
Abstract
Background
Informal caregivers of older patients often neglect their self-care, despite the mental and physical health effects of caregiving. Randomized controlled trials (RCTs) on self-care interventions for informal caregivers are lacking, making it difficult to determine effective strategies. This systematic review explored the definition and categories of self-care RCTs for informal caregivers and a meta-analysis was conducted to determine the effectiveness of these interventions.
Methods
Seven databases (Scopus, Web of Science, MEDLINE, PubMed, ProQuest, CINAHL, and Embase) were searched for articles in English reporting on self-care intervention outcomes for informal caregivers of patients aged 60 years or older. Standardized mean differences (SMD) with 95% confidence intervals (CI) were calculated using a random-effects model. Subgroup, sensitivity, and publication bias analyses were conducted.
Results
Eighteen studies were included in the systematic review, of which fifteen studies were included in the meta-analysis. RCTs lacked a clear definition of self-care, mainly focused on promoting physical and mental health and individual capacity, and neglected disease prevention. The interventions focused on self-management for health and individual agency, with less attention on health literacy, decision-making capacity, self-monitoring for health status, and linkage to the health system. Meta-analysis results showed that RCTs had a small effect on reducing anxiety (SMD = -0.142, 95% CI [-0.302, 0.017], p = .081) but a significant effect on reducing depression (SMD = -0.214, 95% CI [-0.353, -0.076], p = .002). Country and type of caregiver significantly contributed to the effect of reducing caregivers’ depression in subgroup analysis.
Conclusions
Studies on caregiver-centered self-care interventions are limited, resulting in a lack of a clear definition and comprehensive intervention. RCTs indicated a small effect on informal caregivers’ mental health, and interventions should consider both mental and physical health. More evidence is needed on the effectiveness of self-care interventions for informal caregivers’ anxiety and physical health.
Similar content being viewed by others


Introduction
Informal caregivers are relatives, friends, or neighbors who provide ongoing assistance, typically unpaid, to someone with limitations in their physical, mental, or cognitive function [1, 2]. Their mental and physical health can be adversely affected by the role change and financial stress until the caregiving role ends [3]. As outlined by Pearlin’s stress process model, anxiety, depression, irascibility, and cognitive disturbance are important outcomes of caregivers’ mental health [4]. Self-care behaviors are an important contributor to health outcomes [5] that can reduce the effect of caregiver stress on general well-being [6]. According to the Embracing Carers International Global Survey, 42% of informal caregivers prioritized the health of the care recipients over their personal care in 2017, and this further increased to 89% in 2020 [7, 8]. More importantly, caregivers and care recipients share a reciprocal relationship [9]. Negative psychological emotions in caregivers have a negative impact on care recipients’ cognitive function [10] and dependence in activities of daily living (ADLs) [9]. In other words, if caregivers take good care of themselves, this will benefit both them and their care recipients. Therefore, it is important for caregivers to have more awareness of their health status and engage in health-promoting self-care behavior [6, 11], especially physical activity, stress management, social support, and support resources [12].
Self-care was first defined in 1983 by the World Health Organization (WHO) [13] and updated in 2013 as “the ability of individuals to promote and maintain health, prevent disease, and cope with illness and disability with or without the support of a healthcare provider” [14]. The concept of self-care has been developed and applied in the field of informal caregivers of older patients during recent decades. Self-care interventions are tools that support self-care [15], encompassing practices and approaches that intersect with health systems and health professionals [16]. Self-care interventions include but are not limited to self-management, self-testing, and self-awareness [5]. In 2022, WHO further classified these interventions into individual agency, health information-seeking, social and community support, personal health tracking, self-diagnosis of health conditions, self-management of health, health system, and financial aspects [15]. Self-care for caregivers is important, and some interventions have emerged to enable their self-care. However, current research on self-care interventions for caregivers shows limitations. First, self-care has often been defined as self-management, because they are often thought of as synonymous, making evidence relating to self-care interventions obscure and confusing [17]. Moreover, most interventions have focused on helping caregivers support the disease management of patients, rather than aiding the caregivers [18,19,20]. Although a scoping review of interventions for family caregiver self-care was completed, the results were not comprehensive because it only involved family caregivers of people with dementia [21]. People with dementia only account for 48% of all patients with informal caregivers, suggesting that self-care interventions for more than half of older patients’ caregivers remain unclear [22]. Given these limitations, this study systematically collected randomized controlled trials (RCTs) on promoting self-care behaviors among informal caregivers of older patients, including the definition of self-care and categories of self-care interventions in these studies. A meta-analysis followed to determine the effectiveness of these RCTs for informal caregivers’ self-care.
Methods
This study was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [23], as shown in Additional file 1. This review was registered on PROSPERO: CRD42023393329.
Search strategy
A comprehensive search was conducted using seven electronic databases in the field of social science, gerontology, public health, medicine, and nursing: Scopus, Web of Science, MEDLINE, PubMed, ProQuest, CINAHL, and Embase. In November 2022, two independent reviewers searched titles, abstracts, and keywords for relevant journal articles published between January 1, 2000, and October 31, 2022, with language restricted to English. The general search strategies and queries are listed in Table 1. The detailed search strategy for each database is listed in Additional file 2. A social science librarian at the affiliated university enriched the search strategies.
Selection criteria
Studies were included based on the following criteria: (a) patients aged 60 years old or older; (b) informal caregivers aged 18 years old or older; (c) RCT or pilot RCT; (d) included detailed intervention procedures and outcomes; (e) peer-reviewed; and (f) written and published in English. Studies were excluded if they were: (a) not caregiver-centered; (b) RCT protocol; (c) not published in a journal; or (d) not available as full text.
Data extraction
The web-based literature review tool Covidence (http://www.covidence.org) was used to facilitate the systematic review process. After identifying all relevant articles and removing duplicates, two reviewers screened the titles, abstracts, and full-text articles together. Disagreements were addressed by the third researcher. The following components for each article were extracted by two reviewers together and stored and synthesized in Microsoft Excel: (a) author and publication year; (b) study country; (c) definition of self-care; (d) self-care category (based on the WHO Self-Care Framework); (e) study design (RCT or pilot RCT, single-blinded, double-blinded, or not blinded); (f) participants in the intervention group and control group; (g) care recipients’ diagnosis; (h) study intervention details (duration, intensity, type, and frequency); and (i) outcome.
Assessment of risk of bias
The Cochrane risk of bias tool for RCTs was used to evaluate the methodological quality. It measures risks in seven domains: random sequence generation, allocation concealment, selective reporting, blinding of participants and personnel, blinding of outcome measurement, incomplete outcome data, and other bias [24]. Each domain is scored as “low” (low risk of bias), “high” (high risk of bias), or “unclear” (insufficient rationale or information for judgment). The result is determined by the number of “low” scores in each dimension, with less than or equal to two indicating high risk of bias, three to five indicating moderate risk of bias, and six or seven indicating low risk of bias. In this study, two reviewers independently assessed the risk of bias in each study, and disagreements were resolved by discussion with the third reviewer.
Data synthesis and analysis
The meta-analysis was conducted using the “meta” package in R studio 2022.07.2. Because the outcomes were all continuous variables, this study used standardized mean differences (SMD) as a composite effect measure, along with 95% confidence intervals (CI). We extracted data on the number of participants, means, and standard deviations for the intervention and control groups after the intervention. Where standard deviations were not reported by the authors, they were calculated by the researchers using the formula (SD = SE × √n). For studies with multiple follow-ups, only the first outcome measurement after the intervention or follow-up was extracted for this study.
For each meta-analysis, statistical heterogeneity was assessed using the Cochran Q test and I2 statistic. Due to the various populations and criteria in different studies, this study used random-effects modeling to pool the results. Heterogeneity was indicated if the p-value was less than 0.05 and the I2 value was greater than 40% [25]. Subgroup analysis was also performed according to the country, intervention type, participants, type of patient, evaluation instruments, and outcome measure time. Heterogeneity tests assessed differences between studies using Q or I I2 statistics. If heterogeneity is significant (p-value < 0.05 or I2 > 50%), it indicates that effect sizes differ significantly across studies. Funnel plots and Egger’s test were used to assess publication bias. Sensitivity analyses were used to explore the robustness of the results, and pooled effect sizes were re-estimated after excluding studies at high risk of bias and compared with the meta-analysis results before exclusion. If no change in the results occurred, the conclusions obtained from this study were robust.
Results
Selection and characteristics of studies
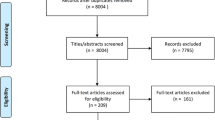
Figure 1 summarizes the review process. The initial search yielded 1,341 articles from seven electronic databases, with 651 duplicates removed. After screening the titles and abstracts and reviewing full-text articles, 18 articles met the inclusion criteria for systematic review and 15 articles were included in the meta-analysis.

Flow diagram of search
This systematic review included eighteen studies involving RCTs (details in Table 2). The sample sizes of these studies ranged from 26 to 642 individuals. These studies were published between 2006 and 2022. Ten studies were not blinded or did not describe blinding [26,27,28,29,30,31,32,33,34,35], five studies were single-blinded [36,37,38,39,40], and three studies were double-blinded [41,42,43]. Eight studies occurred in the United States [30,31,32,33,34,35,36, 41], one in Australia [38], three in the Netherlands [26, 37, 43], two in Hong Kong [40, 42], and one each in Japan [28], Singapore [27], Korea [39], and Germany [29]. Among these eighteen studies, seven studies involved caregivers and patients [27, 32, 34, 37, 38, 42, 43], whereas eleven studies involved only caregivers [26, 28,29,30,31, 33, 35, 36, 39,40,41]. In terms of the minimum age requirement for caregivers, the available literature presents varying findings. Nine studies established the minimum age for caregivers at 18 [26, 33, 35,36,37,38, 40,41,42], whereas four studies set the minimum age limit at either 21 or 40 years old [27, 30, 32, 39]. Additionally, five studies did not identify any specific age restrictions. It is noteworthy that most studies examined both male and female caregivers, with only two studies specifically focusing on the gender of caregivers: one study concentrating on female caregivers [30] and another on male caregivers [34]. Regarding the relationship between caregivers and patients, the majority of studies encompassed spouses, partners, relatives, and friends. However, two studies exclusively concentrated on spouses [30, 34], while one study specifically targeted adult children [42]. Eight studies focused on older patients with dementia and cognitive impairment [28,29,30,31,32, 37, 41, 42], five studies involved older patients with cancer [27, 33, 34, 36, 38], one study focused on patients who were depressed [26], one study involved patients with Parkinson’s disease [43], one study involved patients with chronic disease [40], one study targeted people under long-term care [39], and one study focused on patients with hematopoietic stem cell transplantation [35]. Thirteen studies used depression [27, 28, 30, 33, 34, 36,37,38,39,40,41,42,43] and six studies used anxiety [26, 33, 34, 36, 37, 40] as the mental health outcome measure; two studies used physical function as the outcome measure [30, 31]. The first outcome measurement time varied ranging from immediately postintervention to 6 months.
Risk of bias assessment
Figure 2 shows that two studies had low risk of bias [29, 42], three studies had high risk of bias [27, 30, 31], and the other thirdteen studies had moderate risk of bias. Most studies ensured randomization, allocation concealment, but ten studies have high risk in blinding of participants and personnel [26, 29, 30, 33, 35,36,37,38,39] and three studies have high risk in blinding of outcome measurement [35, 36, 41]. Nine studies [26, 29, 33, 35,36,37,38, 41, 42] had no selection reporting bias; the remainder could not be verified. Although most of the studies had reasonable attrition, only two studies had a remaining sample size of less than 30 participants, which we believe may have resulted in bias due to incomplete outcome data [28, 33]. We could not verify other risks of bias in these studies due to the lack of primary data, so other forms of bias in each study were unclear.

Risk of bias of 18 studies included in the systematic review. Studies: (1) Dionne-Odom, 2022 [36]; (2) Bijker, 2017 [26]; (3) Leow, 2015 [27]; (4) Fuju, 2021 [28]; (5) Boots, 2018 [37]; (6) Terracciano, 2020 [41]; (7) Connell, 2009 [30]; (8) Heckel, 2018 [38]; (9): Elliott, 2010 [31]; (10) Nightingale, 2022 [33]; (11) Lewis, 2019 [34]; (12) Au, 2020 [42]; (13) Han, 2020 [39]; (14) A’Campo, 2010 [43]; (15) Hou, 2014 [40]; (16) Behrndt, 2019 [29]; (17) Belle, 2006 [32]; (18) El-Jawahri, 2020 [35]
Definition of self-care
The WHO’s definition of self-care was adopted in analyzing the data [14]. For studies that did not have a clear definition of self-care, we summarized the definition based on the objectives and intervention content. Table 2 shows all these studies regarded self-care as activities that promote and maintain physical or mental health status. Additionally, most studies considered individual capacity growth and empowerment, including self-efficacy [30, 33, 34, 37], communication skills [35, 39,40,41], health literacy [27, 35, 38, 40], decision-making ability [36, 38, 39, 41], and self-empowerment [29, 32] of caregivers. However, no studies focused on preventing certain diseases among caregivers, and only two studies focused on coping with illness and disability [29, 32], instead aiming to address care recipients’ behavior problems instead of caregivers.
Therefore, most studies defined self-care as activities or practices that promote and maintain physical and mental health and enhance individual capacity and empowerment, but very few studies addressed the prevention and management of diseases among caregivers.
Category of self-care interventions
Regarding self-care interventions for self-carers and caregivers, this study classified these interventions into eight aspects. As shown in Table 2, all these studies fell in the “self-management of health” category, which includes self-care prevention that supports physical and mental health and well-being. Most studies also fell into the “individual agency” category, which encompasses promoting awareness of self-care, confidence and efficacy, self-care capacity, health and digital literacy, and sustained adoption of self-care practices and behaviors. Seven studies were classified in the “social and community support” category [27, 32,33,34, 38, 42, 43], which means these interventions can help caregivers get support from local networks, such as family, community, university, and the internet. Only two studies belonged to the “health information-seeking” category, related to acquiring health education for health-related decision-making [36, 41]. One study was classified as the “individual financial transactions for health” category, which involves financial support and practical difficulties (such as legal affairs) among caregivers [38]. No studies focused on personal health tracking (self-monitoring of health at home or in the community, data capture or documentation by self-care user or device), self-diagnosis of health conditions (self-testing and self-collection of samples for external testing), and individual linkage to the health system (identifying the location of health facilities and receiving feedback from health workers).
Results of meta-analysis
Although these studies reported results from more than a dozen RCTs of caregiver self-care, such as burden, stress, self-efficacy, the only outcomes truly relevant to caregivers included mental health (depression, anxiety, irascibility, cognitive disturbance) and physical health, according to the stress process model presented by Pearlin in 1990 [4]. In these 15 studies, the mental health outcomes were anxiety and depression, whereas physical health outcomes were rare and not consistent with each other in conceptualization and operationalization. Subgroup analysis was also performed by country, intervention form, intervention duration, type of caregivers, participants, type of patients, evaluation instruments, and outcome measure time.
Anxiety
Six studies were included in a meta-analysis to evaluate the impact of current interventions on reducing the anxiety of caregivers. The result of the meta-analysis shows these interventions did not significantly affect the anxiety of caregivers (SMD = -0.142, 95% CI [-0.302, 0.017], p = 0.081; see Fig. 3) and had low heterogeneity (I2 = 0.0%, p = 0.646). No publication bias was found from the funnel plot (details in Additional file 3) and Egger’s test (p = 0.291). Considering the absence of studies of substandard quality within the selected pool of six studies, we conduct a leave-one-out approach for the sensitivity analysis and get the same results (SMD = -0.142, 95% CI [-0.302, 0.017], p = 0.081). However, none of the variables contributed significantly to the between-group variance in effect sizes, suggesting that these six studies did not differ by subgroup factors in reducing caregiver anxiety (details in Additional file 3).

Forest plot of the effect of 6 studies on anxiety level
Depression
Thirteen studies were included in a meta-analysis to assess the effectiveness of these interventions in reducing depression in caregivers. Results show they significantly reduced depression among caregivers (SMD = -0.214, 95% CI [-0.353, -0.076], p = 0.002; see Fig. 4) and had moderate heterogeneity (I2 = 44.2%, p = 0.043). No publication bias was shown from the funnel plot (details in Additional file 4) and Egger’s test (p = 0.340). After excluding low-quality studies [27, 30], the results were stable after a sensitivity analysis of the remaining eleven studies (95% CI [-0.343, -0.053], p = 0.008).

Forest plot of the effect of 13 studies on depression level
As for subgroup analysis, we found that country and type of caregiver contributed significantly to the between-group variance in effect sizes (details in Table 3 and Additional file 4). Studies from Asia (Hong Kong, Singapore, and Japan) showed a stronger effect in reducing depression than other countries (p = 0.009). RCTs just involving family caregivers showed a stronger effect in reducing depression than all types of informal caregivers in these studies (p = 0.003).
Physical function
Two studies focused on physical health, one focused on the improvement of self-rated physical health status, and another explored the exercise behavior of participants. Considering the limited studies and inconsistent variables, we could not conduct a meta-analysis of caregivers’ physical health. But RCT results suggest that interventions for caregivers can increase their exercise behavior and improve their self-rated physical health [31].
Discussion
To our knowledge, this is the first systematic review of RCTs to promote self-care behavior among informal caregivers of older patients, with effectiveness examined by meta-analysis. From this review, we found that most existing RCTs conflated caregiver self-care with the self-management of patients, which is consistent with previous studies [17]. Meanwhile, some studies included self-care intervention as one of many subdomains, which made it difficult to affirm its true effectiveness [44]. As a result, it is clear that caregivers’ self-care has been overlooked and understudied.
Few RCTs have clearly defined self-care. Sakuma illustrated two types of self-care—direct provision of self-care technologies and indirect help with involvement in patient care—but this is not caregiver-centered self-care [45]. Although the WHO proposed a definition of self-care 40 years ago [13], no RCTs on caregivers’ self-care have used this definition. Based on this framework, our study defined the concept of self-care for each article and found that most studies focused on maintaining the physical and mental health of caregivers and promoting caregiver capacity related to caregiving, but they all neglected the prevention of future illnesses among caregivers, although caregiving often has a negative impact on both the physical and mental health of informal caregivers for older adults [2].
After categorizing these RCTs, we found that most focused on self-management for health and individual agency, but these studies only emphasized the importance of personal care, instead of teaching caregivers how to self-monitor their health status in daily life. Besides, few studies have paid attention to the importance of health-related decision-making, a critical issue because older patients and their caregivers often report low levels of self-perceived health literacy and low confidence in the information available to assess health-related decision-making [46]. Additionally, caregivers need social and local community support to avoid social isolation, cope with financial affairs, and engage in personal health care activities [12]. Therefore, future interventions on self-care for older patients’ caregivers should focus on building capacity for decision-making and establishing links between individuals and the health system.
Regarding the outcomes of these RCTs, we found that they mostly focused on caregivers’ mental health, with physical health rarely appearing as the outcome. This result is consistent with another systematic review on family caregivers’ health status [47]. Although the physical effects of caregiving are generally less intensive and unnoticeable than the psychological effects [48], physical health is as important as psychological health and often affected by mental health [49]. In addition, mental health outcomes were mainly depression and anxiety, with no mention of irritability and cognitive impairment as mentioned in Pearlin’s stress process model [4]. Hence, this study suggests practitioners involved in caregiver self-care could focus on improvements in caregivers’ physical health and cognitive function.
We noticed that very few studies measure caregivers’ self-care behavior, one study measures caregivers' confidence in helping themselves deal with the demands and challenges of the patient’s disease instead of their own health self-care [34], but this is not caregiver-centered self-care. Only two studies measure the self-efficacy in taking care of themselves [30] and obtaining respite and controlling upsetting thoughts about the caregiving situation [27] but do not focus on the improvement of self-care ability. In other words, the measurement of caregivers’ self-care in research has been notably lacking. Moreover, the existing studies that have examined caregivers’ self-care abilty have predominantly concentrated on subjective assessments of self-care efficacy, rather than objective evaluations of actual self-care behaviors. Consequently, it is imperative for future research endeavors to place emphasis on directly measuring both the competence and efficacy of caregivers’ self-care. This comprehensive approach would enable the development of interventions that genuinely prioritize the unique needs and preferences of caregivers. By adopting such an approach, caregiver-centered interventions can be truly aligned with the well-being and specific requirements of the caregivers themselves.
The heterogeneity of caregivers’ anxiety was not analyzed in the subgroup due to limited studies. Country and type of caregiver proved to be reasons for heterogeneity in these studies regarding informal caregivers’ depression. In studies from Asia—including Japan, Singapore, and Hong Kong—the intervention was more effective in reducing depression among caregivers compared to the control group. This may be because of the importance of filial piety in most Asian countries, such that filial piety can protect informal caregivers from depression by altering appraisals of the caregiver role [50,51,52]. The type of caregiver was another reason for the heterogeneity of RCTs in reducing depression. These interventions were more effective for family caregivers than informal caregivers. Compared with informal caregivers, family caregivers often have a stronger emotional bond with care recipients, which might motivate them to take better care of themselves to ensure better care to older patients.
As for the intervention format, our subgroup results also confirm a combination of face-to-face and online intervention was more beneficial for caregivers compared to the control group [21], with only face-to-face or only online interventions (such as telephone-based interventions) not significantly different between control and intervention groups. Currently, telephone-based interventions for caregiver self-care are becoming increasingly popular with researchers, but more evidence is needed to verify their effectiveness. RCTs conducted within 3 months indicated the interventions were more effective in reducing informal caregivers’ depressive symptoms than in control groups, which suggests that future RCTs need to pay more attention to the durability of intervention effects with longer follow-up sessions [53].
We also examined the participants, types of patients, and evaluation instruments during subgroup analysis. However, improvements in caregivers’ mental health and physical health did not differ depending on these factors. Therefore, the inclusion of patients in the intervention is a possible direction to pursue to improve the self-care ability of both patients and caregivers. Previous studies have shown the benefits of dyadic intervention for patients [54], but the effects of dyadic interventions on the mental and physical health of caregivers need to be further explored. Because we focused on caregivers’ self-care outcomes, the effectiveness of these RCTs did not differ by the patients’ illness. But considering the limited studies in this meta-analysis, this finding still needs to be validated by more RCTs and meta-analyses.
Measurements of physical health in the included studies were not well established or widely used in caregiver self-care interventions. Caregivers’ physical health was not used as an outcome of most interventions, but rather as basic information about participants at baseline. Measurements of physical health were less consistent in two studies, which only used a self-reported questionnaire testing exercise condition and self-rated improvement in physical health, respectively [30, 31]. Although improvements in physical health are not achievable in the short term, we still recommend that physical health be valued in these interventions and assessed as an outcome.
Although quality of life is related to both physical and mental health dimensions and can also reflect the effectiveness of self-care interventions, it is a multidimensional concept that can be either a health-based approach, determined by the severity of the illness and the quality of care, or a person-centered approach, which is determined by the individual’s experience, subjective interpretations of health and illness and personal knowledge [55]. This heterogeneity poses challenges in conducting a reliable meta-analysis. Some studies adopted health-related approaches, focusing on the impact of caregiving on caregivers’ health-related quality of life (Hr-Qol) [26, 43]. Others employed person-centered approaches, capturing subjective aspects of quality of life, such as caregivers’ perceptions of their position in life and their overall well-being [27, 28, 33, 36, 37]. There was also one study that encompassed both physical and mental health dimensions in its measurement of quality of life [40]. While we acknowledge that quality of life is an important outcome measure in the context of self-care interventions for caregivers, the heterogeneity and conceptual challenges associated with its measurement within the included studies warranted caution in its inclusion in our meta-analysis. To ensure the reliability and validity of our meta-analysis results, we chose to focus on outcome measures that exhibited greater consistency and comparability across studies, such as depressive symptoms and anxiety.
This study has several limitations. To begin, the generalizability of our results may be limited because we only included studies in English. Additionally, we did not search for each subdimension under the WHO’s self-care framework, which prevented us from examining existing interventions in greater detail. Future reviews should focus on self-care interventions for informal caregivers based on each subdimension. Because different databases have different starting points of data collection, we restricted our time frame to 2000 onward and thus, records before 2000 were not explored. Finally, the effectiveness of RCTs on caregiver anxiety and physical function were not verified in our meta-analysis, which may be due to the limited number of included studies.
Conclusion
Self-care for caregivers of older patients is an emerging topic. Based on the framework of self-care from the WHO, this study suggests that informal caregiver self-care should focus on the maintenance of both physical health and mental well-being and promote individual capacity and illness prevention. RCTs have mainly focused on self-management for health and individual agency and neglected education to improve health literacy, decision-making capacity, self-monitoring of health status, and access to resources from the community and health system.
The results of the meta-analysis indicated small associations between informal caregivers’ self-care interventions with their mental health. This study suggests that in addition to caregivers’ mental health, we should also focus on improving their physical health. The results of our sensitivity analysis show that our results are robust and stable, but due to the limited studies in the meta-analysis, the results of this subgroup analysis can only provide us with preliminary knowledge. More evidence from RCTs is needed on the effectiveness of informal caregivers’ self-care.
References
Roth DL, Fredman L, Haley WE. Informal caregiving and its impact on health: a reappraisal from population-based studies. Gerontologist. 2015;55:309–19.
Bom J, Bakx P, Schut F, van Doorslaer E. The impact of informal caregiving for older adults on the health of various types of caregivers: a systematic review. Gerontologist. 2018. https://doi.org/10.1093/geront/gny137.
Weitzner MA, Haley WE, Chen H. The family caregiver of the older cancer patient. Hematol Oncol Clin North Am. 2000;14:269–81.
Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: an overview of concepts and their measures. Gerontologist. 1990;30:583–94.
Narasimhan M, Allotey P, Hardon A. Self care interventions to advance health and wellbeing: a conceptual framework to inform normative guidance. BMJ. 2019;365:l688.
Acton GJ. Health-promoting self-care in family caregivers. West J Nurs Res. 2002;24:73–86.
Sullivan AB, Miller D. Who is taking care of the caregiver? J Patient Exp. 2015;2:7–12.
Embracing Carers. Global carer well-being index: who cares for carers? Perspectives on COVID-19 pressures and lack of support. 2020. Available from: https://www.embracingcarers.com/wp-content/uploads/Embracing-Carers-Merck-Survey-Results_FINAL.pdf. Accessed 21 Dec 2023.
Lu N, Liu J, Lou VWQ. Exploring the reciprocal relationship between caregiver burden and the functional health of frail older adults in China: a cross-lag analysis. Geriatr Nur (Lond). 2016;37:19–24.
Jiang N, Sun Q, Lou VWQ. The impact of caregiver’s depressive symptoms on trajectories of cognitive function in older adults with functional limitations. Int J Geriatr Psychiatry. 2021;36:1284–94.
Oliveira D, Zarit SH, Orrell M. Health-promoting self-care in family caregivers of people with dementia: the views of multiple stakeholders. Gerontologist. 2019;59:e501–11.
Sabo K, Chin E. Self-care needs and practices for the older adult caregiver: an integrative review. Geriatr Nur (Lond). 2021;42:570–81.
World Health Organization. Health Education Service. Health education in self-care: possibilities and limitations. 1984;HED/84.1.
World Health Organization. Regional office for South-East Asia self care for health. New Delhi: WHO Regional Office for South-East Asia; 2014.
World Health Organization. Classification of self-care interventions for health: a shared language to describe the uses of self-care interventions. 2021. Available from: https://www.who.int/publications-detail-redirect/9789240039469. Accessed 30 Jan 2023.
World Health Organization. WHO guideline on self-care interventions for health and well-being, 2022 revision. 2022. Available from: https://www.who.int/publications-detail-redirect/9789240052192. Accessed 24 Mar 2023.
Nichols T, Calder R, Morgan M, Lawn S, Beauchamp A, Trezona A, Byambasuren O, Bowman J, Clinton-McHarg T, Willis K, Kearns R, Harris-Roxas B, Duggan M, Wardle J, Litt J, Menzies D, Dawda P, Benrimoj S, Dineen-Griffin S, Banfield M, Fetherston H, Klepac-Pogrmilovic B. Self-care for health: a national policy blueprint. Policy paper 2020-01, Mitchell Institute, Victoria University, Melbourne. 2020. Available from: https://www.vu.edu.au/mitchell-institute/prevention-risk/self-care-for-health-a-national-policy-blueprint. Accessed 21 Dec 2023.
Barsuk JH, Wilcox JE, Cohen ER, Harap RS, Shanklin KB, Grady KL, et al. Simulation-based mastery learning improves patient and caregiver ventricular assist device self-care skills. Circ Cardiovasc Qual Outcomes. 2019;12:e005794.
Chester H, Beresford R, Clarkson P, Entwistle C, Gillan V, Hughes J, et al. The Dementia Early Stage Cognitive Aids New Trial (DESCANT) intervention: a goal attainment scaling approach to promote self-management. Int J Geriatr Psychiatry. 2021;36:784–93.
Cockayne S, Pattenden J, Worthy G, Richardson G, Lewin R. Nurse facilitated self-management support for people with heart failure and their family carers (SEMAPHFOR): a randomised controlled trial. Int J Nurs Stud. 2014;51:1207–13.
Oliveira D, Sousa L, Orrell M. Improving health-promoting self-care in family carers of people with dementia: a review of interventions. Clin Interv Aging. 2019;14:515–23.
Alzheimer’s Association. 2023 Alzheimer’s disease facts and figures. Alzheimers Dement. 2023;19:1598–695.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Deeks JJ, Higgins JP, Altman DG, Group on behalf of the CSM. Analysing data and undertaking meta-analyses. In: Cochrane Handbook for Systematic Reviews of Interventions. Wiley. 2019. p. 241–84.
Bijker L, Kleiboer A, Riper HM, Cuijpers P, Donker T. A pilot randomized controlled trial of E-care for caregivers: an internet intervention for caregivers of depressed patients. Internet Interv. 2017;9:88–99.
Leow M, Chan S, Fai CM. A pilot randomized, controlled trial of the effectiveness of a psychoeducational intervention on family caregivers of patients with advanced cancer. Oncol Nurs Forum. 2015;42:E63–72.
Fuju T, Yamagami T, Yamaguchi H, Yamazaki T. A randomized controlled trial of the “positive diary” intervention for family caregivers of people with dementia. Perspect Psychiatr Care. 2021;58:1949–58.
Behrndt E-M, Straubmeier M, Seidl H, Vetter C, Luttenberger K, Graessel E. Brief telephone counselling is effective for caregivers who do not experience any major life events – caregiver-related outcomes of the German day-care study. BMC Health Serv Res. 2019;19:20.
Connell CM, Janevic MR. Effects of a telephone-based exercise intervention for dementia caregiving wives: a randomized controlled trial. J Appl Gerontol Off J South Gerontol Soc. 2009;28:171–94.
Elliott AF, Burgio LD, DeCoster J. Enhancing caregiver health: findings from the resources for enhancing alzheimer’s caregiver health II intervention. J Am Geriatr Soc. 2010;58:30–7.
Belle SH. Enhancing the quality of life of dementia caregivers from different ethnic or racial groups: a randomized. Controlled Trial Ann Intern Med. 2006;145:727.
Nightingale C, Sterba KR, Levine B, Tooze JA, Greven K, Frizzell B, et al. Feasibility and acceptability of a multi-modality self-management intervention for head and neck cancer caregivers: a pilot randomized trial. Integr Cancer Ther. 2022;21:153473542210989.
Lewis FM, Griffith KA, Alzawad Z, Dawson PL, Zahlis EH, Shands ME. Helping her heal: randomized clinical trial to enhance dyadic outcomes in couples. Psychooncology. 2019;28:430–8.
El-Jawahri A, Jacobs JM, Nelson AM, Traeger L, Greer JA, Nicholson S, et al. Multimodal psychosocial intervention for family caregivers of patients undergoing hematopoietic stem cell transplantation: a randomized clinical trial. Cancer. 2020;126:1758–65.
Dionne-Odom JN, Azuero A, Taylor RA, Dosse C, Bechthold AC, Currie E, et al. A lay navigator-led, early palliative care intervention for African American and rural family caregivers of individuals with advanced cancer (Project Cornerstone): results of a pilot randomized trial. Cancer. 2022;128:1321–30.
Boots LM, de Vugt ME, Kempen GI, Verhey FR. Effectiveness of a blended care self-management program for caregivers of people with early-stage dementia (Partner in Balance): randomized controlled trial. J Med Internet Res. 2018;20:e10017.
Heckel L, Fennell KM, Reynolds J, Boltong A, Botti M, Osborne RH, et al. Efficacy of a telephone outcall program to reduce caregiver burden among caregivers of cancer patients [PROTECT]: a randomised controlled trial. BMC Cancer. 2018;18:59.
Han E-J, Park M, Park S, Giap TTT, Han D. Randomized controlled trial of the Caregiver Orientation for Mobilizing Personal Assets and Strengths for Self-Care (COMPASS) for caregiving journey: a national family caregiver support program in a long-term care insurance system. J Am Med Dir Assoc. 2020;21:1906–1913.e3.
Hou RJ, Wong SYS, Yip BHK, Hung ATF, Lo HHM, Chan PHS, et al. The effects of mindfulness-based stress reduction program on the mental health of family caregivers: a randomized controlled trial. Psychother Psychosom. 2014;83:45–53.
Terracciano A, Artese A, Yeh J, Edgerton L, Granville L, Aschwanden D, et al. Effectiveness of powerful tools for caregivers on caregiver burden and on care recipient behavioral and psychological symptoms of dementia: a randomized controlled trial. J Am Med Dir Assoc. 2020;21:1121–1127.e1.
Au A, Lai DWL, Biggs S, Cheng S-T, Haapala-Biggs I, Chow A, et al. Perspective-taking interventions for intergenerational caregivers of Alzheimer’s diseases: a randomized controlled trial. Res Soc Work Pract. 2020;30:306–19.
A’Campo LEI, Wekking EM, Spliethoff-Kamminga NGA, Le Cessie S, Roos RAC. The benefits of a standardized patient education program for patients with Parkinson’s disease and their caregivers. Parkinsonism Relat Disord. 2010;16:89–95.
Mavandadi S, Wray LO, Toseland RW. Measuring self-appraised changes following participation in an intervention for caregivers of individuals with dementia. J Gerontol Soc Work. 2019;62:324–37.
Sakuma H, Hasuo H, Fukunaga M. Effect of handholding on heart rate variability in both patients with cancer and their family caregivers: a randomized crossover study. Biopsychosoc Med. 2021;15:14.
Verma R, Saldanha C, Ellis U, Sattar S, Haase KR. eHealth literacy among older adults living with cancer and their caregivers: a scoping review. J Geriatr Oncol. 2022;13:555–62.
Ahn S, Romo RD, Campbell CL. A systematic review of interventions for family caregivers who care for patients with advanced cancer at home. Patient Educ Couns. 2020;103:1518–30.
Schulz R, Sherwood PR. Physical and mental health effects of family caregiving. AJN Am J Nurs. 2008;108:23–7.
Chang H-Y, Chiou C-J, Chen N-S. Impact of mental health and caregiver burden on family caregivers’ physical health. Arch Gerontol Geriatr. 2010;50:267–71.
Lai DWL. Filial piety, caregiving appraisal, and caregiving burden. Res Aging. 2010;32:200–23.
Pan Y, Jones PS, Winslow BW. The relationship between mutuality, filial piety, and depression in family caregivers in China. J Transcult Nurs. 2017;28:455–63.
Ng HY, Griva K, Lim HA, Tan JYS, Mahendran R. The burden of filial piety: a qualitative study on caregiving motivations amongst family caregivers of patients with cancer in Singapore. Psychol Health. 2016;31:1293–310.
Lambert S, Brahim LO, McCusker J, Coumoundouros C, Audet L-A, Yaffe M, et al. Non-pharmacological Interventions for caregivers with depression and caregivers of care recipients with co-morbid depression: systematic review and meta-analysis. J Gen Intern Med. 2021;36:3159–78.
Moon H, Adams KB. The effectiveness of dyadic interventions for people with dementia and their caregivers. Dementia. 2013;12:821–39.
Glozman JM. Quality of life of caregivers. Neuropsychol Rev. 2004;14:183–96.
Acknowledgements
Not applicable.
Funding
This work was supported by the Hong Kong Jockey Club Charities Trust for Sau Po Centre on Ageing of The University of Hong Kong for the Trust Initiated “Jockey Club Carer Space” Project. The funder has no role in study design, data collection and analysis, preparation of manuscript, or decision to submit for publication.
Author information
Authors and Affiliations
Contributions
L.H.R contributes to the conceptualization, systematic review and meta-analysis, and writes the original manuscript. V.W.Q.L is the corresponding author and contributes to the conception and suggestions of this study, and supervises the whole research process. X.S.C and L.H.R conduct the systematic review and contribute to the search strategy and data extraction in the original manuscript together. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA 2020 Checklist.
Additional file 2.
Search strategies in different databases.
Additional file 3.
Meta-analysis for anxiety.
Additional file 4.
Meta-analysis of depression.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, H., Lou, V.W.Q. & Xu, S. Randomized controlled trials on promoting self-care behaviors among informal caregivers of older patients: a systematic review and meta-analysis. BMC Geriatr 24, 86 (2024). https://doi.org/10.1186/s12877-023-04614-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04614-6