
Abstract
Background
Malnutrition is linked to a higher risk of unfavorable outcomes in various illnesses. The present investigation explored the correlation between inadequate nutritional condition and outcomes in older individuals diagnosed with hyperlipidemia.
Methods
The geriatric nutritional risk index (GNRI) was used to evaluate the nutritional status. All patients were divided into two groups according to GNRI. A Kaplan-Meier analysis was used to assess the survival rates of different groups at risk of malnutrition. In addition, GNRI was used in COX proportional risk regression models to evaluate its predictive effect on both overall mortality and cardiovascular mortality among patients with hyperlipidemia. Furthermore, the study employed restricted cubic splines (RCS) to examine the nonlinear correlation between GNRI and mortality.
Results
The study included 4,532 elderly individuals diagnosed with hyperlipidemia. During a median follow-up duration of 139 months, a total of 1498 deaths from all causes and 410 deaths from cardiovascular causes occurred. The Kaplan-Meier analysis demonstrated significantly poorer survival among individuals at risk of malnutrition, as indicated by the GNRI. In the malnutrition risk group, the modified COX proportional hazards model revealed that a decrease in GNRI was associated with a higher risk of all-cause mortality (HR=1.686, 95% CI 1.212-2.347) and cardiovascular mortality (HR=3.041, 95% CI 1.797-5.147). Furthermore, the restricted cubic splines revealed a non-linear association between GNRI and both all-cause mortality and cardiovascular mortality (p-value for non-linearity = 0.0039, p-value for non-linearity=0.0386).
Conclusions
In older patients with hyperlipidemia, lower levels of GNRI are associated with mortality. The GNRI could potentially be used to predict all-cause mortality and cardiovascular mortality.
Similar content being viewed by others

Introduction
Hyperlipidemia is characterized by abnormal levels of blood lipids or lipoproteins caused by issues in lipid metabolism or functions, such as eating disorders, obesity, inherited conditions like familial hypercholesterolemia (FH), or other diseases like diabetes [1]. The condition has been proven to be strongly associated with various cardio-metabolic disorders, including hypertension, coronary heart disease, cancer, chronic kidney disease [2,3,4] . In the United States, over 100 million adults, or approximately 53% of the population, exhibit high LDL-C levels [5]. Furthermore, approximately 31 million American adults possess total cholesterol levels surpassing 240 mg/dL, which approximately doubles the risk of ASCVD compared to individuals with cholesterol levels within the suggested range [6]. Hyperlipidemia, both in the general population and among individuals with atherosclerotic CVD, has consistently been linked to poor outcomes such as high mortality, cardiovascular events, and the onset of heart failure [7, 8]. Therefore, hyperlipidemia has emerged as a pressing health issue.
Malnutrition is also a worldwide health problem that is worsening as the global population structure changes [9, 10]. A systematic review revealed that malnutrition, as detected by nutritional assessment, is associated with longer stays in the ICU, higher rates of readmission to the ICU, elevated infection rates, and increased mortality during hospitalization [11]. Numerous studies have indicated that malnutrition is associated with the advancement of cardiovascular disorders [12,13,14,15], including inflammation, atherosclerosis, and arterial calcification [16]. A number of factors contribute to malnourishment in people with heart failure, including impaired metabolism, increased body expenditure, gastrointestinal dysfunction, and others [17]. Consequently, undernourished individuals are at a higher risk of vascular endothelial cell damage, which increases the risk of cardiovascular incidents.
In recent years, the Geriatric Nutritional Risk Index (GNRI) has gained recognition as a crucial tool for assessing the nutritional status of the elderly [18]. The GNRI is an enhanced iteration of the Nutritional Risk Index, which takes into account the weight, stature, and plasma albumin levels. It is employed to evaluate the nutritional condition of elderly individuals under pathological conditions [19]. Compared to previous nutritional assessment indicators, the GNRI provides a more objective method to evaluate the nutritional status of older adults. According to recent research, the GNRI is strongly associated with various conditions, including chronic heart failure [20], hypertension [21], diabetes [22], chronic kidney failure [23], and cirrhosis [24]. Our study aimed to investigate the association between GNRI and overall mortality and cardiovascular mortality in individuals with hyperlipidemia.
Methods
Study design and study population
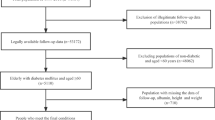
Information was obtained from ten consecutive cycles of the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018. The NHANES dataset was created and maintained by the National Center for Health Statistics of the Centers for Disease Control and Prevention [25], utilizing hierarchical, multilevel, and probabilistic clustering methods. To carry out physical examinations and gather blood samples, a mobile examination center (MEC) was utilized. The data included demographic information, dietary surveys, laboratory analyses, and assessments, which were carried out by qualified personnel [26]. In this study, 14,309 hyperlipidemia patients over 60 years old with eligible follow-up data were included. Afterward, participants with incomplete data such as albumin, height, weight, covariates, fasting subsample weight, and follow-up time exceeding 168 months were removed, leading to a total sample size of 4,532. The comprehensive details regarding the sampling procedure and criteria for exclusion are displayed in Fig. 1. All participants provided written informed consent to participate in the NHANES research, which was approved by the NCHS Research Ethics Review Committee (Clinical Trial Number ID: NCT00005154).

Flow chart of study population
Covariates
Clinical experience and previous literature were the cornerstone of the selection of covariates [27]. Demographic features, physical examination, and laboratory tests were considered as covariates in this study. Socio-demographic characteristics and medical history were evaluated using standard surveys. The demographic attributes comprised age, sex, educational background, race/ethnicity (Mexican American, non-Hispanic White, non-Hispanic Black, or other race), level of physical activity, smoking habits, usage of antihyperlipidemic medications, and alcohol consumption habits. Height (cm), weight (kg), and blood pressure (mmHg) were measured at the mobile examination centers (MECs). Participants were required to fast for a minimum of 8.5 hours, but no more than 24 hours, before blood sample collection. The blood tests included neutrophils, lymphocytes, serum creatinine, uric acid, and glycated hemoglobin (HbA1c). Individuals who claimed to have smoked less than 100 cigarettes throughout their entire life were categorized as individuals who have never smoked. Those who have smoked more than 100 cigarettes in their lifetime but stopped were considered former smokers. Individuals who have smoked over 100 cigarettes during their lifetime and have smoked on certain days or daily were categorized as present smokers. The drinking status was divided into different categories: non-drinker (consumed less than 12 drinks in their lifetime), former drinker (consumed 12 or more drinks in one year but did not drink last year, or did not drink last year but consumed 12 or more drinks in their lifetime), mild drinker (females who consume at least 1 drink per day, males who consume at least 2 drinks per day), moderate drinker (females who consume at least 2 drinks per day, males who consume at least 3 drinks per day or engage in binge drinking at least 2 days per month), or heavy drinker (females who consume at least 3 drinks per day, males who consume at least 4 drinks per day or engage in binge drinking [at least 4 drinks on the same occasion for females, at least 5 drinks on the same occasion for males] on 5 or more days per month) [28]. Furthermore, the physical activity levels were evaluated based on the suggested amount of moderate to vigorous activity per week, including (1) insufficient, meaning fewer than 150 minutes per week; (2) adequate, meaning 150 to 300 minutes per week; and (3) exceeds, meaning more than 300 minutes per week [29]. CVD status was determined by asking the individuals whether a physician or other healthcare professional ever diagnosed them with congestive heart failure, coronary heart disease, angina pectoris, heart attack, or stroke). The Glomerular filtration rate (eGFR) was determined based on the KDIGO 2021 Clinical Practice Guideline for Glomerular Diseases management [30]. Chronic kidney disease (CKD) was characterized by irregularities in the structure or functioning of the kidneys, persisting for a duration exceeding three months and having consequences for one's well-being. Chronic kidney disease (CKD) was defined by a calculated eGFR below 60 ml/min/ 1.73 m2 [30]. Diabetes mellitus was recorded based on any of the following criteria: receiving a diagnosis of diabetes from a physician and utilizing diabetes medication or insulin.
Diagnosis of hyperlipidemia
Hyperlipidemia was defined by elevated triglyceride (TG) levels of 150 mg/dl (1.7 mmol/L) or higher, or total cholesterol (TC) levels of 200 mg/dl (5.18 mmol/L) or higher, along with increased low-density lipoprotein (LDL) levels of 130 mg/dl (3.37 mmol/L) or higher, or high-density lipoprotein (HDL) below 40 mg/dl (1.04 mmol/L) in men and under 50 mg/dl (1.30 mmol/L) in women [31]. Moreover, individuals who admitted to taking cholesterol-lowering drugs were considered hyperlipidemic.
Assessment of nutritional status
The GNRI is a widely utilized and dependable tool to assess malnutrition in different clinical settings. The GNRI was developed to evaluate the nutritional risk of every participant and was computed using the formula GNRI = [1.489×serum albumin (g/L)] + [41.7×(actual weight (kg) / ideal weight (kg)]. The Lorenze equation (WLo) was used to calculate the optimal weight, which was H-100-[(H-150)/4] for males, and H-100-[(H-150)/2.5] for females. When the patient's weight exceeded the ideal weight, the ratio of weight to ideal weight was adjusted to 1 [32]. The participants enrolled in this research were categorized into two cohorts: the no-risk cohort (GNRI ≥ 98) and the risk cohort (GNRI < 98).
Ascertainment of mortality
In the follow-up study, participant survival status was determined using the publicly available mortality files from the survey date to December 31, 2018. This involved connecting the National Center for Health Statistics (NCHS) with the National Death Index (NDI) using a probability matching algorithm [33]. Death from any cause was used to define overall mortality. To determine deaths related to cardiovascular diseases, the I00–I09, I11, I13, and I20–I51 codes of the International Statistical Classification of Diseases, 10th Revision (ICD-10) were used [34].
Statistical analysis
Based on the NHANES analytical guidelines, the calculations were adjusted for the uneven selection probabilities, the oversampling of certain subgroups, and nonresponse in the analyses with sampling weights, strata, and primary sampling units [33]. The following formula was used to calculate sampling weights. The fasting subsample 10-year weight was determined by multiplying the fasting subsample 4-year weight by 2/10 for the period of 1999-2002, and the fasting subsample 2-year weight by 1/10 for the period of 2003-2018. All analyses were conducted using the statistical software package R (version 4.3.1). Data extraction and analysis were performed using the 'nhanesR' package. The initial patient characteristics were evaluated by dividing the sample into two categories according to the GNRI thresholds, namely the no-risk cohort and the risk cohort. Weighted t-tests were carried out to compare the means and proportions of the baseline characteristics. Continuous variables were expressed as weighted mean (standard error). In addition, Rao-Scott's χ2 test was used to compare categorical variables, which were presented as weighted frequencies and percentages. The reference group (GNRI > 98) was categorized as normal. Both crude and adjusted models were used for these analyses. Model 1 was constructed after adjusting for BMI, age, Neu, Lyn, UA, Scr, and HbA1c. In Model 2, ethnicity, gender, levels of education, smoking habits, and physical exercise were adjusted in addition to the covariates from Model 1. Moreover, alcohol intake, medications for high cholesterol, CVD, CKD, DM, and the covariates from Model 2 were adjusted in Model 3. The Cox proportional hazard regression model and 95% confidence interval (CI) were employed to examine the association between GNRI and the occurrence of cardiovascular and all-cause mortality. Malnutrition-risk groups were analyzed using Kaplan-Meier survival analysis. After adjusting for multiple variables, a cox restricted cubic spline regression model was used to evaluate the nonlinear link between GNRI and all-cause mortality and cardiovascular mortality. Additionally, a further analysis was carried out based on subgroups including age, gender, education levels, smoking status, ethnicity, physical activity, alcohol consumption, CVD, DM, and CKD. In all of these analyses, statistically significant differences were characterized by a two-tailed p-value less than 0.05.
Results
Participant characteristics according to malnutrition risk
This study included 4,532 elderly with hyperlipidemia. In our sample, approximately 33,594,599 older Americans with hyperlipidemia were represented by the weight calculations. Out of the total 4,532 participants, 2,200 were males and 2,312 were females. The median duration of follow-up was 139 months. Based on GNRI levels, the baseline characteristics was displayed in Table 1. The majority of the participants were identified as non-Hispanic white. Furthermore, in terms of statistical significance, differences were observed in age, BMI, serum uric acid, gender, smoking, and physical activity between the two groups classified by GNRI (P<0.05). Older individuals, particularly females and those with lower body mass index (BMI), reduced uric acid levels, current smokers, inactive lifestyle, cardiovascular disease, and chronic kidney disease patients, were exposed to a higher risk of malnutrition. However, no differences in the risk of malnutrition were found with respect to ethnicity, level of education, alcohol consumption, use of antihyperlipidemic drugs, neutrophil count, lymphocyte count, serum creatinine, glycated hemoglobin, and diabetes. The following table summarizes the fundamental characteristics of the participants.
Association between GNRI and all-cause mortality and cardiovascular mortality
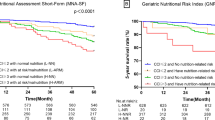
During the follow-up period, 1498 (33.1%) patients passed away. Based on the basic, all-multivariate model (Table 2), the risk group exhibited a higher mortality rate than the no-risk group. According to the COX proportional hazard regression model, a positive correlation was observed between GNRI and the risk of all-cause mortality and cardiovascular mortality. The basic model did not include any variables that needed to be adjusted. As well as mortality risk, a higher GNRI had a marginally reduced impact on cardiovascular disease and mortality from any cause (HR= 0.984, 95% CI 0.973, 0.995 and HR= 0.981, 95% CI 0.975, 0.988), respectively. Similar results were observed in adjusted Models 1, 2, and 3. In model 3, after making all necessary adjustments, every increment in GNRI was linked to a 3% decline in the risk of overall mortality (HR=0.971, 95% CI 0.958, 0.985) and a 5% drop in cardiovascular mortality (HR=0.951, 95% CI 0.929, 0.974). When GNRI was employed as a categorical factor, the unadjusted model demonstrated an association between the risk of malnutrition and the risk of mortality from any cause, and cardiovascular mortality (HR= 2.500, 95% CI 1.810, 3.452 and HR = 2.771, 95% CI 1.360, 5.646), respectively. After adjusting for the entire model (Table 2), the multifactorial COX regression analysis revealed that GNRI was also significantly linked to the risk of all-cause mortality and cardiovascular mortality, with hazard ratios of 1.686 (95% CI 1.212-2.347) and 3.041 (95% CI 1.797-5.147) respectively. The Kaplan-Meyer survival rates for overall mortality and cardiovascular death exhibited a obvious difference between the risk and no-risk groups (p < 0.05) (Fig. 2A and B).

Kaplan–Meier survival rates for mortality among different GNRI groups with older hyperlipidemia. A all-cause mortality; B cardiovascular mortality
Subgroup analyses
In subgroup analyses (Table 3), the correlation between GNRI and all-cause mortality, as well as cardiovascular mortality, was explored. The results indicated that GNRI interacted with gender, education level, and physical activity in terms of overall mortality. There were interactions between the GNRI and education level, alcohol intake, and cardiovascular disease with respect to cardiovascular disease mortality. Furthermore, GNRI showed no correlation with overall mortality and cardiovascular mortality among elderly hyperlipidemia populations of other race and with a university degree (P > 0.05).
Non-linear relationship between GNRI and mortality from all causes and cardiovascular diseases.
In a fully adjusted restricted cubic spline regression model (RCS) that accounted for confounding factors, higher GNRI in elderly individuals with hyperlipidemia was linked to a decreased likelihood of mortality from any cause and cardiovascular mortality. However, both outcomes exhibited non-linear patterns (p = 0.0039 for non-linearity and p = 0.0386 for non-linearity, respectively), as shown in Fig. 3.

Restricted cubic splines of GNRI and mortality in older adults with hyperlipidemia. A All-cause mortality. B Cardiovascular mortality. Adjusted for BMI, age, NEU, Lyn, UA, Scr, HbA1c, ethnicity, gender, education level, smoking, physical activity, CKD, CVD, DM, alcohol intake, ATHP)
Discussion
In this retrospective cohort study, we conducted a nutritional assessment of 4,532 older adults with hyperlipidemia using the GNRI. In hyperlipidemia patients with varying nutritional risks, overall mortality and cardiovascular mortality were analyzed using Kaplan-Meier simulation. Moreover, the COX proportional hazard regression models revealed that GNRI could potentially act as a novel marker for both overall and cardiovascular mortality among elderly individuals with hyperlipidemia. Furthermore, according to the restricted cubic spline regression models, a significant association was found between GNRI and cardiovascular mortality and overall mortality. Moreover, subgroup analyses demonstrated that GNRI was linked to mortality risk in various subgroups of elderly individuals with hyperlipidemia, indicating that malnutrition may be a modifiable risk factor.
Nutritional status plays an essential role in predicting the mortality of various diseases [35, 36]. Long-lasting, enduring illnesses such as diabetes can result in malnourishment, exacerbate the advancement of the disease, and affect patient prognosis [37]. Malnutrition, resulting from insufficient, excessive, or unbalanced intake of energy or nutrients, is linked to physical and cognitive decline, diminished quality of life, increased illness, and higher mortality in older adults [38, 39]. Additionally, a growing number of studies suggest that undernourishment may cause oxidative stress, impaired insulin release [40], breakdown of fats, and oxidation of lipids [41], negatively impacting tissues, diabetes, and fatty liver [42]. Albumin and BMI are fundamental components of the GNRI [32]; low levels of albumin and underweight are indicative of malnutrition. Research has shown that both immediate and long-term inflammation play a role in reducing albumin levels, and a low body mass index (BMI) could be a significant sign of malnourishment. This is consistent with our results. Additionally, a decrease in albumin levels and a decrease in BMI could indicate a reduction in both muscle and adipose tissue [43, 44]. Initially developed to assess the likelihood of complications associated with malnutrition in elderly individuals, the GNRI has been proven to be a valuable measure for various medical conditions. Recent studies have demonstrated the GNRI has significant implications for the nutritional condition and forecasting of individuals with ischemic cardiac failure, chronic renal disease, hemodialysis, and diabetes [22, 45,46,47]. The GNRI can be calculated without any particular requirement such as patient participation or nutrition specialist guidance, highlighting its practical value. Currently, research on the association between GNRI and mortality in people with hyperlipidemia is lacking. However, our study demonstrated that GNRI could potentially be a valuable predictive marker for elderly individuals diagnosed with hyperlipidemia.
Hyperlipidemia, a prevalent metabolic condition, poses a risk for cardiovascular conditions. An increased risk for cardiovascular disease or the presence of non-alcoholic steatohepatitis is indicated by moderately raised levels of plasma or serum triglycerides (2-10 mmol/L). Moreover, triglyceride levels that are considerably higher than 10 mmol/L suggest a greater likelihood of developing pancreatitis and lipemia retinalis [48, 49]. Elevated levels of cholesterol in the blood are linked to heightened oxidative stress, neurotoxicity, and Alzheimer's disease [50, 51]. In addition, hyperlipidemia has been shown to increase the likelihood of non-ischemic heart failure, while lowering serum lipid levels can reverse cardiac dysfunction. Furthermore, hyperlipidemia not only indirectly impacts cardiac function by facilitating the growth of atherosclerosis but also directly influences cardiac systolic function and cardiac electrophysiological reactions [52, 53]. These effects could be attributed to the gradual buildup of cardiac lipids, leading to systemic oxidative stress, a pro-inflammatory condition, and mitochondrial dysfunction [54]. Meanwhile, serum uric acid (SUA) could serve as a significant antioxidant compound, constituting half of the body's overall antioxidant capacity [55]. Research has shown that decreased SUA levels has been linked to a decline in the ability to eliminate free radicals, potentially resulting in increased vascular endothelial cell damage, and ultimately raising the risk of cardiovascular-related death [56]. Moreover, a recent investigation revealed that inadequate nutrition significantly increases the risk of cardiovascular disease-related death in elderly individuals with reduced uric acid levels [27]. Consistently, studies have discovered a correlation between low levels of uric acid in the blood and a low body mass index (BMI) below 18.5 kg/m2, as well as increased rates of weight reduction [57]. Several studies have suggested a U-shaped correlation between BMI and mortality, as indicated by previous research [58, 59]. However, a high BMI does not necessarily imply sufficient nourishment [60]. On the other hand, the buildup of fat and being overweight can indirectly lead to further nutritional imbalances as a result of changes in metabolism and overall body composition. Moreover, obesity may promote the emergence of both short-term and long-term illnesses that negatively affect nutritional well-being [61]. Likewise, our ongoing investigation revealed that people with a low body mass index (BMI) faced an increased risk of reduced uric acid levels in their blood, suggesting a potential sign of inadequate nutrition.
This observational study suggested the challenge behind precisely elucidating the relationship between malnutrition and cardiovascular and overall mortality in hyperlipidemia patients. Still, the following mechanisms may be involved. Malnutrition associated with diseases can stimulate the sympathetic nervous system, immune system, and hypothalamic-pituitary-adrenal axis [62]. This involves the secretion of pro-inflammatory proteins like IL-6, IL-1, and TNF-α, leading to reduced appetite, muscle degradation, and insulin insensitivity [63]. In addition, malnutrition can be accompanied by specific deficiencies in micronutrients, such as vitamin D. Vitamin D supplementation has been shown to modulate adipose tissue function. According to Farhangi MA's research, vitamin D consumption increases the activity of antioxidant enzymes SOD and GSH-Px in adipose tissue, hence decreasing the TNF-α levels and improving oxidative stress and inflammatory factors in the adipose tissue of obese rats [64]. In addition, an extended elevation in circulating fatty acids and triglycerides and the buildup of pericardial adipose tissue may initiate inflammatory signaling in the heart. This results in cardiac impairment in metabolic disorders, characterized by mitochondrial dysfunction and heightened ROS and NFB activity [65]. Consequently, individuals suffering from hyperlipidemia are at an increased risk of complications, leading to a greater mortality and morbidity rate.
Nevertheless, the limitations of the study should be acknowledged. Uncovering the precise mechanisms underlying the influence of malnutrition on overall mortality and cardiovascular mortality was challenging. Furthermore, since the NHANES study gathered information at a single time point, essential nutritional details were only documented once for every participant, overlooking their fluctuations over time. This could potentially introduce some bias in GNRI. Therefore, longitudinal clinical trials involving multiple centers should be conducted to confirm our discoveries and conduct extended monitoring to explore the precise influence of nutrition levels on the advancement and growth of hyperlipidemia in elderly individuals.
Conclusions
Through a nationwide cross-sectional study, this research revealed a notable correlation between diminished GNRI levels and the occurrence of hyperlipidemia among elderly individuals. This study examined a representative sample of an entire nation, indicating that low GNRI levels were associated with the occurrence of hyperlipidemia in elderly individuals. GNRI can also serve as an indicator for predicting the risk of hyperlipidemia in older adults.
Availability of data and materials
The datasets analyzed during the current study were publicly available from the NAHNES online website:https://www.cdc.gov/nchs/nhanes/index.htm.
Abbreviations
- GNRI:
-
Geriatric nutrition risk index
- ASCVD:
-
Arteriosclerotic cardiovascular disease
- CVD:
-
Cardiovascular disease
- CKD:
-
Chronic kidney disease
- ICU:
-
Intensive care unit
- MEC:
-
Mobile examination center
- NCHS:
-
National Center for Health Statistics
- eGFR:
-
Glomerular filtration rate
- NDI:
-
National Death Index
- CI:
-
Confidence interval
- BMI:
-
Body mass index
- Lyn:
-
Lymphocyte coun
- Neu:
-
Neutrophil count
- Scr:
-
Serum creatinine
- UA:
-
Uric acid
- ATHP:
-
Antihyperlipidemic agents
- HbA1c:
-
Glycated hemoglobin
- RCS:
-
Restricted cubic spline
- FH:
-
Familial hypercholesterolemia
- χ2:
-
Chi-square
- DM:
-
Diabetes mellitus
References
Sudhakaran S, Bottiglieri T, Tecson KM, Kluger AY, McCullough PA. Alteration of lipid metabolism in chronic kidney disease, the role of novel antihyperlipidemic agents, and future directions. Rev Cardiovasc Med. 2018;19(3):77–88.
Su X, Peng D. New insight into sortilin in controlling lipid metabolism and the risk of atherogenesis. Biol Rev Camb Philos Soc. 2020;95(1):232–43.
Siddiqui AA. Metabolic syndrome and its association with colorectal cancer: a review. Am J Med Sci. 2011;341(3):227–31.
Ruan XZ, Varghese Z, Moorhead JF. An update on the lipid nephrotoxicity hypothesis. Nat Rev Nephrol. 2009;5(12):713–21.
Centers for Disease C, Prevention. Vital signs: prevalence, treatment, and control of high levels of low-density lipoprotein cholesterol–United States, 1999–2002 and 2005–200. MMWR Morb Mortal Wkly Rep. 2011;60(4):109–14.
Writing Group M, Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, et al. Heart Disease and Stroke Statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38–360.
Pekkanen J, Linn S, Heiss G, Suchindran CM, Leon A, Rifkind BM, et al. Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N Engl J Med. 1990;322(24):1700–7.
Zhou H, Ding X, Yang Q, Chen S, Li Y, Zhou X, et al. Associations of hypertriglyceridemia onset age with cardiovascular disease and all-cause mortality in adults: a cohort study. J Am Heart Assoc. 2022;11(20):e026632.
Yu Z, Kong D, Peng J, Wang Z, Chen Y. Association of malnutrition with all-cause mortality in the elderly population: a 6-year cohort study. Nutr Metab Cardiovasc Dis. 2021;31(1):52–9.
Mostafa N, Sayed A, Rashad O, Baqal O. Malnutrition-related mortality trends in older adults in the United States from 1999 to 2020. BMC Med. 2023;21(1):421.
Lew CCH, Yandell R, Fraser RJL, Chua AP, Chong MFF, Miller M. Association between malnutrition and clinical outcomes in the intensive care unit: a systematic review [formula: see text]. JPEN J Parenter Enteral Nutr. 2017;41(5):744–58.
Lapenna D, Ciofani G, Ucchino S, Pierdomenico SD, Cuccurullo C, Giamberardino MA, et al. Serum albumin and biomolecular oxidative damage of human atherosclerotic plaques. Clin Biochem. 2010;43(18):1458–60.
Matsuzaki K, Fukushima N, Saito Y, Matsumoto N, Nagaoka M, Katsuda Y, et al. The effects of long-term nutrition counseling according to the behavioral modification stages in patients with cardiovascular disease. Nutrients. 2021;13(2):414.
Fukumoto Y. Nutrition and cardiovascular diseases. Nutrients. 2021;14(1):94.
Sze S, Pellicori P, Zhang J, Clark AL. Malnutrition, congestion and mortality in ambulatory patients with heart failure. Heart. 2019;105(4):297–306.
Nakagomi A, Kohashi K, Morisawa T, Kosugi M, Endoh I, Kusama Y, et al. Nutritional status is associated with inflammation and predicts a poor outcome in patients with chronic heart failure. J Atheroscler Thromb. 2016;23(6):713–27.
Minamisawa M, Seidelmann SB, Claggett B, Hegde SM, Shah AM, Desai AS, et al. Impact of malnutrition using geriatric nutritional risk index in heart failure with preserved ejection fraction. JACC Heart Fail. 2019;7(8):664–75.
Cereda E, Pedrolli C. The geriatric nutritional risk index. Curr Opin Clin Nutr Metab Care. 2009;12(1):1–7.
Takahashi H, Ito Y, Ishii H, Aoyama T, Kamoi D, Kasuga H, et al. Geriatric nutritional risk index accurately predicts cardiovascular mortality in incident hemodialysis patients. J Cardiol. 2014;64(1):32–6.
Nishi I, Seo Y, Hamada-Harimura Y, Yamamoto M, Ishizu T, Sugano A, et al. Geriatric nutritional risk index predicts all-cause deaths in heart failure with preserved ejection fraction. ESC Heart Fail. 2019;6(2):396–405.
Cao Z, Dai S, Liu X. The geriatric nutritional risk index mediated the relationship between serum uric acid and hypertension: a mediation analysis. BMC Geriatr. 2021;21(1):527.
Shen X, Yang L, Gu X, Liu YY, Jiang L. Geriatric Nutrition Risk Index as a predictor of cardiovascular and all-cause mortality in older Americans with diabetes. Diabetol Metab Syndr. 2023;15(1):89.
Maenosono R, Fukushima T, Kobayashi D, Matsunaga T, Yano Y, Taniguchi S, et al. Unplanned hemodialysis initiation and low geriatric nutritional risk index scores are associated with end-stage renal disease outcomes. Sci Rep. 2022;12(1):11101.
Saeki C, Kinoshita A, Kanai T, Ueda K, Nakano M, Oikawa T, et al. The Geriatric Nutritional Risk Index predicts sarcopenia in patients with cirrhosis. Sci Rep. 2023;13(1):3888.
Zipf G, Chiappa M, Porter KS, Ostchega Y, Lewis BG, Dostal J. National health and nutrition examination survey: plan and operations, 1999–2010. Vital Health Stat 1. 2013;56:1–37.
Morris AA, Ko YA, Hutcheson SH, Quyyumi A. Race/ethnic and sex differences in the association of atherosclerotic cardiovascular disease risk and healthy lifestyle behaviors. J Am Heart Assoc. 2018;7(10):e008250.
Tseng WC, Chen YT, Ou SM, Shih CJ, Tarng DC, Taiwan Geriatric Kidney Disease Research G. U-shaped association between serum uric acid levels with cardiovascular and all-cause mortality in the elderly: the role of malnourishment. J Am Heart Assoc. 2018;7(4):e007523.
Rattan P, Penrice DD, Ahn JC, Ferrer A, Patnaik M, Shah VH, et al. Inverse association of telomere length with liver disease and mortality in the US population. Hepatol Commun. 2022;6(2):399–410.
Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–8.
Kidney Disease: Improving Global Outcomes Glomerular Diseases Work G. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021;100(4S):S1–276.
National Cholesterol Education Program Expert Panel on Detection E, Treatment of High Blood Cholesterol in A. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143–421.
Bouillanne O, Morineau G, Dupont C, Coulombel I, Vincent JP, Nicolis I, et al. Geriatric Nutritional Risk Index: a new index for evaluating at-risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777–83.
Bao W, Liu B, Simonsen DW, Lehmler H-J. Association Between Exposure to Pyrethroid Insecticides and Risk of All-Cause and Cause-Specific Mortality in the General US Adult Population. JAMA Intern Med. 2020;180(3):367–74.
Bramer GR. International statistical classification of diseases and related health problems Tenth revision. World Health Stat Q. 1988;41(1):32–6.
Huang W, Xiao Y, Wang H, Li K. Association of geriatric nutritional risk index with the risk of osteoporosis in the elderly population in the NHANES. Front Endocrinol (Lausanne). 2022;13:965487.
Lee M, Lim JS, Kim Y, Lee JH, Kim CH, Lee SH, et al. Association between Geriatric Nutritional Risk Index and Post-Stroke Cognitive Outcomes. Nutrients. 2021;13(6):1776.
Saintrain MVL, Sandrin R, Bezerra CB, Lima AOP, Nobre MA, Braga DRA. Nutritional assessment of older adults with diabetes mellitus. Diabetes Res Clin Pract. 2019;155:107819.
Jayanama K, Theou O, Blodgett JM, Cahill L, Rockwood K. Frailty, nutrition-related parameters, and mortality across the adult age spectrum. BMC Med. 2018;16(1):188.
Wei K, Nyunt MS, Gao Q, Wee SL, Yap KB, Ng TP. Association of frailty and malnutrition with long-term functional and mortality outcomes among community-dwelling older adults: results from the Singapore longitudinal aging study 1. JAMA Netw Open. 2018;1(3):e180650.
Bandsma RH, Ackerley C, Koulajian K, Zhang L, van Zutphen T, van Dijk TH, et al. A low-protein diet combined with low-dose endotoxin leads to changes in glucose homeostasis in weanling rats. Am J Physiol Endocrinol Metab. 2015;309(5):E466–73.
Badaloo AV, Forrester T, Reid M, Jahoor F. Lipid kinetic differences between children with kwashiorkor and those with marasmus. Am J Clin Nutr. 2006;83(6):1283–8.
Thompson DS, Bourdon C, Massara P, Boyne MS, Forrester TE, Gonzales GB, et al. Childhood severe acute malnutrition is associated with metabolic changes in adulthood. JCI Insight. 2020;5(24):e141316.
Kovesdy CP, Kalantar-Zadeh K. Why is protein-energy wasting associated with mortality in chronic kidney disease? Semin Nephrol. 2009;29(1):3–14.
Cederholm T, Jensen GL, Correia M, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM criteria for the diagnosis of malnutrition - a consensus report from the global clinical nutrition community. Clin Nutr. 2019;38(1):1–9.
Xiong J, Wang M, Wang J, Yang K, Shi Y, Zhang J, et al. Geriatric nutrition risk index is associated with renal progression, cardiovascular events and all-cause mortality in chronic kidney disease. J Nephrol. 2020;33(4):783–93.
Sun T, Ma M, Huang X, Zhang B, Chen Z, Zhao Z, et al. Prognostic impacts of geriatric nutritional risk index in patients with ischemic heart failure after percutaneous coronary intervention. Clin Nutr. 2023;42(8):1260–7.
Jung YS, You G, Shin HS, Rim H. Relationship between Geriatric Nutritional Risk Index and total lymphocyte count and mortality of hemodialysis patients. Hemodial Int. 2014;18(1):104–12.
Pitha J, Kovar J, Blahova T. Fasting and nonfasting triglycerides in cardiovascular and other diseases. Physiol Res. 2015;64(Suppl 3):S323–30.
Sahebkar A, Watts GF. Challenges in the treatment of hypertriglyceridemia: glass half empty or half full? Expert Rev Clin Pharmacol. 2015;8(4):363–6.
El-Sayyad HI. Cholesterol overload impairing cerebellar function: the promise of natural products. Nutrition. 2015;31(5):621–30.
Xue-Shan Z, Juan P, Qi W, Zhong R, Li-Hong P, Zhi-Han T, et al. Imbalanced cholesterol metabolism in Alzheimer’s disease. Clin Chim Acta. 2016;456:107–14.
Pathak RK, Mahajan R, Lau DH, Sanders P. The implications of obesity for cardiac arrhythmia mechanisms and management. Can J Cardiol. 2015;31(2):203–10.
Balakumar P, Babbar L. Preconditioning the hyperlipidemic myocardium: fact or fantasy? Cell Signal. 2012;24(3):589–95.
Yao YS, Li TD, Zeng ZH. Mechanisms underlying direct actions of hyperlipidemia on myocardium: an updated review. Lipids Health Dis. 2020;19(1):23.
Ndrepepa G. Uric acid and cardiovascular disease. Clin Chim Acta. 2018;484:150–63.
Zheng Y, Ou J, Huang D, Zhou Z, Dong X, Chen J, et al. The U-shaped relationship between serum uric acid and long-term all-cause mortality in coronary artery disease patients: a cohort study of 33,034 patients. Front Cardiovasc Med. 2022;9:858889.
Baker JF, Weber DR, Neogi T, George MD, Long J, Helget LN, et al. Associations between low serum urate, body composition, and mortality. Arthritis Rheumatol. 2023;75(1):133–40.
Xu W, Shubina M, Goldberg SI, Turchin A. Body mass index and all-cause mortality in patients with hypertension. Obesity (Silver Spring). 2015;23(8):1712–20.
Jayedi A, Shab-Bidar S. Nonlinear dose-response association between body mass index and risk of all-cause and cardiovascular mortality in patients with hypertension: a meta-analysis. Obes Res Clin Pract. 2018;12(1):16–28.
Wells JC, Sawaya AL, Wibaek R, Mwangome M, Poullas MS, Yajnik CS, et al. The double burden of malnutrition: aetiological pathways and consequences for health. Lancet. 2020;395(10217):75–88.
Barazzoni R, Gortan Cappellari G. Double burden of malnutrition in persons with obesity. Rev Endocr Metab Disord. 2020;21(3):307–13.
Preiser JC, Ichai C, Orban JC, Groeneveld AB. Metabolic response to the stress of critical illness. Br J Anaesth. 2014;113(6):945–54.
Stumpf F, Keller B, Gressies C, Schuetz P. Inflammation and Nutrition: Friend or Foe? Nutrients. 2023;15(5):1159.
Farhangi MA, Mesgari-Abbasi M, Hajiluian G, Nameni G, Shahabi P. Adipose tissue inflammation and oxidative stress: the ameliorative effects of vitamin D. Inflammation. 2017;40(5):1688–97.
Dirkx E, Schwenk RW, Glatz JF, Luiken JJ, van Eys GJ. High fat diet induced diabetic cardiomyopathy. Prostaglandins Leukot Essent Fatty Acids. 2011;85(5):219–25.
Acknowledgements
We thank Home for Researchers editorial team (www.home-for-researchers.com) for language editing service.
Funding
The General Program of Natural Science Foundation of Fujian Province (Grant Number 2023J011179) provided support for this study.
Author information
Authors and Affiliations
Contributions
Kun Cheng and Jing Zhang contributed to this study equally. The manuscript's conception, design, data analysis, and writing were contributed by Kun Cheng, Jing Zhang, and Xiao-Fen Zhou. Xiao-Yan Ding, Xiao-E Zheng, Mou-Hui Lin, and Lu-Ya Ye were involved in the interpretation and analysis of the data. All authors approved the final version, and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent of participate
All the participants from NHANES 1999–2001 gave documented signed consent. These studies were approved by the ethics reviews from the National Center for Health Statistics (NCHS) Ethics Review Board. The NCHS IRB/ERB protocol number for 1999-2004 was # 98-12, 2005-2010 was #2005-06 and the number for 2011–2018 was #2011-17 and #2018-01.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cheng, K., Zhang, J., Ye, LY. et al. Geriatric nutrition risk index in the prediction of all-cause and cardiovascular mortality in older adults with hyperlipidemia: NHANES 1999–2018. BMC Geriatr 24, 634 (2024). https://doi.org/10.1186/s12877-024-05232-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-024-05232-6