
Abstract
Background
Population aging has increased the prevalence of multimorbidity, jeopardizing the sustainability and efficiency of healthcare systems. This study aimed to evaluate the effects of an integrated ambulatory care program (IACP) on healthcare utilization and costs among older patients with multimorbidity while accounting for the confounding effects of frailty.
Methods
A retrospective cohort study using propensity matching including patients aged 65 or older with two or more chronic conditions attending the outpatient clinic at our hospital between June 1 and December 31, 2019, was conducted. Exposure was defined as receipt of IACP care. Patients not undergoing the IACP comprised the unexposed group and were matched at a ratio of 1:4 to patients undergoing the IACP group according to sex, age, Charlson Comorbidity Index score, multimorbidity frailty index score, and number of outpatient visits within 6 months before the index date. Outcomes were changes in healthcare utilization and related costs between 6 months before and after receiving IACP care. Multivariate regression analyses were used for data analysis and the Generalized Estimation Equation method was used to fit the regression models.
Results
A total of 166 (IACP) and 664 (non-exposed) patients were analyzed. The mean participant baseline ages were 77.15 ± 7.77 (IACP) and 77.28 ± 7.90 years (unexposed). In univariate analyses, the IACP group demonstrated greater reductions than the unexposed group in the frequency of outpatient visits (-3.16 vs. -1.36, p < 0.001), number of physicians visited (-0.99 vs. -0.17, p < 0.001), diagnostic fees (-1300 New Taiwan Dollar [NTD] vs. -520 NTD, p < 0.001), drug prescription fees (-250 NTD vs. -70 NTD, p < 0.001), and examination fees (-1620 NTD vs. -700 NTD, p = 0.014). Multivariate analyses demonstrated that patients in the IACP group experienced significant reduction in the frequency of outpatient visits (95% CI: -0.357 to -0.181, p < 0.001), number of physicians visited (95% CI: -0.334 to -0.199, p < 0.001), and overall outpatient costs (95% CI: -0.082 to -0.011, p = 0.01). However, emergency department utilization, hospitalization, and costs did not differ significantly.
Conclusions
Expanding IACPs may help patients with multimorbidity reduce their use of outpatient clinics at the 6-month follow-up, reduce care fragmentation, and promote sustainability of the healthcare system.
Similar content being viewed by others


Background
Progress in public health and demographic changes are causing a shift in the burden of disease towards chronic noncommunicable diseases, which pose considerable challenges for healthcare systems. According to the World Health Organization (WHO), the global population aged > 60 years will increase to two billion by 2050, and the prevalence of chronic noncommunicable diseases may increase thereafter, particularly among older adults [1]. Multimorbidity, defined as the presence of two or more chronic diseases in the same individual, is associated with complex care needs and leads to increased utilization of healthcare services [2]. Knickman et al. reported that 85% of all healthcare resources are utilized by patients with at least one chronic disease and 65% are spent on patients with multimorbidity [3]. Despite the fact that management of multimorbidity exhausts most healthcare resources, health outcomes are suboptimal [4, 5]. There is an increasing concern that the highly specialized modern medical science and evidence-based guidelines tend to focus on single conditions; however, this approach fails to meet the growing needs of patients with multimorbidity and leads to fragmented medical care that is potentially harmful and duplicated services [6, 7].
According to a systematic review by Desmedt et al., integrated care has received increasing attention because it is considered effective in reducing fragmented services, improving the quality and continuity of care, and controlling healthcare expenditures [8]. According to the WHO integrated care encompasses a wide spectrum of delivery, management, and organizational health services related to health promotion, disease prevention, diagnosis, treatment, disease management, rehabilitation, and palliative care [9]. Integration aims to ensure that people receive a continuum of care at different levels and sites within the health system according to their needs throughout their life course. It also facilitates improvement in patient experiences through care coordination [10].
Although there is a widespread belief that integrated care can control or reduce healthcare utilization and related costs, relatively few studies have evaluated the economic impact of integrated care approaches [8, 11,12,13,14]. Earlier studies suggested that integrated care is cost-effective [13] and is likely to reduce costs and improve healthcare outcomes [12]. However, a recent systematic review of randomized clinical trials assessing the effectiveness of integrated models for older patients with chronic diseases in 2022 found that interventions implemented in the models are varied, and it was not possible to determine a single care model as effective [11]. The present body of literature is inconclusive regarding the potential economic impact of integrated care. However, most economic outcomes focus on hospital utilization, including (re)admission rates and emergency visits [13]. There is a scarcity of robust evidence on the economic impact of integrated care on the utilization of outpatient services.
Asia is experiencing a rapidly aging population. In addition to Japan, which has the world’s leading life expectancy and percentage of older people, many Asian countries are experiencing faster demographic changes than European and North American countries, and healthcare expenditures have increased substantially [15]. Therefore, Asia faces the double burden of multimorbidity and the risk of financial sustainability of the healthcare system as many countries provide universal health coverage [16]. For example, a study in Beijing, China, showed that the medical costs of patients with multimorbidity were 3.4 to 5.3 times higher than those with only one chronic condition [17]. Nevertheless, little is known about the impact of integrated care, particularly outpatient-based interventions, on healthcare utilization and costs among older patients with multimorbidity in Asian countries. In four recent systematic reviews on the effectiveness of integrated care models that included 252 studies [8, 11, 12, 14] only two were conducted in Asia [18, 19]. Lin et al. identified 23 integrated care programs in 7 Asian countries; however, only one examined outpatient attendance changes, and only four examined cost changes, indicating that more research is needed for the development of integrated care programs [20].
Moreover, to date, no previous study has considered the confounding effects of frailty on healthcare utilization and costs in relation to integrated care among older adults. Frail older adults are susceptible to adverse health outcomes, including falls, delirium, disability, hospitalization, and mortality, thereby increasing their healthcare utilization [21]. Li et al. demonstrated the significant impact of frailty status on outpatient visits and medical expenditures [22]. To improve research validity and minimize bias, it is essential to collect information on frailty status and effectively manage confounding effects on economic outcomes through proper study design and statistical analyses.
To bridge this knowledge gap, we evaluated the impact of an integrated ambulatory care program (IACP) on healthcare utilization and cost-related outcomes among older adults with multimorbidity at a university hospital in Taiwan.
Methods
Study design
This retrospective cohort study was conducted at a 1,193-bed university hospital in Taiwan. This study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology statement [23] (Supplementary Table 1).
Data source
The dataset for this study was extracted from hospital medical records by hospital information technologists.
The integrated ambulatory care program
The IACP in the study hospital was developed and has been offered to patients with multimorbidity since July 1, 2019, to reduce unnecessary utilization of healthcare resources and negative health outcomes. The program was partially supported by the Taiwan National Health Insurance (NHI) [24]. Patients voluntarily participated in the program, and written informed consent was obtained before attending the program. The program involves multidisciplinary teamwork, comprehensive functional assessments, medication reviews, and case management. The multidisciplinary team that implemented the program consisted of case managers, physicians trained as integrated care specialists, and pharmacists. During the first service session, the case manager comprehensively assessed physical, cognitive, nutritional, and mood functions. The comprehensive assessment evaluated the activities of daily living, according to the Barthel Index [25]; cognitive function, according to the Short Portable Mental Status Questionnaire (SPMSQ) [26]; frailty, according to the Clinical Frailty Scale (CFS) [27]; mood, according to the five-item Geriatric Depression Scale (GDS-5) [28]; and nutritional status, according to the Mini Nutritional Assessment–Short Form (MNA-SF) [29]. A pharmacist reviewed the medication regimens of patients. Information on each medication regimen was retrieved from the NHI MediCloud system of Taiwan, which allows medical professionals to access prescription records provided by various hospitals and clinics [30]. The case manager and pharmacist then provided feedback to the physician responsible for the integration. The physician then created a care plan according to the medical condition and preferences of the patient, and the recommendations of the multidisciplinary team. After the initial service session, the patients were followed-up on two occasions by case managers to ensure that no major adverse responses required further evaluation or intervention.
Study setting and participants
The study included patients who visited the internal, geriatric, or family medicine outpatient clinic at our hospital between June 1 and December 31, 2019. The index date was defined as the date of the first outpatient visit.
Inclusion criteria were as follows: (1) age 65 years or older, (2) more than two chronic conditions, (3) use of more than five medications for chronic disease management, and (4) consultation with more than two physicians for chronic disease management. Patients aged 65 years or older were selected because the pharmacists applied the latest version of the Beers Criteria to identify potentially inappropriate medication and these criteria only apply to patients aged 65 years or older [31]. Patients with more than two chronic conditions were included to meet the criteria for multimorbidity [2]. Patients undergoing treatment with more than five medications were included according to the most commonly reported definition of polypharmacy [32] To evaluate the effectiveness of the complete process of the IACP and to compare healthcare utilization and costs for 6 months before and 6 months after the program, we excluded the following: (1) patients undergoing active cancer treatment (chemotherapy, radiation therapy, and target therapy); (2) patients undergoing clinical trials; (3) patients with no outpatient utilization at the study hospital at 6 months after the index date; (4) patients who died within 6 months after the index date; (5) patients extreme medical costs; (6) patients lost to follow-up after the index date (6) received the program during the outcome evaluation period (between January 1 and June 30, 2020).
Exposed and unexposed group
Exposure was defined as receiving care under the IACP between June 1 and December 31, 2019. Patients in the unexposed group included those who were not in the IACP and were matched using a propensity score matching algorithm at a ratio of 1:4 to those in the IACP group using five variables: sex, age, Charlson Comorbidity Index (CCI) score [33], multimorbidity Frailty Index (mFI) score [34], and number of outpatient visits within 6 months before the index date. The matching was processed using a greedy nearest neighbor algorithm with a caliper of 0.2 times the standard deviation of the logit of the propensity score, with a random matching order and without replacement.
Outcomes
The primary outcomes were changes in outpatient service utilization, including the number of outpatient clinic visits, number of physicians visited, and outpatient service costs between 6 months before and 6 months after the commencement of the program. We measured the overall costs of the outpatient services and subsidiaries, including diagnostics, drugs, prescription services, treatment, and examination fees.
Secondary outcomes included changes in the number of emergency department (ED) visits, hospitalizations, length of hospitalization (days), costs of ED visits, and costs of hospitalizations between 6 months before and 6 months after the commencement of the program. We measured only the overall costs of ED visits and hospitalizations.
Taiwan’s NHI system has adopted a single-payer system that primarily uses fee-for-service payments for medical services, examinations, and medications [35]. This study measured reimbursement payments from the NHI for general diagnoses and treatment, medical consultations and operations, and related expenses. We did not include out-of-pocket fees in this study.
Baseline characteristics and covariates
Baseline data on demographic characteristics, namely age, sex, and place of residence, were collected upon the inclusion of participants (index date). Furthermore, clinical data, including body mass index (BMI), CCI scores for comorbidity status [33], number of chronic disease diagnoses, and mFI score for frailty status [35]. Potential covariates included age, sex, distance between home and hospital, comorbidities, frailty status, number of chronic diseases, and baseline use of outpatient services. The distance between home and hospital was categorized according to whether the distance required more than 30 min of driving by car (yes or no).
Statistical analysis
Continuous variables are presented as means with standard deviations, and categorical variables are expressed as counts with percentages. Comparisons of variables between the exposed and unexposed groups were performed using the chi-square test or Fisher’s exact test for categorical variables and the 2-sample t-test or Mann–Whitney U test for continuous variables. Univariate analysis of the outcomes between 6 months before IACP and 6 months after IACP or without IACP was performed using paired t-tests.
To adjust for the potential confounding effect of covariates and assess the independent effect of IACP on outcomes, we used (1) multivariate Poisson regression analyses for the number of outpatient visits, number of physicians visited, and length of hospital stay; (2) multivariate linear regression analyses for the costs of outpatient services, ED visits, and hospitalizations; and (3) negative binominal regression analyses for the number of ED visits and hospitalizations. In addition, to account for the intercorrelations of data collected from exposed and unexposed participants 6 months before and 6 months after the index date, we used a Generalized Estimation Equation (GEE) to fit the Poisson, linear, and negative binomial regression models. Medical costs in New Taiwan dollars (NTD) were expressed after the logarithmic transformation of the original values in the multivariate analyses.
All the tests were two-tailed. Statistical significance was defined as p < 0.05. All statistical analyses were performed using SAS software (version 9.4; SAS Inc., Cary, N.C., USA).
Ethical approval
The study protocol was approved by the Institutional Review Board of the National Cheng Kung University Hospital (A-ER-109-311).
Results
Characteristics of the study population
From June 1 to December 31, 2019, 194 patients participated in the IACP and 2,098 did not participate in the IACP. Following the application of the exclusion criteria, 167 older patients were included in the IACP group and 1,830 in the unexposed group. Each IACP participant was matched 1:4 ratio to the unexposed group. No match was obtained for one patient in the IACP group, who was excluded. A total of 830 patients were enrolled in the final analysis: 166 in the IACP and 664 patients in the unexposed group. The mean age was 77.25 ± 7.87 years, and 48.3% were male. The patients presented a high degree of comorbidity (mean CCI:3.70 SD:2.32) and mild frailty (mean mFI:0.10, SD:0.06). A flowchart of the patient selection process is shown in Fig. 1.

Patient selection flowchart
Initially, 16 patients participated in the IACP; however, they were lost to follow-up and were excluded. A comparison of the demographic characteristics and clinical conditions of the IACP participants included in the study and those lost to follow-up is presented in Supplementary Table 2. The analysis revealed no significant differences in demographic characteristics or clinical conditions between the participants included in the study and those lost to follow-up.
A comparison of the demographic characteristics and clinical conditions between the exposed and unexposed groups is presented in Table 1. Compared with the unexposed group, the IACP group had a significantly higher percentage of patients with diabetes (52.4% vs. 38%, p = 0.001) and a lower percentage of patients with chronic pulmonary diseases (13.3% vs. 22.7%, p = 0.008). No significant differences in the other variables were observed between the IACP and unexposed groups.
Impact of the integrated ambulatory care program
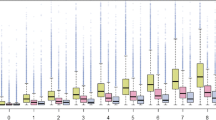
The results of the univariate analysis of the outcome differences between 6 months before and 6 months with or without IACP are presented in Table 2; Fig. 2. Compared with the unexposed group, the IACP group experienced significant reductions in the frequency of outpatient visits (-3.16 vs. -1.36, p < 0.001) and the number of physicians visited (-0.99 vs. -0.17, p < 0.001). Reductions in the frequency of ED visits, hospitalizations, length of hospital stay, overall outpatient and ED care costs were also observed; however, these effects were not significant. Despite no significant reduction in the overall outpatient costs, the IACP group showed significant reductions in diagnostic costs, drug prescriptions, and examination fees. In contrast, hospitalization costs increased 6 months after the index date in both the IACP and unexposed groups; however, the differences were not significant between the two groups. The results of the multivariate analyses using regression models with the GEE method are presented in Table 3. After controlling for several confounding variables, patients in the IACP group experienced significant reduction in frequencies of outpatient visits (β=-0.269, 95% CI: -0.357 to -0.181, p < 0.001), number of physicians visited (β=-0.266, 95% CI: -0.334 to -0.199, p < 0.001), and overall outpatient costs (β=-0.046, 95% CI: -0.082 to -0.011, p = 0.01). Although reductions in the frequency of ED visits, length of hospital stay, and overall ED care costs were observed, these differences were not significant. The frequency and cost of hospitalization tended to increase 6 months after the index date in the IACP group, but no significant effects were found.

Univariate paired t-test results for outcome variables
Discussion
This study presents empirical results on the impact of implementing the IACP in Taiwan, including results on healthcare use, particularly outpatient attendance, and costs among older adults with multimorbidity. Our results showed that at the 6-month follow-up, program participants had a significant decrease in the frequency of outpatient visits, the number of doctors visited, and the overall cost of outpatient services. Therefore, the IACP may improve fragmented care and economic sustainability in outpatient settings for older patients with multimorbidity.
Excessive outpatient clinic visits among patients with multimorbidity is a major problem in Taiwan. Although most healthcare services are covered by the NHI, high accessibility, low co-payment, and fee-for-service payment schemes result in high healthcare service utilization and disjointed care [36]. On average, older adults in Taiwan attend outpatient services nearly 30 times per year [37]. Therefore, since 2019, the NHI has encouraged and supported hospitals in establishing integrated ambulatory care services [24]. To the best of our knowledge, this is the first cohort study to explore the economic impact of an IACP in Taiwan.
Our finding that the number of outpatient clinic visits by IACP participants was reduced by 3.16 in 6 months suggests that the program may reduce the unnecessary use of outpatient services. Previous studies have demonstrated a similar effect of integrated care programs. Leung et al. demonstrated that case management in a randomized controlled trial reduced outpatient attendance [38]. In a UK study, Goldzahl et al. evaluated the effect of multi-disciplinary group meetings for the discussion of high-risk older patients on healthcare utilization, and found that an integrated care intervention reduced the probability of visiting primary care nurses [39]. Case management and multi-disciplinary teamwork are important components of the program.
Multivariate analysis revealed that the IACP participants exhibited a significant decrease in the overall cost of outpatient services during the 6-month follow-up period. However, our study did not measure the costs associated with out-of-pocket payments, transportation, forgone earnings, productivity losses resulting from treatment, or time spent during informal caregiving. Considering the reduction in 3.16 outpatient clinic visits observed 6 months after starting the program, it is likely that costs related to transportation, earnings forgone, productivity losses, and time during informal caregiving were also saved after the program.
Wei et al. reported that an integrated geriatric outpatient clinic reduced the annual costs of outpatient care and hospitalization by the time of the 1- and 2-year follow-up. Although our findings are consistent with those reported by Wei et al. on the reduction of outpatient care costs, hospitalization costs were not reduced at the 6-month follow-up in our study. Ye et al. examined the effectiveness of a pilot integrated care model (Louhu) among older Chinese adults and found no impact on hospitalization costs at 1 year [40]. An explanation could be that the average number of hospitalizations among the participants in our study was less than 0.4 in 6 months. Therefore, our study may have been underpowered to determine this outcome. Further research with a larger sample size or participants with a higher risk of admission (e.g., participants recently discharged from the hospital) is required to determine the effect of the program on the prevalence of hospitalization among older patients with multimorbidity.
The three aims of integrated care are to improve health and quality of care and reduce costs [12]. However, despite the increasing attention that integrated care has received, evidence indicates that reported programs are heterogeneous, and there is currently no universally accepted single best practice model or set of guidelines for implementing integrated care. Our study focused on older patients with multimorbidity, a group that experienced the detrimental effects of a fragmented healthcare system. This group has the greatest potential for improvement in terms of quality, cost-effectiveness, and efficiency.
Limitations and strengths
This study has several limitations, indicating the need for caution when interpreting the findings. First, our study is susceptible to selection bias because we excluded patients who died or were lost to follow-up. Despite the efforts of our case managers to contact participants who refused further follow-up and suggested rescheduling appointments, the patients still preferred to forego further services. Nevertheless, there were no significant differences in the demographic characteristics and clinical conditions between patients included in the study and those lost to follow-up. Second, we did not consider healthcare use at other medical facilities because we could only access the medical records at the study hospital. Third, this study involved patients from a single university hospital, and our findings may not be generalizable to patients receiving health services at other institutions. Fourth, the cohort study design made it impossible to create a comparable unexposed group; therefore, residual confounding and confounding by indication might have affected the interpretation of the results. However, we addressed this problem in both the study design and data analysis stages by adopting propensity score matching and the GEE method with regression models. Propensity score matching was used to eliminate confounding factors due to the measured covariates, particularly the effect of frailty status. Furthermore, we measured various covariates that were not considered in previous studies, such as frailty status, distance from home to the hospital, and baseline healthcare utilization. Our outcomes were repeatedly measured 6 months before and 6 months after the index date in both groups; therefore, the data were highly correlated. Using GEE methods with regression models helps improve the validity and precision of data analyses [41]. Finally, the retrospective data did not cover changes in the participant function or patient-related outcome measures, which are helpful in conducting different economic evaluations, such as cost-utility or cost-benefit studies, and strengthen the value of the study.
Despite these limitations, the strengths of this study include the evaluation of economic outcomes, which are lacking in the current literature. The positive results obtained in this study can serve as a reference for other Asian countries wishing to develop integrated care for older adults with multimorbidity, and are therefore directly relevant to program managers and healthcare professionals. Our results can serve as a reference for future studies aimed at elucidating the influence of outpatient-based integrated care interventions on the economic outcomes of older patients with multimorbidity. From a public health efficiency perspective, integrated care programs may serve as a promising solution to address the fragmentation and growing healthcare expenditures related to population aging.
Conclusions
Population aging has increased the prevalence of multimorbidity, jeopardizing the sustainability and efficiency of healthcare systems. Hospital-based multidisciplinary IACP reduced outpatient visit frequency, physician visits, and outpatient service costs among older patients with multimorbidity at the 6-month follow-up. Integrated care may reduce care fragmentation and promote sustainability of healthcare systems. However, future efforts should be made to develop integrated care models in various settings and assess their cost-effectiveness of integrated care.
Data availability
Data and resources were shared with eligible researchers through established academic channels. The datasets used in this study are available from the corresponding authors upon request.
Abbreviations
- WHO:
-
World Health Organization
- IACP:
-
Integrated ambulatory care program
- TIDieR:
-
Template for Intervention Description and Replication
- NHI:
-
National Health Insurance
- CCI:
-
Charlson Comorbidity Index
- mFI:
-
Multimorbidity Frailty Index
- ED:
-
Emergency department
- GEE:
-
Generalized Estimation Equation
- NTD:
-
New Taiwan Dollar
References
World Health Organization. World report on ageing and health. Geneva: Switzerland; 2015.
Ofori-Asenso R, Chin KL, Curtis AJ, Zomer E, Zoungas S, Liew D. Recent patterns of multimorbidity among older adults in high-income countries. Popul Health Manag. 2019;22(2):127–37.
Knickman JR, Jing M, Schear S, Anderson G, Horvath J, Colby DC. Chronic conditions: making the case for ongoing care. Partnership for solutions; 2010. https://policycommons.net/artifacts/1174992/chronic-conditions/1728121/.
Picco L, Achilla E, Abdin E, Chong SA, Vaingankar JA, McCrone P, et al. Economic burden of multimorbidity among older adults: impact on healthcare and societal costs. BMC Health Serv Res. 2016;16:173.
Bähler C, Huber CA, Brüngger B, Reich O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: a claims data based observational study. BMC Health Serv Res. 2015;15:23.
Griffith LE, Gilsing A, Mangin D, Patterson C, van den Heuvel E, Sohel N, et al. Multimorbidity frameworks impact prevalence and relationships with patient-important outcomes. J Am Geriatr Soc. 2019;67(8):1632–40.
Guiding principles for the care of older adults with. Multimorbidity: an approach for clinicians: American Geriatrics Society Expert Panel on the care of older adults with Multimorbidity. J Am Geriatr Soc. 2012;60(10):E1–E25.
Desmedt M, Vertriest S, Hellings J, Bergs J, Dessers E, Vankrunkelsven P, et al. Economic impact of integrated care models for patients with chronic diseases: a systematic review. Value Health. 2016;19(6):892–902.
World Health Organization. WHO global strategy on people-centred and integrated health services: interim report. Geneva: Switzerland; 2015.
Maruthappu M, Hasan A, Zeltner T. Enablers and barriers in implementing integrated care. Health Syst Reform. 2015;1:250–6.
Barajas-Nava LA, Garduño-Espinosa J, Mireles Dorantes JM, Medina-Campos R, García-Peña MC. Models of comprehensive care for older persons with chronic diseases: a systematic review with a focus on effectiveness. BMJ Open. 2022;12(8):e059606.
Rocks S, Berntson D, Gil-Salmerón A, Kadu M, Ehrenberg N, Stein V, et al. Cost and effects of integrated care: a systematic literature review and meta-analysis. Eur J Health Econ. 2020;21(8):1211–21.
Nolte E, Pitchforth E. What is the evidence of economic impacts of integrated care? World Health Organization, Regional Office for Europe, European Observatory on Health Systems and Policies; 2014.
Baxter S, Johnson M, Chambers D, Sutton A, Goyder E, Booth A. The effects of integrated care: a systematic review of UK and international evidence. BMC Health Serv Res. 2018;18(1):350.
OECD. Health at a glance 2021: OECD indicators. Paris: OECD Publishing; 2021.
Chen LK. Population aging and health care services: what governments should do. Arch Gerontol Geriatr. 2021;92:104296.
Chen H, Chen Y, Cui B. The association of multimorbidity with healthcare expenditure among the elderly patients in Beijing, China. Arch Gerontol Geriatr. 2018;79:32–8.
Siaw MYL, Malone DC, Ko Y, Lee JY. Cost-effectiveness of multidisciplinary collaborative care versus usual care in the management of high-risk patients with diabetes in Singapore: short-term results from a randomized controlled trial. J Clin Pharm Ther. 2018;43(6):775–83.
Tzeng DS, Lian LC, Chang CU, Yang CY, Lee GT, Pan P, et al. Healthcare in schizophrenia: effectiveness and progress of a redesigned care network. BMC Health Serv Res. 2007;7:129.
Lin J, Islam K, Leeder S, Huo Z, Hung CT, Yeoh EK, et al. Integrated care for multimorbidity population in Asian countries: a scoping review. Int J Integr Care. 2022;22(1):22.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–56.
Li CM, Lin CH, Li CI, Liu CS, Lin WY, Li TC, et al. Frailty status changes are associated with healthcare utilization and subsequent mortality in the elderly population. BMC Public Health. 2021;21(1):645.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of Observational studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573–7.
National Health Insurance Administration., Ministry of Health and Welfare, Taiwan. Program of patient-centered integrated clinic. https://www.nhi.gov.tw/resource/Query/%E9%86%AB%E9%99%A2%E4%BB%A5%E7%97%85%E4%BA%BA%E7%82%BA%E4%B8%AD%E5%BF%83%E9%96%80%E8%A8%BA%E6%95%B4%E5%90%88%E7%85%A7%E8%AD%B7%E8%A8%88%E7%95%AB.pdf. Accessed 1 Dec 2020.
Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–5.
Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc. 1975;23(10):433–41.
Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–95.
Hoyl MT, Alessi CA, Harker JO, Josephson KR, Pietruszka FM, Koelfgen M, et al. Development and testing of a five-item version of the geriatric Depression Scale. J Am Geriatr Soc. 1999;47(7):873–8.
Kaiser MJ, Bauer JM, Ramsch C, Uter W, Guigoz Y, Cederholm T, et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging. 2009;13(9):782–8.
National Health Insurance Administration. NHI MediCloud System. Taipei: National Health Insurance Administration, Ministry of Health and Welfare. Volume 21. Taiwan; 2020. https://www.nhi.gov.tw/Content_List.aspx?n=8FD3AB971.F557AD4&topn=5FE8C9FEAE863B46. Accessed 19 Nor 2023.
By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 updated AGS beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–94.
Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–9.
Lai HY, Huang ST, Chen LK, Hsiao FY. Development of frailty index using ICD-10 codes to predict mortality and rehospitalization of older adults: an update of the multimorbidity frailty index. Arch Gerontol Geriatr. 2022;100:104646.
Wu TY, Majeed A, Kuo KN. An overview of the healthcare system in Taiwan. Lond J Prim Care (Abingdon). 2010;3(2):115–9.
Yen KH, Hsu CC, Yu PC, Liu HY, Chen ZJ, Chen YW, et al. Determinants of improved quality of life among older adults with multimorbidity receiving integrated outpatient services: a hospital-based retrospective cohort study. Arch Gerontol Geriatr. 2021;97:104475.
Hsu WC, Hsu YP. Patterns of outpatient care utilization by seniors under the National Health Insurance in Taiwan. J Formos Med Assoc. 2016;115(5):325–34.
Leung AC, Yau DC, Liu CP, Yeoh CS, Chui TY, Chi I, et al. Reducing utilisation of hospital services by case management: a randomised controlled trial. Aust Health Rev. 2004;28(1):79–86.
Goldzahl L, Stokes J, Sutton M. The effects of multi-disciplinary integrated care on healthcare utilization: evidence from a natural experiment in the UK. Health Econ. 2022;31(10):2142–69.
Ye Z, Jiang Y. Title: the impact of a pilot integrated care model on the quality and costs of inpatient care among Chinese elderly: a difference-in-difference analysis of repeated cross-sectional data. Cost Eff Resour Alloc. 2022;20(1):28.
Hanley JA, Negassa A, Edwardes MD, Forrester JE. Statistical analysis of correlated data using generalized estimating equations: an orientation. Am J Epidemiol. 2003;157(4):364–75.
Acknowledgements
We thank the case managers Wei Lee and Jung Chen for their assistance in data collection and the information technicians at the National Cheng Kung University Hospital for helping to extract data from the electronic medical records of the patients.
Funding
This study was supported in part by grants from the National Cheng Kung University Hospital (NCKUH-11003007, NCKUH-V101-10), Ministry of Science and Technology (MOST 110-2314-B-006-016), and National Health Research Institute (NHRI-11A1-CG-CO-04-2225-1). The sponsors had no influence on the study design, data collection and analysis, decision to publish, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
YTL, MHC, THL, and YPY conceptualized the study. YTL and MHC collected data and performed the analyses. YTL was the primary contributor to the first draft of the manuscript. YCY, CMC, MHC, THL, and YPY provided feedback on the draft protocol and manuscript. All authors have read and approved the final manuscript before submission, agreed to submit it to the journal, and agreed to take responsibility for the content of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of National Cheng Kung University Hospital (A-ER-109-311). Considering the retrospective nature of the study and the fact that privacy precautions were taken, the Institutional Review Board waived the requirement for written informed consent from participants.
Consent for publication
Not applicable. This study does not contain personal data.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lo, YT., Chen, MH., Lu, TH. et al. Effects of an integrated ambulatory care program on healthcare utilization and costs in older patients with multimorbidity: a propensity score-matched cohort study. BMC Geriatr 24, 109 (2024). https://doi.org/10.1186/s12877-023-04654-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04654-y