
Abstract
Background
To achieve the best treatment of heart failure, it is important to use all recommended drugs at their target doses. Given that underuse of medications can occur in individuals with cognitive impairment, we investigated the filled prescriptions and target doses of heart failure medication for older individuals with and without cognitive impairment as well as associated factors.
Methods
The study was based on two separate datasets. The first dataset, which was based on data from questionnaires sent to nursing homes in Sweden, included 405 individuals with heart failure. The data were linked with the Swedish Prescribed Drug Register and the National Patient Register to obtain information regarding filled prescriptions of heart failure medications and heart failure diagnoses among the population. In the second dataset, medical records of individuals aged 75 years or older admitted to a hospital in northern Sweden were reviewed and individuals with heart failure were identified. Target doses of heart failure medications were evaluated in 66 individuals who lived at home.
Results
Filled prescriptions of mineralocorticoid receptor antagonists and loop diuretics were significantly more common in individuals without cognitive impairment (OR 1.087; 95% CI 1.026–1.152, p < 0.05) and (OR 1.057; 95% CI 1.017–1.098, p < 0.05), respectively. There were no significant differences between individuals with and without cognitive impairment in terms of achieving target doses for any of the drug classes. A higher age was associated with fewer filled prescriptions and less ability to reach the target doses of beta blockers (OR 0.950; 95% CI 0.918–0.984, p < 0.05) and (OR 0.781; 95% CI 0.645–0.946, p < 0.05), respectively.
Conclusions
Our results suggest that individuals with cognitive impairment are partly undertreated for heart failure in that they had fewer filled prescriptions of important heart medications. Separately, the relatively low proportion of older individuals reaching target doses is an important observation and indicates that treatment of heart failure could be further optimised among older individuals.
Similar content being viewed by others


Background
Heart failure is a disease that leads to high mortality and a decreased quality of life. Depending on the definition of heart failure, its prevalence is ~ 10% among people 70 years or older in developed countries. However, significant advances have been made in its treatment in recent years and the pharmacological guidelines have been revised [1, 2]. Pharmacological treatment with an angiotensin converting enzyme inhibitor (ACEI), a beta blocker (BB), and a mineralocorticoid receptor antagonist (MRA) have a class I recommendation for all individuals with heart failure with reduced ejection fraction (HFrEF) or with mildly reduced ejection fraction (HFmrEF), with New York Heart Association (NYHA) II–IV [1]. In 2021, sodium-glucose transport protein 2 (SGLT2)-inhibitors also received a class I recommendation for individuals with HFrEF, NYHA II–IV. For individuals with persistent symptoms, ACEI is recommended to be replaced with an angiotensin receptor-neprilysin inhibitor (ARNI). For individuals who do not tolerate ACEI or ARNI, an angiotensin receptor blocker (ARB) is recommended.
Both ACEI and BB reduce mortality and hospitalisation caused by heart failure and reduce the symptoms compared with a placebo in individuals with heart failure [3,4,5,6]. ACEI has also shown positive effects on quality of life in this population [4]. The addition of MRA further reduces hospitalisation due to heart failure and decreases mortality [7]. SGLT2 inhibitors can further reduce cardiovascular mortality [8]. ARNI has recently been recommended to replace ACEI before the use of an ARB because ARNI can reduce total mortality in contrast to ARB [1, 9, 10]. ARNI, like ACEI, also has positive effects on quality of life [9]. Besides these drugs with a class I recommendation, loop diuretics, ivabradine, or digoxin can be added for individuals with persistent symptoms of heart failure [1]. Diuretics improve exercise tolerance and decrease hospitalisations due to heart failure [11], ivabradine decreases the combined measures of cardiovascular mortality and hospitalisations due to heart failure [12], and digoxin reduces the risk for hospitalisation due to heart failure [13].
The use of two or more drug classes with class I recommendation is associated with an additive effect in reducing mortality and decreasing rates of rehospitalisation in individuals with heart failure, according to a meta-analysis [14]. In addition to the importance of the number of heart failure medications prescribed, reaching the target doses of heart failure medications is recommended to achieve the maximum effect of the drugs. Previous studies have found that many patients with heart failure do not reach the target doses of their prescribed drugs [15, 16]. Target doses of ACEI/ARB and BB were prescribed for 25–69% of individuals with heart failure according to one study [15], while another study found that only 33–35% of individuals with heart failure with BB prescriptions achieved their target dose [16]. However, the population with HFrEF has become larger and older and is at higher risk for adverse events. Many of the studies performed regarding heart failure treatment have also excluded multimorbidity and frail individuals, thereby limiting the evidence for this population [17].
The risk for cognitive impairment increases with age [18]. In addition, there is a comorbidity between heart failure and cognitive impairment. According to a meta-analysis of 4,176 individuals with heart failure, 43% had cognitive impairment as a comorbidity [19]. Previous studies have found that individuals with cognitive impairment are undertreated for some cardiovascular diseases [20, 21] and that individuals with concomitant heart failure and cognitive impairment have a high risk of drug-related hospital admissions [22].
To achieve the optimal treatment of heart failure, it is important to use all the recommended drugs and to reach the target doses of these drugs. Given that undertreatment occurs in individuals with cognitive impairment, we evaluate whether there are differences in the prescription of drugs for heart failure between those with and without cognitive impairment.
Aim
The first aim of this study was to investigate the filled prescriptions of each drug class of heart failure medication in individuals with and without cognitive impairment. The second aim was to evaluate any possible differences between individuals with and without cognitive impairment in terms of whether they reached the target doses of their heart failure medications. A third aim was to investigate factors associated with filled prescriptions and target doses.
Methods
This study was based on two separate datasets. The first dataset (dataset 1) was based on a survey and included older individuals living in nursing homes. The second dataset (dataset 2) was based on a randomised controlled study, and the population included older individuals living at home. The different populations are described below.
Data based on a survey
Dataset 1 was based on a survey from the Swedish National Inventory of Care and Health in Residential Aged Care (SWENIS), which was sent randomly to a nationally representative sample of nursing homes in Sweden in 2018–2019. A total of 315 nursing homes were contacted for participation, and 235 agreed to participate. In total, 7073 questionnaires were sent to these 235 nursing homes, and the final sample included 3894 residents (response rate of 55%) from 187 nursing homes. The surveys were completed by staff at the nursing home who had the best knowledge of individuals. The survey included, for example, questions regarding demographic information, quality of life according to EuroQuol five dimension (EQ-5D) [23], assessments of functioning in the activities of daily living (ADL) [24], and cognition. Cognitive function was classified according to Gottfries’ cognitive scale with 27 items, where a score < 24 is classified as cognitive impairment [25]. This correlates with 90% sensitivity and 91% specificity [24] to the cut-off of 24/30 used in the Mini-Mental State Examination [26].
In the present study, the data from the survey were linked with the Swedish Prescribed Drug Register, the Swedish Cause of Death Registry, and the National Patient Register through personal identity numbers to obtain information regarding heart failure medications and heart failure diagnoses among the population.
Study population
Of the 3894 individuals who completed and returned the questionnaires, 2771 individuals had complete personal identity numbers and could be linked to the Swedish Prescribed Drug Register. Data regarding filled prescriptions for heart failure medication were collected for the period January 01–June 30, 2019. The Swedish Cause of Death Register was used to select individuals alive on June 30, 2019. Of the 2479 living individuals, those with heart failure according to International Classification of Diseases ICD-10 code I50 [27] were selected. A total of 411 individuals had a heart failure diagnosis, but 6 individuals who did not have their cognitive function graded were excluded from the study, and thus 405 individuals were included in the analysis.
Definitions
Drug use was defined as one or more filled prescriptions during a 6-month timeframe. Drugs included in the analysis were agents acting on the renin-angiotensin system (Anatomical Therapeutic Chemical (ATC) classification C09), recommended BBs at heart failure (bisoprolol, carvedilol, and metoprolol) [1], MRA (C03DA), loop diuretics (C03C), digoxin (C01AA05), and ivabradine (C01EB17). SGLT2-inhibitors were not included in the analysis because the recommendation was not yet introduced during the inclusion period for dataset 1 and for most of the time of dataset 2.
Data based on an ongoing randomised controlled study
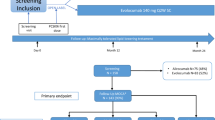
Dataset 2 was based on an ongoing randomised controlled study of 700 individuals in the University Hospital in Umeå [28]. The study included individuals ≥ 75 years old living at home, listed at predefined health care units, and hospitalised at an emergency medical ward or an orthopaedic ward. During the first interview at the ward, each individual was classified by cognitive function according to a shortened four-item version of Gottfries’ cognitive scale [28, 29]. A score < 3 was classified as cognitive impairment. Medication adherence according to the Medication Adherence Report Scale (MARS-5) [30] and quality of life according to the EQ-5D were also assessed during the first interview. The individuals were randomised to the intervention group or control group when discharged from the hospital [28]. The intervention group received an extensive clinical pharmacy service for 180 days including medication reconciliation every second week and medication phone interviews at 7, 30, and 60 days after discharge from the hospital. The pharmacists discussed drug related problems with the primary care physician. The control group received standard care, including medication reviews at the ward from a clinical pharmacist. The primary aim was to investigate whether the intervention during the transition from hospital care to primary care could reduce the risk of drug-related hospital readmission within 180 days after discharge from the hospital. The inclusion of the individuals started in September 2018 and is still ongoing.
Study population
In the present study, the first 271 individuals from both the intervention and control group were included (2018-09-20 through 2021-09-14). Of these 271 individuals, those diagnosed with heart failure and at least one of following prescribed drugs were analysed: agents acting on the renin-angiotensin system (ATC classification C09), BBs recommended at heart failure (bisoprolol, carvedilol, and metoprolol), and MRA (C03DA). To exclude people with heart failure with preserved ejection fraction, (HFpEF) one inclusion criteria was to have at least one heart failure drug prescribed. Heart failure diagnosis was identified by ICD-I50 or notes of heart failure diagnosis in the medical record. Only individuals who already had a heart failure diagnosis on the day of admission were included in the study because the analysed medication lists were the individuals’ current medications at the time of admission to the hospital. Of the 271 individuals, 70 had a heart failure diagnosis at admission, and 68 of these individuals had at least one of the above-mentioned drugs prescribed. The exclusion criterion was individuals with a diagnosis of right ventricular failure with preserved left ventricular function. Two of the 68 individuals were excluded according to this criterion. Thus, 66 individuals were included in the current analysis.
Definitions
Information about the population was obtained from the medical records and included the individuals’ medication list when included in the previous study, laboratory values, admission notes, doctors notes, and discharge summary. Any readmission note was not analysed. The medication lists at inclusion to the study, i.e., at admission to hospital, were analysed according to whether the individual had reached the target doses of the prescribed drugs. Target doses for the medications were analysed according to European Society of Cardiology (ESC) guidelines [1, 2, 31]. For MRA, target doses according to Västerbotten County Council’s guidelines were used. Target doses were analysed for drugs with ATC classification C09 (captopril, enalapril, lisinopril, ramipril, candesartan, losartan, and sacubitril/valsartan), C07 (bisoprolol, carvedilol, and metoprolol), and C03DA (eplerenone and spironolactone). Target doses of the analysed drugs are presented in Supplementary Table S1.
For individuals who did not reach target doses, laboratory values and notes from the medical record were analysed to identify any possible reason for not reaching the target dose. The values analysed were renal function, potassium level, heart rate, blood pressure, and other apparent contraindications for the drugs. In cases where possible information regarding contraindications was missing from the notes, the following thresholds were used: a relative estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73 m2 or a serum potassium level of > 5.5 mmol/L were classified as a possible reason for not reaching target dose of ACEI/ARB/ARNI and MRA [32], a heart rate < 60 was classified as a possible reason for not reaching target doses of BB [33], and a systolic blood pressure of < 90 mmHg [34] or an orthostatic blood pressure (defined as ≥20 fall in systolic pressure or ≥10 mmHg in diastolic pressure with standing) [35] was classified as a possible reason for not reaching the target dose of any of the drugs.
Statistics
To analyse if there was a difference between individuals with and without cognitive impairment and drug use, a chi-squared test was used for both datasets. To adjust for other factors associated with drug use, multiple logistic regression models were constructed in both datasets. In dataset 1, filled prescriptions of each drug class was the dependent variable. The independent variables were cognitive function (Gottfries’ cognitive scale as a continuous variable), sex, age, EQ-5D, and ADL dependency. In the multiple regression model in dataset 2, the achieved target dose of each drug class was the dependent variable. The independent variables were cognitive function (the short version of Gottfries’ cognitive scale as a dichotomous variable), sex, age, and EQ-5D. For ACEI/ARB/ARNI and MRA, the potassium level and relative eGFR were also independent variables in dataset 2. Relative eGFR was estimated using the Chronic Kidney Disease Epidemiology Collaboration equation [36]. The statistical program used was Statistical Package for the Social Sciences for Windows, Version 25. We considered p-values < 0.05 significant for all statistical tests, and odds ratios were calculated with 95% confidence intervals.
Results
The basic characteristics of the populations are presented in Table 1. In dataset 1, 405 individuals were included. More than half of the individuals were women, and the mean age was 86.8 years. Of the included individuals, 55% had cognitive impairment according to Gottfries’ cognitive scale, and the mean score was 20.0. In dataset 2, 66 cases were included in the analysis with a mean age of 86.0 years. Of these, 37 were women and 30% had a cognitive impairment classification according to the short version of Gottfries’ cognitive scale.
BB and loop diuretics were the most common drug classes in dataset 1 in both individuals with and without cognitive impairment (Table 2). BB, MRA, and loop diuretics were all significantly more common in individuals without cognitive impairment. For agents acting on the renin-angiotensin system and digoxin, no significant differences were observed between the groups. None of the individuals had ivabradine as a filled prescription. When adjusting for different factors, the association with cognitive impairment was significant only for MRA and loop diuretics. There was also a significant association between lower age and filled prescriptions of BB. All results from the multiple logistic regression analysis from dataset 1 are shown in Table 3.
Of the population in dataset 2, 91% were prescribed a BB, 80% percent were prescribed an ACEI/ARB/ARNI, and 41% were prescribed an MRA (Table 4). Of all individuals included in dataset 2, 79% had at least two of the drug classes prescribed, and one-third had all three drug classes prescribed. In Table 4, the proportions of individuals reaching target doses are also presented. In total, 12 individuals reached target doses of ACEI/ARB/ARNI, 9 individuals reached target doses of BB, and 18 individuals reached target doses of MRA. In terms of percentages, most individuals were able to reach target doses of eplerenone, ramipril, and spironolactone. None of the individuals reached target doses of losartan, sacubitril/valsartan, or carvedilol. There were no significant differences in reaching target doses for any of the drug classes between individuals with and without cognitive impairment according to the chi-squared test.
The multiple logistic regression analysis in dataset 2 showed that the only significant association was between younger age and reaching the target dose of BB (Table 5).
Of the 41 individuals who did not reach target doses of ACEI/ARB/ARNI, possible reasons were identified in 12 cases. In 8 cases, the renal function was below 30 mL/min/1.73 m2), and therefore a possible reason for not reaching target doses was due to decreased renal function. One of these eight individuals had decreased renal function in combination with a high serum potassium level. Four of the individuals where a possible reason was found had hypotension or orthostatic hypotension. Of the 29 remaining individuals, no possible reason was identified.
In those with BB prescriptions, 51 individuals did not reach target doses. Possible reasons were found in seven of these individuals. Of these seven, five had hypotension or orthostatic hypotension and two had bradycardia. No possible reasons why target doses were not achieved were identified in the 44 remaining individuals.
Of the nine individuals who did not achieve the target dose of MRA, a reason was identified for only one individual, which was orthostatic hypotension.
Discussion
In this study we found that individuals with cognitive impairment were less likely to receive MRA and loop diuretics. Further, there were no significant differences in reaching target doses for any of the drug classes between individuals with and without cognitive impairment. A higher age was associated with fewer filled prescriptions and less ability to reach target doses of BBs.
Undertreatment of individuals with cognitive impairment was observed in previous research [20, 21], but in the present study undertreatment was not observed with ACEI/ARB/ARNI, BB, or digoxin. The prescription of ACEI/ARB/ARNI and BB to individuals with cognitive impairment might have increased during recent years. A previous study found that cognitive impairment was associated with under-prescription of ACE/ARB and BB in 2007, but between 2007 and 2013 an improvement in treatment with these drugs in individuals with cognitive impairment was observed [37]. However, no significant difference in MRA prescription was observed in this population during this period. One possible reason for the difference between these drug groups could be that physicians are somewhat more restrictive in prescribing according to the latest recommendations for individuals with cognitive impairment. Agents that affect the renin-angiotensin system and BB have been recommended as class I recommendations for heart failure for several years [38, 39], but immediate prescription of both MRA, SGLT2 inhibitors, agents that affect the renin-angiotensin system, and BB was not implemented in ESC guidelines until 2021 [1, 2]. In the guidelines from 2016, prescription of MRA was only recommended if the individual still had symptoms or still had an ejection fraction ≤ 35% despite treatment with agents that affect the renin-angiotensin system and BB [2]. The other group of drugs that individuals without cognitive impairment more often received in this study was loop diuretics. This is somewhat surprising because loop diuretics might be prescribed more for individuals with insufficient treatment of heart failure to improve their symptoms. One possible explanation for this might be that individuals without cognitive impairment might be more likely to report symptoms and request symptomatic treatment.
In the present study, no significant differences in reaching target doses were seen between individuals with and without cognitive impairment. The study population may be too small, and even if there was a true difference between individuals with and without cognitive impairment, the number of individuals may be too limited to detect it. What we found in this study, however, was that a relatively low proportion of the individuals reached target doses of heart failure medications. In the relatively few cases where a reason for not achieving a target dose was identified, the most common was decreased renal function for ACEI/ARB/ARNI and hypotension/orthostatic hypotension for BB and MRA. Another possible reason for not reaching target doses of heart failure medications is treatment with other blood pressure lowering agents, such as calcium channel blockers [1], which lower the blood pressure and give less ability to increase the dose of heart failure medication. Additionally, a clinician’s definition of hypotension as a contraindication to reaching target dosing is likely higher than the definition used in this study (< 90 mmHg). In the present study, other blood pressure-lowering agents were not included in the analyses. Target doses of MRA and of ACEI/ARB/ARNI were achieved in 67% and 23% of the individuals, respectively, but regarding BB, target doses were only achieved in 15% of the individuals, which was lower than what was determined in a previous study [16]. The regression analyses in the present study showed that older individuals were not as likely to have a filled prescription of BB or to reach target doses of BB. This is consistent with earlier research [37, 40]. However, a previous study found that BBs decrease mortality in older individuals regardless of dose, but more research is needed to confirm this [41]. A probable reason for under-prescribing BBs to older individuals are the adverse effects, such as bradycardia and orthostatic hypotension, associated with these drugs [42, 43]. The prescribing physicians might therefore be more cautious about prescribing BB and increasing doses for older individuals. In addition, older individuals are generally underrepresented in clinical trials of heart failure medications, and the reduced risk in mortality is not as established as in younger individuals [17]. However, a benefit of receiving a BB after admission in terms of reduced rehospitalisations and mortality in individuals ≥ 75 years with heart failure was observed in one study [17]. Considering the adverse effects associated with these drugs, it is important to carefully follow-up the individual’s response to treatment. Nevertheless, the results show that the treatment of heart failure could be further optimised among older individuals.
No other factor than age was associated with reaching target doses in the regression analysis. Surprisingly, there was no found association between target doses of ACEI/ARB/ARNI and a lower eGFR. The use of these drugs in individuals with severely reduced renal function may cause undesirable outcomes such as hyperkalemia [44]. Although decreased renal function was identified as one reason for not reaching target doses, the study population may be too small to detect an association.
A major limitation to this study is that detailed heart failure diagnoses were missing in both datasets. We do not know if the diagnoses were based on echocardiography, and especially older people might receive the diagnosis of heart failure without objective findings. In dataset 1, all individuals with heart failure according to ICD-10 code I50 were included [27]. It would be more desirable to include only individuals with NYHA II-IV and HFrEF or HFmrEF because these are the individuals with indications for heart failure medications [1]. The broader group in dataset 1 has implications for the findings in this study. Further, we had no data regarding frailty, which might have affected the prescription of drugs. Also, if a major neurocognitive disorder (NCD) diagnosis had been used instead of Gottfries’ cognitive scale to identify people with and without cognitive impairment, the results may have been different. Gottfries’ cognitive scale was used in the present study to also include those people who suffer from cognitive impairment but have not yet received a major NCD diagnosis.
For MRA, a lower target dose was recommended in Region Västerbotten’s guidelines compared with ESC [1, 31]. For these drugs, Region Västerbotten’s target doses were used because most of the individuals had the drugs prescribed in this region. SGLT2 inhibitors were introduced to all individuals with heart failure NYHA II-IV and HFrEF or HFmrEF in the ESC guidelines for heart failure in 2021 [1, 2]. Because the recommendation was not yet introduced during the inclusion period in dataset 1 or for most of the time in dataset 2, this drug class was not included in the analysis.
In dataset 2, relative eGFR is used to find possible reasons for why individuals did not reach target doses. For drug dosing, absolute eGFR is recommended because it is a more accurate estimation of an individual’s renal function [45]. To estimate absolute eGFR, information regarding weight and height is necessary, and in most cases this information was missing. For ACEI/ARB/ARNI, decreased renal function is not an absolute contraindication for target doses of these drugs. In our analysis, a limit of eGFR < 30 mL/min/1.73 m2 was used as a possible reason for not reaching target doses. This, in combination with relative eGFR instead of absolute eGFR, is a limitation in explaining why individuals did not reach target doses. Another limitation in the present study is that the values of eGFR, potassium levels, heart rate, and blood pressure were non-recurring values. Further, a systolic blood pressure of < 90 mmHg used as a definition in this study is not adapted for an elderly person with cognitive impairment. In analysing the possible reasons for not reaching target doses, the number of individuals was too small to evaluate possible differences between individuals with and without cognitive impairment.
Conclusions
This study found that filled prescriptions of MRA and loop diuretics were significantly less common in individuals with cognitive impairment. No difference regarding cognitive impairment was observed in terms of reaching target doses, but a higher age was associated with fewer filled prescriptions and less ability to reach the target doses of BBs. Our results suggest that individuals with cognitive impairment are partly undertreated for heart failure. The relatively low proportion of individuals reaching target doses is an important observation and indicates that the treatment of heart failure could be further optimised among older individuals.
Data Availability
The datasets used and/or analysed during the current study are not publicly available since it contains personal sensitive data, in accordance to the EU’s data protection regulation, General Data Protection Regulation (GDPR), but are available from the corresponding author on reasonable request.
Abbreviations
- ACEI:
-
angiotensin converting enzyme inhibitor
- ADL:
-
activity of daily living
- ARB:
-
angiotensin receptor blocker
- ARNI:
-
angiotensin receptor-neprilysin inhibitor
- ATC classification:
-
Anatomical Therapeutic Chemical classification:BB:beta blocker
- CI:
-
confidence interval
- EQ-5D:
-
quality of life according to EuroQuol five dimension
- ESC:
-
European Society of Cardiology
- HFmrEF:
-
heart failure with mildly reduced ejection fraction
- HFrEF:
-
heart failure with reduced ejection fraction
- MARS-5:
-
Medication Adherence Report Scale
- MRA:
-
mineralocorticoid receptor antagonist
- NCD:
-
neurocognitive disorder
- NYHA:
-
New York Heart Association
- OR:
-
odds ratio
- SWENIS:
-
Swedish National Inventory of Care and Health in Residential Aged Care
References
McDonagh TA, Metra M, Adamo M, ESC Scientific Document Group., 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC, European Heart Journal, 2021;42(36):3599–3726. https://doi.org/10.1093/eurheartj/ehab368.
Ponikowski P, Voors AA, Anker SD, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the heart failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18:891–975. https://doi.org/10.1002/ejhf.592.
Swedberg K, Kjekshus J. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). Am J Cardiol. 1988;62(2):60A–6. https://doi.org/10.1016/s0002-9149(88)80087-0. PMID: 2839019.
Packer M, Poole-Wilson PA, Armstrong PW, et al. Comparative effects of low and high doses of the angiotensin-converting enzyme inhibitor, lisinopril, on morbidity and mortality in chronic heart failure. ATLAS Study Group Circulation. 1999;100:23122318.
Packer M, Coats AJ, Fowler MB, et al. Carvedilol prospective randomized cumulative survival Study Group. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med. 2001;344:1651–8.
Flather MD, Shibata MC, Coats AJ, et al. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J. 2005;26:215–25.
Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized aldactone evaluation study investigators. N Engl J Med. 1999;341:709–17.
McMurray JJV, Solomon SD, Inzucchi SE, et al. DAPA-HF Trial Committees and Investigators. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381:1995–2008.
McMurray JJ, Packer M, Desai AS, et al. PARADIGM-HF Investigators Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371:993–1004.
Granger CB, McMurray JJ, Yusuf S, et al. CHARM investigators and committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trial. Lancet. 2003;362:772–6.
Faris R, Flather M, Purcell H et al. Current evidence supporting the role of diuretics in heart failure: a meta analysis of randomised controlled trials. Int J Cardiol. 2002;82(2):149–58. https://doi.org/10.1016/s0167-5273(01)00600-3. PMID: 11853901.
Swedberg K, Komajda M, Bohm M, et al. SHIFT investigators. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet. 2010;376:875–85.
Abdul-Rahim AH, Shen L, Rush CJ, et al. VICCTA Heart failure collaborators. Effect of digoxin in patients with heart failure and mid-range (borderline) left ventricular ejection fraction. Eur J Heart Fail. 2018;20:1139–45.
El Hadidi S, Darweesh E, Byrne S, et al. A tool for assessment of heart failure prescribing quality: a systematic review and meta-analysis. Pharmacoepidemiol Drug Saf. 2018;27(7):685–94. https://doi.org/10.1002/pds.4430.
Crissinger ME, Marchionda KM, Dunlap ME. Adherence to clinical guidelines in heart failure (HF) outpatients: impact of an interprofessional HF team on evidence-based medication use. J Interprof Care. 2015;29(5):483–7. https://doi.org/10.3109/13561820.2015.1027334.
McCarren M, Furmaga E, Jackevicius CA, et al. Improvement of guideline β-blocker prescribing in heart failure: a cluster-randomized pragmatic trial of a pharmacy intervention. J Card Fail. 2013;19(8):525–32. https://doi.org/10.1016/j.cardfail.2013.06.004.
Gilstrap L, Austin AM, O’Malley AJ, et al. Association between Beta-Blockers and Mortality and Readmission in older patients with heart failure: an instrumental variable analysis. J Gen Intern Med. 2021;36(8):2361–9. https://doi.org/10.1007/s11606-021-06901-7.
Heckman GA, Patterson CJ, Demers C, et al. Heart failure and cognitive impairment: challenges and opportunities. Clin Interv Aging. 2007;2:209–18.
Cannon JA, Moffitt P, Perez-Moreno AC, et al. Cognitive impairment and heart failure: systematic review and Meta-analysis. J Card Fail. 2017;23(6):464–75. https://doi.org/10.1016/j.cardfail.2017.04.007.
Lopponen M, Raiha I, Isoaho R, et al. Dementia associates with undermedication of cardiovascular diseases in the elderly: a population-based study. Dement Geriatr Cogn Disord. 2006;22:132–41. https://doi.org/10.1159/000093739.
Klarin I, Fastbom J, Wimo A. A population-based study of drug use in the very old living in a rural district of Sweden, with focus on cardiovascular drug consumption: comparison with an urban cohort. Pharmacoepidemiol Drug Saf. 2003;12:669–78. https://doi.org/10.1002/pds.878.
Gustafsson M, Sjölander M, Pfister B, et al. Pharmacist participation in hospital ward teams and hospital readmissions rates among people with dementia - a randomized controlled trial. Eur J Clin Pharmacol. 2017;73(7):827-835. https://doi.org/10.1007/s00228-017-2249-8.
Burström K, Johannesson M, Diderichsen F. Swedish population health-related quality of life results using the EQ-5D. Qual Life Res. 2001;10:621–35.
Sandman PO, Adolfsson R, Norberg A, et al. Long-term care of the elderly. A descriptive study of 3600 institutionalized patients in the county of Vasterbotten, Sweden. Compr Gerontol A. 1988;2:120–32.
Adolfsson R, Gottfries CG, Nystrom L, et al. Prevalence of dementia disorders in institutionalized swedish old people. The work load imposed by caring for these patients. Acta Psychiatr Scand. 1981;63:225–44.
Folstein MF, Folstein SE, McHugh PR. Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–98.
World Health Organization (WHO). International Statistical Classification of Diseases and Related Health Problems (ICD-10). 10th Revision. 2019. [cited 2022-05-18]. https://icd.who.int/browse10/2019/en#/I50.0.
Kindstedt J, Svahn S, Sjölander M, et al. Investigating the effect of clinical pharmacist intervention in transitions of care on drug-related hospital readmissions among the elderly: study protocol for a randomised controlled trial. BMJ Open. 2020;10:e036650. https://doi.org/10.1136/bmjopen-2019-036650.
Lövheim H, Gustafsson M, Isaksson U, et al. Gottfries’ cognitive scale for staff proxy rating of cognitive function among nursing home residents. J Alzheimers Dis. 2019;72:1251–60.
Mahler C, Hermann K, Horne R, et al. Assessing reported adherence to pharmacological treatment recommendations. Translation and evaluation of the Medication Adherence Report Scale (Mars) in Germany. J Eval Clin Pract. 2010;16(3):574–9. https://doi.org/10.1111/j.1365-2753.2009.01169.x.
Västerbottens County Councils guidelines. (2022). https://regionvasterbotten.se/for-vardgivare/behandlingsstod-och-vardriktlinjer/lakemedel/behandlingsrekommendationer/terapirekommendationer.
Janusinfo. Cardiovascular therapy area. Assessed 2022-05-12. https://klokalistan.se/terapiomrade/hjarta-och-karl.html.
Mayo Clinic. Bradycardia. Assessed 2022-05-12. https://www.mayoclinic.org/diseases-conditions/bradycardia/symptoms-causes/syc-20355474#:~:text=If%20you%20have%20bradycardia%2 C%20your,weak%2 C%20and%20short%20of%20breath.
National Health Service., NHS. Low blood pressure (hypotension). England. Assessed 2022-05-12. https://www.nhs.uk/conditions/low-blood-pressure-hypotension/.
Gaieski D, Mikkelsen M, UpToDate. Evaluation of and initial approach to the adult patient with undifferentiated hypotension and shock. Topic 98976, version 32.0. [updated 2022-05-09; cited 2022-05-12]. https://www.uptodate.com/contents/evaluation-of-and-initial-approach-to-the-adult-patient-with-undifferentiated-hypotension-and-shock?search=hypotension%20%20&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2.
Jones GRD. Estimating renal function for drug dosing decisions. Clin Biochem Rev. 2011;32(2):81–8.
Svahn S, Lövheim H, Isaksson U, et al. Cardiovascular drug use among people with cognitive impairment living in nursing homes in northern Sweden. Eur J Clin Pharmacol. 2020;76(4):525–37. https://doi.org/10.1007/s00228-019-02778-y.
Dickstein K, Cohen-Solal A, ESC Committee for Practice Guidelines (CPG), et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the diagnosis and treatment of Acute and Chronic Heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the heart failure association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. 2008;29(19):2388–442. https://doi.org/10.1093/eurheartj/ehn309.
McMurray JJ, Adamopoulos S, Anker SD, ESC Committee for Practice Guidelines, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the diagnosis and treatment of Acute and Chronic Heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the heart failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14(8):803–69. https://doi.org/10.1093/eurjhf/hfs105.
Fu M. Beta-blocker therapy in heart failure in the elderly. Int J Cardiol. 2008;10(2):149–53. https://doi.org/10.1016/j.ijcard.2007.10.010.
Franco Peláez JA, Cortés García M, et al. Relationship between different doses of beta-blockers and prognosis in elderly patients with reduced ejection fraction. Int J Cardiol. 2016;1:220:219–25. https://doi.org/10.1016/j.ijcard.2016.06.178.
Bolon J, McCutcheon K, Klug E, et al. Beta-blocker target dosing and tolerability in a dedicated heart failure clinic in Johannesburg. Cardiovasc J Afr. 2019;23(2):103–7. https://doi.org/10.5830/CVJA-2019-001.
Cremer A, Boutouyrie P, Laurent S, et al. Orthostatic hypotension: a marker of blood pressure variability and arterial stiffness: a cross-sectional study on an elderly population: the 3-City study. J Hypertens. 2020;38(6):1103–9. https://doi.org/10.1097/HJH.0000000000002374.
Weir MR, Lakkis JI, Jaar B, et al. Use of Renin-Angiotensin System Blockade in Advanced CKD: an NKF-KDOQI Controversies Report. Am J Kidney Dis. 2018;72(6):873–84. https://doi.org/10.1053/j.ajkd.2018.06.010.
Swedish Agency for Health Technology Assessment and Assessment of Social Services. Estimate of Renal Function. A systematic literature review. SBU. ; 2012. Assessed 2022-05-09. https://www.sbu.se/contentassets/8f432cbce7ad454dbf3040627371951a/njurfunktion_141110.pdf.
Acknowledgements
We thank the nursing home staff and managers for taking the time to complete these surveys and participate in this research. This study received financial support from the Swedish Research Council for Health, Working Life and Welfare: FORTE (2014–4016) and (2017 − 01438), the Swedish Research Council (521-2014-2715) and (2019 − 01078), Region Västerbotten, the Swedish Society of Medicine, and the Umeå University Foundation for Medical Research. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Funding
Open access funding provided by Umea University. The authors have no relevant financial or non-financial interests to disclose.
Author information
Authors and Affiliations
Contributions
DE, AB, HL, LA, and MG contributed to the study conception and design. Material preparation and data collection were performed by DE, AB, HL, LA, and MG. Statistical analyses were performed by LA and MG. The first draft of the manuscript was written by LA, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Regarding dataset 1, informed consent was obtained from all subjects and/or their legal guardian(s) using an opt-out procedure in accordance with the Swedish Ethical Review Law. Written information was provided to all participants and posters with information about the study was available by the entrance of the nursing homes. Residents and their relatives could decline to participate in the study. Ethical approval was obtained from the Swedish Regional Ethical Review Board (Dnr 2018/145 − 31). Regarding dataset 2, people who fulfilled the inclusion criteria were given oral and written information about the study, and informed consent was obtained from those who wished to participate. Anyone who did not wish to participate was free to decline or withdraw at any time during the trial. In Sweden, the Ethical Review Law permits research involving persons with cognitive impairment under certain conditions, even though they cannot give a full informed consent. Individuals with major NCD participated without formal written informed consent, although in these cases both the intended participant and the next of kin were informed about the study and were given the opportunity to decline participation. This procedure of informing the intended participant and next of kin is approved by the Regional Ethical Review Board in Umeå, Sweden, registration number Dnr 2017-69-31 M, 2018-83-32 M, and 2018-254-32 M). All methods were carried out in accordance with the Helsinki declaration.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abramsson, L., Backman, A., Lövheim, H. et al. Use of heart failure medications in older individuals and associations with cognitive impairment. BMC Geriatr 23, 524 (2023). https://doi.org/10.1186/s12877-023-04223-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04223-3