
Abstract
Background
Falls are common among older people in long-term care facilities (LTCFs). Falls cause considerable morbidity, mortality and reduced quality of life. Of numerous interventional studies of fall prevention interventions in LTCFs, some reduced falls. However, there are challenges to implementing these interventions in real-world (non-trial) clinical practice, and the implementation techniques may be crucial to successful translation. This systematic review thus aimed to synthesise the evidence on implementation strategies, implementation outcomes and clinical outcomes included in fall prevention intervention studies.
Methods
A systematic search of six electronic databases (PubMed, CINAHL, EMBASE, PsycINFO, SCOPUS, Web of Science) and eight grey literature databases was conducted, involving papers published during 2001–2021, in English or Arabic, targeting original empirical studies of fall prevention interventions (experimental and quasi-experimental). Two seminal implementation frameworks guided the categorisation of implementation strategies and outcomes: the Expert Recommendations for Implementing Change (ERIC) Taxonomy and the Implementation Outcomes Framework. Four ERIC sub-categories and three additional implementation strategies were created to clarify overlapping definitions and reflect the implementation approach. Two independent researchers completed title/abstract and full-text screening, quality appraisal assessment, data abstraction and coding of the implementation strategies and outcomes. A narrative synthesis was performed to analyse results.
Results
Four thousand three hundred ninety-seven potential papers were identified; 31 papers were included, describing 27 different fall prevention studies. These studies used 39 implementation strategies (3–17 per study). Educational and training strategies were used in almost all (n = 26), followed by evaluative strategies (n = 20) and developing stakeholders’ interrelationships (n = 20). Within educational and training strategies, education outreach/meetings (n = 17), distributing educational materials (n = 17) and developing educational materials (n = 13) were the most common, with 36 strategies coded to the ERIC taxonomy. Three strategies were added to allow coding of once-off training, dynamic education and ongoing medical consultation. Among the 15 studies reporting implementation outcomes, fidelity was the most common (n = 8).
Conclusion
This is the first study to comprehensively identify the implementation strategies used in falls prevention interventions in LTCFs. Education is the most common implementation strategy used in this setting. This review highlighted that there was poor reporting of the implementation strategies, limited assessment of implementation outcomes, and there was no discernible pattern of implementation strategies used in effective interventions, which should be improved and clearly defined.
Trial registration
This systematic review was registered on the PROSPERO database; registration number: CRD42021239604.
Similar content being viewed by others

Background
Falling is a substantial health problem, as one of the most common geriatric syndromes among older people and linked to significant morbidity and mortality. The World Health Organisation (WHO) reports that approximately 30–50% of people aged 65 or above experience a fall at least annually, and 40% fall recurrently [1]. While falling is a problem in all health care settings, long-term care facilities (LTCFs) have the highest rate of falls of any setting – more than three times the rate of community settings, with an estimated 1.7 falls per resident-year [2, 3], and ranging between 3–13 falls per 1,000 bed days [4]. Indeed, half of residents in LTCFs experienced a fall more than once per year [5].
Falls often leads to physical and psychological consequences and economic burdens. One-third of residents suffer physical injuries after falling, most commonly hip fracture, estimated to occur in 3–5% annually [6]. Falls also produce psychological consequences such as depression, fear of falling, loss of confidence and decreased quality of life among residents [2, 7]. Falls in LTCFs are associated with a considerable economic burden to health care systems through prolonged hospitalisation. According to the National Institute for Clinical Excellence (NICE), the annual costs of falls and fall-related fractures are 2.3 and 1.7 billion pounds sterling, respectively [8]. Furthermore, fall-related death is considered the second most common cause of death globally [9]. The WHO (2021) estimates that 684,000 individuals die from falls each year, and it was reported in 2015 that 23% to 40% of fatal injuries in older people are due to falls [9, 10].
Falls are caused by various factors, including intrinsic factors, extrinsic factors and behaviour-related factors, and often result from a combination of factors. Intrinsic factors include chronic diseases, cognitive impairment, ageing, etc. Extrinsic factors include environmental hazards and medication, while behaviour-related factors linked to risk-taking and threat appraisal range from fear of falling on one side to risk-taking behaviour and impulsivity on the other [11,12,13,14]. Fall prevention interventions have been developed for LTCFs to identify and reduce risk factors related to falls and to reduce the rates of falls and fall-related injuries [5, 15]. They are typically multi-component interventions that provide standardised fall prevention interventions to reduce two or more risk factors related to falls. However, single intervention and multi-factorial interventions (i.e., where the intervention was tailored to the identified risk factors and needs of the residents) have also been described in the literature [16]. Interventions typically include exercises, staff education, environmental modification, medication review, etc.) [15, 16].
Many systematic reviews (SRs) and meta-analyses (MAs) have explored the effectiveness of fall prevention interventions in LTCFs [17,18,19,20,21,22,23,24,25] In 2015, Vlaeyen et al. published an SR and MA, reporting that fall prevention interventions overall reduced recurrent faller rates significantly, by 21%, but not the number of falls or fallers [18]. Within these studies, multifactorial interventions, as opposed to single or multiple interventions, appeared to reduce the number of fallers and recurrent fallers. Staff training as a single intervention appeared to increase the number of falls in two (low quality) studies. Lee et al., who conducted an MA in 2017, reported that exercise interventions reduced the fall rate substantially, and also decreased the number of falls and the fall rate when combined with other fall interventions [17]. Vitamin D supplementation also reduced the fall rate as a single intervention, according to a Cochrane collaborative review published in 2018, whereas other single or multifactorial interventions did not [23]. This review also noted the uncertainty of the effect of various fall prevention interventions in reducing the risk of falls. More recently, Gulka et al.’s SR and MA in 2020 indicated that all types of fall interventions reduced the numbers of falls (27%), fallers (20%), and recurrent fallers (30%) [22]. Exercise as a single intervention reduced the number of fallers (36%) and recurrent fallers (41%), respectively. However, it was reported that exercise interventions overall did not reduce falls, only exercise with a balance component, or using a technical device (like a balance board) or lasting over 6 months in duration [22]. It was also noted that staff education and training intervention revealed benefits in reducing falls and recurrent falls, unlike other single interventions [22].
Thus, the evidence for fall prevention interventions in LTCFs exist is mixed, reflecting the exact intervention in “single intervention” studies (with more evidence for exercise than staff education), the cohort studied (i.e. frailty and cognitive status influence outcomes), and the choice of outcome itself (e.g. falls, or fallers, or recurrent fallers). Clinicians work with older people who have varying levels of frailty, morbidity and functional capacity, and encounter many barriers to implementing fall prevention interventions in LTCFs [3, 26]. In 2017, an SR of eight mixed-methods studies found 27 barriers to implementing fall prevention interventions in LTCFs, with the most cited barriers as follows: staff feeling overwhelmed, helpless, frustrated and concerned about their ability to control falls management; staffing issues; limited knowledge and skills; and poor communication [27]. These challenges might impact on the success of fall prevention interventions, and thus it is necessary to identify techniques to facilitate the implementation of fall prevention interventions in LTCFs.
Implementation strategies are defined as “the methods and techniques used to enhance the adoption, implementation, and sustainability of a clinical programme or practice” [28]. Strategies such as audits and feedback, tailored strategies, educational meetings and educational outreach have been shown to improve the implementation of evidence-based care [29,30,31,32]. The successful implementation of fall prevention interventions can be achieved via multi-faceted influential strategies (e.g., audits and feedback, educational meetings, local opinion leaders) and strategies tailored to the needs of the clinical context, as determined by participants, that help staff, organisations and patients to overcome barriers and adopt a clinical intervention in real-world clinical settings [33]. The implementation strategies used, and how the implementation process is carried out (which is in turn assessed using implementation outcomes), may have an impact on the intervention’s effectiveness [34]. Nonetheless, previous SRs of fall prevention interventions in LTCFs have not included implementation strategies or outcomes. This review thus aims to synthesise the evidence on implementation strategies used to support fall prevention interventions in LTCFs, and also to describe the implementation outcomes included in the studies and how they were measured; along with clinical outcomes (i.e., Fall-related outcomes).
Methods
A narrative SR was planned, given the nature of the topics of interest (implementation strategies and implementation outcomes) and the expected methodological and clinical heterogeneity of the studies. The SR was registered on the International Prospective Register of Systematic Reviews (PROSPERO) database (registration number CRD42021239604) and the protocol was published in BMJ Open [35]. The SR reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline [36, 37].
Eligibility criteria
All fall prevention intervention studies incorporating using experimental and quasi-experimental designs were included, considering single-site and cluster randomised controlled trials (RCTs), feasibility studies for RCTs (including pilot studies), pre and post-test design and quality improvement empirical studies. We only included qualitative studies, RCT protocol papers or mixed methods papers that accompanied eligible RCTs or pre-post studies, where these provided more detail on intervention implementation and clarified the context of implementation strategies (i.e., protocol papers). These complementary papers were not included in the quality appraisal process, but their content was used to aid our interpretation and synthesis of the main study. The inclusion and exclusion criteria were based on the Population, Intervention, Comparison, Outcome (PICO) framework, presented in Table 1. All relevant studies were published in English or Arabic (based on the authors’ native languages), between January 1, 2001, and December 31, 2021. The search dates reflected the relative newness of the field of implementation science such that no relevant data was expected prior to 2000.
Information sources and search strategy
After consulting with a medical librarian at University College Cork regarding search strategy terms and electronic and grey literature databases, a search was carried out on PubMed, CINAHL, EMBASE, Psyc INFO, SCOPUS and Web of Science for published intervention studies. In addition, a search was conducted for all published theses on OPEN GREY, Open Access Theses and Dissertations (OATD), ProQuest, British Library EThOS, EBSCO Open dissertation, RIAN, LENUS and CORA, to include studies where usable data existed in a published thesis but where paper publications were still in progress or there was a possibility of publication bias. The search was limited to the last 20 years, until 31st December 2021. Search terms and medical subject headings (MeSH) incorporated keywords such as "long-term care facilities", "fall prevention" and "implementation outcomes", including free or controlled terms, combined with Boolean operators (see “Additional file 1 for search terms used, and PubMed database search strategy sample”). We conducted a forward and backward citation search of the studies included and a manual search for any related feasibility or implementation papers using the names of intervention study authors. We also hand-searched the reference lists of the published SRs on this topic.
Selection process
Two reviewers (NA, LA) independently assessed the abstracts and titles of all papers retrieved to identify potentially relevant studies for a full review, using the evidence synthesis software Covidence (www.covidence.org). The software was used to eliminate the duplicate studies. Three independent reviewers (NA, LA and LO) then screened the full texts of all papers eligible for inclusion. All disagreements were resolved by a senior researcher (ST). In addition, two senior researchers (ST, NC) peer-reviewed and screened randomly selected papers to ensure the quality of the two screening phases: title/abstracts (100 checked) and full texts (50 checked). The consistency of all papers included was finally double-checked by a senior researcher (RM).
Data collection process and data items
Two independent reviewers (NA, LA) extracted data from papers included. The data were compared, and any disagreement was resolved by discussing until consensus was reached. The extraction table included the following details: first author, publication year, country, study design, study duration (intervention and follow-up periods), participant eligibility criteria and sample size (e.g., patient criteria, staff criteria), participant data, fall intervention characteristics (e.g., type of intervention, usual care or control intervention), implementation strategy, implementation outcomes (e.g., fidelity) and intervention outcome (i.e., direct fall-related outcomes).
The outcomes (or outcome domains) of the present review were as follows. Firstly, the implementation strategies of fall prevention interventions were categorised and labelled using the Expert Recommendation for Implementing Change taxonomy (ERIC) [39, 40]. This framework provides a comprehensive definition of 73 discrete implementation strategies, mapped under nine subheadings. This list was developed by researchers and expert clinicians, generating expert consensus on a common set of terms and definitions, refining the original compilation implementation strategy list of Powell et al. (2009) from health care and mental health care literature [41]. The descriptions of the implementation strategies in many studies can be varied, leading to difficulty in comparing and categorising them; selecting ERIC in this review facilitated a more systematic description and reporting of the implementation strategies, regardless of terminology discrepancies.
Secondly, the implementation outcomes were categorised based on the Proctor et al. taxonomy, which defines eight implementation outcomes: feasibility, fidelity, adoption, appropriateness, implementation cost, sustainability, acceptability and penetration [34, 42]. An expert group from the implementation sciences developed the implementation outcome taxonomy to identify the precise concept for labelling the implementation process by collating definitions of implementation outcomes and determining the distinctions between them.
The clinical outcome of interest was the effect of the intervention on fall reduction, which was reported in different ways in intervention studies, in terms of fall risk reduction, fall rate reduction, time to first fall, etc. We considered the primary outcome without distinguishing between injurious and non-injurious falls, and secondary outcomes (e.g., mortality rate) are not presented in this review.
Risk of bias assessment
Two independent reviewers (NA, LA) assessed the quality of the papers included using the relevant checklists for RCT and quasi-experimental studies from the Joanna Briggs Institute (JBI) Critical Appraisal Tool, in which these checklists assessed studies according to a total of 13 and nine assessment criteria, respectively [43, 44]. All disagreements were resolved by discussion. Each item was rated as "yes", "no", "unclear" or "not applicable", based on whether or not the information was obviously reported or if the criteria were irrelevant to the study [45]. One point was given to every criterion rated "yes", whereas 0 was given to criteria rated "no", "unclear" or "not applicable". Following this, a total score for each study was calculated by adding all of the “yes” responses for each study out of 13 criteria for RCT and nine criteria for quasi-experimental studies. The authors a priori decided to not exclude papers based on their quality appraisal results, so as to be able to include quasi-experimental and quality improvement studies which were likely to have useful implementation data.
Synthesis methods
A narrative synthesis was undertaken because of the methodological and clinical heterogeneity of the studies included in this review (both variety in intervention components and outcome measures), and a metanalysis was not practical. Two independent reviewers (NA, LA) coded each study's implementation strategies data according to the best match with the labels and definitions for the 73 ERIC strategies, then synthesised them into the nine subheadings. To code strategies we used the definitions in the published ERIC taxonomy and the detailed descriptions contained in the supplementary files of that paper. We used NVivo software (QSR International) to organise the data for the coding and labelling process, and we resolved any conflict via discussion. There was a challenge in coding some education-related text to ERIC strategies, where the described strategy did not fit into an existing ERIC strategy. As a result, additional strategies, in terms of frequency, mode of delivery, variety of information delivery techniques, and consultation-focused strategies, were required. Similarly, the implementation outcomes were coded and synthesised using Proctor’s taxonomy, considering the actual measurement of their outcome and data reporting from the target population. A senior researcher (SM) checked all implementation strategy and outcome coding.
Coding assumptions
When coding implementation strategies, we made the following assumptions: firstly, all references to the assessment of environment hazards and modification, such as rugs, slippery floors, electrical cords, floor lighting at night, etc., or the assessment/repair of assistive devices, when provided as a core component of the intervention, were excluded from coding, because these were considered clinical interventions for preventing falls. Although we excluded environmental modifications because they were clinical interventions for preventing falls, we did include infrastructure changes at the organisation level, because they support the implementation of intervention strategies. Secondly, any references to educating residents as part of the intervention were not coded, despite being similar to the “prepare patients to be active" implementation strategy, because this is a part of a fall prevention intervention, not an implementation intervention. Thirdly, we used the ERIC label “create a learning collaborative” for studies where there were efforts to bring together the intervention providers, although the collaboration purpose was not always clear. Fourthly, we categorised references to staff reminders as “clinicians’ reminders” strategies, without detailed description, because such information was not stated in the paper. This assumption was made to ensure that even the minimum level of content of any strategies was acknowledged. In addition, any reference to individuals who assisted staff in their practice by providing problem-solving, discussion or support, whether involving internal or external facilitators, was coded under the “facilitation” strategy.
Some strategies involved both audit and feedback, whereas other interventions only implemented audit; we grouped these together, noting which aspect was used. Similarly, the development and the distribution of educational material were deemed likely to occur together, and so were grouped together, unless the study explicitly described using existing educational material sourced from elsewhere. Furthermore, the definition of the strategy “conduct educational outreach visits” contained many aspects of teaching delivery and was broad in scope based on the detailed description in the ERIC supplementary file. To more accurately capture the nature of the strategy, we adapted four subcategories of an existing strategy (i.e., education meeting/outreach) based on the mode of delivery (e.g., in-service vs online) and frequency of education/training delivery (e.g., once off vs ongoing sessions). When using a variety of information delivery methods (i.e., dynamic training versus dynamic education), a distinction has been made between training (e.g., group discussion) and education (e.g., videos, posters). We distinguished references to “ongoing consultation strategies” (which provided consultations focused on fall prevention implementation strategies) from references to medical consultation to solve medical problems linked to falls. Thus, three additional strategies have been identified under one of the ERIC subheadings, namely training and educating stakeholders. All new subcategories and strategies developed in this SR that were not found in ERIC lists were added to the codebook (see “Additional file 4”).
Reporting bias assessment
We contacted the authors of studies where only the abstracts or trial protocols were published, to seek full-text articles and we included published theses to avoid potential publication bias for unpublished negative studies or slow publication of thesis results.
Result
Study selection
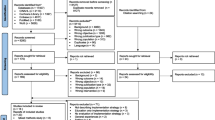
We identified 4,397 papers from the search of all databases and other resources. After duplicate studies were removed, 3,027 unique papers remained for title/abstract screening. Of these, 2,832 papers were irrelevant and excluded based on titles/abstracts, leaving 195 papers for full-text screening. In total, 27 studies met our eligibility criteria and were included [46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72], and four additional papers related to two of the intervention studies were included to provide more detail on the intervention implementation [73,74,75,76] (See Fig. 1).

PRISMA flow diagram of study selection and inclusion process. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. https://doi.org/10.1136/bmj.n71
Study characteristics
Overall, 7 out of 27 studies included were cluster randomised controlled trials (CRCTs) [60,61,62,63,64,65,66]. The remaining studies were quasi-experimental studies, 14 of which were peer-reviewed journal articles [46,47,48,49,50,51,52,53,54,55,56,57,58,59] and six of which were published theses [67,68,69,70,71,72]. A pre-post design accounted for the majority of the quasi-experimental studies, and nine of these were quality improvement projects. Additionally, two out of 4 additional papers were protocol papers [74, 76], while the other two referred to a single intervention. In the first, the validated process of fall outcomes was measured using clinical vignettes and chart abstraction in a cross-sectional study within CRCT [75]. The second was a qualitative study comparing staff descriptions of the learning climate, the use of social constructivist learning processes and outcomes between the intervention and control groups [73].
In total, 17 studies were conducted in the United States; six were in European countries (Spain, Poland, Sweden, Belgium, Germany and Scotland) [47, 51, 54, 60, 63, 66]; three were in Australia or New Zealand [56, 61, 65], while one study was conducted in Japan [58]. Overall, 10 out of 27 studies were conducted in nursing homes [47, 49,50,51,52, 54, 59, 63, 64, 66]; four involved skilled nursing facilities [57, 67, 69, 71]; one was in a state-provided veterans home [55]. In total, 16 were carried out at single sites [46,47,48, 50, 53, 54, 56, 58, 59, 67,68,69,70,71,72, 77]. In eleven studies, the intervention was directed at nursing staff only (i.e., registered nurses, certified nurses’ assistants, licensed practical nurses) [46, 48, 56, 58, 63, 66,67,68,69,70,71]. Nine studies delivered a single fall-prevention intervention (e.g., staff education) [48, 52, 62, 63, 65, 67, 68, 70, 71], while nine included multi-component interventions (i.e., a standardised approach for all participants) [46, 49, 50, 55, 59, 64, 66, 69, 72], and nine were multi-factorial interventions that tailored the intervention to the needs of the participants and the residents [47, 51, 53, 54, 56, 60, 61, 77]. The majority of intervention components concentrated on training and educating staff in falls risk assessment, risk factor modification, and post-fall management and medication review (see Table 2). The duration of the included interventions ranged from four to 104 weeks, and most (21 studies) involved falls interventions lasting 26 weeks or less. Only eleven studies included follow-up periods after the intervention, ranging from 13 to 52 weeks. Ten studies involved control groups, eight of which received usual care, while two studies provided interventions to control groups (Table 2).
Risk of bias in studies
The quality appraisal scores for the seven cluster RCTs ranged from six to nine out of the 13 criteria in the JBI tools. Three studies scored 9 s, while three studies scored 8 s, and one study was assessed as having six of the evaluation criteria. The lack of the blinding of participants and of those who administered the interventions was the weakest area of the cluster RCTs included. The 20 quasi-experimental study scores ranged from four to seven for the nine criteria of the JBI checklist; 10 studies received 5 s, while seven studies received 6 s, two studies received 4 s and one study scored 7 out of all the appraisal criteria, as the use of control groups was limited in the studies included. As planned, no studies were excluded based on the quality appraisal results; all studies included were of low to moderate quality (Additional file 2).
Implementation strategy descriptions
Across 27 studies, this review identified 39 implementation strategies used in falls prevention interventions, of which 36 strategies were aligned directly with the ERIC list. Three strategies from the ERIC Taxonomy were added to better reflect the implementation approach: once-off training, dynamic education and the provision of ongoing medical consultation strategies. The number of discrete implementation strategies per study varied from 3 to 17. Table 3 provides an overview of the ERIC implementation strategies used, grouped into nine ERIC subheadings, and “Additional file 3” provides detailed descriptions of the implementation strategies in all studies.
Most studies used multiple implementation strategies to support the delivery of the fall prevention intervention. As per Table 3, one study reported implementation strategies in eight categories [46], two studies in six categories [49, 54], three studies in five categories [50, 55, 61], while eight [47, 53, 56,57,58, 62, 64, 65] and ten [51, 52, 59, 60, 66,67,68,69, 71, 72] respectively reported implementation strategies in either four or three categories. Three studies [48, 63, 70] discussed implementation strategies in two and one categories, respectively.
The most frequent categories of implementation strategy in the studies included in this review related to the following: training and educating stakeholders (n = 26); the use of evaluative and iterative strategies and the development of stakeholders’ interrelationships (n = 20); providing interactive assistance (n = 14); supporting clinicians (n = 10); changing infrastructure (n = 5); tailoring to the context (n = 4); engaging consumers (n = 2); and utilising financial strategies (n = 1). The results are organised according to these groups.
Train and educate stakeholders
The three most common implementation strategies used in this group were conducting an education outreach/meeting (n = 17), distributing educational materials (n = 17) and developing educational materials (n = 13) (for more details, see “Additional file 3”). In the 17 studies which involved an education outreach/meeting for improving staff knowledge, 12 studies of which [46, 48, 56, 60, 61, 63, 64, 67, 68, 70,71,72] involved in-service education sessions at organisational sites; one study [55] included a virtual education session, and one study incorporated in-person and teleconference sessions [52]. Ten studies included once-off education sessions ranging from a number of hours in a single day to a number of days in a single week [46, 47, 60, 61, 63, 67,68,69,70, 72]. Seven studies involved ongoing education sessions, such as monthly or quarterly [48, 52, 55, 56, 58, 64, 71].
In total, 17 studies distributed educational material physically or online (e.g., via notebooks, posters, brochures or manual training materials [48, 49, 52, 53, 56, 57, 61,62,63,64,65,66,67, 69,70,71,72]. Thirteen studies involved the development of new educational materials related to interventions (e.g., presentations, falls forms, videos, modules) [48, 49, 52, 61,62,63,64,65,66, 69, 71, 72, 77]. Six studies focused on improving staff skills via frequent ongoing training (i.e., workshops) [48, 49, 53, 64, 65, 77],whilst five involved once-off training days/hours, also in the form of workshops [50, 51, 54, 62, 66]. We identified two studies that concerned both staff education (knowledge) and training (skills) [48, 64]. The strategy of making training dynamic was used in five studies by varying the learning style of training to ensure it was interactive (e.g., group discussions, storytelling and role play, problem-solving) [49, 62,63,64]. One study used dynamic education strategies (i.e., acronyms, pictures, videos) [68], and two studies used dynamic strategies for both training and education [48, 71]. Two studies [48, 49] provided ongoing consultation to support the implementation strategy needed for fall prevention, whereas one study involved ongoing clinical consultation with experts to solve medical problems [58]. One study fostered a collaborative learning environment by creating a specific collaborative learning strategy connecting all staff participating in the intervention with the fall prevention resources and encouraging them to use them through continuous networking meetings [65].
Developing stakeholder interrelationships
Eight studies used the identification and preparation of champions for supporting implementation in sites, [46, 49, 54, 55, 67,68,69, 72], while one study only reported the process of identifying champions (ref single study). Seven studies used advisory workgroups including formal groups of falls teams or multi-disciplinary committees to provide recommendations on implementation [49, 50, 52, 58, 59, 72, 77]. Seven studies held weekly/monthly meetings with clinician implementation teams to reflect implementation efforts and issues as an integrated part of interventions [46, 50, 53, 54, 58, 60, 64]. Six studies employed leadership recruitment, design and training to support changes in care plans, monitor staff performance and offer intervention recommendations [49, 55, 56, 61, 62, 67]. Two studies captured and shared local knowledge of staff to allow them to discuss their experiences with current fall issues and techniques they applied to prevents falls [55, 71]. One study promoted staff to weave a network by creating a group-to-group and individual-to-individual relationship map to improve staff interaction and communication [64]. One study used a coalition-building strategy by describing all of the interventions and activities that were required to participate in the study [49].
Using evaluative and iterative strategies
Eleven out of the 27 studies developed and implemented tools for quality monitoring (i.e., falls forms, flow charts, log, checklists, staff diaries) [49,50,51, 53, 54, 60, 65, 66, 69, 72, 77]. Six studies purposefully re-examined the implementation to assess the success of, and impediments to, interventions and to track progress [46, 49, 55, 56, 68, 72]. Six studies conducted audits and provided feedback by informing staff about the implementation outcomes and progress [55, 56, 64, 77], and two of them only conducted audits, without feedback [58, 61]. Five studies developed and organised quality monitoring systems for monitoring the outcomes using software programs, or tracking reports, or via clinical documentation processes [49, 50, 59, 67, 72]. Four studies conducted local needs assessments relevant to their current fall approaches to determine the need for interventions [49, 54,55,56]. One study assessed readiness [55], and one included five small cyclical test changes to complete a fall risk intervention tool with refinement in each cycle [54].
Providing interactive assistance
Eleven studies employed facilitation strategies that provided staff encouragement and support in their responsibilities as implementers of the intervention, in problem-solving processes and in managing interpersonal staff communication problems, using researchers, organisational coaches, external consultants and paid facilitators [46,47,48,49,50, 54, 61, 62, 64, 65, 71]. Three studies used local professionals’ (e.g., nurses, coaches) to provide technical assistance for implementation concerns [54, 55, 59]. Three studies involved clinician supervision (e.g., weekly supervision visits) [46, 49, 51]. Two studies included centralised technical assistance systems such as weekly visits to support staff for the purpose of filling in falls forms and open discussion calls to answer questions and troubleshoot [59, 63].
Supporting clinicians
Clinicians were given reminders in seven studies via electronic reminders in the registration systems or labelling/colouring dots on residents’ profiles, on armbands, or reminders in residents’ rooms [46, 47, 52, 56, 61, 66, 77]. Four studies created new clinician teams to implement interventions [55, 62, 70, 77]. One study revised professional roles by outlining their responsibilities [47].
Changing infrastructure
Two studies changed the physical structure and equipment in sites (the placement of laundry receptacles in hallways, the use and storage of housekeeping and maintenance equipment, and the location of a fall registry) [46, 47]. Two changed record systems on falls risk assessment tools in the registration systems [47, 49]. One study mandated change by obtaining support for the interventions from divisions of general practice [65]. One study started to disseminate information in a more organised way, as two senior care assistants and two nurses on site took responsibility for initiating huddles [54].
Adopting and tailoring to the context
Three studies promoted adaptability of the intervention (e.g., exercise interventions or care plans tailored to the residents' needs based on assessment and staff communication procedures) [49, 50, 58]. One study used tailored strategies to address barriers (e.g., translating educational sessions for non-English-speaking staff) [46].
Engaging consumers
Two studies involved family caregivers in educational sessions and root cause analysis activities [53, 54].
Utilising financial strategies
One study altered incentive/allowance structures by compensating staff who attended educational sessions on their days off [46].
Implementation outcomes description
Implementation outcomes were identified and synthesised from 15 of the 27 studies, with four studies reporting two or three implementation outcomes [52, 53, 55, 57]. Table 4 shows how each study's implementation outcomes were measured. Most studies used both administrative data (i.e., medical records or other documentation) and/or self-reported data (audits of staff/facilities, self-reports) to assess implementation outcomes. Fidelity (n = 8) was the most commonly reported implementation result outcome [47, 49, 50, 52, 55, 56, 61, 62], measured as the level of compliance with interventions conducted, at either the facility level or the staff level. Three studies evaluated the acceptability of the training by surveying staff satisfaction [48, 53, 55], whereas one study reported acceptability, but this was at the level of the resident, based on how many of them did not agree to do their recommend exercises or activities, which was documented by monitoring staff [57]. Similarly, three studies assessed adoption by determining the percentage of residents who completed entire fall risk assessment and exercise regimens from all residents referred to a physiotherapy programme and could be evaluated, as well as the uptake of interventions by staff at each facility [51, 55, 64]. One study measured the level of participation in executing the programme at the facility, to determine penetration [52]. One study evaluated feasibility by monitoring the implementation process for completing fall intervention tools over The Plan-Do-Study-Act (PDSA) cycles; the falls champions were unable to complete the use of the tools when tested among new residents [54]. Only one study reported appropriateness, but this was at the level of the resident, based on residents' rejection of an exercise programme due to their health status, and their performance was monitored by staff [77]. One study reported the nursing care implementation cost by calculating how long it takes an average nurse to complete a falls assessment risk tool (Downton index) and multiplying it by the nursing wage per hour [63]. The sole implementation outcome that was not addressed in any of the studies presented was sustainability.
Intervention effectiveness
Because the studies included varied significantly in terms of study aims, outcomes, assessments, intervention durations and follow-up timing, a descriptive summary of the interventions’ effects on primary outcomes was provided, such as fall-related outcomes and staff-related outcomes. Although the effectiveness of the interventions was not the primary focus of this SR, we described the interventions’ effects in Table 2, where the exact effect sizes and, confidence intervals and p values are presented where available. To present data on the types of strategies used in studies that reduced falls rates, and those that did not, we colour-coded Table 3 to show that non-significant or neutral/adverse studies for falls rates (n = 4; n = 3 respectively) used a similar range of implementation strategies to the 10 effective studies, highlighting to the absence of a clear pattern of which implementation strategies are most effective.
Fall-related outcomes
Overall, 25 out of 27 studies reported fall-related outcomes; fall rates and the number of falls were the most common clinical outcome reported in all studies, while a few reported fall-related injuries and fall-related circumstances. Regarding fall rates, 10 reported effective reductions of fall rates [46, 50, 53, 54, 58, 60, 68, 69, 71, 72], while four reported a reduction of falls without statistical significance [51, 52, 55, 77]. However, Rask et al. indicated that the fall rate in the intervention group remained unchanged [49]. Keres et al. reported that the fall rate increased and was higher in the intervention groups during implementation compared to control groups [61], while Ward et al. found no change in the fall rate for both pre- and post-intervention across both groups [65].
Twelve studies determined that there was a decrease in the number of falls [47, 53, 56, 58,59,60, 66,67,68,69, 71, 77]. In contrast, two study reported a reduction of falls without statistical significance between both groups [63, 66], and Keres et al. reported an increase in the number of falls in the intervention groups. Four studies reported on recurrent falls or reported the number of fallers. Wongrakapnich et al. indicated a reduction in frequent falls [53], whilst Kato et al. reported that the number of fallers increased in both groups [58]. Colon-Emeric et al.,B reported no effect and no differences between groups concerning the recurrent fall rate [64]. Hofmann et al. reported the number of fallers and the percentage of recurrent falls during the follow-up year without making any comparisons or statistical analysis pre-post interventions [59].
Four studies reported on fall-related characteristics. Jackson et al. found that half of falls occurred during the day, and the majority fell in their bedroom. Hofmann et al. reported that the most common fall period was during the 3–11 p.m. shift, and Ogundu et al. reported that the evening shift had no reduction in the number of falls with their intervention. Meanwhile, Lomax et al. found that the night shift had a greater number of falls, and that rising from beds and walking were the most common activities associated with fall incidents.
Seven studies measured fall-related injuries; two of them reported a significant reduction of injuries from falls [53, 55], while one study indicated an increasing number of fall-related injuries in the intervention group [61]; Keto et al., conversely, reported that the number of injuries and the number of injured persons decreased significantly in the intervention groups compared to control groups, which had an increase in injured persons but no change in the number of injuries [58]. Two studies reported no statistically significant change in fall injuries in intervention or control groups [62, 64], while Jackson et al. reported the quality assurance documentation for the average number of injuries during the intervention [50]. Moreover, two studies reported fall-related fracture injuries; one indicated a reduction in hip fractures rate compared to before the intervention [59], while the other found no difference in the number of femoral fractures between both groups [65].
Six studies that were CRCTs reported no differences between intervention and control groups in the fall rate, fall-related injuries or recurrent falls [61,62,63,64,65,66]. In contrast, Jensen et al. indicated a statistically significantly reduced number of falls and fall rates between the intervention and control groups, with no differences in time to first falls between the two groups [60]. From the quasi-experimental studies, only three had a control group. Two reported no significant differentiation of fall rate between groups [52, 61], whereas another reported a relative reduction in the falls rate in the intervention group, although the number of fallers increased in both [58]. Some studies included other fall-relevant outcomes, (e.g., vitamin D prescription, etc.) which are detailed in Table 2.
Staff-related outcomes
Four studies measured staff knowledge using surveys; three reported a positive effect on improving their knowledge [46, 50, 68], whereas one reported no significant effect [71]. Three studies measured nursing staff self-efficacy and reported a positive impact [48, 58, 70]. Staff motivation and empowerment was measured in one study, and effective results were noted [58]. Staff communication was measured by Colon-Emeric et al.,B with no effect nor difference between groups [64].
Discussion
Many SRs have described intervention effectiveness as regards the clinical effectiveness of fall prevention interventions among LTCF residents; however, this is the first SR to synthesis the interventions’ implementation strategies and implementation outcomes in order to provide insight into how they have been used in LTCF fall prevention interventions. Two frameworks from the implementation science, namely the ERIC implementation strategy and Proctor implementation outcome taxonomies, were used to synthesise the implementation strategies used and outcomes, as these were described in various ways, with varying terms used for the same strategy in some cases.
The findings identified that 39 implementation strategies were used across 27 fall-prevention studies targeting LTCF staff. Training-and-education implementation strategies were the most popular. Other SRs also found that educational strategies were comprehensively used, targeting health workers to change their professional practice or behaviour [78,79,80,81,82]. A recent SR published in 2020, found that staff education interventions on how to prevent falls among residents have benefits for minimising falls and recurrent falls [22]. The studies included in this SR incorporated multi-faceted strategies and education sessions, and distributed educational materials were commonly used. The studies used varied frequencies and modes of education and training delivery. The delivery methods included formal lectures, teleconferences, education calls. Focussing on the frequency of education delivery (once or continuous) helped to understand the educational implementation process. We established subcategories regarding frequency and delivery mode related to education meetings/outreach strategies in order to clarify overlapping definitions. We also identified other non-ERIC-codable strategies related to staff education and training: once-off training, dynamic education, ongoing medical consultation.
Some studies focused on enhancing staff skills through hands-on training, whether once-off or ongoing, including different interactive learning and training activities (e.g., problem-solving skills). They showed a mixture of passive (e.g., distribute education material) and active (dynamic education/consultation) education strategies, as previous literature indicates that passive education strategies are highly likely to be ineffective for adherence [83]. However, not all studies reported the educational dose durations, which is an integral part of describing the education sessions. This is consistent with a previous scoping review, which found that there are many falls prevention education programmes available for health workers, but that many aspects of reporting education programmes are of poor quality [84].
Vlaeyen et al. identified 27 barriers for staff in terms of implementing fall interventions in LTCFs, reporting that a lack of staff knowledge and skills was one of the most common barriers, requiring a focus on fall prevention interventions, as it is considered a changeable factor [27]. This aligns with our review, where the most common strategies used for implementing fall prevention interventions in LTCFs were education and training, reflecting their perceived status as modifiable and influential on care. Moreover, identifying barriers and facilitators is a strategy that is considered a critical precursor to determining the best implementation methods and processes, allowing the use of evidence-based interventions to address the barriers. Additionally, it has been found that tailored strategies to address determinants of interventions during practice are considered effective for improving health worker performance, support for uptake, and determining an adequate implementation strategy [31]. This review identified limited use of evaluation of barriers/facilitators at the level of staff/facilities before conducting the interventions and hence tailoring of the implementation strategies to address barriers, with only one study doing so. This may have affected the success of the implementation of the others.
Our findings also identified that most studies used a combination of strategies for fall interventions (e.g., audits/feedback, facilitation, education outreach/meetings, clinicians’ reminders and leadership). These strategies have been identified as the most influential strategies in terms of success in complex interventions by supporting health workers in their real-world practice [29, 30, 32, 82, 85, 86]. Moreover, all of the studies used a varying number of strategies, ranging from three to 17 strategies. This review gained insight into strategies that were used regularly, as well as the multi-faceted nature of implementation strategies, in terms of the total number of strategies or the degree of use of strategies that are reported to be the most influential (e.g., audits/feedback), but it did not reveal the relative impact of single or combined implementation strategies. It is essential to consider the relationships between the quantity and combination of strategies used and the success of their implementation [87].
Although many studies measured implementation outcomes, 12 studies did not. Fidelity was the most commonly measured implementation outcome, in eight studies. It was reported based on levels of compliance with delivering the falls intervention(s), but this, when used as a sole implementation outcome, is not enough to assess behaviour change or full adoption of the intervention. The findings also revealed varying lengths of study duration and follow-up. Only a few studies included short-term follow-up measurements. Sustainability, one of Proctor et al.’s eight implementation outcomes, requires a follow-up period for the measurement of long-term compliance, and reflects the impact of intervention implementation in terms of continued acceptability, effectiveness and adaptability, as is required in a real clinical setting [88]; this review did not identify any study that reported on it.
According to the literature, the healthcare system is burdened by fall-related costs, reported to be approximately 4 million bed days (£2.3 billion per year), and 50% of these costs involve hospitalisation [8, 88]. However, we found only a few references to fall-related costs. One study employed one of the nine financial ERIC strategies, titled “Alter incentive/allowance structures”, to compensate staff who attended the education session on their day off, but otherwise there was an absence of the use of financial strategies, as found in other SRs [79]. Another considered the delivery cost as an outcome, without any cost–benefit analysis. More information related to fall-related costs is needed, as it is significant for implementing fall prevention interventions in LTCF. Indeed, a SR found that multifactorial fall prevention interventions were beneficial in reducing the fall rate in LTCF only when combined with external resources and financing [20].Economic evaluations are vital for clarifying the cost benefits of making clinical and policy decisions about fall prevention in LTCFs. This should be the focus of future implementation work in falls prevention interventions in LTCFs.
Although the majority of the studies in our SR reported a significant positive effect on fall-related outcomes, there was heterogeneity in the studies in terms of study aims, outcomes, assessments, intervention durations and follow-up timing, as previously reported by others [78]. Two of the studies measured staff-related outcomes (i.e., staff knowledge) only. In the others, there was variable reporting of falls indices such as fall rates, the number of fallers, and so on. This led us to narratively describe the results and, in this review, there was no discernible pattern of strategies used exclusively in effective fall prevention interventions. Future research on fall prevention must therefore explicitly describe the effectiveness of implementation strategies on implementation outcome and clinical outcomes.
Despite the fact that a wide variety of implementation strategies were identified, detailed reporting of how strategies were applied, along with the implementation outcomes in the studies included, were under-reported. Therefore, the effectiveness of fall interventions was often attributed to the programmes, without regard for what implementation strategies had the greatest impact. Ongoing efforts to operationalise and measure implementation outcomes is necessary, as has been previously described [79].
Thus, this review highlights that there is a lack of consistency in reporting implementation strategies and outcomes, leaving no possibility to conclude what eventually influences the prevention of falls among LTCF residents. This points to the need for more research to identify the relationship between the implementation strategies and both clinical and implementation outcomes in the future.
Limitations and strengths
The present SR has made a novel contribution to implementation science by providing a comprehensive synthesis of implementation strategies used for LTCF fall prevention interventions. The SR’s processes and analyses were double-checked and reviewed. Even though we included only English and Arabic texts, we excluded only one paper based on language, so the potential impact of language bias is likely negligible. We included published theses to reduce publication bias; an extensive search strategy of multiple grey literature databases might have further reduced possible publication bias, but the quality of the data would likely be low. We did not exclude studies based on the quality appraisal scores, with a view to being as inclusive as possible of studies that reported implementation strategies and outcomes in LTCF fall prevention. The majority of the studies included were quasi-experimental studies. Others were cluster RCTs; however, this approach does not produce the same level of confidence as RCTs, and it makes it difficult to compare between studies. There is also a limitation to a narrative synthesis due to the heterogeneity of the studies included, as compared to meta-analysis.
The ERIC and Proctor implementation outcome taxonomies are seminal implementation frameworks that provide a unified language for clearly understanding implementation strategies and outcomes, respectively. However, ERIC definitions of strategies are broad, and they include many aspects that lead to overlap and conflict of some strategies’ definitions, which may hinder a judgement concerning the labelling of some strategies (e.g., conducting education outreach/meetings). Moreover, there was a wide variety in the degree of reported details regarding the components of strategies. The results were weighted similarly for all studies that used the same strategy. To completely comprehend the effects of strategies, more detailed description and standard reporting of the implementation strategies using precise terminology is required. Proctor et al. have provided recommendations on how to specify implementation strategies designed to improve specific implementation outcomes, including the following: naming, describing and specifying the strategies [28]. The use of specific implementation guidelines such as the Standard for Quality Improvement Reporting Excellence (SQUIRE) and the Standard for Reporting Implementation Studies (StaRI) could help to standardise descriptions of strategies [89].
Conclusion
This is the first study to synthesis the comprehensive implementation strategies used in LTCFs as regards falls prevention interventions. Many implementation strategies have been used, with education being the most common. Outside of the ERIC lists, three novel educational strategies were identified: providing once-off training, dynamic education and ongoing medical consultation. This review highlighted difficulties in learning from the implementation of fall prevention interventions, especially in relation to poor reporting of the implementation strategies used and implementation outcomes, which should be improved and clearly defined in future studies. There was no discernible pattern of implementation strategies used in effective interventions; thus, future falls prevention research needs to clearly describe the implementation along with the clinical intervention, and both clinical and implementation outcomes need to be included.
Availability of data and materials
All Data generated and analysed during this review is available in the supplement file.
Abbreviations
- LTCFs:
-
Long-term care facilities
- WHO:
-
The World Health Organisation
- SR:
-
Systematic review
- MAs:
-
Meta-analyses
- RCT:
-
Randomised controlled trial
- PROSPERO:
-
The International Prospective Register of Systematic Reviews
- PRISMA-P:
-
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocol
- MeSH:
-
Medical subject headings
- ERIC:
-
The Expert Recommendation for Implementing Change Taxonomy
- JBI:
-
The Joanna Briggs Institute
- NICE:
-
The National Institute for Clinical Excellence
- SQUIRE:
-
The Standard for Quality Improvement Reporting Excellence
- StaRI:
-
The Standard for Reporting Implementation Studies
References
World Health Organization. WHO Global Report on falls prevention in older age. Community Health; 2007. p. 53. Available from: http://www.who.int/ageing/publications/Falls_prevention7March.pdf.
Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. 2006;35(SUPPL.2):37–41.
Vu MQ, Weintraub N, Rubenstein LZ. Falls in the nursing home: are they preventable? J Am Med Dir Assoc. 2006;7(3 SUPPL):S53-8, 52.
Pountney D. Preventing and managing falls in residential care settings. Nurs Residential Care. 2009;11(8):410–4.
Kannus P, Sievänen H, Palvanen M, Järvinen T, Parkkari J. Prevention of falls and consequent injuries in elderly people. Lancet. 2005;366(9500):1885–93.
Rapp K, Becker C, Lamb SE, Icks A, Klenk J. Hip fractures in institutionalized elderly people: incidence rates and excess mortality. J Bone Miner Res. 2008;23(11):1825–31.
Lehtola S, Koistinen P, Luukinen H. Falls and injurious falls late in home-dwelling life. Arch Gerontol Geriatr. 2006;42:217–24.
NICE. NICE clinical guideline 161. Falls: Assessment and prevention of falls in older people. Nat Inst Health and Care Excellence 2013;161(June):1–315. Available from: www.nice.org.uk/guidance/CG161.
World Health Organisation [WHO]. Falls. Fact sheet. 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/falls. Cited 2021 Dec 4.
World Health Organization. World report on ageing and health. World Health Organization; 2015. Retrieved from from http://www.who.int/ageing/publications/world-report-2015/en/.
Deandrea S, Bravi F, Turati F, Lucenteforte E, La C, Negri E. Risk factors for falls in older people in nursing homes and hospitals. A systematic review and meta-analysis. Arch Gerontol Geriatr. 2013;56(3):407–15. https://doi.org/10.1016/j.archger.2012.12.006.
Shobha SR. Prevention of falls in older patients. Am Fam Physician. 2005;72(1):81–8.
Fonad E, Wahlin TBR, Winblad B, Emami A, Sandmark H. Falls and fall risk among nursing home residents. J Clin Nurs. 2008;17(1):126–34.
Ferrari M, Rn D, Harrison B, Gnp Bc A, Lewis D. The risk factors for impulsivity-related falls among hospitalized older adults. Rehabil Nurs. 2012;37(3):145–50.
Quigley P, Bulat T, Kurtzman E, Olney R, Powell-Cope G, Rubenstein L. Fall prevention and injury protection for nursing home residents. J Am Med Dir Assoc. 2010;11(4):284–93. https://doi.org/10.1016/j.jamda.2009.09.009.
Developed by the Panel on Prevention of Falls in Older Persons AGS and BS. Summary of the updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc. 2011;59(1):148–57.
Lee SH, Kim HS. Exercise interventions for preventing falls among older people in care facilities: a meta-analysis. Worldviews Evid Based Nurs. 2017;14(1):74–80.
Vlaeyen E, Coussement J, Leysens G, van der Elst E, Delbaere K, Cambier D, et al. Characteristics and effectiveness of fall prevention programs in nursing homes: A systematic review and meta-analysis of randomized controlled trials. J Am Geriatr Soc. 2015;63(2):211–21.
Neyens JC, van Haastregt JC, Dijcks BP, Martens M, van den Heuvel WJ, de Witte LP, et al. Effectiveness and implementation aspects of interventions for preventing falls in elderly people in long-term care facilities: a systematic review of RCTs. J Am Med Dir Assoc. 2011;12(6):410–25. https://doi.org/10.1016/j.jamda.2010.07.018.
Francis-Coad J, Etherton-Beer C, Burton E, Naseri C, Hill AM. Effectiveness of complex falls prevention interventions in residential aged care settings: a systematic review. JBI Database System Rev Implement Rep. 2018;16(4):973–1002.
Schoberer D, Breimaier HE. Meta-analysis and GRADE profiles of exercise interventions for falls prevention in long-term care facilities. J Adv Nurs. 2020;76(1):121–34.
Gulka HJ, Patel V, Arora T, McArthur C, Iaboni A. Efficacy and generalizability of falls prevention interventions in nursing homes: a systematic review and meta-analysis. J Am Med Dir Assoc. 2020;21(8):1024–10354. https://doi.org/10.1016/j.jamda.2019.11.012.
Cameron ID, Dyer SM, Panagoda CE, Murray GR, Hill KD, Cumming RG, et al. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev. 2018;2018(9):CD005465.
Stubbs B, Denkinger MD, Brefka S, Dallmeier D. What works to prevent falls in older adults dwelling in long term care facilities and hospitals? An umbrella review of meta-analyses of randomised controlled trials. Maturitas. 2015;81(3):335–42. https://doi.org/10.1016/j.maturitas.2015.03.026.
Abdullah Alfadhel SA, Vennu V, Alotaibi ADA, Algarni AM, Saad Bindawas SM. The effect of a multicomponent exercise programme on elderly adults’ risk of falling in nursing homes: a systematic review. J Pak Med Assoc. 2020;70(4):699–704.
Tinetti ME. Preventing Falls in Elderly Persons. N Engl J Med. 2003;348(1):42–9.
Vlaeyen E, Stas J, Leysens G, van der Elst E, Janssens E, Dejaeger E, et al. Implementation of fall prevention in residential care facilities: a systematic review of barriers and facilitators. Int J Nurs Stud. 2017;70:110–21. https://doi.org/10.1016/j.ijnurstu.2017.02.002.
Proctor EK, Powell BJ, McMillen JC. Implementation strategies: Recommendations for specifying and reporting. Implement Sci. 2013;8(1):1–11.
Ma OB, Rogers S, Jamtvedt G, Ad O, Dt K, Forsetlund L, et al. Educational outreach visits: effects on professional practice and health care outcomes (Review). Cochrane Database Syst Rev Educ. 2007;2007(4):CD000409.
Ivers N, Jamtvedt G, Flottorp S, Young JM, Odgaard-Jensen J, French SD, et al. Audit and feedback: effects on professional practice and healthcare outcomes (Review). Cochrane Database Syst Rev Audit. 2012;2012(6):CD00025.
Baker R, Camosso-Stefinovic J, Gillies C, Shaw EJ, Cheater F, Flottorp S, et al. Tailored interventions to address determinants of practice. Cochrane Database Syst Rev. 2015;2015(4):CD005470.
Forsetlund L, O’Brien MA, Forsén L, Reinar LM, Okwen MP, Horsley T, et al. Continuing education meetings and workshops: effects on professional practice and healthcare outcomes. Cochrane Database Syst Revi. 2021;2021(9):CD003030.
Breimaier HE, Halfens RJG, Lohrmann C. Effectiveness of multifaceted and tailored strategies to implement a fall-prevention guideline into acute care nursing practice: a before-and-after, mixed-method study using a participatory action research approach. BMC Nurs. 2015;14(1):1–12.
Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health Ment Health Service Res. 2011;38(2):65–76.
Albasha N, Mccullagh R, Cornally N, Mchugh S, Timmons S. Implementation strategies supporting fall prevention interventions in a long-term care facility for older persons: a systematic review protocol. BMJ Open. 2022;12(e055149):1–6 Available from: http://bmjopen.bmj.com/.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Research methods and reporting Prisma 2020 explanation and elaboration : updated guidance and exemplars for reporting systematic reviews review findings. The preferred. BMJ. 2021;372:n:160.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Ageing and Health unit. Available from: https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/ageing-and-health/integrated-continuum-of-long-term-care. Cited 2022 Dec 8.
Waltz TJ, Powell BJ, Matthieu MM, Damschroder LJ, Chinman MJ, Smith JL, et al. Use of concept mapping to characterize relationships among implementation strategies and assess their feasibility and importance : results from the Expert Recommendations for Implementing Change ( ERIC ) study. Implement Sci. 2015;10:109. https://doi.org/10.1186/s13012-015-0295-0.
Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et al. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implement Sci. 2015;10(1):1–14.
Powell BJ, Mcmillen JC, Proctor EK, Christopher R, Griffey RT, Bunger AC, et al. A compilation of strategies for implementing clinical innovations in health and mental Health. Med Care Res Rev. 2012;69(2):123–57.
Proctor EK, Landsverk J, Aarons G, Chambers D, Glisson C, Mittman B. Implementation research in mental health services: an emerging science with conceptual, methodological, and training challenges. Admin Policy Mental Health Mental Health Services Res. 2009;36(1):24–34.
The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews. Checklist for Quasi-experimental studies (non-randomized experimental studies). 2017. Available from: http://joannabriggs.org/research/critical-appraisal-tools.
Critical Appraisal tools for use in JBI Systematic Reviews. Checklist for randomized controlled trials. 2020. Available from: https://joannabriggs.org/critical-appraisal-tools.
Porritt K, Gomersall J, Lockwood C. JBI’s systematic reviews: study selection and critical appraisal. Am J Nurs. 2014;114(6):47–52.
Bonner A, MacCulloch P, Gardner T, Chase CW. A student-led demonstration project on fall prevention in a long-term care facility. Geriatr Nurs (Minneap). 2007;28(5):312–8.
Gama ZAS, Medina-Mirapeix F, Saturno PJ. Ensuring evidence-based practices for falls prevention in a nursing home setting. J Am Med Dir Assoc. 2011;12(6):398–402. https://doi.org/10.1016/j.jamda.2011.01.008.
Leverenz M, Lape J. Education on fall prevention to improve self-efficacy of nursing staff in long term care: a pilot study. Internet J Allied Health Sci Pract. 2018;16(3):6.
Rask K, Parmelee PA, Taylor JA, Green D, Brown H, Hawley J, et al. Implementation and evaluation of a nursing home fall management program. J Am Geriatr Soc. 2007;55(3):342–9.
Jackson KM. Improving nursing home falls management program by enhancing standard of care with collaborative care multi-interventional protocol focused on fall prevention. J Nurs Educ Pract. 2016;6(6):84–96.
Szczerbińska K, Zak M, Ziomkiewicz A. Role of method of implementing multi-factorial falls prevention in nursing homes for elderly persons The EUNESE project. Aging Clin Exp Res. 2010;22(3):261–9.
Colón-Emeric C, Schenck A, Gorospe J, McArdle J, Dobson L, DePorter C, et al. Translating evidence-based falls prevention into clinical practice in nursing facilities: results and lessons from a quality improvement collaborative. J Am Geriatr Soc. 2006;54(9):1414–8.
Wongrakpanich S, Danji K, Lipsitz L, Berry S. Stop-falling: a simple checklist tool for fall prevention in a nursing facility. J Am Med Dir Assoc. 2019;20(7):916–8. https://doi.org/10.1016/j.jamda.2018.10.002.
Cooper R. Reducing falls in a care home. BMJ Qual Improv Rep. 2017;6(1):u214186.w5626.
Zubkoff L, Neily J, Delanko V, Young-Xu Y, Boar S, Bulat T, et al. How to prevent falls and fall-related injuries: a virtual breakthrough series collaborative in long term care. Phys Occup Ther Geriatr. 2019;37(4):234–46.
Beasley K. Benefits of implementing an interdisciplinary and multifactorial strategy to falls prevention in a rural, residential aged-care facility. Int J Evid Based Healthc. 2009;7(3):187–92.
Theodos P. Fall prevention in frail elderly nursing. Lippincott’s Case Manag. 2004;9(1):32–44.
Kato M, Izumi K, Shirai S, Kondo K, Kanda M, Watanabe I, et al. Development of a fall prevention program for elderly Japanese people. Nurs Health Sci. 2008;10(4):281–90.
Hofmann MT, Bankes PF, Javed A, Selhat M. Decreasing the incidence of falls in the nursing home in a cost-conscious environment: a pilot study. Am Med Dir Assoc. 2003;4:95–7.
Jensen J, Lillemor LO, Lars N, Gustafson Y. Fall and injury prevention in older people living in residential care facilities. Ann Intern Med. 2002;136(10):733–41.
Kerse N, Butler M, Robinson E, Todd M. Fall prevention in residential care: a cluster, randomized controlled trial. J Am Geriatr Soc. 2004;52(4):524–31.
Ray WA, Taylor JA, Brown AK, Gideon P, Hall K, Arbogast P, et al. Prevention of fall-related injuries in long-term care: a randomized controlled trial of staff education. Arch Intern Med. 2005;165:2293–8.
Meyer G, Köpke S, Haastert B, Mühlhauser I. Comparison of a fall risk assessment tool with nurses’ judgement alone: a cluster-randomised controlled trial. Age Ageing. 2009;38(4):417–23.
Colón-Emeric CS, Corazzini K, McConnell ES, Pan W, Toles M, Hall R, et al. Effect of promoting high-quality staff interactions on fall prevention in nursing homes: a cluster-randomized trial. JAMA Intern Med. 2017;177(11):1634–41.
Ward JA, Harden M, Gibson RE, Byles JE. A cluster randomised controlled trial to prevent injury due to falls in a residential aged care population. Med J Aust. 2010;192(6):319–22.
Bouwen A, de Lepeleire J, Buntinx F. Rate of accidental falls in institutionalised older people with and without cognitive impairment halved as a result of a staff-oriented intervention. Age Ageing. 2008;37(3):306–10.
Lomax P. Implementation of post falls huddles in skilled nursing facility. Valparaiso University. 2020. Available from: https://scholar.valpo.edu/ebpr.
Ofosuhene A. Staff development project for fall prevention in long-term care. Walden University. 2021. Available from: https://scholarworks.waldenu.edu/dissertations.
Ogundu OU. Fall reduction among elderly residents in skilled nursing facility. Regis University. 2016. Available from: https://epublications.regis.edu/theses.
Aguwa H. Nursing education to prevent resident falls in long-term care. Walden University. 2019. Available from: https://scholarworks.waldenu.edu/dissertations.
Wells PR, An. Preventing falls in a nursing home. A.T. Still University. 2011. Available from: https://search.proquest.com/dissertations-theses.
Hurst MN. Implementation of an electronic fall risk scale assessment tool. Wilmington University. 2019. Available from: https://search.proquest.com/dissertations-theses.
Colón-Emeric CS, Pinheiro SO, Anderson RA, Porter K, McConnell E, Corazzini K, et al. Connecting the learners: Improving uptake of a nursing home educational program by focusing on staff interactions. Gerontologist. 2014;54(3):446–59.
Anderson RA, Corazzini K, Porter K, Daily K, McDaniel RR, Colón-Emeric C. Connect for quality: protocol of a cluster randomized controlled trial to improve fall prevention in nursing homes. Implement Sci. 2012;7(1):1–14.
Colón-Emeric CS, Corazzini KN, McConnell ES, Pan W, Toles MP, Hall R, et al. Resident vignettes for assessing care quality in nursing homes. J Am Med Dir Assoc. 2019;19(5):405–10.
Theodos P, Theodos P. Fall prevention in frail elderly nursing home residents a challenge to case management: part I. Lippincott’s Case Manag. 2003;8(6):246. Available from: https://journals.lww.com/professionalcasemanagementjournal/Fulltext/2003/11000/Fall_Prevention_in_Frail_Elderly_Nursing_Home.6.aspx.
Theodos P. Fall prevention in frail elderly nursing home residents a challenge to case management: part I. Lippincott’s Case Manag. 2003;8(6):246.
Spoon D, Rietbergen T, Huis A, Heinen M, van Dijk M, van Bodegom-vos L, et al. Implementation strategies used to implement nursing guidelines in daily practice: a systematic review. Int J Nurs Stud. 2020;111:103748. https://doi.org/10.1016/j.ijnurstu.2020.103748.
Peven K, Bick D, Purssell E, Rotevatn TA, Nielsen JH, Taylor C. Evaluating implementation strategies for essential newborn care interventions in low- and low middle-income countries : a systematic review. Health Policy Plan. 2020;35:ii4-65.
Watkins K, Wood H, Schneider CR, Clifford R. Effectiveness of implementation strategies for clinical guidelines to community pharmacy: a systematic review. Implement Sci. 2015;10(1):151. https://doi.org/10.1186/s13012-015-0337-7.
Johnson LG, Armstrong A, Joyce CM, Teitelman AM, Buttenheim AM. Implementation strategies to improve cervical cancer prevention in sub-Saharan Africa: A systematic review. Implement Sci. 2018;13(1):1–18.
Pantoja T, Opiyo N, Lewin S, Paulsen E, Ciapponi A, Wiysonge CS, et al. Implementation strategies for health systems in low-income countries: an overview of systematic reviews (Review). Cochrane Database Syst Rev. 2017;9:CD011086.
Villarosa AR, Maneze D, Ramjan LM, Srinivas R, Camilleri M, George A. The effectiveness of guideline implementation strategies in the dental setting: A systematic review. Implement Sci. 2019;14(1):1–16.
Shaw L, Kiegaldie D, Farlie MK. Education interventions for health professionals on falls prevention in health care settings: a 10-year scoping review. BMC Geriatr. 2020;20(1):1–13.
Reeves S, Pelone F, Harrison R, Goldman J, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6(6):CD000072.
Pantoja T, Grimshaw JM, Colomer N, Castañon C, Leniz Martelli J. Manually-generated reminders delivered on paper: effects on professional practice and patient outcomes. Cochrane Database Syst Rev. 2019;12(12). Available from: https://pubmed.ncbi.nlm.nih.gov/31858588/. Cited 2022 May 22.
Northridge ME, Paone D, Maylahn CM, Powell BJ, Fernandez ME, Williams NJ, et al. Enhancing the impact of implementation strategies in healthcare: a research Agenda. Front Public Health. 2019;1(3). Available from: www.frontiersin.org.
Department of health. National service framework for older people. DH, London. Br J Nurs. 2001;23(10):543.
Leeman J, Birken SA, Powell BJ, Rohweder C, Shea CM. Beyond “implementation strategies”: classifying the full range of strategies used in implementation science and practice. Implement Sci. 2017;12(1):1–9.
Acknowledgements
The authors are grateful to Dr Aisling Jennings, a medical director in a local LTCF, who contributed to developing the paper's discussion and conclusion sections by reviewing and contextualising the findings as an external stakeholder.
Funding
This systematic review will be conducted as a part of the PhD project for the first author, which is funded by Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia (Grant Number: Not applicable).
Author information
Authors and Affiliations
Contributions
ST, NC, RM, SM and NA conceptualised and designed this review. NA conducted the search, reviewed abstracts and full texts, quality-assessed the papers included, extracted data and analysed data. LA reviewed abstracts and full texts, quality-assessed the papers included and extracted data. LO reviewed the full texts. ST, NC and RM peer-reviewed and double-checked all of the screening stages and the extraction data table. SM reviewed the categorisation of implementation strategies. NA drafted the initial manuscript. ST, NC, SM and RM critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategy used and PubMed database search strategy results.
Additional file 2: Table 1.
The quality appraisal results of included CRCTs (Experimental studies). Table 2. The quality appraisal results of included Quasi-experimental studies.
Additional file 3.
Detailed description of implementation strategies identified.
Additional file 4.
The codebook definitions of implementation strategies identified.
Additional file 5.
Detailed description of the reasons for excluding papers.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Albasha, N., Ahern, L., O’Mahony, L. et al. Implementation strategies to support fall prevention interventions in long-term care facilities for older persons: a systematic review. BMC Geriatr 23, 47 (2023). https://doi.org/10.1186/s12877-023-03738-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-03738-z