
Abstract
Background
People with dementia and their caregivers are prone to suicidal behaviors due to difficulty adjusting to their initial caregiving role and due to emotional disturbances resulting from deterioration of functioning. The present systematic review (1) explored the prevalence of and risk factors for suicidal behavior and (2) assessed the similarities and differences in the prevalence and risk factors for suicidal behavior between people with dementia and their caregivers.
Methods
A comprehensive literature search for research articles published between 1950 and 2023 was carried out using major databases, such as Google Scholar, Web of Science, PubMed, Scopus, PsycINFO, EMBASE, the Cochrane Library, and Medline.
Results
A total of 40 research articles were selected for review. A total of 12 research articles revealed that the prevalence of suicidal behavior among caregivers ranged from 4.7% to 26%. However, the risk of suicidal behavior among people with dementia was inconsistent, as only 17 out of 28 selected studies reported the risk of suicidal behavior among people with dementia. The risk factors associated with suicidal behavior among caregivers of people with dementia could be both self-related and care receiver-related factors, whereas risk factors in people with dementia were self-related factors. Notably, greater cognitive decline, which impairs individuals’ ability to carry out complex acts and planning, may lower their suicidal risk. Finally, assessment of the risk of bias indicated that 95% of the selected studies had unclear risk.
Conclusion
Self-related and care receiver-related factors should be assessed among caregivers of people with dementia to evaluate the risk of suicidal behavior. In addition, we recommend evaluating suicidal risk in people with dementia in the early phase of dementia when cognitive decline is less severe. However, as the majority of the selected studies had unclear risk of bias, future studies with improved methodologies are warranted to confirm our study findings.
Similar content being viewed by others


Introduction
Suicide is defined as any act of taking one’s own life on purpose [1]. Annually, suicide results in more than 700,000 life losses globally, and it is prevalent not only in developed countries but also in low- and middle-income countries [2]. Suicidal behavior can be classified into three categories: (1) suicidal ideation, which refers to thoughts of engaging in behavior that leads to the end of one’s life on purpose; (2) suicide planning, which is the formulation of a specific method that leads to the end of one’s life on purpose; and (3) suicidal attempts, which involve engaging in acts that potentially lead to self-injury and at least with some intent to die on purpose [3].
Dementia has been recognized as a global public health issue, as more than 55 million people live with dementia worldwide. Every year, approximately 10 million incident diagnoses are recorded, and current projections assume that by 2050, approximately 139 million people globally will live with dementia [4]. People with dementia not only are affected by cognitive decline but also experience various emotional problems [5,6,7]. Caregivers—predominantly family but also friends—provide a majority of dementia care, estimated to represent 40% of the total cost of dementia worldwide [8]. Several studies have shown that mental health aspects play a central role in the overall health of people with dementia [8]. For instance, caregivers of people with dementia have been reported to exhibit a greater risk of experiencing depression and anxiety than caregivers of patients with other medical conditions [9]. In essence, people with dementia and their caregivers are at risk of suicidal behaviors. In the context of caregivers of people with dementia, the prevalence of suicidal ideation range from 4.69% to 77.78%, while the prevalence of suicidal attempt range from 5.9% to 16.1% [10]. For suicidal behavior among people with dementia, the odds of suicidal ideation, suicidal attempt, and completed suicide have increased by 1.37-fold, 2.24-fold, and 1.28-fold, respectively compared to those of control subjects (age-matched or non-age-matched subjects without dementia) [11]. Despite the documented risk of suicidal behavior among people with dementia, the findings are still inconclusive, as some studies on suicidal behavior among people with dementia have not reported an increased risk of suicide [12]. Hence, exploring the possible reasons underlying the inconsistencies in suicidal risk among people with dementia is interesting.
According to a systematic review and meta-analysis of eight studies on suicidal behavior among caregivers of people with dementia, the risk factors contributing to increased suicidal behavior include depression, previous suicidal attempts, a sense of hopelessness, a history of comorbid psychiatric illness, lack of social support, demoralization, pain, and a feeling of being a burden on others [10]. Risk factors leading to suicidal behavior among people with dementia include being diagnosed with dementia at a younger age, having advanced dementia, feeling a loss of control, feeling a burden due to functional impairment, feeling lonely and being isolated [11].
Basically, the mental health of people with dementia and their caregivers is expected to exhibit a bidirectional effect in which the mental health of one group affects the mental health of another group and vice versa [13]. It would be interesting to explore whether the risk factors leading to suicidal behavior among caregivers of people with dementia as well as for people with dementia are both caregiver-related and care receiver-related, as management should then be tailored to include early identification and treatment of risk factors for both caregiver stress and neuropsychiatric symptoms in people with dementia.
In addition, although previous studies on the risk of suicidal behavior among people with dementia and their caregivers have identified numerous risk factors, none of these studies have analyzed and categorized the risk factors in a systematic way so that specific psychosocial interventions and special attention could be given to managing these risk factors appropriately to safeguard the mental well-being of both caregivers and people with dementia. To the best of our knowledge, although the mental health of people with dementia and their caregivers is expected to exhibit a bidirectional effect, none of the previous studies have identified risk factors that are associated with suicidal behavior in both caregivers and people with dementia. Moreover, to date, no narrative or systematic review has explored the risk factors for suicidal behavior in people with dementia and their caregivers within the same review or investigated the similarities and differences in the risk factors contributing to suicidal behavior among people with dementia and their caregivers.
Hence, the present systematic review addresses this research gap by: (1) exploring the prevalence and risk factors for suicidal behavior among these two target populations and (2) assessing the similarities and differences in the prevalence and risk factors for suicidal behavior between people with dementia and their caregivers.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement [14].
Search strategies
An electronic search of published literature from 1950 to 2023 was carried out using major databases, such as Google Scholar, Web of Science, PubMed, Scopus, PsycINFO, EMBASE, the Cochrane Library, and Medline. Initially, a preliminary search was performed using keywords such as “dementia” and “suicide” OR “suicide and dementia” OR “suicide and people with dementia”, “caregivers of people with dementia” and “suicide” OR “suicide and caregivers of people with dementia”. In addition, hand searching was carried out in this review, resulting in a page-to-page review of the key journals that may have published studies on suicidal behaviors of people with dementia and their caregivers. The list of key journals in which the authors performed manual searching is listed in Additional file 1. Hand searching was also carried out for conference proceedings.
Inclusion and exclusion criteria
The literature was eligible for review if it fulfilled the following inclusion criteria: (1) was published in English language peer review journals, including in-press articles; (2) was published in research articles, case reports, or case series; and (3) was related to the prevalence and associated factors of suicide among people with dementia and caregivers of people with dementia. The literature was excluded if (1) the preprint version of the research article was not peer reviewed and its content changed.
Data extraction
Two independent reviews of the search results were carried out by two authors (MFILBA and NIS) during the title/abstract screening stage and full-text screening stage. Dual independent review of the search results was reported to increase the number of relevant studies identified for systematic review [15]. During screening for the inclusion of the articles for review, any discrepancies in the findings between the two authors were discussed and resolved. If there was difficulty resolving any discrepancies, the opinion of the 3rd author (MAM) was sought. The details of the search steps in this review in one of the major databases are described in Additional file 2.
Initially, during the data extraction, two authors (MFILBA and NIS) individually extracted information from the articles for cross-checking (the information extracted included (information about the article [author(s), year of publication, title, and DOI]; eligibility for review; methods [study type, participant recruitment and selection; study duration; and study quality]; participants [total number, sample size estimation and actual sample size; age, sex, ethnicity, country, diagnostic criteria, sociodemographics, types of dementia, and history of mental illness]; outcomes [outcomes and timepoint(s) collected and reported; instrument used for diagnosis and rating]; results [for each outcome of interest: look for sample size, missing data, estimation of effect with confidence intervals and p value; and subgroup analysis]; and others [funding source, key conclusion, references to other relevant studies, correspondence requirement, and miscellaneous comments by study authors]. After reviewing a few articles together, a consensus on what to extract from the articles was reached, and the work was split between the two authors. During individual data extraction, the authors remained in constant communication. Articles that were difficult to determine were discussed among the authors. The interrater reliability between the authors was computed as Cohen’s kappa (κ) using the following formula: κ = (p0 - pe)/(1- pe), where p0 = relative observed agreement among the raters and pe = hypothetical probability of chance agreement. po = the degree to which both of the raters agreed with each other (both raters rated “Yes” or “No” divided by the total ratings), which was 0.8830; both raters agreed “Yes” = 151; both raters agreed “No” = 151; and the total number of ratings = 342. pe = the sum of “Yes” divided by the total ratings, multiple with rater 2 rating as “Yes” divided by the total ratings and (rater 1 rating as “No” divided by the total ratings, multiple with rater 2 rating as “No” divided by the total ratings). Hence, Cohen’s kappa was good (κ = 0.77), with substantial agreement between the two raters. The authors then coded the study characteristics and findings into a database. The coded data included methodological characteristics (study design; participants’ sociodemographic characteristics, such as age and sex; sampling method; sample size estimation; study objectives; and outcome measures); study findings; and study limitations. The review was organized into the following categories: prevalence of suicide among people with dementia, prevalence of suicide among caregivers of people with dementia, associated factors of suicide among people with dementia, associated factors of suicide among caregivers of people with dementia, and differences in prevalence of suicide, associated factors and suicidal behavior between people with dementia and caregivers of people with dementia.
In addition, the risk of bias of the selected studies was assessed with the Risk of Bias Assessment Tool for Nonrandomized Studies (RoBANS). The RoBANS is a tool developed to assess the risk of bias in the findings of nonrandomized studies. The RoBANS consists of 6 domains: selection of participants, confounding variables, measurement of intervention (exposure), blinding of outcome assessment, incomplete outcome data and selective outcome reporting (table). The mean time needed to complete the RoBANS was shorter than that needed for another risk assessment tool, the Methodological Items for NOn-Randomized Studies (MINORS) (9.5 min [SD = 3.39] per study vs. 10.45 [SD = 3.54] per study). RoBANS exhibited good ratings in terms of user convenience for 3 items evaluated by reviewers (mean of 5.7 of 7 on the Likert scale; 0.81%). Additionally, the facial validity of 7 items evaluated by external experts was “fair” (mean 5.4 of 7 on the Likert scale), and all the experts recommended the use of this scale to assess the risk of bias in nonrandomized studies [16].
Initially, two authors (MFILBA and NIS) independently assessed the risk of bias in the selected studies. Then, any disagreements were discussed and resolved, and arbitration was performed by the third author (MAM).
Results
Characteristics of the selected studies
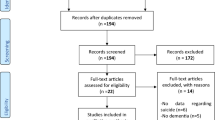
An initial database search for titles and abstracts yielded 2,400 articles, but 2,150 articles were excluded as duplicates. Careful screening of the abstracts of the 250 remaining articles resulted in the exclusion of another 130 articles because they were not specific to suicide and/or were systematic reviews, narrative reviews, letters to the editor and editorials, commentaries, correspondences, or unpublished articles. Then, 120 full-text articles were screened for eligibility, and another 88 articles were excluded because they focused on assisted suicide or suicide in patients with illnesses and caregivers of patients with illnesses other than dementia or did not present enough information (studies that did not include study type, participant recruitment and selection, study duration, diagnostic criteria, sociodemographics, missing data, estimation of effects with confidence intervals and p values, or key conclusions). Hence, 40 articles were ultimately included in the review after another 8 additional articles were discovered through manual searching. The flow of the search findings is illustrated in Fig. 1.

PRISMA flowchart summarizing the selection of research articles for this systematic review
The studies selected for review included 12 studies on suicidal behavior among caregivers of people with dementia and 28 studies on suicidal behavior among people with dementia. Six of the selected studies on suicidal behavior among caregivers of people with dementia were quantitative studies, 5 were qualitative studies, and 1 was an intervention study. All 26 selected studies on suicidal behavior among people with dementia were quantitative studies. The total combined sample size of studies on suicidal behavior among caregivers of people with dementia was 1,555,251 subjects (range from 9 subjects to 1,018,000 subjects), while the total combined sample size of studies on suicidal behavior among caregivers of people with dementia was 6,646,808 subjects (range from 24 to 2,667,987 subjects). None of the 40 selected studies mentioned the sampling method, except for the Valente et al. (2011), Lewis (2015) studies, and Choi et al. (2021) [17,18,19]. Similarly, all 40 studies did not calculate the estimated sample size needed to achieve the objectives of the studies. The characteristics, findings, and limitations of the selected studies are summarized in Table 1.
Bias assessment of the selected studies
For the assessment of the risk of bias of the selected studies using the RoBANS, the findings are summarized in Fig. 2 and Additional file 3. Regarding bias arising from the selection of participants (65%) and confounding factors (60%), more than half of the selected studies had a high risk of bias, whereas most of the selected studies with a low risk of bias investigated suicidal behavior among people with dementia. In contrast, with regard to bias arising from inadequate measures of exposure, the majority of the selected studies had a low risk (85%). In terms of inadequate blinding of outcome assessment, the risk of bias of all the selected studies was unclear because the studies did not assess this outcome. Due to inadequate handling of incomplete outcome data and bias caused by selective outcome reporting, all the selected studies had a low risk of bias, as there was no missing data. According to the overall assessment of risk of bias, 92.5% of the selected studies had an overall risk of bias, as they had a low risk of bias for at least two items in the RoBANS, but the risk of bias for other items was high or unclear (Fig. 2).

Risk of bias assessment of the selected studies using the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS)
Suicidal behavior among caregivers of people with dementia
Only two out of the twelve selected studies had relatively larger sample sizes (with a sample size of more than 1000 subjects) [26, 28]. Almost all the selected studies included a larger proportion of female subjects, ranging from 55.6% to 100%. The prevalence of suicidal behavior among caregivers of people with dementia in selected cross-sectional quantitative studies ranged from 4.7% to 26% [17, 22, 28]. However, in large quantitative studies involving sampling at the national level, the prevalence of suicidal behavior reported among caregivers of people with dementia ranged from 0.19% to 2.9% [26, 28]. The suicidal behaviors exhibited included suicidal thoughts, death wishes, and contemplating suicide [17, 18, 21, 22, 24, 25, 28]. Despite having suicidal thoughts, only half of the caregivers reported that they may commit suicide, and 30% of the caregivers disclosed that they may inform someone if they plan to attempt suicide in the future [22].
Regarding the thoughts and emotional responses of the caregivers toward caring for people with dementia, the selected qualitative studies identified several themes, which included concern about being trapped in an unescapable role as a caregiver, providing end-of-life care to one’s loved ones, thinking about impending death and wish for euthanasia, the caregiver’s role in surrogate decision making on behalf of one’s care receiver, experience of suicidal thoughts of the caregiver, thoughts of homicide and euthanasia of the caregiver toward the care receiver, challenges finding useful resources by the caregiver to facilitate caregiving, struggle of the caregiver with mental health issues (such as emotional disturbances, health management and family dynamics), acceptance of the caregiver’s role and attempt to do their best caring for the family member with dementia, and discovery of a strategy to survive the caregiver’s role (such as engaging in health diet, rest and sleep, walking, hobbies, and continuing medical checkup) [18, 23, 25, 27].
The most significant risk factor led to the occurrence of suicidal behavior among caregivers of people with dementia was the presence of depression [17, 20,21,22, 24, 26]. The prevalence of depression reported among caregivers of people with dementia with suicidal behavior ranged from 39.6% to 94% [21, 24]. In addition, other significant risk factors that predispose individuals to suicidal behavior among caregivers of people with dementia included increased severity of anxiety symptoms [17, 24, 26], preexisting physical health conditions [24,25,26], preexisting mental health problems [23, 28], and absence of social and family support [24, 26]. The frequencies of the risk factors that contribute to the occurrence of suicidal behavior among caregivers of people with dementia identified in the selected studies are summarized in Table 2.
Suicidal behavior among people with dementia
Most of the selected studies consisted of a larger proportion of female subjects, except for nine studies, which consisted of more male subjects [19, 32, 35, 37, 39, 43, 50, 52, 53]. In most of the studies, the proportion of female subjects ranged from 52.8% to 82.0% [29,30,31, 33, 34, 36, 38, 40,41,42, 44,45,46,47]. Among the selected studies, only 13 studies specified the types of dementia diagnosed among the subjects; 11 studies examined subjects with Alzheimer’s disease [19, 29, 32,33,34,35, 42, 43, 46, 49, 55], while only one study investigated mixed Alzheimer’s disease and vascular dementia and frontotemporal dementia [31, 45].
Among the included studies that reported the prevalence of suicidal behavior among people with dementia, the prevalence ranged from 0.005% to 40% [19, 29, 42, 44,45,46,47,48,49, 51, 54]. The suicide rates reported in two included studies among people with dementia [52, 55] were 9.3 per 100,000 persons per year and 26.4 per 100,000 persons per year. However, the risk of suicidal behavior among people with dementia was inconclusive, as 17 selected studies reported the risk of suicidal behavior among people with dementia [19, 33, 34, 36, 37, 45,46,47, 49,50,51,52,53,54,55], but 11 selected studies did not [29, 30, 32, 35, 39,40,41,42,43,44, 48]. Among studies with relatively large sample sizes (more than 1000 subjects), only nine reported an increased risk of suicidal behavior [19, 36, 49,50,51,52,53,54,55], whereas four studies found no association between the risk of suicidal behavior and dementia [37, 38, 40, 48].
The suicidal behaviors reported included deliberate self-harm, suicidal ideation, and suicidal attempts (such as self poisoning, drowning, hanging, and the use of firearms) [31, 33, 34, 36, 37, 45,46,47, 49, 50, 52]. Six large-scale population-based studies indicated that the risk of suicidal behavior was greater within the first 3 months to 1 year after diagnosis and in people diagnosed with dementia before the age of 65 years [36, 48,49,50, 52, 53].
Two of the most significant risk factors for suicidal behavior among people with dementia were greater severity of depression and anxiety [31, 34, 45, 46, 50, 52, 54] and shortly or within 3 months of being diagnosed with dementia [36, 47, 48, 50, 52,53,54]. In addition, the other significant risk factors contributing to suicidal behavior among people with dementia included younger age at diagnosis (within 50 to 69 years old) [36, 45, 48, 52], history of inpatient psychiatric hospitalization [37, 38, 50], diagnosis of Alzheimer’s disease alone [19, 47], passive self-harm such as refusal to eat, drink, or take medication [33, 37], presence of comorbid psychiatric illnesses (such as mood disorders, schizophrenia, somatoform disorders and anxiety disorders) [19, 48], better cognitive function [43, 47], and advanced dementia [47, 49]. The frequencies of the risk factors that contributed to the occurrence of suicidal behavior among people with dementia, as identified in the selected studies, are presented in Table 2.
Discussion
This comprehensive systematic review summarized the prevalence and risk factors associated with the occurrence of suicidal behavior and the differences between people with dementia and their caregivers.
Prevalence of suicidal behavior in people with dementia and their caregivers
There were a few differences in the prevalence and risk of suicidal behavior between people with dementia and their caregivers. First, there was significant and clear evidence from selected studies that the risk of suicide was associated with caregivers of people with dementia (all selected studies indicate suicidal risk among caregivers of people with dementia). In contrast, evidence of the risk of suicide among people with dementia has been inconclusive (only 17 out of 28 studies indicated the risk of suicide among people with dementia). Notably, there were wide ranges of prevalence rates for both caregivers (4.7% to 26%) and people with dementia (0.005% to 40.0%), which is indicative of heterogeneity among the selected studies, which differ in methodology and causes of dementia. This may be a possible reason for the discrepancy between the association of suicidal behavior in people with dementia and that in their caregivers. Another possible reason for the inconclusive risk of suicidal behavior among people with dementia is that suicidal risk involves complex acts and include planning for suicide. Commonly, people with Alzheimer’s disease at an earlier stage after diagnosis and at a younger age (less than 65 years old) may have intact cognition, characterize by lesser cognitive decline and more intact daily functioning, could have higher ability to carry out complex act such as attempted suicide and planning for suicide, leading to higher suicidal risk among this group of people with dementia [29, 33, 40, 43, 48,49,50, 52, 53]. Moreover, the risk factors for suicidal behavior among people with dementia (lower degree of wish to live, greater degree of expression of wishing to die, greater severity of depression and anxiety symptoms, and stress and hopelessness) also pinpoint toward a greater risk of suicidal behavior among those with more intact cognitive function [31, 40, 45, 50].
Second, with reference to selected studies with larger population-based sample sizes (n > 100,000), the prevalence of suicidal behavior is relatively greater among people with dementia (0.005% to 8.17%) [19, 36, 49, 50, 52, 53] than among caregivers of people with dementia (0.19% to 2.9%) [17, 26]. However, larger-scale population-based studies that report data on the prevalence of suicidal behavior are still scarce; there are only four studies among people with dementia and two studies among caregivers. Hence, additional large-scale studies are needed to determine the prevalence of suicidal behavior more reliably among people with dementia and caregivers before a definitive conclusion can be drawn.
Risk factors for suicidal behavior in caregivers of people with dementia
The risk factors for suicidal behavior among caregivers of people with dementia could also be classified into four main themes: high caregiver burden (unemployment, intense caregiving, lower sense of competence and mastery, impaired basic activities of daily living and the presence of BPSD among care receivers) [17, 21, 24, 26]; greater emotional burnout (greater severity of depression and anxiety symptoms, depersonalization leading to greater odds of emotional problems and the use of dysfunctional coping) [17, 20,21,22, 24, 26]; lack of social support (absence of social and family support, lower self-efficacy in seeking assistance from community service, conflict with family or care staff; feeling of loneliness, living without a partner, and issuing with family dynamics) [24, 26]; and history of preexisting illness (preexisting mental illness, mood disorders, and chronic physical illness) [17, 21, 25].
Among these risk factors categories, greater emotional burnout and history of preexisting illness stood out as the commonly identified risk factors of suicidal behavior among caregivers of people with dementia in the selected studies. These two categories of risk factors have also been reported as common risk factors among caregivers of people with dementia in other systematic and scoping reviews [10, 56]. The risk factors of suicidal behavior among caregivers of people with dementia will be discussed in more details later.
Risk factors for suicidal behavior in people with dementia
Similarly, risk factors for suicidal behavior among people with dementia may also be categorized into emotion-related factors (higher severity of depression and anxiety, passive self-harm, presence of comorbid mood disorder, schizophrenia, somatoform disorder or anxiety disorder, history of inpatient psychiatric hospitalization, lower degree of wish to live, greater degree of wish to die, stress and hopelessness, delusional symptoms, previous suicidal attempts, more severe behavioral and psychological syndrome of dementia, and prescription of antidepressant and anxiolytic medication) [19, 31, 34, 37, 38, 45,46,47,48,49,50, 52, 54], dementia-related factors (shortly or within 3 months after diagnosis of dementia, younger age of diagnosis, Alzheimer’s disease alone, better cognitive function, advanced dementia, higher thought and concentration disturbance, worsening of cognitive decline, reduced QoL, mixed Alzheimer’s disease and vascular dementia, antidementia medication prescription, higher daily functioning, recent mild cognitive impairment, comorbid Parkinson’s disease, and moderate dementia) [19, 23, 31, 34, 36, 43, 45, 47,48,49,50, 52, 55], physical health-related factors (history of physical health problem and chronic pain) [52, 55], and psychosocial factors (living in rural areas and substance use) [55].
Among these risk factors categories, emotion and dementia-related factors were identified as the commonly identified risk factors of suicidal behavior among people with dementia in the selected studies. These two categories of risk factors have also been reported as common risk factors among people with dementia in other literature and systematic reviews [11, 57]. The risk factors of suicidal behavior among people with dementia will be discussed in more details later.
Communalities and differences in the risk factors for people with dementia and their caregivers
A few risk factors were identified as risk factors contributing to suicidal behavior in people with dementia and their caregivers, such as greater emotional burnout (presence of and greater severity of depression and anxiety), which was the most commonly reported risk factor; preexisting mental health problems; preexisting physical health conditions; and the presence of or more severe behavioral and psychological symptoms of dementia (BPSD) (Table 2).
In the context of caregivers of people with dementia, the burden of caregiving creates mixed feelings among caregivers, contributing to a dilemma between carrying out the responsibility to provide end-of-life care to the care receiver with dementia and the homicidal thought of death of the care receiver. Hence, to end years of suffering because being bound to the role of a caregiver may subsequently contribute to depression and anxiety and the risk of carrying out suicidal behavior among caregivers of people with dementia [18, 25].
Major depressive disorder and anxiety among elderly people presented with pertinent deficits in processing speed or working memory and executive dysfunction, which may increase the risk of developing Alzheimer’s disease. Moreover, late-stage depression may be linked to hippocampal atrophy and generalized ischemia affecting the frontostriatal region of the brain, contributing to cognitive impairment, which may hasten the development of Alzheimer’s disease. Cognitive impairment in late-life depression could increase the risk of developing suicidal behavior [58]. Hence, these factors may explain how greater severity of depression and anxiety may contribute to higher risk of suicidal behavior among people with dementia.
Essentially, people with dementia and depression who present with passive self-harm would require urgent treatment and care, as they may harbor a high risk of presenting with suicidal behavior. Moreover, self-harm is well recognized as an early warning sign of suicide [59].
Preexisting physical health conditions and preexisting mental health problems were also common risk factors leading to suicidal behavior among caregivers of people with dementia. As anticipated, our findings consistently indicated that the caregiving role could predispose individuals to exacerbation of preexisting physical health and mental health conditions, consequently leading to an increased risk of developing suicidal behavior [23]. Similarly, in people with dementia, the presence of preexisting mental health problems (such as schizophrenia, mood disorders, somatoform disorders, or anxiety disorders) and comorbid physical illnesses (such as diabetes mellitus, cancer, ischemic heart disease, stroke, chronic kidney disease, or Parkinson’s disease) could worsen the risk of suicidal behavior [19, 48]. This should prompt clinicians to carefully screen people with dementia with comorbidities for risk of suicide. However, it remains unclear whether preexisting mental and physical illnesses play a predominant role as risk factors for dementia and suicidal behavior or as mediators in the relationship between dementia and suicidal behavior, or both, which may warrant further investigation.
In addition, greater severity of BPSD also increased the risk of suicidal behavior in people with dementia and their caregivers. Among the common BPSD experienced by people with dementia were agitation and sleep disturbance. Agitation arises when a person with dementia (a care receiver) experiences some unmet needs (such as a lack of attention received from the caregiver and inadequate interaction between the caregiver and the person with dementia), which creates a significant degree of caregiver burden and may ultimately contribute to the risk of suicidal behavior among caregivers. Similarly, sleep disturbance in people with dementia may contribute to or exacerbate sleep deprivation in caregivers, leading to emotional burnout and in turn increasing the risk of suicidal behavior among caregivers [60]. In the context of people with dementia, more severe BPSD may enhance perceived burdensomeness and diminish quality of life, leading them to value their life as less worth living than people with better quality of life [47].
Despite some commonalities in the risk factors contributing to suicidal behavior between people with dementia and their caregivers, there were some notable differences in risk factors between the two groups. Risk factors associated with suicidal behavior among caregivers of people with dementia were both self-related and related to caring for those people with dementia, whereas risk factors in people with dementia were self-related factors and not related to care received from caregivers.
There were several common risk factors that were associated with suicidal behavior only among people with dementia. Intriguingly, shortly after or within 3 months of diagnosis with dementia and young age at diagnosis of dementia (aged 50 to 69 years) were among the most common risk factors associated with suicidal behavior among people with dementia. Basically, individuals who have recently been diagnosed with dementia are still in a state where they have the cognitive capability and functioning to perceive their deficits and are still capable of planning and executing suicidal behaviors [31, 40, 45, 50]. Hence, people recently diagnosed with dementia are at higher risk of exhibiting suicidal behavior. Similarly, people who are diagnosed with dementia at a relatively younger age (50 to 69 years) carry a higher risk of presenting with suicidal behavior, as they may anticipate and must endure worsening and persistent loss of functioning for a long time in relation to their life expectancy, which will hamper their productive years and their responsibility to take care of their family. This experience of perceived burdensomeness leads to a decreased ability to accept and adjust to having to live with dementia, ultimately resulting in suicidal behavior [47]. Our findings also revealed that a history of psychiatric inpatient admission; the presence of Alzheimer’s disease alone; and the presence of passive self-harm, such as refusal to eat, drink and take medication, worsened the mental health of people with dementia and contributed to the development of suicidal behavior. Hence, people with dementia and the above risk factors need to be screened for suicide risk, and special attention is needed from treating clinicians.
In addition, our findings also pinpoint the importance of facilitating caregivers to maintain a sufficient degree of social and family support. Conventionally, social and family support are vital protective factors against depression [61]. The absence of social and family support may worsen depression and increase the risk of developing suicidal behavior among caregivers of people with dementia.
Other notable findings
Most of the selected studies on the suicidal behavior of people with dementia and their caregivers involve a larger proportion of female participants. In the context of gender preponderance, the proportion of female caregivers of people with dementia is greater than that of male caregivers (ratio of 2:1), who are usually spouses or daughters of dementia patients [62]. This explained the larger proportion of female subjects in almost all of our selected studies. Similarly, the larger proportion of female dementia subjects reported in our review also confirmed the finding that females are more prone to dementia, particularly Alzheimer’s disease [63].
Limitations
There were a few limitations to be considered in the selected studies on the suicidal behavior of caregivers of people with dementia. First, most of the selected studies had small sample sizes, except for two studies [17, 26]. Second, most of the selected studies were cross-sectional studies, except for two studies [24, 26]. Hence, causal inference of the risk factors identified for the occurrence of suicidal behavior among caregivers of people with dementia could not be deduced. Third, although there were two selected studies with large sample sizes, these studies were limited by retrospective recall of suicidal behavior, leading to the risk of recall bias, a small number of subjects with suicidal behavior [26], and a lack of diverse demographic backgrounds [18].
Due to the limitations of the selected studies on the suicidal behavior of people with dementia, most of the studies were cross-sectional or case‒control studies, and causal inference of the risk factors for the occurrence of suicidal behavior could not be made. In addition, six selected studies examined the autopsy findings of people with dementia who died due to suicide; these studies involved retrospective history of suicidal behavior and were prone to recall bias. Moreover, more than half of the selected studies recruited subjects from a single center; hence, the findings cannot be generalized to the entire dementia population. Finally, more than half of the studies did not specifically recruit subjects with dementia.
This systematic review has several limitations that must be considered. First, this narrative review did not include research articles, case reports, or case series published in languages other than English. Hence, we may have missed research findings that were reported in other languages. Second, this systematic review did not include preprint versions of the research articles; hence, we may have missed the latest research findings, which were still in the preprint version.
Clinical implications
The findings of this systematic review should alert clinicians to pay special attention to screening caregivers of people with dementia who may be at high risk of developing suicidal behavior, such as those with greater severity of depression and anxiety, preexisting physical health and mental health conditions, and poor social and family support. Similarly, treating clinicians should be prepared to screen people with dementia for suicide risk, particularly those with more severe depression and anxiety, especially those with passive self-harm; those diagnosed with dementia within 3 months; especially those with better cognitive function; younger patients diagnosed with dementia (with age 50 to 69 years); and those with comorbid mental illness and a history of inpatient psychiatric hospitalization. Hence, people with dementia and their caregivers with a high risk of suicide should receive cognitive-focused control intervention and interpersonal psychotherapy to alleviate their risk of suicide [63, 64].
However, it remains inconclusive whether the specific cause of dementia could increase the risk of suicidal behavior among people with dementia, as the presence of Alzheimer’s disease alone and having a mixed diagnosis of both Alzheimer’s disease and vascular dementia have been reported to increase the risk of suicidal behavior. In addition, the selected studies in this review did not mention which types of suicidal behavior are more common among caregivers and people with dementia. These research gaps should be explored further in future studies.
Conclusions
This systematic review pinpointed the definitive risk of suicidal behavior as a consequence of the caregiving role of caregivers of people with dementia, while the risk of suicidal behavior among people with dementia still remains inconclusive. Large population-based studies have revealed that the prevalence of suicidal behavior among people with dementia is greater than that among caregivers. There were a few risk factors that were associated with suicidal behavior in people with dementia and their caregivers, such as the presence and greater severity of depression and anxiety, preexisting mental illness and physical illness, and greater severity of BPSD among people with dementia. Hence, treating clinicians should carefully manage these risk factors to safeguard the mental health of people with dementia and their caregivers. We also recommend that clinicians conduct early suicide risk screening among people with dementia during the early phase of dementia, as intact cognitive function, complex acts and planning may increase the risk of suicidal behavior. Despite the potential implications of our review findings, the overall risk of bias of the majority of the selected studies was unclear, as a larger proportion of the selected studies had a high risk of bias due to inadequate selection of participants and inadequate consideration of confounding variables. These methodological limitations warrant improvement in future studies to confirm the findings in this review.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
- RoBANS:
-
Risk of Bias Assessment Tool for Non-randomized Studies
- BPSD:
-
Behavioral and psychological symptoms of dementia
- bvFTD:
-
Behavioral variant of frontotemporal dementia
- ADAD:
-
Autosomal dominant Alzheimer’s disease
References
Centre for Disease Control and Prevention. Facts about suicide. 2023. https://www.cdc.gov/suicide/facts/index.html. Accessed 4 Nov 2023.
World Health Organization. Suicide. 2021. https://www.who.int/news-room/fact-sheets/detail/suicide. Accessed 27 Apr 2023.
Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and suicidal behavior. Epidemiol Rev. 2008;30:133–54.
Alzheimer’s Disease International. Dementia statistics. https://www.alzint.org/about/dementia-facts-figures/dementia-statistics/. Accessed 4 Nov 2023.
World Health Organization. Global action plan on the public health response to dementia 2017–2025. Geneva: World Health Organization; 2017.
Shah H, Albanese E, Duggan C, Rudan I, Langa KM, Carrillo MC, et al. Research priorities to reduce the global burden of dementia by 2025. Lancet Neurol. 2016;15:1285–94.
Livingston G, Sommerlad A, Orgeta V, Costafreda SG, Huntley J, Ames D, et al. Dementia prevention, intervention, and care. Lancet. 2017;390:2673–734.
Koyama A, Matsushita M, Hashimoto M, Fujise N, Ishikawa T, Tanaka H, et al. Mental health among younger and older caregivers of dementia patients. Psychogeriatrics. 2017;17:108–14.
Puga F, Wang D, Rafford M, Poe A, Pickering CEZ. The relationship between daily stressors, social support, depression and anxiety among dementia family caregivers: a micro-longitudinal study. Aging Ment Health. 2022;29:1–9.
Solimando L, Fasulo M, Cavallero S, Veronese N, Smith L, Vernuccio L, et al. Suicide risk in caregivers of people with dementia: a systematic review and meta-analysis. Aging Clin Exp Res. 2022;34:2255–60.
Álvarez Muñoz FJ, Rubio-Aparicio M, Gurillo Muñoz P, García Herrero AM, Sánchez-Meca J, Navarro-Mateu F. Suicide and dementia: systematic review and meta-analysis. Rev Psiquiatr Salud Ment (Engl Ed). 2020;13:213–27. English, Spanish.
Kong JW, Park JY. Understanding suicide risk in people with dementia and family caregivers in South Korea: a systematic review. Behav Sci (Basel). 2022;12:97.
Isik AT, Soysal P, Solmi M, Veronese N. Bidirectional relationship between caregiver burden and neuropsychiatric symptoms in patients with Alzheimer’s disease: a narrative review. Int J Geriatr Psychiatry. 2019;34:1326–34.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Stoll CRT, Izadi S, Fowler S, Green P, Suls J, Colditz GA. The value of a second reviewer for study selection in systematic review. Res Synth Methods. 2019;19:539–45.
Park J, Lee Y, Seo H, Jang B, Son H, Kim S, Shin S, Hahn S. Risk of Bias Assessment tool for Non-randomized Studies (RoBANS): development and validation of a new instrument. In: Abstracts of the 19th Cochrane Colloquium; 2011 19–22 Oct. Madrid: Wiley; 2011.
Valente LE, Truzzi A, Souza WF, Alves GS, Alves CE, Sudo FK, et al. Health self-perception by dementia family caregivers: sociodemographic and clinical factors. Arq Neuropsiquiatr. 2011;69:739–44.
Lewis LF. Caregiving for a loved one with dementia at the end of life: an emergent theory of rediscovering. Am J Alzheimers Dis Other Demen. 2015;30:488–96.
Choi JW, Lee KS, Han E. Suicide risk within 1 year of dementia diagnosis in older adults: a nationwide retrospective cohort study. J Psychiatry Neurosci. 2021;46:E119–27.
Hosaka T, Sugiyama Y. Structured intervention in family caregivers of the demented elderly and changes in their immune function. Psychiatry Clin Neurosci. 2003;57:147–51.
Shaji KS, Smitha K, Lal KP, Prince MJ. Caregivers of people with Alzheimer’s disease: a qualitative study from the Indian 10/66 Dementia Research Network. Int J Geriatr Psychiatry. 2003;18:1–6.
O’Dwyer S, Moyle W, van Wyk S. Suicidal ideation and resilience in family carers of people with dementia: a pilot qualitative study. Aging Ment Health. 2012;17:753–60.
O’Dwyer ST, Moyle W, Zimmer-Gembeck M, De Leo D. Suicidal ideation in family carers of people with dementia: a pilot study. Int J Geriatr Psychiatry. 2013;28:1182–8.
Joling KJ, O’Dwyer ST, Hertogh CMPM, van Hout HPJ. The occurrence and persistence of thoughts of suicide, self-harm and death in family caregivers of people with dementia: a longitudinal data analysis over 2 years. Int J Geriatr Psychiatry. 2018;33:263–70.
Anderson JG, Eppes A, O’Dwyer ST. “Like death is near”: expressions of suicidal and homicidal ideation in the blog posts of family caregivers of people with dementia. Behav Sci (Basel). 2019;9:22.
Joling KJ, Ten Have M, de Graaf R, O’Dwyer ST. Risk factors for suicidal thoughts in informal caregivers: results from the population-based Netherlands mental health survey and incidence Study-2 (NEMESIS-2). BMC Psychiatry. 2019;19:320.
Kim HJ, Kehoe P, Gibbs LM, Lee JA. Caregiving experience of dementia among korean american family caregivers. Issues Ment Health Nurs. 2019;40:158–65.
Rosato M, Tseliou F, Wright DM, Maguire A, O’Reilly D. Are volunteering and caregiving associated with suicide risk? A census-based longitudinal study. BMC Psychiatry. 2019;19:296.
Lyness JM, Conwell Y, Nelson JC. Suicide attempts in elderly psychiatric inpatients. J Am Geriatr Soc. 1992;40:320–4.
Florio ER, Hendryx MS, Jensen JE, Rockwood TH, Raschko R, Dyck DG. A comparison of suicidal and nonsuicidal elders referred to a community mental health center program. Suicide Life Threat Behav. 1997;27:182–93.
Rao R, Dening T, Brayne C, Huppert FA. Suicidal thinking in community residents over eighty. Int J Geriatr Psychiatry. 1997;12:337–43.
Rubio A, Vestner AL, Stewart JM, Forbes NT, Conwell Y, Cox C. Suicide and Alzheimer’s pathology in the elderly: a case-control study. Biol Psychiatry. 2001;49:137–45.
Draper B, Brodaty H, Low LF, Richards V. Prediction of mortality in nursing home residents: impact of passive self-harm behaviors. Int Psychogeriatr. 2003;15:187–96.
Heun R, Kockler M, Ptok U. Lifetime symptoms of depression in Alzheimer’s disease. Eur Psychiatry. 2003;18:63–9.
Peisah C, Snowdon J, Gorrie C, Kril J, Rodriguez M. Investigation of Alzheimer’s disease-related pathology in community dwelling older subjects who committed suicide. J Affect Disord. 2007;99:127–32.
Erlangsen A, Zarit SH, Conwell Y. Hospital-diagnosed dementia and suicide: a longitudinal study using prospective, nationwide register data. Am J Geriatr Psychiatry. 2008;16:220–8.
Purandare N, Voshaar RC, Rodway C, Bickley H, Burns A, Kapur N. Suicide in dementia: 9-year national clinical survey in England and Wales. Br J Psychiatry. 2009;194:175–80.
Qin P. The impact of psychiatric illness on suicide: differences by diagnosis of disorders and by sex and age of subjects. J Psychiatr Res. 2011;45:1445–52.
McCarthy JF, Szymanski BR, Karlin BE, Katz IR. Suicide mortality following nursing home discharge in the Department of Veterans Affairs health system. Am J Public Health. 2013;103:2261–6.
Borges G, Acosta I, Sosa AL. Suicide ideation, dementia and mental disorders among a community sample of older people in Mexico. Int J Geriatr Psychiatry. 2015;30:247–55.
Randall JR, Walld R, Finlayson G, Sareen J, Martens PJ, Bolton JM. Acute risk of suicide and suicide attempts associated with recent diagnosis of mental disorders: a population-based, propensity score-matched analysis. Can J Psychiatry. 2014;59:531–8.
Nishida N, Hata Y, Yoshida K, Kinoshita K. Neuropathologic features of suicide victims who presented with acute poststroke depression: significance of association with neurodegenerative disorders. J Neuropathol Exp Neurol. 2015;74:401–10.
Matschke J, Sehner S, Gallinat J, Siegers J, Murroni M, Püschel K, et al. No difference in the prevalence of Alzheimer-type neurodegenerative changes in the brains of suicides when compared with controls: an explorative neuropathologic study. Eur Arch Psychiatry Clin Neurosci. 2018;268:509–17.
Morgan C, Webb RT, Carr MJ, Kontopantelis E, Chew-Graham CA, Kapur N, Ashcroft DM. Self-harm in a primary care cohort of older people: incidence, clinical management, and risk of suicide and other causes of death. Lancet Psychiatry. 2018;5:905–12.
Zucca M, Rubino E, Vacca A, Govone F, Gai A, De Martino P, et al. High risk of suicide in behavioral variant frontotemporal dementia. Am J Alzheimers Dis Other Demen. 2019;34:265–71.
Ng KP, Richard-Devantoy S, Bertrand JA, Jiang L, Pascoal TA, Mathotaarachchi S, et al. Suicidal ideation is common in autosomal dominant Alzheimer’s disease at-risk persons. Int J Geriatr Psychiatry. 2020;35:60–8.
Ortner M, Riedl L, Jox RJ, Hartmann J, Roßmeier C, Dorn B, et al. Suicidal ideations and behavior in patients with young and late onset dementia. Front Neurol. 2021;12:647396.
Alothman D, Card T, Lewis S, Tyrrell E, Fogarty AW, Marshall CR. Risk of suicide after dementia diagnosis. JAMA Neurol. 2022;79:1148–54.
Barak Y, Aizenberg D. Suicide amongst Alzheimer’s disease patients: a 10-year survey. Dement Geriatr Cogn Disord. 2002;14:101–3.
Seyfried LS, Kales HC, Ignacio RV, Conwell Y, Valenstein M. Predictors of suicide in patients with dementia. Alzheimers Dement. 2011;7:567–73.
Tu YA, Chen MH, Tsai CF, Su TP, Bai YM, Li CT, et al. Geriatric suicide attempt and risk of subsequent dementia: a nationwide longitudinal follow-up study in Taiwan. Am J Geriatr Psychiatry. 2016;24:1211–8.
Annor FB, Bayakly RA, Morrison RA, Bryan MJ, Gilbert LK, Ivey-Stephenson AZ, et al. Suicide among persons with dementia, Georgia, 2013 to 2016. J Geriatr Psychiatry Neurol. 2019;32:31–9.
Günak MM, Barnes DE, Yaffe K, Li Y, Byers AL. Risk of suicide attempt in patients with recent diagnosis of mild cognitive impairment or dementia. JAMA Psychiat. 2021;78:659–66.
Holmstrand C, Rahm Hallberg I, Saks K, Leino-Kilpi H, Renom Guiteras A, Verbeek H, et al. Associated factors of suicidal ideation among older persons with dementia living at home in eight European countries. Aging Ment Health. 2021;25:1730–9.
Schmutte T, Olfson M, Maust DT, Xie M, Marcus SC. Suicide risk in first year after dementia diagnosis in older adults. Alzheimers Dement. 2022;18:262–71.
O’Dwyer ST, Janssens A, Sansom A, Biddle L, Mars B, Slater T, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261.
Kułak-Bejda A, Bejda G, Waszkiewicz N. Mental disorders, cognitive impairment and the risk of suicide in older adults. Front Psychiatry. 2021;12:695286.
Knipe D, Padmanathan P, Newton-Howes G, Chan LF, Kapur N. Suicide and self-harm. Lancet. 2022;399:1903–16.
Lu X, Ye R, Wu J, Rao D, Liao X. Comparing behavioral and psychological symptoms of dementia and caregiver distress caused between older adults with dementia living in the community and in nursing homes. Front Psychiatry. 2022;13:881215.
Wickramaratne PJ, Yangchen T, Lepow L, Patra BG, Glicksburg B, Talati A, et al. Social connectedness as a determinant of mental health: a scoping review. PLoS One. 2022;17:e0275004.
Center for Disease Control and Prevention. Caregiving for a person with Alzheimer’s disease or a related dementia. 2019. https://www.cdc.gov/aging/caregiving/alzheimer.htm. Accessed 26 Apr 2023.
Beam CR, Kaneshiro C, Jang JY, Reynolds CA, Pedersen NL, Gatz M. Differences between women and men in incidence rates of dementia and Alzheimer’s disease. J Alzheimers Dis. 2018;64:1077–83.
Celano CM, Beale EE, Mastromauro CA, Stewart JG, Millstein RA, Auerbach RP, et al. Psychological interventions to reduce suicidality in high-risk patients with major depression: a randomized controlled trial. Psychol Med. 2017;47:810–21.
van Bentum JS, van Bronswijk SC, Sijbrandij M, Lemmens LHJM, Peeters FFPML, Drukker M, et al. Cognitive therapy and interpersonal psychotherapy reduce suicidal ideation independent from their effect on depression. Depress Anxiety. 2021;38:940–9.
Acknowledgements
Not applicable.
Funding
This study was funded by the Fundamental Research Grant Scheme of Ministry of Higher Education of Malaysia (code: FRGS/1/2022/SSI13/USM/02/2) and the Research University TopDown Grant (RU TopDown) from Universiti Sains Malaysia (grant number: 1001/CIPPT/8070034, URL = https://research.usm.my/) based on research program (Dementia Multidisciplinary Research Program of IPPT). The funders play no role in the design of the study and collection, analysis, interpretation of data and in writing the manuscript, and submission for publication.
Author information
Authors and Affiliations
Contributions
M.F.I.L.B.A conceptualized the review. M.F.I.L.B.A, N.I.S, and M.A.M involved in literature search and selection of articles for review. M.F.I.L.B.A, N.I.S, and M.A.M reviewed the selected articles. M.F.I.L.B.A wrote the first draft of the manuscript. M.F.I.L.B.A, N.I.S, and M.A.M revised the draft and approved the manuscript for submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mohamad, M.A., Leong Bin Abdullah, M.F.I. & Shari, N.I. Similarities and differences in the prevalence and risk factors of suicidal behavior between caregivers and people with dementia: a systematic review. BMC Geriatr 24, 254 (2024). https://doi.org/10.1186/s12877-024-04753-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-024-04753-4