
Abstract
Objective
The aim of present study was to evaluate the combined effect of hypertension and activities of daily living (ADL)/instrumental activities of daily living (IADL) with the risk of CVD, stroke and cardiac events.
Methods
A total of 14,083 participants aged 45 years or older from the China Health and Retirement longitudinal study were included in current study. Participants were divided into 4 groups according to hypertension and ADL/IADL status. Cox proportional hazards regression model was used to explore the associations between hypertension, ADL/IADL and new-onset CVD, stroke and cardiac events.
Results
During the 7-year follow-up, a total of 2,324 respondents experienced CVD (including 783 stroke and 1,740 cardiac events). Individuals with limitations in ADL alone, or with hypertension alone, or with both limitations in ADL and hypertension were associated with increased risk of CVD, with the adjusted hazard ratios (95% confidence intervals) were 1.17(1.00-1.35), 1.36(1.24–1.49) and 1.44(1.23–1.68), respectively. Those with limitations in ADL and hypertension also had higher risk of stroke (hazard ratios = 1.64; 1.26–2.14) and cardiac events (hazard ratios = 1.37; 1.14–1.64). Similarly, individuals with both limitations in IADL and hypertension were associated with increased risk of CVD (hazard ratios = 1.34; 1.15–1.57), stroke (hazard ratios = 1.50; 1.17–1.95) and cardiac events (hazard ratios = 1.27; 1.06–1.53).
Conclusion
Hypertension and limitations in ADL/IADL jointly increased the risk of CVD, stroke and cardiac events.
Similar content being viewed by others


Introduction
Cardiovascular diseases (CVD), well known for their heavy economic and social burden, seriously endanger health and quality of life, are the largest single contributor to global mortality and responsible for 18.6 million deaths in 2019, which is estimated to account for 32.3% of all-cause global deaths [1,2,3]. CVD progression involves the interaction of multiple risk factors in the long term, suggesting that the potential mechanism, risk factors and improved treatment of CVD are still hot areas of further research.
As one of the most fundamental ability, activities of daily living (ADL) and instrumental activities of daily living (IADL) refers to the repetitive primary acts that people must accomplish in their daily life in order to meet their basic needs [4, 5]. With the aging of the population and the increase of the elderly population, the reported estimated prevalence of the overall functional disability (up to 41.0% in Chinese elderly) among this group is relatively high and posing significant medical challenges to the nation and care-givers [6]. Both functional disability limitations are associated with aging and chronic diseases, such as stroke and heart disease [7,8,9,10]. Hypertension is the most important manageable risk factor for CVD. It is estimated that 43% of CVD events can be attributed to hypertension [11, 12]. In recent years, several studies have found a significant association between hypertension and limitation in ADL and IADL. Previous studies had reported the relation to limitation in ADL and IADL and hypertension [13, 14]. Individuals with hypertension tended to had a lower poorer ability to perform ADL [15]. However, no previous study has specifically evaluated the cumulative effect of hypertension and functional limitations (ADL or IADL limitation) on risk of CVD in the general population.
Therefore, in present study, we aimed to evaluate the combined effect of hypertension and functional limitations (focus on the ADL limitation) on the development of CVD among the middle-aged and elderly Chinese people, based on the data from the China Health and Retirement Longitudinal Study (CHARLS).
Methods
Study population
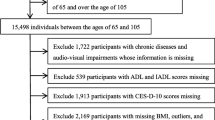
The CHARLS is an ongoing nationally representative and population-based study, that uses a multistage clustering sample method to select participants and conducted to collect a series of data regarding demographics, economic status, social networks, physical and psychological health in China [16, 17]. The first visit was accomplished in 2011–2012 (Wave 1) of 17,708 patients, subsequently third follow-up visits carried out after that, each nearly two years apart among survivors (2013–2014: Wave 2, 2015–2016: Wave 3 and 2017–2018: Wave 4) [17]. In current study, individuals who met all the following criteria were included: aged ≥ 45 years; with information about hypertension and ADL/ IADL status in Wave 1; without reported history of stroke and cardiac events in Wave 1; without loss to follow-up or death in follow-up [17]. Finally, a total of 14,083 individuals were eligible for subsequent analysis (Fig. 1).

Flow chart of sample selection and the exclusion criteria
The original CHARLS was approved by the Ethical Review Committee of Peking University (IRB00001052–11,015), and all participants signed the informed consent at the time of participation. The CHARLS publicly available at http://charls.pku.edu.cn [17]..
Assessment of hypertension and functional limitations
Blood pressure was measured with an electronic sphygmomanometer (Omron HEM-7200 Monitor) after 5 min of rest in the sitting position and was defined as the average of three separate measurements (record which arm’s blood pressure was measured). Hypertension was defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, current use of antihypertensive medications, or self-reported history of hypertension [17].
Functional limitations at baseline were assessed by the Katz ADL scale and the IADL scale [4, 18]. CHARLS asked respondents if they required assistance with any of the six ADLs (dressing, bathing, eating, getting into and out of bed, toileting and controlling urination and defecation) and with any of the five IADLs (preparing a hot meal, shopping for groceries, doing housework, taking medicines and managing money). Each item was divided into four responses as follows: [1] No, I do not have any difficulty [2], I have difficulty but still can do it [3], Yes, I have difficulty and need help, and [4] I cannot do it. Participants were scored 0 for responding “no difficulty” [1], for responding “have difficulty but still can do it” [2], for responding “have difficulty and need help”, and [3] for responding “cannot do it”. Participants who reported needing any help in any item (score of 2 or 3 in any item) were classified as having ADL or/and IADL limitations, thereafter called functional limitations [19].
Outcome assessments
The study outcome was CVD events, including heart disease and stroke. Similar to previous studies [17, 20],, CVD events were assessed by the following questions: “Have.
you been told by a doctor that you have been diagnosed with a heart attack, angina, coronary heart disease, heart failure, or other heart problems?” or “Have you been told by a doctor that you have been diagnosed with a stroke?”. Participants who reported heart disease or stroke were defined as having CVD.
Covariates assessments
The covariates were collected at baseline including age, sex, place of residence (rural vs. urban), smoking status (never smoking vs. ex-smoking vs. current smoking), educational level (illiteracy; primary school; middle school; high school or above), drinking status (never drinking vs. ex- drinking vs. current drinking), BMI (the weight.
in kilograms divided by the square of the height in meters), the presence or absence of other chronic diseases (dyslipidemia, diabetes mellitus, cancer, chronic lung disease, kidney disease, liver disease, arthritis, digestive disease and asthma) [17]. Dyslipidemia was defined as triglycerides ≥ 150 mg/dL, or total cholesterol ≥ 240 mg/dL, or high-density lipoprotein cholesterol < 40 mg/dL, or low-density lipoproteins cholesterol ≥ 160 mg/dL, or current use of the lipid-lowering medications, or self-reported history of dyslipidemia [21, 22]. And diabetes was defined as fasting glucose ≥ 126 mg/dL, or glycosylated hemoglobin (HbA1c) ≥ 6.5%, or treatment for diabetes mellitus, or self-reported history of diabetes [17].
Statistical analysis
Participants were divided into four subgroups according to hypertension and ADL/IADL status: group 1 (nonhypertension without limitations in ADL/IADL); group 2 (nonhypertension with limitations in ADL/IADL); group 3 (hypertension without limitations in ADL/IADL); group 4 (hypertension with limitations in ADL/IADL) [17].
Participants’ baseline characteristics are presented as percentages for categorical variables, as the means with standard deviation for normally distributed variables and as medians with interquartile range for nonnormally distributed variables. Demographic and clinical characteristics were compared between four subgroups by ANOVA or Kruskal–Wallis test for continuous variables and χ2 test for categorical variables. Kaplan–Meier curves and the log-rank test were used to compare the cumulative risk of events among four different groups [17]. We computed hazard ratios (HRs) and 95% confidence intervals (95% CIs) for CVD, stroke and cardiac events by using Cox proportional hazards models. Cox proportional hazards models were performed using three incremental levels of covariate adjustments. In model 1, age and sex were controlled. Model 2 was based on model 1, with the addition of living place, education level, smoking status, drinking status and BMI. In model 3, diabetes mellitus, cancer, chronic lung disease, kidney disease, liver disease, arthritis, digestive disease and asthma were further included with the variables in model 2 [17]. Furthermore, we analyzed both the additive and multiplicative interactions between the hypertension and ADL/IADL with CVD risk.
In the subgroup analyses, we were further performed to evaluate the association between the combined effect of hypertension and ADL/IADL with risk of CVD according to sex, age, living place, smoking, drinking, diabetes mellitus and BMI subgroups [17]. In sensitivity analysis, we evaluate the association between the combined effect of hypertension and ADL/IADL with study outcome using data from Wave 2 to Wave 4. Furthermore, we performed to evaluate the association between the combined effect of hypertension and ADL/IADL with risk of CVD, stroke and cardiac events using Cox proportional hazards regression models and assessed the influence of death as a competing risk for CVD, stroke and cardiac events in our interpretations by performing competing risk analyses [17]. Two tailed P < 0.05 was considered to be statistically significant. All statistical analyses were conducted using SAS statistical software (version 9.4, Cary, NC).
Results
A total of 14,083 participants (7,049 men and 7,034 women) were included in the analysis, and the average age was 58.65 ± 9.70 years. In current study, baseline characteristics were well balanced between included and excluded participants (Table S1). According to study design, participants were divided into four subgroups: group 1 (nonhypertension without limitations in ADL, n = 7,361); group 2 (nonhypertension with limitations in ADL, n = 1,196); group 3 (hypertension without limitations in ADL, n = 4,669); group 4 (hypertension with limitations in ADL, n = 857). Baseline characteristics, including age, sex, education level, history of dyslipidemia and diabetes mellitus, BMI, FBG, SBP and DBP were significantly different among the four subgroups (Table 1).
A total of 2,324 individuals experienced CVD (including 783 stroke and 1,740 cardiac events), during the 7-year follow-up. We found significant additive and/or multiplicative interactions of hypertension and ADL/IADL with CVD risk. Participants with hypertension and limitations in ADL or limitations in IADL had the highest cumulative incidence of CVD, stroke and cardiac events (Fig. 2; Figure. S1). In the age and sex adjusted model, compared with individuals without limitations in ADL and nonhypertension, the HRs (95% CIs) for the risk of CVD were 1.49(1.27–1.75), 1.49(1.35–1.65) and 1.95(1.64–2.32) for those with limitations in ADL and nonhypertension, with hypertension and without limitations in ADL, with limitations in ADL and hypertension, respectively. After further adjusting for covariates, individuals with limitations in ADL alone (HR = 1.17, 95%CI 1.00-1.35), or with hypertension alone (HR = 1.36, 95%CI 1.24–1.35), or with both limitations in ADL and hypertension were associated with increased risk of CVD (HR = 1.44, 95%CI 1.23–1.68) (Table 2). Similarly, participants with limitations in ADL alone, or with hypertension alone, or with both limitations in ADL and hypertension were associated with higher risk of stroke, and those with hypertension alone, or with both limitations in ADL and hypertension were associated with higher risk of cardiac events (Table 2). When it comes to IADL, individuals with both limitations in IADL and hypertension were associated with increased risk of CVD (HR = 1.34, 95%CI 1.15–1.57), stroke (HR = 1.50, 95%CI 1.17–1.95) and cardiac events (HR = 1.27, 95%CI 1.06–1.53) (Table 3).

Kaplan–Meier curves for the cumulative risk of CVD, stroke and cardiac events by hypertension/ADL status
Group 1 (nonhypertension without limitations in ADL); group 2 (nonhypertension with limitations in AD); group 3 (hypertension without limitations in ADL); group 4 (hypertension with limitations in ADL)
In the subgroup analysis, the significant associations between hypertension alone, or with both limitations in ADL and hypertension with risk of CVD were observed in almost all subgroups (Table 4). Significant interactions between hypertension/ADL and subgroups were observed in sex, age, diabetes mellitus and BMI subgroups (all P-interaction<0.05). In sensitivity analysis, we evaluate the association between the combined effect of hypertension and ADL/IADL with study outcome using data from Wave 2 to Wave 4 (from 2013 to 2018), and significant associations were found between hypertension and ADL/IADL with increasing risk of CVD, stroke and cardiac events (Table 5). In the competing risk analyses, the associations between hypertension and ADL/IADL with risk of CVD, stroke and cardiac events also yielded similar patterns of results as the main analyses when death was defined as competing events (Table S2).
Discussion
In current nationwide longitudinal prospective cohort study of Chinese adults aged 45 years and above, we first demonstrated that coexistent of hypertension and ADL/IADL limitation conferred increased risk of CVD, stroke and cardiac events than each component individually, and the combined effect was independent of age, sex and other covariates. To our knowledge, this is the first study to assess the cumulative effect of hypertension and ADL/IADL on CVD, stroke and cardiac events in the Chinese adults. Our findings suggest a combination of hypertension and ADL/IADL could provide potentially predictive information for CVD risk.
As we all known, hypertension is the most important modifiable risk factor for CVD [23]. Accumulating evidence suggests the importance of antihypertensive pharmacotherapy and blood pressure management not only toward preventing CVD but also in the management of other diseases [24, 25]. Evidence from the Chinese Longitudinal Healthy Longevity Survey (CLHLS) indicated that individuals with ADL limitations group had a 77% higher risk of developing stroke than the non-ADL limitations group [26]. Another study from CHARLS also found functional limitations were significantly associated with subsequent incident CVD, stroke and death among the middle-aged and older Chinese adults [9]. In consistent with previous studies, our finding suggested that individuals with ADL limitations or hypertension were associated with increased risk of CVD. All of the studies provided more valid evidence that both hypertension and ADL limitations were risk factors for CVD risk. However, whether there is a synergistic effect between hypertension and functional limitations (ADL or IADL limitation) on CVD risk is still unknown.
Previous studies had found a mean home SBP of ≥ 135 mmHg was a significantly important risk factor for a loss of functional independence in the elderly aged 75 years or older [14]. In a meta-analysis of 6 studies, blood pressure lowering using antihypertensive drugs was associated with preservation in ability to carry out ADL (OR = 0.84; 95% CI = 0.77–0.92) [15]. Activities of daily living was reported associated with blood pressure [27]. In a cohort of community-dwelling elders, results indicated that ADL status modifies the associations between blood pressure components and incident CVD and all-cause mortality [28]. Considering the closely relationship between hypertension, ADL/IADL and CVD, we focused on the combined effect of hypertension and ADL/IADL. In current study, we found significant additive and/or multiplicative interactions of hypertension and ADL/IADL with CVD risk. Participants with hypertension and limitation in ADL/IADL had the highest cumulative incidence and highest risk of CVD, stroke and cardiac events indicating that co-existence of hypertension and limitation in ADL/IADL had a higher risk of CVD than each factor alone. Our findings provide a more valid appraisal of the relationship between hypertension and ADL/IADL, especially on CVD risk.
Considering the high prevalence of hypertension and limitation in ADL/IADL and coexistence of them, especially with the growing aging population [29, 30]. It is clinical interest to monitor hypertension and ADL/IADL status through frequent BP measurement and routine ADL/IADL measurement for primary prevention of CVD in the general population. Although significant interaction with the joint effect of hypertension and ADL/IADL on CVD risk were found in sex, age, diabetes and BMI subgroups. Whether in males or females, age more than or less 60 years, with or without diabetes, BMI more than or less 24 (kg/m2) subgroups, individuals with co-existence of hypertension and limitation in ADL/IADL had a higher risk of CVD. Therefore, the associations between hypertension and limitation in ADL/IADL on CVD risk were robust in individuals with or without CVD risk factor.
The precise mechanisms linking hypertension and limitation in ADL/IADL with risk of CVD are incompletely understood but several potential explanations could be proposed. Limitation in ADL/IADL restrict actives, influence lifestyle behaviors, increase financial burden, and delay the treatment of related chronic diseases, such as hypertension and diabetes [31, 32]. Furthermore, ADL limitations may also increase the prevalence of depressive symptoms, anxiety symptoms and suicidal ideation [33, 34], which evoke inflammation, platelet activation and thrombosis, and autonomic nerve dysfunction [35]. While, hypertension is one of the most important risk factors for CVD, which was associated with oxidative stress on the arterial wall, vascular damage, and vascular endothelial cell dysfunction [36,37,38]. Accordingly, it is biologically plausible that hypertension and functional limitations could interact with each other and jointly increase the possibility of CVD through different mechanisms.
Some strengths of our study include, first, the current study was based on the data from the CHARLS study, which is a large nationally representative cohort study with a high response rate, and potential confounders were collected and controlled in the multivariable models. Second, unlike previous studies, this is the first to assess the cumulative effect of hypertension and ADL/IADL on CVD, stroke and cardiac events. However, several potential limitations of present study need to be mentioned. First, the present study was not a prespecified analysis. Although, we had adjusted a series of confounders. This observational analysis could be influenced by potential biases and confounding factors. Therefore, our study only generates hypotheses for future studies. Second, the CHARLS study was exclusively a Chinese population aged 45 years and older. Thus, the findings from our study might not be generalizable to other populations or younger individuals. Third, some of the participants were excluded from analysis due to incomplete exposure or outcome data. Fourth, CVD was based on self-reported doctor’s diagnosis of stroke or cardiac events, which may cause information bias. However, self-reported history of disease has been proven to possess relatively good reliability [39, 40]. Finally, individuals who lack knowledge about household tasks due to a historical lack of engagement may also cause bias in ADL and IADL assessment.
In conclusion, our results suggested that there was a combined effect of hypertension and ADL/IADL on risk of CVD, stroke and cardiac events among the middle-aged and elderly Chinese. Using the combination indicator of hypertension and ADL/IADL could better assess CVD risk. Further study needs to be conducted to explore the biological mechanism.
Data availability
The datasets generated during and/or analyzed during the current study are available in the CHARLS repository, http://charls.pku.edu.cn.
References
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021.
Liu S, Li Y, Zeng X, Wang H, Yin P, Wang L, et al. Burden of cardiovascular diseases in China, 1990–2016: findings from the 2016 global burden of disease study. JAMA Cardiol. 2019;4(4):342–52.
Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596.
Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914–9.
Norström T, Thorslund M. The structure of IADL and ADL measures: some findings from a Swedish study. Age Ageing. 1991;20(1):23–8.
Report of the World Health Organization. Active ageing: a policy framework. Aging male: Official J Int Soc Study Aging Male. 2002;5(1):1–37.
Kishimoto M, Ojima T, Nakamura Y, Yanagawa H, Fujita Y, Kasagi F, et al. Relationship between the level of activities of daily living and chronic medical conditions among the elderly. J Epidemiol. 1998;8(5):272–7.
Sousa RM, Ferri CP, Acosta D, Albanese E, Guerra M, Huang Y, et al. Contribution of chronic diseases to disability in elderly people in countries with low and middle incomes: a 10/66 Dementia research group population-based survey. Lancet (London England). 2009;374(9704):1821–30.
Hu Z, Zheng B, Kaminga AC, Zhou F, Xu H. Association between functional limitations and incident cardiovascular diseases and all-cause mortality among the middle-aged and older adults in China: a population-based prospective cohort study. Front Public Health. 2022;10:751985.
Gohbara M, Nishimura K, Nakai M, Sumita Y, Endo T, Matsuzawa Y, et al. Low activities of daily living associated with increased cardiovascular disease mortality in Japan - analysis of health records from a nationwide claim-based database, JROAD-DPC. Circulation Rep. 2018;1(1):20–8.
Zhang G, Yu C, Zhou M, Wang L, Zhang Y, Luo L. Burden of ischaemic heart disease and attributable risk factors in China from 1990 to 2015: findings from the global burden of disease 2015 study. BMC Cardiovasc Disord. 2018;18(1):18.
Global regional. National disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet (London England). 2016;388(10053):1603–58.
Kuo HK, Jones RN, Milberg WP, Tennstedt S, Talbot L, Morris JN, et al. Effect of blood pressure and diabetes mellitus on cognitive and physical functions in older adults: a longitudinal analysis of the advanced cognitive training for independent and vital elderly cohort. J Am Geriatr Soc. 2005;53(7):1154–61.
Nishinaga M, Takata J, Okumiya K, Matsubayashi K, Ozawa T, Doi Y. High morning home blood pressure is associated with a loss of functional independence in the community-dwelling elderly aged 75 years or older. Hypertens Research: Official J Japanese Soc Hypertens. 2005;28(8):657–63.
Canavan M, Smyth A, Bosch J, Jensen M, McGrath ER, Mulkerrin EC, et al. Does lowering blood pressure with antihypertensive therapy preserve independence in activities of daily living? A systematic review. Am J Hypertens. 2015;28(2):273–9.
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. 2014;43(1):61–8.
Zheng X, Han L, Shen S. Hypertension, remnant cholesterol and cardiovascular disease: evidence from the China health and retirement longitudinal study. J Hypertens. 2022;40(11):2292–8.
Katz S. Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living. J Am Geriatr Soc. 1983;31(12):721–7.
Connolly D, Garvey J, McKee G. Factors associated with ADL/IADL disability in community dwelling older adults in the Irish longitudinal study on ageing (TILDA). Disabil Rehabil. 2017;39(8):809–16.
Chen J, Kuang J, Tang X, Mao L, Guo X, Luo Q, et al. Comparison of calculated remnant lipoprotein cholesterol levels with levels directly measured by nuclear magnetic resonance. Lipids Health Dis. 2020;19(1):132.
2016 Chinese guideline for the management of dyslipidemia in adults. Zhonghua Xin xue guan bing za zhi. 2016;44(10):833–53.
Deng Y, Gao Q, Yang T, Wu B, Liu Y, Liu R. Indoor solid fuel use and incident arthritis among middle-aged and older adults in rural China: a nationwide population-based cohort study. Sci Total Environ. 2021;772:145395.
Oparil S, Acelajado MC, Bakris GL, Berlowitz DR, Cífková R, Dominiczak AF, et al. Hypertens Nat Reviews Disease Primers. 2018;4:18014.
Kokubo Y, Iwashima Y. Higher blood pressure as a risk factor for diseases other than stroke and ischemic heart disease. Hypertens (Dallas Tex: 1979). 2015;66(2):254–9.
Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. 2021;52(7):e364–e467.
Wei ZS, Chen YS, Wu Y, Kang CY, Wu JY, Yang Y, et al. Limitations in activities of daily living increase the risk of stroke in older Chinese adults: a population-based longitudinal study. Neural Regeneration Res. 2022;17(3):643–8.
Valenzuela PL, Carrera-Bastos P, Gálvez BG, Ruiz-Hurtado G, Ordovas JM, Ruilope LM, et al. Lifestyle interventions for the prevention and treatment of hypertension. Nat Reviews Cardiol. 2021;18(4):251–75.
Peralta CA, Katz R, Newman AB, Psaty BM, Odden MC. Systolic and diastolic blood pressure, incident cardiovascular events, and death in elderly persons: the role of functional limitation in the cardiovascular health study. Hypertension (Dallas, Tex: 1979). 2014;64(3):472–80.
Liang Y, Song A, Du S, Guralnik JM, Qiu C. Trends in disability in activities of daily living among Chinese older adults, 1997–2006: the China health and nutrition survey. Journals Gerontol Ser Biol Sci Med Sci. 2015;70(6):739–45.
Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–37.
Pavela G. Functional status and social contact among older adults. Res Aging. 2015;37(8):815–36.
Fingerman KL, Ng YT, Huo M, Birditt KS, Charles ST, Zarit S. Functional limitations, social integration, and daily activities in late life. Journals Gerontol Ser B Psychol Sci Social Sci. 2021;76(10):1937–47.
Ahn J, Kim BJ. The relationships between functional limitation, depression, suicidal ideation, and coping in older Korean immigrants. J Immigr Minor Health. 2015;17(6):1643–53.
Backe IF, Patil GG, Nes RB, Clench-Aas J. The relationship between physical functional limitations, and psychological distress: considering a possible mediating role of pain, social support and sense of mastery. SSM - Popul Health. 2018;4:153–63.
Corrigendum to. Depression and coronary heart disease: 2018 position paper of the ESC working group on coronary pathophysiology and microcirculation developed under the auspices of the ESC committee for practice guidelines. Eur Heart J. 2020;41(17):1696.
Carey RM, Moran AE, Whelton PK. Treatment of hypertension: a review. JAMA. 2022;328(18):1849–61.
Alexander RW. Theodore Cooper memorial lecture. Hypertension and the pathogenesis of atherosclerosis. Oxidative stress and the mediation of arterial inflammatory response: a new perspective. Hypertension (Dallas, Tex: 1979). 1995;25(2):155–61.
Drazner MH. The progression of hypertensive heart disease. Circulation. 2011;123(3):327–34.
St Sauver JL, Hagen PT, Cha SS, Bagniewski SM, Mandrekar JN, Curoe AM et al. Agreement between patient reports of cardiovascular disease and patient medical records. Mayo Clinic proceedings. 2005;80(2):203–10.
Gao K, Cao LF, Ma WZ, Gao YJ, Luo MS, Zhu J, et al. Association between sarcopenia and cardiovascular disease among middle-aged and older adults: findings from the China health and retirement longitudinal study. EClinicalMedicine. 2022;44:101264.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Xiaowei Zheng and Wenyan Wu conceived and designed the research; Yiqun Li and Xiaowei Zheng wrote the manuscript; and Xiao Ren, Minglan Jiang, Longyang Han performed the data analysis. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The original CHARLS was approved by the Ethical Review Committee of Peking University (IRB00001052–11015), and all participants signed the informed consent at the time of participation. This research followed the guidance of the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Y., Jiang, M., Ren, X. et al. Hypertension combined with limitations in activities of daily living and the risk for cardiovascular disease. BMC Geriatr 24, 225 (2024). https://doi.org/10.1186/s12877-024-04832-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-024-04832-6