
Abstract
Background
Diabetes mellitus is a prevalent and potentially devastating chronic illness affecting many older adults. Given spousal involvement in many aspects of diabetes management, coping with their partners is increasingly seen as a potential solution to make up for limited resources. This study aimed to identify the key conditions for optimal implementation of couple-based collaborative management model (CCMM) among Chinese older couples with type 2 diabetes mellitus.
Methods
Older couples and community healthcare practitioners were selected according to couples’ joint intervention attendance rate and community’s average attendance rate. This mixed methods research consisted of a qualitative phase and a quantitative phase. In the qualitative phase, in-depth interviews were conducted among 12 pairs of couples in the intervention group and 4 corresponding practitioners, in the follow-up period of the multicentered RCT from January to April 2022. Qualitative comparative analysis (QCA) in the quantitative phase to identify conditions influencing CCMM’s implementation and to explore necessary and sufficient combinations of conditions (i.e., solutions) for improving patients’ glycated hemoglobin (HbA1c) control (outcome).
Results
Key conditions included implementation process, couple’s role in diabetes management, their belief and perception of CCMM, as well as objective obstacles and subjective initiative for behavior change. Accordingly, major barriers in CCMM’s implementation were patients’ strong autonomy (particularly among husbands), misbelief and misperception about diabetes management as a result of low literacy, and mistrust of the practitioners. QCA further revealed that no single condition was necessary for effective HbA1c control, while three types of their combinations would be sufficient. Solution 1 and 2 both comprised the presence of spousal willingness to help, plus correct belief and perception of diabetes management, well embodying the utility of couple collaborative management in supporting patients’ HbA1c control. On the other hand, solution 3 indicated that high-quality implementation even without spousal support, can promote the patient’s subjective initiative to overcome objective obstacles, suggesting enhanced self-management for HbA1c control.
Conclusions
Tailored CCMM should be implemented in reference to older couple’s preferences and literacy levels, to ensure intervention fidelity, and establish correct understanding of collaborative management among them.
Similar content being viewed by others

Introduction
Community-based disease management is an important healthcare delivery strategy for chronic diseases such as diabetes mellitus [1]. It involves community engagement in defining the problem and develops partnerships to implement management strategies [2]. In the past three years, considerable community healthcare resources have been devoted to the prevention and control of COVID-19 in China [3], resulting in overlooking many other health issues including chronic disease management. Increased attention thus has been paid to family involvement as a protentional solution to compensate the limited resources [4]. Increasing evidence has suggested that family members significantly improved the self-management activities of older people [5]. Cooperative management of family members, particularly spouses, have great influences on patients’ blood sugar control, including physical activities, dietary behaviors, medication adherence, and glucose monitoring [6,7,8].
The couple-based collaborative management model (CCMM) was proposed as a solution to better engage family in older patients’ care [9]. CCMM utilizes the interdependence of patients and their spouses for disease management. Through promoting health behaviors and mutual supports between the couple, CCMM seeks to enhance the couple’s disease management efficacy and improve their health as a whole [10]. CCMM roots in two theories, the Dyadic Model of Coping with Chronic Illness (DMCCI) and Social Cognitive Theory (SCT). DMCCI describes couples’ dyadic appraisal of the illness severity, ownership and management responsibility, and dyadic coping strategies [11]. Social Cognitive Theory (SCT) is an interpersonal level theory suggesting that we learn from the dynamic interaction between people (personal factors), their behavior, and their environments [12]. DMCCI elaborates on the couple’s coping process with chronic diseases, while SCT emphasizes the efficacy of disease management through collaboration. It is hypothesized that when the couple agrees on disease management as a joint responsibility, they may have more supportive behaviors and collective efficacy to facilitate their joint changes in behaviors and health conditions [13].
Despite developed theoretical basis of CCMM, its implementation remains challenging. By and large, barriers to implementing CCMM reported in previous studies can be grouped into two categories: low recruitment rates and poor adherence of couple-based interventions [14, 15]; as well as difficulties in forming couple collaboration [16, 17]. One qualitative study among Chinese couples indicates that the patients were reluctant to express feelings to their spouses, which might have hindered the formation of spousal empathy and common beliefs [18]. In addition, some spouses may refuse to be involved or get over-involved [16, 19]. Compared to young people, older couples may be more suitable for CCMM as they tend to spend more time together after retirement and have higher marital satisfaction with fewer conflicts in long-enduring marriages [11]. However, there is limited evidence on the barriers to implementing CCMM among older couples and their associations with different implementation outcomes.
To investigate the effect of CCMM on patients with type 2 diabetes mellitus, we conducted a multicentered randomized controlled trial (RCT) among 207 pairs of Chinese older couples in 14 community health centers in Guangzhou, China from August 2020 to May 2022 (Trial No. 2019-064) [20]. The coupled-based interventions consisted of four-week group education sessions and two-month telephone booster, delivered by community healthcare practitioners. Similar to previous couple-based trials, our study encountered difficulties especially low participation rate. We thus conducted the current study to explore the combinations of conditions necessary and sufficient (i.e., solutions) for CCMM’s implementation. Specifically, we utilized the qualitative comparative analysis (QCA) to disentangle key conditions of complex intervention [21] and generates plausible solutions (combination of conditions) [22], which would help improve implementing CCMM in diabetes management among older people.
Methods
Study design
This research consisted of a qualitative phase and a quantitative phase. In the qualitative phase, in-depth interviews were conducted among couples of the intervention group and corresponding practitioners, in the follow-up period of the multicentered RCT from January to April 2022 [20]. Key conditions identified through the interviews were analyzed then by QCA in the quantitative phase. The study was approved by the Ethics Committee of Sun Yat-sen University (2019-064).
Study participants
Couples for the interviews were selected using a purposive sampling method. To cover heterogeneity and enhance representative of the participants, we first selected five communities based on the community’s average attendance rate (two above the mean and three below); among them, four couples per community were invited for the interview based on their joint attendance rate (two each above and below 50%), alongside the community’s healthcare practitioners. Couples were invited by telephone to conduct the interview together at the community health center. Detailed participants information has been described in previous articles [20]. The recordings and transcripts were kept strictly confidential and could only be accessed by the authors of this study.
Qualitative phase: in-depth interviews
In order to better capture the influences of couple-based collaborative management, we designed an interview guide (see Appendix 1) based on the capability, opportunity, motivation–behavior (COM-B) model. COM-B model is an integrative theoretical model based on causal mechanisms to identify individual and environmental factors that influence behavioral change [23], and has been successfully applied to various health-related behaviors, such as smoking cessation [24] and vaccination [25, 26].
Each interview lasted 30 to 60 min and was conducted by three female researchers together (J.Z., CH.Y., YX.L.): a moderator who asked questions, a recorder, and an observer who captured the facial expressions, body movements, tone of the interviewee, and the interview settings. Audio recordings and interview notes were kept for all interviews. All the researchers were trained before the start of the study.
The interview data were coded verbatim and analyzed using NVivo 12.0 software. Two researchers (J.Z., CH.Y.) repeatedly read and coded the interview transcripts independently, prior to coding the interviews using thematic analysis. Each researcher described the meaning of the code they developed and developed the coding structure individually. Guided by the CCMM theoretical framework [20], codebooks were created and categorized into relevant themes and sub-themes, with newly identified themes added as separate components to the CCMM framework. We refined the codebook in an iterative loop. Two coders independently applied the codebook to the most recent interview data, compared codes, discussed differences with a third coder (YX.L.), and improved the codes. The final codebook was generated after the researchers had achieved at least 80% internal consistency in coding the same case. A prefinal thematic structure was reviewed at length and all researchers agreed on the expanded CCMM framework.
Quantitative phase: QCA
Themes identified from the interviews were included as conditions in QCA. Each couple or healthcare practitioner was regarded as a case (the unit of QCA analysis) [27]. Fuzzy-set QCA (fs QCA) was used to explore possible combination(s) of conditions leading to CCMM implementation. Successful CCMM implementation (outcome) was defined as controlled glycemic level (HbA1c level ≤ 7.0%) from baseline to 6-month follow-up, in line with diabetes management clinical guideline [28]. The HbA1c level was collected from the multicentered RCT and tested by Daan Gene testing company. Using Boolean algebra [29], QCA is a set-theoretic approach to summarizing elements across cases, and establishing nonlinear causal relationships via identifying necessary conditions (i.e., always present if the outcome occurs), sufficient conditions (i.e. outcome always occurs if the condition exists), as well as combinations of conditions (i.e. solutions) [30, 31].
We examined each condition following the criteria developed by Ragin [27], and calibrated it to a truth table with values ranging from 0 to 1 to describe the relationship between solution and the outcome [32]. The condition necessity is quantified by a consistency level (indicating relationship strength, range 0 ~ 1) above 0.9, and solution sufficiency is quantified by a consistency level of 0.8 [27]. We also conducted robustness analyses by examining proportional reduction in inconsistency (measuring the probability of logical errors) and consistency levels. All analyses were conducted in fsqca software. Detailed assignment and analysis steps were provided in Appendix 2.
Results
Participants’ characteristics
Among the 20 couples and 5 healthcare practitioners initially invited, 12 couples (response rate: 60%) and 4 healthcare practitioners (response rate: 80%) agreed to be interviewed. No new themes emerged as the interviews progressed to the 12th couple and the 4th practitioner, which was considered as data saturation. As shown in Table 1, the interviewed couples had an average age of 68 years, with the patients on average one year older than their spouses. The average disease duration of patients was eight years. The majority of patients had below high school education and spouses had high school education. Couples were mostly retired and lived in the city. Most community healthcare practitioners were community physicians with an average of ten years of practicing experience.
Conditions of CCMM implementation identified through interviews
Based on the interviews, 6 themes and 26 sub-themes were identified. Detailed explanations, descriptions and quotations for each theme are provided in Table 2.
Implementation process showed the implementation dilemma from the practitioners’ perspective. The community healthcare practitioners all reported (4/4) that older adults had established inherent ways of thinking and behaving, and it was difficult to achieve rapid change in their long-term habits. In addition, they believed that outcomes largely relied on the patient’s adherence and the couple’s relationship than the intervention itself, meaning that the effectiveness of the intervention was limited by the couple’s willingness and capability to collaborate in diabetes management.
Couple’s role in management showed the distribution of management responsibility between the couple. Although the majority of spouses (11/12) were more or less involved in the patient’s diabetes management, patients still believed diabetes health management to be their responsibility. Female patients were more willing to accept their spouse’s company and advice, whereas male patients seemed to show more independence.
Belief and perception reflected the common misconceptions about diabetes mellitus in older adults. Most couples (10/12) attributed the causes of diabetes to age, occupational experience, and genetic factors. But their knowledge about normal glucose ranges or possible consequences associated with high or low blood glucose was inadequate, which may contribute to poor engagement and adherence of the couple.
Subjective imitative, and objective obstacle were two themes related to promoting and hindering factors of behavior changes required by the intervention. Care and reminders from spouses were the strongest motivations to generate positive behaviors, while illness and frailty were the most significant physical obstacles which impeded the capability of adhering to daily health management activities. In addition, patients also generally reported that caring for grandchildren took up too much of their time, and such conflicting commitments may result in the absence of intervention.
Behavioral change occurred after the couple-based intervention. Among 12 couples interviewed, 10 patients simultaneously generated sole behavioral change while receiving assistance from their spouses. And one patient only reported sole behavioral change with a complete absence of spousal assistance, and one patient’s diabetes management was completely dependent on spousal assistance. Daily glucose monitoring was the most difficult management behavior for older couples to conduct. Some couples found management behaviors required by the intervention were just too strict or complex for them to perform.
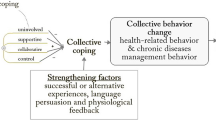
Given the themes of implementation conditions identified above, the CCMM framework was expanded into Fig. 1. The expanded framework additionally highlighted the role of intervention implementation, subjective initiative, and objective obstacles on management behavior changes, which may then lead to HbA1c control.

Expanded implementation framework of couple-based collaborative management model
Solutions for successful CCMM implementation suggested by QCA
The hypothetical solution as in Fig. 1 was then validated via QCA and the necessity of the single conditions was displayed in Table 3. Judging by the consistency level of 0.90 criterion for a necessary condition [27], no single condition of Fig. 1 alone was necessary to control HbA1c. On the other hand, three combinations of conditions were identified as solutions for successful implementation. As shown in Table 4, cases fulfilling either solution had a 62.6% possibility of achieving a successful outcome, and the three solutions together explained 84.5% of the successful cases.
For Solution 1 (a consistency level of 0.87, explained 25.4% of successful cases), the reduction of HbA1c was achieved via a combination of a high-quality intervention process, collaborative couple’s roles, correct belief, and perception as well as subjective initiative for CCMM. Similarly, Solution 2 (a consistency level of 0.82, explained 26.3% of successful cases) also emphasized collaborative couple’s roles, correct belief, and perception, but with a low-quality intervention process and lacking initiative, this solution can only achieve the reduction of HbA1c in the absence of objective obstacles. Both solutions entailed the couple’s collaboration and correct belief and perception of diabetes and its management, and this collaborative effect helps the patients manage diabetes.
On the contrary, Solution 3 (a consistency level of 0.86, explained 25.2% of successful cases) suggested a solution without the couple’s collaboration, such that high-quality intervention may nevertheless change the patient’s misunderstanding about diabetes, and promote self-motivation to overcome objective obstacles. For example, the spouse of couple 08 missed many couple-based intervention courses, which were attended by the patient alone. However, the courses provided instruments to patients for glucose monitoring, which motivated the patient to accomplish health management by herself.
Discussion
The present study investigated conditions and solutions of implementing CCMM in Chinese older couples with type 2 diabetes mellitus. We found that the main conditions centered on implementation process, couple’s role in diabetes management, and their belief toward CCMM and ability to perform it. QCA further identified three solutions-either promoting couple collaborative management (Solution 1 & 2) or enhancing patient self-management (Solution 3).
Implementation conditions of CCMM
Most of the identified conditions associated with couple’s role were in line with prior couple-based interventions, including marital discord [33], inappropriate forms of collaboration [17, 19], and discomfort with role change [18]. In addition, enacting a couple-based intervention requires coordinating participation of the couple pair, either one of them encountered objective obstacles such as distance and time [34], conflicting commitments [35], or financial difficulties [36] would hinder the implementation. Our study further contributes to the literature by identifying some unique implementation conditions of couple-based interventions among older Chinese couples, associated with older patients’ strong autonomy and low literacy. As regards strong autonomy, some older patients were just too stubborn to accept assistance from their spouses. It might result from older couples have already established a stable and deeply-rooted lifestyle, and formed an equilibrium in diabetes management over the long disease duration. Such that additional couple-based management may seem to be unnecessary, or difficult to achieve fundamental change through short-term interventions.
Moreover, the majority of our study participants were born between 1943 and 1965, generations with relatively poor education (i.e., lower than senior high school). The older couples’ low literacy may further result in their misconceptions about diabetes, and thus impede their understanding and application of couple-based interventions [37]. Our between-sex comparisons further showed that male patients were less likely to view diabetes care as a couple-shared responsibility, or to express concerns and emotions about diabetes to their spouses than their female counterparts. This may reflect that Chinese older men were used to characterize themselves as “tough guys” in life, thus would be shameful to show their distress or weakness, and discomfort with role change [18]. This gendered care pattern was also reported in American couples over food-related behavior changes [38]. Masculine gender roles were identified as a barrier, with husbands paying less attention to their wives’ health promotion activities [39]. It also may be a manner of protective buffering [17], such that protecting their spouses from negative emotions and avoiding arguments due to diabetes symptoms or management requirements.
Under the aforementioned circumstances, CCMM implementation would be even more difficult when the trust between older patients and their healthcare practitioners was low. Practitioners generally reported that it was hard to reason with older patients, let alone alter the older couple’s behaviors to obey the interventions. This frustration may in turn affect practitioners’ motivation to further implement CCMM. Previous studies have shown that Chinese residents’ trust in the healthcare system was low [40], especially in community healthcare centers [41]. In turn, patients’ mistrust may lead to practitioners’ negative attitudes [42], hence reducing the motivation and quality of the intervention implemented [43].
Solutions for successful CCMM implementation
To overcome the implementation conditions identified above, we found three solutions leading to HbA1c control, which can be further grouped into couple collaborative management type and self-management type.
The couple collaborative management type is embodied by Solution 1 and 2, both emphasizing the core conditions of couple collaboration and the correct perception of diabetes management. Our interviews indicated that supportive behaviors from the spouses provided more care and assistance for the patients, and created a harmonious family atmosphere encouraging patients to be responsible for their health. Previous studies have also found that spouse engagement is strong social support leading to significant and lasting improvements in glycemic control [44]. Moreover, we noted that older couples’ correct perception of diabetes and its management was a prerequisite for them to form a beneficial collaboration. Similar findings have been reported previously that spouses with more knowledge about diabetes may associate with performing more supportive and collaborative behaviors [45]. In addition, our previous studies also indicated that couple pairs’ relative differences in sociodemographic characteristics should be taken into account in couple-based intervention, such as the spouse’s age in reference to the patient’s (i.e., younger, the same, or older than the patients) and retirement status [46].
Despite the similarity in couple collaborative management type, these two solutions differed by several conditions. A high-quality intervention process and subjective initiative to change were needed for Solution1; while a low-quality intervention process rendering no motivation to change, the absence of objective obstacles was essential for Solution 2. Taken together, Solution 2 reflects an ideal situation when older couples with adequate knowledge about diabetes and neglectable objective obstacle, formed collaborative relationships in daily diabetes management, regardless of the CCMM intervention. Solution 1, in contrast, indicates the importance of high-quality CCMM intervention to enhance older couples’ knowledge and motivation to counteract objective obstacles, which may be more commonly seen in real practice.
On the other hand, the self-management type suggests the control of HbA1c can also be achieved through motivating the patients alone. Although against our intention to promote the couple’s collaboration via the CCMM intervention, patients who joined the courses without the company of their spouses were still able to achieve satisfying management results. It is suspected two main reasons may lead to the unintended self-management type. First, CCMM interventions were misinterpreted by some practitioners. Our interviews with the practitioners indicated that few of them overlooked the emphasis should be on “dyadic coping” in diabetes management, while purely delivered the courses as regular “self-management” education. The fidelity of intervention implementation (i.e., the extent to which the intervention is delivered as intended) is critical to the successful translation of CCMM strategies into practice [47]. Second, the older couples’ education levels and marital quality also affected their willingness to collaborate. As discussed above, some couples’ poor health literacy may confine their ability to comprehend the intervention contents or adapt to the recommended way of co-management. Despite relatively good marital quality would be expected among older couples who participated in our study, uncooperative behaviors of the spouses were also common such as non-attendance of the courses. One couple even divorced during our study follow-up. Collaboration would be hard for couples with negative attitudes or undesirable collaboration modes such as strong independence centrality, which may even lead to negative affect on the physiological and psychological function of the couples [48, 49]. For these couple pairs, couple-based intervention may be not suitable [16].
Implications for theory and practice
The present study extends the CCMM theoretical framework. We added new themes of implementation process, subjective initiative, and objective obstacles to CCMM, and highlighted the core conditions-the correct view of diabetes and collective efficacy, for the collaborative management type of couple. Older couples’ characteristics and marital quality should be taken into consideration. Furthermore, the original CCMM emphasizes collective behavior change. However, our study has extended this by proposing the other potential pathway for individual patient behavior change. As described in the DMCCI [11], it is possible that individual coping as well as dyadic coping may be involved simultaneously in different aspects of diabetes management. Future research on couple collaboration could further explore the relationship between self-management and co-management.
The practical contribution of this study is to provide evidence to apply tailored CCMM in accordance with couples’ preference and literacy. For couples who are willing to cope with diabetes together, enhancing couple collaboration and correct perception would be more likely to control diabetes successfully. For those who are not suitable for couple collaborative management, self-management plan should be preferred. In addition, intervention fidelity, adequate support, and incentives are important to help overcome setbacks during the intervention implementation. Apart from that, policymakers should strengthen the trust between physicians and patients, which would promote the improvement of physicians’ work attitudes and patients’ adherence.
Strengths and limitations
Our study innovatively used QCA to systematically investigate the theoretical framework utilized in the intervention and identified core solutions of successful CCMM implementation. Nevertheless, several caveats require attention. First, our study sample was small and with limited representativeness. Participants with unsatisfying marital quality and poor adherence to our intervention may not respond to our study. Second, QCA is semiquantitative by nature, and the causal relationship was verified based on qualitative information. To minimize subjective judgment, we involved five well-trained researchers with a different research background in coding and assigning values and used the robustness analyses to test confidence in the proposed relationships. The further quantitative analysis would be insightful to complement the findings here. Last, some information was lost due to compressing the rich interview findings into several themes and subthemes. This loss of information is unavoidable to identify the core conditions, and the case elaboration was used to expand and recover this missing.
Conclusions
Main barriers of CCMM implementation among Chinese older couples were patients’ strong autonomy, low literacy, and mistrust between practitioners and older patients. This multicomponent intervention should be flexible, as interventions are most effective when they are tailored to older couples’ characteristics and literacy (either collaborative management or self-management). For collaborative management, the emphasis should be put on correct belief and perception about diabetes and the couple’s collective efficacy; while for patients preferred self-management, high-quality interventions to improve knowledge and skills of diabetes care would be essential. Our findings contribute to the development of tailored program to achieve better chronic disease management in older couples with different barriers.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CCMM:
-
Couple-based collaborative management model
- DMCCI:
-
Dyadic Model of Coping with Chronic Illness
- HbA1c:
-
glycated hemoglobin
- QCA:
-
qualitative comparative analysis
- RCT:
-
randomized controlled trial
- SCT:
-
Social Cognitive Theory
References
Gyawali B, et al. Community-based interventions for prevention of type 2 Diabetes in low- and middle-income countries: a systematic review. Health Promot Int. 2019;34(6):1218–30.
Plumb J, et al. Community-based partnerships for improving chronic Disease management. Prim Care. 2012;39(2):433–47.
the State Council, t.P.s.R.o.C. Notice on Further Optimizing the Prevention and Control Measures of the COVID-19 with Scientific Precision. 2022 [cited 2022 Dec 6th]; Available from: http://www.gov.cn/xinwen/2022-11/11/content_5726122.htm.
Rosland AM, Piette JD. Emerging models for mobilizing family support for chronic Disease management: a structured review. Chronic Illn. 2010;6(1):7–21.
Gilliss CL, Pan W, Davis LL. Family Involvement in Adult Chronic Disease Care: Reviewing the Systematic Reviews. 2019. 25(1): p. 3–27.
Cobb LK et al. Spousal influence on physical activity in middle-aged and older adults: the ARIC study. 2016. 183(5): p. 444–51.
Pereira MG, et al. Family and couple variables regarding adherence in type 2 Diabetes patients in the initial stages of the Disease. J Marital Fam Ther. 2019;45(1):134–48.
Shih D-P et al. Spousal concordance in dietary behaviors and metabolic components, and their association: a cross-sectional study. 2020. 12(11): p. 3332.
Liao J, et al. Couple-based collaborative management model of type 2 Diabetes Mellitus for community-dwelling older adults in China: protocol for a hybrid type 1 randomized controlled trial. BMC Geriatr. 2020;20(1):123.
Wichit N, et al. Randomized controlled trial of a family-oriented self-management program to improve self-efficacy, glycemic control and quality of life among Thai individuals with type 2 Diabetes. Diabetes Res Clin Pract. 2017;123:37–48.
Berg CA, Upchurch R. A developmental-contextual model of couples coping with chronic Illness across the adult life span. Psychol Bull. 2007;133:920–54.
Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31:143–64.
Li Q, et al. The development of a complex intervention in China: the ‘Caring for couples coping with Cancer 4Cs Programme’ to support couples coping with cancer. BMC Palliat Care. 2015;14:64.
Tankha H, et al. A novel couple-based intervention for Chronic Pain and Relationship Distress: a pilot study. Couple Family Psychol. 2020;9:13–32.
Coningsby I, Ainsworth B, Dack C. A qualitative study exploring the barriers to attending structured education programmes among adults with type 2 Diabetes. BMC Health Serv Res. 2022;22(1):584.
Griesemer I, et al. Developing a couple typology: a qualitative study of couple dynamics around physical activity. Transl Behav Med. 2020;10:751–9.
Hasson-Ohayon I, et al. Beyond being open about it: a systematic review on cancer related communication within couples. Clin Psychol Rev. 2022;96:102176.
Li Q, et al. Mutual support and challenges among Chinese couples living with Colorectal Cancer: a qualitative study. Cancer Nurs. 2018;41:E50–E60.
Helgeson VS, et al. Implications of supportive and unsupportive behavior for couples with newly diagnosed Diabetes. Health Psychol. 2016;35:1047–58.
Liao J, et al. Couple-based collaborative management model of type 2 Diabetes Mellitus for community-dwelling older adults in China: protocol for a hybrid type 1 randomized controlled trial. BMC Geriatr. 2020;20:123.
Warren J, Wistow J, Bambra C. Applying qualitative comparative analysis (QCA) in public health: a case study of a health improvement service for long-term incapacity benefit recipients. J Public Health (Oxf). 2014;36(1):126–33.
Furnari S, et al. Capturing Causal Complexity: Heuristics for Configurational Theorizing. The Academy of Management Review; 2020.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Fulton EA et al. StopApp: using the Behaviour Change Wheel to develop an app to increase uptake and attendance at NHS Stop Smoking Services. Healthc (Basel), 2016. 4(2).
Liu S, Liu J. Understanding behavioral intentions toward COVID-19 vaccines: theory-based content analysis of tweets. J Med Internet Res. 2021;23(5):e28118.
Musa S, et al. A qualitative interview study with parents to identify barriers and drivers to childhood vaccination and inform public health interventions. Hum Vaccin Immunother. 2021;17(9):3023–33.
Ragin CC. Redesigning Social Inquiry: fuzzy sets and Beyond. University of Chicago Press; 2008.
Diabetes Branch of Chinese Medical Association, Guidelines for the Prevention and Treatment od Type 2 Diabetes in China (. 2020 Edition). International Journal of Endocrinology and Metabolism, 2021. 41: p. 482–548.
Ragin CC. The comparative method: moving beyond qualitative and quantitative strategies. University of California Press; 1987.
Berg-Schlosser DGDM. Qualitative Comparative Analysis (QCA) as an Approach. Configurational comparative methods: qualitative comparative analysis (QCA) and related techniques. Thousand Oaks, California: SAGE Publications Inc; 2009.
Shiell A, Hawe P, Gold L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ. 2008;336:1281–3.
Speer J, Basurto X. Structuring the Calibration of Qualitative Data as Sets for Qualitative Comparative Analysis (QCA). Field Methods, 2010. 24.
Schokker MC, et al. Support behavior and relationship satisfaction in couples dealing with Diabetes: main and moderating effects. J Fam Psychol. 2010;24:578–86.
Randall MH, et al. The effect of remote patient monitoring on the primary care clinic visit frequency among adults with type 2 Diabetes. Int J Med Inform. 2020;143:104267.
Coningsby I, Ainsworth B, Dack C. A qualitative study exploring the barriers to attending structured education programmes among adults with type 2 Diabetes. BMC Health Serv Res. 2022;22:584.
Ong SE, et al. Assessing the influence of health systems on type 2 Diabetes Mellitus awareness, treatment, adherence, and control: a systematic review. PLoS ONE. 2018;13:e0195086.
Osborn CY, Bains SS, Egede LE. Health literacy, Diabetes self-care, and glycemic control in adults with type 2 Diabetes. Diabetes Technol Ther. 2010;12:913–9.
Beverly EA, Miller CK, Wray LA. Spousal support and food-related Behavior Change in Middle-aged and older adults living with type 2 Diabetes. 2008. 35(5): p. 707–20.
Howell BM, Peterson JR, Corbett S. Where are all the men? A qualitative review of the barriers, facilitators, and recommendations to Older Male Participation in Health Promotion Interventions. Am J Health Promot. 2023;37(3):386–400.
Zhao D, Zhao H, Cleary PD. Understanding the determinants of public trust in the health care system in China: an analysis of a cross-sectional survey. J Health Serv Res Policy. 2019;24(1):37–43.
Wu H, Hao J, Yang J. Study on the patient trust assessment and influencing factors in different level medical institutions in Beijing. Chin Hosp. 2018;22(02):26–9.
Xie Z, Qiu ZQ, Zhang TH. [Influence of patients’ attitude on doctors’ satisfaction with the doctor-patient relationship]. Beijing Da Xue Xue Bao Yi Xue Ban. 2009;41(2):141–3.
Lee YK, Lee PY, Ng CJ. A qualitative study on healthcare professionals’ perceived barriers to insulin initiation in a multi-ethnic population. BMC Fam Pract. 2012;13:28.
Trief PM, et al. Health and Psychosocial outcomes of a telephonic couples behavior change intervention in patients with poorly controlled type 2 Diabetes: a Randomized Clinical Trial. Diabetes Care. 2016;39:2165–73.
Mayberry LS, Osborn CY. Family support, medication adherence, and glycemic control among adults with type 2 Diabetes. Diabetes Care. 2012;35:1239–45.
Conghui Yang YX, Zhi J, Ma Y, Wu X. Jing Liao Can couple-based intervention improve older Diabetes patients’ attendance of health education: an examination on intervention process outcome of a multicentered randomized controlled trial. BMC public health, under review.
Carroll C, et al. A conceptual framework for implementation fidelity. Implement Science: IS. 2007;2:40–0.
Martire LM, Stephens MA, Schulz R. Independence centrality as a moderator of the effects of spousal support on patient well-being and physical functioning. Health Psychol. 2011;30:651–5.
Nah S, Martire LM, Zhaoyang R. Perceived Gratitude, Role overload, and Mental Health among Spousal caregivers of older adults. J Gerontol B Psychol Sci Soc Sci, 2021.
Acknowledgements
Not applicable.
Funding
This research was funded by the National Natural Science Foundation of China (Grants 71804201 and 72061137003).
Author information
Authors and Affiliations
Contributions
J.L. designed the study, contributed to discussion, and reviewed and edited the manuscript. J.Z. and C.H.Y. researched data, contributed to discussion, and wrote and edited the manuscript. Y.X.L. contributed to discussion, and edited the manuscript. D.D.W. and L.R.L. and contributed to discussion and reviewed the manuscript. H.Q.Z. and D.X. reviewed the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Sun Yat-sen University (2019-064). Informed consent was obtained from all the participants. All methods were carried out in accordance with the guidelines of the Declaration of Helsinki, and no report allowed any individual participant to be identified.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1:
Interview outline
Supplementary Material 2:
Qualitative comparative analysis (QCA) analysis steps
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, J., Yang, C., Liu, Y. et al. Conditions for successful implementation of couple-based collaborative management model of diabetes among community-dwelling older Chinese: a qualitative comparative analysis. BMC Geriatr 23, 832 (2023). https://doi.org/10.1186/s12877-023-04565-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04565-y