectivity, living alone does increase the risk of depression symptoms. In other words, the lack of adequate social relationships among older individuals who live alone can exacerbate depressive symptoms [27].
To date, there have been only a few studies examining the association between living alone and depressive symptoms among older individuals in Taiwan, especially concerning observed gender differences in the moderating roles of social support and financial strain in the link between living alone and depressive symptoms. The aim of this study is twofold: 1) To understand the impact of living alone on depressive emotions from a gender perspective and to explore the effects of financial pressure and social support on changes in depressive emotions.” and 2) To compare gender differences related to whether financial strain and social support moderate the relationship between living alone and depressive symptoms.
Methods
Subjects and database
Data for this study were obtained from respondents who were community-dwelling Chinese aged 65 years and older, selected by the Taiwan Longitudinal Study on Aging (TLSA) using a cross-sectional study method. The sampling for TLSA used Taiwan’s household registration data as the sampling frame, employing a stratified random sampling method to select probability samples. Therefore, TLSA, as a representative sample of the population, provides the best approximation of the entire middle-aged and older population in Taiwan. The sample for this study from 2011 is part of the seventh wave of the TLSA database, which includes the cohort tracked since 1989, a supplementary sample representing individuals aged 65–81 added, and a supplementary sample representing individuals aged 58–64 in 1996. A total of 3,727 individuals were successfully followed up with [29].
The TLSA sample, drawn from the household register, utilized a structured questionnaire. The household sample did not include couples or multiple individuals residing at the same address [30]. All respondents who volunteered for the study underwent face-to-face interviews. To ensure subject confidentiality, participant names were not included, an assigned code was used survey completion, editing, and data analysis. ‘Living alone’ was defined as a senior citizen residing in a household without a spouse, children, or other relatives. A total of 3,727 interviews were completed, representing a response rate of 71.5% (71.5% is equivalent to 2,663 completed questionnaires, of which 1,150 were from middle-aged people and 1,513 from older people). This included 153 older individuals living alone and 1,360 individuals who indicated they lived with family or other relatives.
Measures
Depressive symptoms
Depression Scale (CES-D) which is widely used and highly reliable in measuring depressive symptoms [31]. The short form of the CES-D includes versions such as the Iowa (11 questions), Boston (10 questions), Andresen (10 questions), and TLSA (10 questions) [32]. The items are scored on a standard 4-point scale from 0 to 3 in the Iowa format, with the scale representing the unweighted sum of the 11 component items, yielding a potential range of 0 to 33 in our measurement. Response categories include “no,” “rarely,” “sometimes,” and “often/chronically.” Employing a 1-week time frame allows for a larger sample of recent experience. Higher scores on the scale indicate more depressive symptoms. A scale (alpha = 0.85) is created by summing responses to each of the 11 questions in our study. The Iowa version of the CES-D has been validated in earlier studies. The internal consistence ranged between 0.76 and 0.81 (Cronbach’s alpha) in the samples of older people in these studies. As illustrated in the Iowa EPESE study (established populations for epidemiologic study of older people ), a score of 10 is used as a cut-off point to define the presence depressive symptoms [33].
Financial strain
The independent variable is measured using the financial strain scale developed by Wilkinson [19], consisting of two items. The first item assesses the difficulty in meeting monthly payments, with response categories ranging from 1 “not at all difficult” to 4 “completely difficult.” The second item evaluates satisfaction with one’s current financial situation, with response categories ranging from 1 “completely satisfied” to 5 “not at all satisfied”. Higher total scores indicate greater financial strain. In a previous study, not TLSA, the scale computed from these two items showed internal consistency ranging between 0.79 and 0.81 [19]. In our study, the Cronbach alpha coefficient of the scale differed from that of the individual items. Therefore, both items were standardized to T score (T score = Z score × 10 + 50), resulting in a Cronbach α coefficient value of 0.78.
Social support
The social support scale comprises three questions: (1) the extent to which respondents can discuss sensitive matters with friends, (2) their satisfaction with the amount of time spent doing so, and (3) the extent to which they can turn to a friend for help in making an important decision [34, 35]. The first two items are scored on a standard 5-point scale from 1 to 5, while the last item is scored on a 4-point scale ranging from 1 to 4. Higher total scores indicate greater social support received. The Cronbach’s alpha of this standardized T score for the social support scale in the present sample is 0.67.
Activities of Daily Living (ADL)
The ADL checklist is a composite index comprising the following conditions: bathing, dressing, eating, transferring from bed to chair, moving around the house, and using the toilet, all of which are common activities for older individuals living alone. Response categories range from 0 “not at all difficult” to 3 “completely difficult (reverse-coded).” Higher total scores indicate greater ability in activities of daily living. Exploratory factor analysis was conducted on the six items using principal components. The Kaiser-Meyer-Olkin (KMO) measure indicated that the sample was adequate for analysis (KMO = 0.88, indicating meritorious adequacy) [36]. Bartlett’s test of sphericity (χ2 (15) = 7805.54, p = .000 < .05) suggests that the correlation coefficients among all items are sufficiently large to conduct exploratory factor analysis, resulting in the extraction of only one factor (total variance = 72.24%). The internal consistency of the ADL checklist was 0.91.
Instrumental Activities of Daily Living (IADL)
IADLs are assessed using the tools developed by Lawton and Brody [37]. These items include shopping, financial management, traveling by public transportation, housework, using the phone, cooking, responsibility for own medications, and laundry. Responses to these items are ordered according to a Guttman scale, ranging from ‘‘no difficulty’’ (0) to ‘‘unable to’’ (3), with high scores indicating greater disability. After score conversion, higher total scores indicate higher ability in instrumental activities of daily living. Exploratory factor analyses were conducted on eight items using principal components. The Kaiser-Meyer-Olkin (KMO) measure indicated that the sample was adequate for analysis (KMO = 0.91, indicating marvelous adequacy) [36]. Bartlett’s test of sphericity (χ2 (28) = 7894.20, p = .000 < .05) implies that the correlation coefficients among all items are sufficiently large to conduct exploratory factor analysis, resulting in the extraction of only one factor relates to the scale (total variance = 61.29%). The Lawton and Brody instrumental activities of daily living scale show high internal consistency (Cronbach’s alpha of 0.90).
Receiving stress
Six sets of objective indicators were used to examine stressful well-being: (a) self-health, (b) self-work, (c) health of family or children, (d) work of family or children, (e) marital status of family or children, and (f) relationship with family members (e.g., tension, conflict, etc.). Four response categories were provided for each item: never (0), sometimes (1), fairly often (2), and very often (3). Higher total scores indicate higher perceived stress. Results from exploratory factor analysis indicate a Cronbach α of 0.70, a KMO measure of 0.77 indicating middling adequacy, and Bartlett’s spherical evaluation showing a significant difference (χ2 = 1527.38, df = 15, p = .000 < .05).
Other variables
The demographic data collected include gender, age, level of education, ethnicity, residence, and hospitalization. The variable ”hospitalization” is used to determine if the participant’s resided in a hospital at any time during the past year. Additionally, the participant’s self-rated health status is assessed using the following single-item interview question: “Compared with your health 1 year (or 2 years) ago, would you say that your health is better, the same, or worse now than it was then [38]?
Additionally, among age (1 = 75 and older; 0 = 65–74), education (1 = elementary school and below; 0 = otherwise), ethnic groups (1 = Minnan people; 0 = otherwise), and residential area (1 = north; 0 = otherwise) were represented using binary measures in the hierarchical multiple regression.
Statistical analysis
This study utilized data from the Taiwan Longitudinal Study on Aging for a cross-sectional secondary analysis. All analyses were performed using SPSS 25.0. Characteristics of older individuals, including depressive symptoms, financial strain, social support, activities of daily living, and stress perception, were compiled and analyzed.
Hierarchical multiple regression tests were conducted to examine the moderating effect. Participants were further categorized by gender to investigate the differing effects of financial strain and social support as moderators of the relationship between living alone and depressive symptoms in older individuals.
Multi-collinearity occurs when there is a correlation between predictors (i.e., independent variables) in a model, which can adversely affect regression results. The variance inflation factor (VIF) estimates how much the variance of a regression coefficient is inflated due to multi-collinearity in the model. Multi-collinearity refers to a situation in which two or more explanatory variables in a multiple regression model are highly linearly related. The variance inflation factor (VIF) values were calculated, and the values for all four models ranged from 1.016 to 1.258 in the men’s model and from 1.017 to 1.331 in the women’s model (all values were below 10), indicating the absence of harmful collinearity. These values indicate that accurately the contribution of predictors to the model is not difficult.
Results
Details of the characteristics of all samples can be found in Table 1. The majority of participants were male (55.3%), very old (80+) individuals (28.5%), had attained elementary school education or below (69.7%), identified as Minnan people (69.2%), and resided in southern Taiwan (35%). Most participants lived with their families (89.9%, n = 1360) while the rest lived alone (10.1%, n = 153). Respondents reported having poor (47%) or fair (48%) self-rated health status and were mostly non-hospitalized (82.9%). The final sample consisted of 836 men and 677 women. Initially, 10.1% of the older individuals chose to live alone.
A gender comparison of older individuals living alone or with others is presented in Table 2. The analysis showed no significant differences between respondents living alone and those living with others in terms of residential area, self-rated health status, hospitalization, ADL (Activities of Daily Living), IADL (Instrumental Activities of Daily Living), stress levels, and financial strain among all older individuals, both men and women. However, significant differences were observed in the percentages of respondents in various categories including gender, age, education, and ethnic groups between those living alone and those not living alone among all older individuals. Additionally, significant differences were noted in the mean scores of social support and depressive symptoms between the two groups among all older individuals. In the male sample, differences were found in terms of ethnic groups, social support, and depressive symptoms. Futhermore, statistics revealed significant differences between respondents living alone and those living with others in terms of age and depressive symptoms among female older individuals.
Older individuals resided with a family member reported a higher frequency of social support compared to those who lived alone, among all older individuals and men. As anticipated, individuals living alone reported significantly more depressive symptoms than those cohabiting with a family member, among all older individuals, both men and women. Conversely, the percentage of individuals experiencing depression (based on an Iowa EPESE score of 10 or above) was 21.1% (n = 15) among men and 34.1% (n = 28) among women, with a total of 28.1% (n = 43) of older individuals living alone in this study.
Moderating effect of financial strain and social support
Based on the recommendations of Cohen and Cohen (1983) [39], a hierarchical regression model was employed to examine the moderating effect in the relationship between living alone and depressive symptoms, as depicted in Table 3, and 4. In our initial analysis to control for the effects, the CES-D score was regressed hierarchically on age, education, ethnic groups, residential area, self-rated health status, ADL, IADL, hospitalization, and stress perception.
In this study, 9 control variables were analyzed in Model 1, and living alone additionally added to Model 2. Model 3 includes further analysis incorporating financial pressure and social support, while Model 4 incorporates two interaction terms: one for living alone and financial pressure, and another for living alone and social support, alongside the existing variables from the previous models. Additionally, the same steps were followed for older women, as shown in Table 4.
Regression results for older men
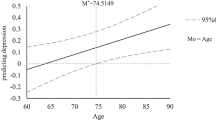
Living alone was found to have a positive and significantly influence on depressive symptoms, as indicated by the β value from Model 2 (β = 0.130, p < .001). In Model 4, the results show that both living alone (LA), financial strain and social support (SS) were significant predictors of CES-D (β = 0. 081, p < .01; β = 0. 164, p < .001; β= -0.257, p < .001), respectively. When interaction terms (LA × FS) were included, the interaction variables demonstrated a significant impact on depressive symptoms (β = 0.076, p < .05). Futhermore, the results indicated that the effect of LA on CES-D scores was more pronounced among respondents with higher levels of financial strain (FS) compared to those with lower levels of FS. It is evident that financial strain moderates the relationship between living alone and depressive symptoms for older men. To visualize this relationship, we plotted the association between living alone and depressive symptoms for high (1 SD above the mean) and low (1 SD below the mean) levels of Financial Strain [40]. And Our research findings indicate that the mean score of Financial Strain plus one standard deviation is -0.07 + 1.77 (M + 1SD), and the mean score of Financial Strain minus one standard deviation is -0.07–1.77 (M − 1SD). The graph illustrates a stronger association between living alone and depressive symptoms for older men reporting high levels of financial strain compared to those reporting low levels of financial strain. The corresponding output is presented in Fig. 1.

Interaction effect between living alone and financial strain on depressive symptoms (older men). Note. Low financial strain = M-1SD= -0.07-1.77, High financial strain = M + 1SD= -0.07 + 1.77, 95% confidence interval of financial strain = 0.31 to 0.68
When the variables of financial pressure and social support were added to Model 3, the explained variation of overall depressive emotions improved, with the adjusted R-squared reaching 0.435. The financial pressure variable showed a positive and significant effect, while the social support variable demonstrated a negative and significant effect. This indicates the meaningfulness of including financial pressure and social support variables in this model. The analysis of Model 3 indicates that when considering the impact of control variables and the influence of living alone on depressive emotions, financial stress also exerts a significant positive predictive effect on depressive emotions (β = 0.191, p < .001), while social support has a significant negative predictive effect on depressive emotions (β= -0.267, p < .001). In other words, individuals experiencing high financial pressure are associated with intense depressive emotions, whereas those with strong social support tend to experience milder depressive emotions.
In Model 4 of Table 3, after considering the effects of control variables, living alone, financial stress, and social support on depressive emotions, financial stress is found to moderate the relationship between living alone and depressive emotions, while social support does not exhibit a moderating effect. The interaction between living alone and financial stress has a significant positive predictive effect on depressive emotions (β = 0.076, p < .05), indicating that financial stress strengthens the relationship between living alone and depressive emotions. To further understand this interaction, this study follows the approach of Aiken and West [40] and divides financial stress into high and low groups based on one standard deviation above/below the mean. Generally, for older men living alone, when financial stress is higher, the impact of living alone on depressive emotions is stronger, whereas when financial stress is lower, the impact of living alone on depressive emotions is milder [41].
Regression results for older women
The analysis results for Model 6, excluding the impact of control variables on depressive emotions, show that living alone has a significant positive predictive effect on depressive emotions (β = 0.104, p < .01). After adding the variables of financial pressure and social support to Model 7, the explained variation of overall depressive emotions has improved, with an adjusted R-squared of 0.419. The financial pressure variable shows a positive and significant effect, while the social support variable demonstrates a negative and significant effect, indicating the meaningfulness of including these variables in the model. On the other hand, the analysis of Model 7 reveals that when considering the effects of control variables and the influence of living alone on depressive emotions, financial stress also exhibits a significant positive predictive effect on depressive emotions (β = 0.117, p < .01), while social support has a significant negative predictive effect on depressive emotions (β= -0.280, p < .001). Model 8 in Table 4 demonstrates that neither financial stress nor social support exhibits moderating effects.
Discussion
The sample data for this study comes from the ‘Taiwan Longitudinal Study on Aging (TLSA)’ database. This database uses household registration data as the sampling framework. Stratified random sampling was used to select probability samples, ensuring comprehensive representation of the older population in Taiwan. Additionally, the database features strict quality control in survey operations and data processing, employs a longitudinal study design with a fixed sample group, does not use replacement samples in case of participant migration, and maintains a high follow-up rate of over 80% [42]. The study found that 10.1% of older people lived alone and 28.1% exhibited symptoms of depression. These proportions closely align with the figures of 11.6% for older people living alone [2] and 27.04% for depression prevalence [43] reported in Taiwan’s official long-term tracking surveys. This demonstrates that the study sample is highly representative.
Living alone carries a more negative stigma in Chinese communities compared to Western communities [44]. The findings of this study indicate that among all older samples in the database, 10.1% of the older individuals in Taiwan were living alone. Official statistics and scholarly data indicate that the average percentage of older individuals opting for living alone in Taiwan over the past 27 years is 11.6% [2, 45]. In Japan, 15% of older individuals were living alone in 2005 [46], with rural communities showing a higher rate at 16.3% [17]. Similarly, in Myanmar, Vietnam, and Thailand, one-tenth of the older people chose to live alone [41]. Therefore, the data are relatively consistent. According to the Korea Institute for Health and Social Affairs (KIHASA) [47], 23% of Korean older adults are living alone, among whom 81.9% are female, indicating a higher proportion of Korean older females living alone compared to other living arrangements. Regarding the gender distribution of those choosing to live alone, the results of this study show that females (53.6%) outnumber males (46.4%), a trend consistent with other research findings from Taiwan [2], Japan [17], South Korea [12], Vietnam [48], the United States [3], and the United Kingdom [49]. This can be attributed to the global phenomenon of women having a longer life expectancy than men and the higher likelihood of older women being divorced, unmarried, or widowed [3, 50]. Furthermore, Chen (2021) [51] also identified three main reasons for older people living alone: (1) Women having longer life expectancies on average. (2) The aging of the baby boomer generation. (3) The declining trend of married couples, resulting in an increased proportion of divorce or widowhood significantly impacting older individuals living alone. Additionally, in countries with better economic development, individuals are more capable of affording the choice of older individuals living alone.
Returning to the topic of depressive emotions, the results of this study indicate that 28.1% of older individuals living alone experience depressive emotions. In a specific administrative district in Taipei City, 36.7% of older individuals living alone were found to have depressive emotions [52]. In Japan, 31.8% of older individuals living alone reported experiencing depressive emotions [17]. Wilson et al.‘s study (2007) [8] found that the prevalence of depressive emotions among older individuals living alone in the United Kingdom was 21%. In comparison, the results of this study demonstrate lower rates of depressive emotions across all cases, except for the United Kingdom. As older individuals experience physical decline, their children grow up and leave home, they retire, and withdraw from various roles, feelings of loneliness are more likely to arise, thus leading to the development of depressive emotions [43, 53].
Regarding depressive emotions among male and female older individuals living alone, the descriptive statistics in this study (21.1% for males and 34.1% for females) indicate that older women have a higher level of depressive emotions than older men. This finding is consistent with the research of Lin & Wang (2011) [10], where a higher percentage of depressive symptoms was found in women compared to men (74% vs. 45%) [10]. This also aligns with the findings of many researchers who emphasize that older women were more prone to depression, consistent with the results of this study [10, 13]. However, Fukunaga et al. (2012) [17] had a different finding, they found that the prevalence of depressive emotions among older individuals living alone in Japan was 34.8% for men and 31.3% for women. Lee & Hong (2016) [13] also point out that older women living alone were vulnerable to certain elements of depression, 38.1% of Korean older women and 43.7% older adults living alone have depressive symptoms [47]. Studiesand New York have also found similar results, suggesting that older men are more susceptible to depression than older women [11, 12]. Furthermore, Chou et al. [4] pointed out that male older individuals living alone and those living with others have the same level of risk for depressive emotions, while female older individuals living alone are more likely to experience depressive emotions than their counterparts living with others.
Golden et al. (2009) [54] suggested that feelings of loneliness are a leading cause of depressive emotions in older women living alone, and loneliness can increase the risk of depression [55]. On the other hand, older men living alone often enjoy solitude and are more likely to engage in satisfying social activities and connections based on their personal needs, contributing to self-growth through unhindered pursuit [56]. Therefore, older men living alone may deliberately use active participation in activities in their surroundings to shift their depressive emotions [14], and, overall, they are satisfied with their solitary lifestyles [56]. The gender differences in geriatric depression warrant further investigation.
Regardless of whether it pertains to the male older individuals, or female older individuals, living alone has a significant positive predictive effect on depressive emotions, indicating that individuals living alone are more likely to experience depressive emotions. Those living alone endure greater psychological stress and distress compared to those living with others [41]. Fukunaga et al. (2012) [17] and Wilson et al. (2007) [8] also found a significant association between living alone and depressive emotions, consistent with the results of this study. Furthermore, many researchers have suggested that older individuals living alone have a higher prevalence of depressive emotions [4, 9]. However, Iliffe et al. (1992) [49] reported different findings, indicating that individuals living alone are not necessarily at a higher risk for depression and that their life satisfaction may be higher than that of non-living alone individuals. Nevertheless, older individuals living alone may be more susceptible to feelings of isolation and a loss of self-esteem, leading to depression [8]. Among all psychological issues affecting older individuals, depression is the most closely related risk factor to suicide [57]. Therefore, the issue of older individuals living alone and their emotional and psychological well-being, particularly regarding depression, warrants further attention and research.
Tsao and Hsieh (2014) [58] argue that older adults without a stable salary income may experience increased financial or economic pressure. Ku’s study (1997) [59] also found that the poverty situation among older individuals in Taiwan is more severe compared to other age groups, and there is a high correlation between the pressure of economic scarcity and depressive symptoms [60,61,62]. This study demonstrates that regardless of whether it pertains to the male older individuals, or female older individuals, financial stress significantly predicts depressive emotions. This finding is consistent with the positive correlation between financial stress and depressive emotions as mentioned by Krause et al. (1998) [63]. Moreover, an increase in financial stress among older individuals living alone is associated with a corresponding increase in depressive emotions [17]. Numerous scholars have also corroborated that financial stress can lead to depressive emotions [12, 19,20,21,22]. However, there is a contrasting viewpoint suggesting that financially independent older individuals living alone are more likely to exhibit symptoms of depression compared to other older individuals [16].
Furthermore, the results of this study reveal that social support has a significant negative predictive effect on depressive emotions for both male and female older individuals. These findings are consistent with the research of Chi and Chou (2001) [23] and Cohen and Wills (1985) [24], who highlighted a negative correlation between social support and depressive symptoms. The absence of positive or adequate social connections can contribute to negative depressive outcomes [64], underscoring the role of social support as a preventive and protective factor against depressive emotions among the older people [23, 65]. Essentially, the social support received by older individuals living alone demonstrates limited impact on depressive emotions [63] and is less effective in alleviating depressive emotions [28].
Financial stress exerts an enhancing (positive) moderating effect on the correlation between living alone and depressive emotions among male older individuals. Studies have validated that higher levels of financial stress correspond to an increased likelihood of older individuals living alone experiencing depressive emotions [11, 17]. In South Korea, older individuals living alone with low income have reported experiencing depressive emotions and are at a higher risk of depression [12]. Similarly, in Hong Kong, there exists a positive correlation between financial stress among older individuals living alone and depressive emotions [4], with heightened financial stress elevating the probability of depression [66]. Tsao and Hsieh (2014) [58] also made similar observations, suggesting that older individuals who were initially not prone to depression exhibited significant differences in depressive tendencies under various levels of economic scarcity, with those facing financial challenges showing a higher propensity towards depressive tendencies. This indicates that both financial stress and economic scarcity have an impact on the depression of older adults, particularly when they lack stable income and must rely on depleting savings or borrowing money from family and friends to sustain their livelihoods [58], which further affects their mental well-being. In contrast, the interaction is somewhat stronger in older men and economic stress does not seem to moderate the relationship between living alone and depressive symptoms in older women. Lin & Wang (2011) [10] pointed out that in early Taiwanese society, women’s traditional roles included managing household affairs and caring for the family. The economic burden of the family was the responsibility of men, which may not increase the risk of depressive symptoms among women. Perry & Johnson (1994) [67] also noted that older women are more likely to seek assistance from family and friends to access resources, whereas older men are less likely to want to be seen as needing help. For them, economics is about courage and capital, which may explain why economic stress is an important moderating factor only among older men, but not observed as a potential cause among older women.
Furthermore, research by Dean et al. (1992) [11] has shown that when older individuals live alone and have other co-existing psychological issues, it significantly increases the risk of depressive emotions. In Taiwan, older individuals living alone typically lack income from employment [5]. While some may receive government assistance or retirement benefits, they often face the burden of rising expenses and the challenges of navigating a difficult financial environment. This firsthand experience of the social and economic hardships encountered by older individuals living alone is commonly referred to as “walking in someone else’s shoes,” and it is only when older individuals live alone and confront financial stress that they truly comprehend the difficulties involved. When older individuals living alone encounter financial stress, they may also undergo a cascade of depressive emotions, such as “loss of appetite, sleep disturbances, and mood fluctuations,” particularly as they perceive the stressors intensifying. While older individuals living alone and maintaining connections with society may not necessarily face social isolation or adaptability issues. However, concurrent research indicates that living alone does indeed increase the risk of experiencing depressive emotions, particularly when other challenges arise among older individuals. In essence, living alone does not always lead to social isolation or coping difficulties, especially when social connections are preserved. However, when older individuals encounter other problems, living alone does indeed elevate the risk of experiencing depressive emotions.
Conclusions & suggestion
With the innovation of medical technology and the prevalence of health promotion trends, the global population is aging, with variations in the pace of aging. It is expected that by the end of the 21st century, populations worldwide will have aged significantly. Modern older individuals have a diverse range of living choices, and the decision to live alone is influenced by various factors. However, at this stage, the choice of living alone is no longer associated with the negative stereotypes of the past. On the contrary, for some older individuals, living alone marks the beginning of a positive experience of renewed life. It represents autonomy and freedom from interference in daily life. It empowers individuals to make decisions about meal times, bedtime, and other aspects of life without having to accommodate the needs and restrictions of cohabitants. Living alone allows individuals to focus on themselves and provides the freedom to move at their own pace in terms of time and space. In fact, those who live alone often compensate by becoming more socially active and frequently enjoy the vibrant atmosphere of urban life, where high numbers of singletons partake in a thriving public culture.
For older individuals living alone in Taiwan, “having money” is more important than “having company.” The results of this study confirm that financial stress among older individuals living alone serves as an enhancing moderating factor for depressive emotions. It also reflects that while living alone increases the risk of depression to some extent, additional financial support can alleviate depressive symptoms in older men. Many previous studies align with the findings of this study, demonstrating the association between living alone and depressive emotions and the impact of financial stress on depressive emotions. Therefore, the financial stress experienced by older individuals living alone is strongly validated as an important moderating factor for depressive emotions. Gender differences are also one of the focuses of this study. Although in early Taiwanese society, the financial burden of the family was the responsibility of men, and women often played traditional roles in managing household chores and acting as family caregivers, whether this would lead to older women being more prone to developing depressive symptoms is also worth further investigation and exploration.
Another significant finding of this study is that the social support received by older individuals living alone may not significantly improve their depressive emotions. In other words, financial support is more critical for older individuals living alone compared to social support. As the saying goes, “Money isn’t everything, but without it, you can’t do anything,” which is aptly demonstrated in this study. It is hoped that the government will focus more on older welfare policies in the future, taking into account the financial stress and gender-related issues of older individuals living alone. These findings can be incorporated into “mental health intervention policies,” providing a deeper understanding of the nuances of financial stress in older individuals living alone and allowing for the implementation of relevant support and welfare policies for the older. It is recommended that future research delve into the themes of assessing the needs related to financial stress and gender issues among older individuals living alone. This would provide policymakers with valuable insights to formulate policies that truly benefit the older and offer practical recommendations for policy development.
Although this study strives for a comprehensive research design, it still has the following limitations. This study adopted six variables from the literature and self-developed three demographic variables as control variables, which were controlled in the study. However, apart from these, other variables that may have an impact could not be controlled, leaving some aspects not fully addressed. Therefore, the results of this study, which are specific to older individuals living alone, cannot be extrapolated to other populations of individuals living alone. Finally, the results of this study can only be inferred to the older individuals living alone in this database and cannot be extended to other groups of older individuals living alone. Living alone serves not just as an exposure factor but also as a matter of choice. Individuals experiencing more pronounced depressive symptoms might opt for solitary living or encounter challenges cohabiting with others. Given the cross-sectional nature of this study and the potential for reverse causality from depressive symptoms to living arrangements, the findings presented merely signify a statistical correlation, not causation.
Data availability
Data are not publicly available but interested parties may contact the authors for more information. The data are not publicly available due to ethical restrictions. The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Statistical Office of the Ministry of the Interior. Taiwan. Key indicators 2023. [updated 10/13/2023] Available online: https://www.moi.gov.tw/cp.aspx?n=15367.
Ministry of Health and Welfare. Taiwan. Report of the senior citizen condition survey. 2017. [updated 10/30/2022] Available online: https://dep.mohw.gov.tw/DOS/lp-5095-113.html.
Fellows of Harvard College. The challenges of living alone. Harvard Women’s Health Watch. 2012;20(3):4–5.
Chou KL, Ho AHY, Chi I. Living alone and depression in Chinese older adults. Aging Mental Health. 2006;10:583–91.
Yeh SCJ, Lo SK. Living alone, social support, and feeling lonely among the elderly. Social Behav Personality: Int J. 2004;32(2):129–38.
Li WDH. East Asian Welfare Model refocus? A case study on economic support for the elderly living alone in Taiwan. Int J Social Welf. 2013;22:260–8.
Chou KL, Chi I. Comparison between elderly Chinese living alone and those living with others. J Gerontol Soc Work. 2000;33(4):51–66.
Wilson K, Mottram P, Sixsmith A. Depressive symptoms in the very old living alone: prevalence, incidence and risk factors. Int J Geriatr Psychiatry. 2007;22(4):361–6.
You KS, Lee HO, Fitzpatrick JJ, Kim S, Marui E, Lee JS, Cook P. Spirituality, depression, living alone, and perceived health among Korean older adults in the community. Arch Psychiatr Nurs. 2009;23(4):309–22.
Lin PC, Wang HH. Factors associated with depressive symptoms among older adults living alone: an analysis of sex difference. Aging Mental Health. 2011;15(8):1038–44.
Dean A, Kolody B, Wood F, Matt GE. The influence of living alone on depression in elderly persons. J Health Aging. 1992;4(1):3–18.
Lim EJ. Gender differences in the relationship between physical functioning and depressive symptoms in low-income older adults living alone. Nurs Health Sci. 2014;16(3):381–6.
Lee S, Hong GRS. Predictors of depression among community dwelling older women living alone in Korea. Arch Psychiatr Nurs. 2016;30(5):513–20.
Compas BE, Ey S, Grant KE. Taxonomy, assessment, and diagnosis of depression during adolescence. Psychol Bull. 1993;114(2):323.
Chou KL, Chi I. Prevalence and correlates of depression in Chinese oldest-old. Int J Geriatr Psychiatry. 2005;20:41–50.
Chou KL, Chi I, Chow NWS. Sources of income and depression in elderly Hong Kong Chinese: Mediating and moderating effects of social support and financial strain. Aging Mental Health. 2004;8(3):212–21.
Fukunaga R, Abe Y, Nakagawa Y, Koyama A, Fujise N, Ikeda M. Living alone is associated with depression among the elderly in a rural community in Japan. Psychogeriatrics. 2012;12(3):179–85.
Chen Y, Hicks A, While AE. Loneliness and social support of older people living alone in a county of Shanghai. China Health Social Care Community. 2014;22(4):429–38.
Wilkinson LR. Financial strain and mental health among older adults during the great recession. Journals Gerontol Ser B: Psychol Sci Social Sci. 2016;71(4):745–54.
Burgard SA, Kalousova L. Effects of the great recession: Health and well-being. Ann Rev Sociol. 2015;41:181–201.
Catalano R, Goldman-Mellor S, Saxton K, Margerison-Zilko C, Subbaraman M, LeWinn K, Anderson E. The health effects of economic decline. Annu Rev Public Health. 2011;32:1–25.
McInerney M, Mellor JM, Nicholas LH. Recession depression: Mental health effects of the 2008 stock market crash. J Health Econ. 2013;32(6):1090–104.
Chi I, Chou KL. Social support and depression among Hong Kong Chinese older adults. Int J Aging Hum Dev. 2001;52:231–52.
Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–57.
Kivett V, Stevenson M, Zwane C. Very-old rural adults: functional status and social support. J Appl Gerontol. 2000;19:58–77.
Stone J, Evandrou M, Falkingham J. The transition to living alone and psychological distress in later life. Age Ageing. 2013;42(3):366–72.
Hughes M, Gove WR. Living alone, social integration, and mental health. Am J Sociol. 1981;87(1):48–74.
Russell D, Taylor J. Living alone and depressive symptoms: the influence of gender, physical disability, and social support among hispanic and non-hispanic older adults. J Gerontology: Social Sci. 2009;64B(1):95–104.
Health Promotion Administration. Ministry of Health and Welfare, Taiwan. Report on the Results of the 2011 Taiwan Longitudinal Study on Aging (Seventh Wave). 2014.
Health Promotion Administration, Ministry of Health and Welfare, Taiwan. Longitudinal Study on Aging (TLSA). 2015. [updated 11/08/2023] Available online: https://www.hpa.gov.tw/EngPages/Detail.aspx?nodeid=1077&pid=6197
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. https://doi.org/10.1177/014662167700100306.
Lee KL, Ou YL, Chen SH, Weng LJ. The psychometric properties of a short form of the CES-D used in the Taiwan longitudinal study on aging. Formosa J Mental Health. 2009;22(4):383–410.
Kohout FJ, Berkman LF, Evans DA. Two shorter forms of the CES-D depression symptoms index. J Aging Health. 1993;5:179–93.
Berkman LF. The assessment of social networks and social support in the elderly. J Am Geriatr Soc. 1983;31:743–9.
Lubben JE. Assessing social networks among elderly populations. Family Community Health. 1988;11:42–52.
Kaiser HF, Rice J. Little jiffy, mark IV. Educ Psychol Meas. 1974;34(1):111–7.
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3Part1):179–86.
Choi NG. Changes in self-assessment of health: comparison of self- perception and self-ratings score measures among young-old persons. J Gerontol Soc Work. 2002;37(1):65–88.
Cohen J, Cohen P. Applied multiple regression for behavioral science. NJ: Lawrence Erlbaum; 1983.
Aiken LS, West SG. Multiple regression: testing and interpreting interactions. Newbury Park, CA: Sage; 1991.
Teerawichitchainan BP, Knodel J, Pothisiri W. What does living alone really mean for older persons? A comparative study of Myanmar, Vietnam, and Thailand. Demographic Res. 2015;32(1):1329.
Health Promotion Administration, Ministry of Health and Welfare, Taiwan. Explanation of Common Issues in the Use of Elderly Survey Data. 2007. Available online: http://www.taic.mohw.gov.tw/public/dept_down/ufile/33da6165ab4953c093c910c8082ba648.pdf.
Lin CH, Chen PH, Lin HS. A panel study on factors affecting the changing status of depression among the elderly in Taiwan. J Popul Stud. 2010; (41): 67–109.
So FH. Living alone: a comparison between Hong Kong and Sweden. Hong Kong Anthropol. 2008;2:94–126.
Ministry of Health and Welfare, Taiwan. Report of the senior citizen condition survey. 2009. [updated 10/10/2023] Available online: http://sowf.moi.gov.tw/stat/week/week10011.pdf.
WHO. Global Health and Aging. 2011. [updated 10/20/2023] Available online: http://www.who.int/ageing/publications/global_health.pdf.
Korea Institute for Health and Social Affairs. National Institute of Population and Social Security Research. 2014. [updated 3/14/2024] Available online: https://www.ipss.go.jp/international/e/visitors/e140624KIHASA.html.
Guilmoto C, de Loenzien M. Emerging, transitory or residual? One-person households in VietNam. Demographic Res. 2015;32:1147–76.
Iliffe S, Tai SS, Haines A, Gallivan S, Goldenberg E, Booroff A, Morgan P. Are elderly people living alone an at risk group? BMJ. 1992;305:1001–4.
Yeung WJJ, Cheung AKL. Living alone: one-person households in Asia. Demographic Res. 2015;32:1099–112.
Chen KM. Inverting the concept of alone old age, a brief discussion on the appearance of elderly people living alone. 2021. [updated 3/14/2024] Available online: https://ccuwelfare.medium.com/%E9%80%B1%E4%B8%89%E7%A4%BE%E7%A6%8F-%E7%BF%BB%E8%BD%89-%E7%8D%A8%E8%80%81-%E7%8D%A8%E5%B1%85%E9%95%B7%E8%80%85%E6%A8%A3%E8%B2%8C%E4%B9%8B%E6%B7%BA%E8%AB%87-848eb16d41b4.
Shu SC, Chang PJ, Rong JR. Effects of learned resourcefulness on depression and quality of life among solitary elderly residents of communities. J Health Sci. 2008;10(2):88–98. https://doi.org/10.6563/TJHS.2008.10(2).2.
National Institute on Aging. Depression and Older Adults. 2024. [updated 3/14/2024] Available online: https://www.nia.nih.gov/health/mental-and-emotional-health/depression-and-older-adults.
Golden J, Conroy RM, Bruce I, Denihan A, Greene E, Kirby M, Lawlor BA. Loneliness, social support networks, mood and wellbeing in community welling elderly. Int J Geriatr Psychiatry. 2009;24:694–700.
Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol Aging. 2006;21(1):140–51.
Yetter LS. The experience of older men living alone. Geriatr Nurs. 2010;31(6):412–8.
Chou KL, Chi I, Boey KW. Determinants of depressive symptoms among elderly Chinese living alone. Clin Gerontologist. 2000;20(4):15–27.
Tsao KH, Hsieh Molly. A study of the relationships between economic stress and tendency toward Depression in Taiwan’s Elderly. Taiwan J Gerontological Health Res. 2014;10(1):44–59.
Ku YW. Research on the economic status and annuity insurance demand of the elderly in Taiwan. Ministry of Interior Social Affairs Department; 1997.
Angel RJ, Frisco M, Angel JL, Chiriboga DA. Financial strain and health among elderly mexican-origin individuals. J Health Soc Behav. 2003;44(4):536–51.
Hobfoll SE, Johnson RJ, Ennis N, Jackson AP. Resource loss, resource gain, and emotional outcomes among inner city women. J Personal Soc Psychol. 2003;84(3):632–43.
Chia HL. Factors Associated with Perceived-Health Stress and Perceived-Financial Stress in ≥ 54-Year Old Taiwanese. 2013. Master Thesis of Department Healthcare Administration of Asia University.
Krause N, Liang J, Gu S. Financial strain, received support, anticipated support, and depressive symptoms in the people’s Republic of China. Psychol Aging. 1998;13:58–68.
Utz RL, Swenson KL, Caserta M, Lund D. Feeling lonely versus being alone: loneliness and social support among recently bereaved persons. Journals Gerontol Ser B: Psychol Sci Social Sci. 2014;69(1):85–94.
Chou KL, Chi I. Stressful life events and depressive symptoms: social support and sense of control as mediators or moderators? Int J Aging Hum Dev. 2001;52:155–71.
Chi I, Chou KL. Financial strain and depressive symptoms among Hong Kong Chinese elderly: a longitudinal study. J Gerontol Soc Work. 2000;32(4):41–60.
Perry CM, Johnson CL. Families and support networks among African American oldest-old. Int Aging Hum Dev. 1994;38(1):41–50.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
T.-F. C., L.-C. P., C.-S. F., K.-L. L. and Y.-W. C. were responsible for the conceptualization and design of the study; T.-F. C., L.-C. P., C.-S. F., K.-L. L. were involved in statistical analysis. All authors contributed to the interpretation of the findings; T.-F. C. and Y.-W. C. wrote the first draft of the paper; Y.-W. C. made critical revisions. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Institutional review board statement
The research data in this study are files and documents obtained legally from government databases (Database Usage Approval Number: Ministry of Health and Welfare Statistics Approval No. 1052560573), which are either disconnected or contain non-identifiable information about specific individuals. The research does not involve ethnic or group interests. As this study involves the analysis of secondary data (publicly available government data), it falls within the scope of human research exempt from obtaining consent from the research subjects. Therefore, it is exempt from ethical review and approval. The protocol of this research was conducted in accordance with the Declaration of Helsinki and has been approved by Research Ethics Committee of National Taiwan University on August 6, 2016, under exempt status for informed consent (NTU-REC No. 201603HM009). The committee is organized under, and operates in accordance with Social and Behavior Research Ethical Principles and Regulations of National Taiwan University and governmental laws and regulations.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, TF., Pien, LC., Fan, CS. et al. Financial strain and social support as moderators of the relationship between living alone and depressive symptoms in older people. BMC Geriatr 24, 646 (2024). https://doi.org/10.1186/s12877-024-05237-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-024-05237-1