
Abstract
Background
Few studies using rigorous clinical diagnosis have considered whether associations with cognitive decline are potentiated by interactions between genetic and modifiable risk factors. Given the increasing burden of cognitive impairment (CI) and dementia, we assessed whether Apolipoprotein E ε4 (APOE4) genotype status modifies the association between incident CI and key modifiable risk factors .
Methods
Older adults (70+) in the US were included. APOE4 status was genotyped. Risk factors for CI were self-reported. Cognitive status (normal, CI, or dementia) was assigned by clinical consensus panel. In eight separate Cox proportional hazard models, we assessed for interactions between APOE4 status and other CI risk factors.
Result
The analytical sample included 181 participants (mean age 77.7 years; 45.9% male). APOE4 was independently associated with a greater hazard of CI in each model (Hazard Ratios [HR] between 1.81–2.66, p < 0.05) except the model evaluating educational attainment (HR 1.65, p = 0.40). The joint effects of APOE4 and high school education or less (HR 2.25, 95% CI: 1.40–3.60, p < 0.001), hypertension (HR 2.46, 95% CI: 1.28–4.73, p = 0.007), elevated depressive symptoms (HR 5.09, 95% CI: 2.59–10.02, p < 0.001), hearing loss (HR 3.44, 95% CI: 1.87–6.33, p < 0.0001), vision impairment (HR 5.14, 95% CI: 2.31–11.43, p < 0.001), smoking (HR 2.35, 95% CI: 1.24–4.47, p = 0.009), or obesity (HR 3.80, 95% CI: 2.11–6.85, p < 0.001) were associated with the hazard of incident CIND (compared to no genetic or modifiable risk factor) in separate models. The joint effect of Apolipoprotein ε4 and type 2 diabetes was not associated with CIND (HR 1.58, 95% CI: 0.67–2.48, p = 0.44).
Discussion
The combination of APOE4 and selected modifiable risk factors conveys a stronger association with incident CI than either type of risk factor alone.
Similar content being viewed by others


Introduction
Dementia affects an estimated 57.4 million individuals worldwide and this number is projected to nearly triple by 2050 [1]. Cognitive impairment typically precedes a diagnosis of dementia, and those with cognitive impairment have an increased risk of dementia compared to cognitively normal adults [2,3,4]. Because interventions to prevent dementia may be most effective when implemented early in the process of cognitive decline, research is needed to characterize early risk factors for cognitive decline [5].
The Apolipoprotein E ε4 (APOE4) genotype is the strongest genetic risk factor for cognitive decline and late onset dementia; yet, when considered in isolation, it accounts for a relatively small portion of population dementia risk [5, 6]. Prior studies have identified several modifiable risk factors for cognitive decline, including less education, hypertension, type 2 diabetes mellitus (T2DM), depression, hearing loss, vision impairment, smoking, and obesity [5, 7]. However, few studies have considered whether interactions between APOE4 and modifiable risk factors may influence the risk of clinically diagnosed cognitive impairment [8,9,10,11,12].
Prior research on dementia risk reported interactions between APOE4 and smoking in the UK Biobank [8] and between APOE4 and depression in Canadian Study of Health and Aging, [9] while other studies have reported no interaction between smoking, [8] healthy lifestyle, [10, 11] or self-reported hearing loss [12] and polygenic risk for dementia [8, 10, 12, 13] or cognitive decline [11, 12]. In light of data suggesting that APOE4 may be more strongly associated with cognitive impairment than dementia, [14] we hypothesized significant modification by APOE4 status on the association of key modifiable risk factors with incident cognitive impairment.
Methods
Study sample
The Aging, Demographics, and Memory Study (ADAMS) was a nationally representative study of a sub-sample of adults age ≥ 70 years recruited from the United States Health and Retirement Study (HRS) from 2000–2002 [15]. The HRS collects a wide array of sociodemographic, health, and economic data that is made publicly available (hrsonline.isr.umich.edu) [16]. Participants returned for study visits approximately every 2 years or until they were diagnosed with dementia. Participants who were cognitively normal at baseline and had ≥ 2 waves of data were included in this analysis. Institutional Review Boards at the University of Michigan and Duke University approved all HRS/ADAMS study procedures. Informed consent was obtained from all study participants or their surrogates. The current secondary analysis of publicly available data was deemed not regulated.
Cognitive assessment
In ADAMS, a nurse and neuropsychology technician administered cognitive tests and obtained a history on health issues, activities, symptoms, medical history, cognitive or functional impairment, and other contributory factors. Further details of ADAMS methodology has been previously described [15]. Using this information, a provisional diagnosis of cognitively normal, cognitive impairment not dementia (CIND), or dementia was determined by judgement of a consensus panel consisting of a geropsychiatrist, neurologist, neuropsychiatrist, and cognitive neuroscientist. After reviewing medical records, the geropsychiatrist revised the provisional diagnosis as needed. The full consensus panel then arrived at a final diagnosis without knowledge of prior HRS or ADAMS assessments or statuses.
The diagnosis of CIND [15, 17] was defined as: self and/or informant report of problems with cognition or daily activities, or performance on neuropsychological measures that was both below expectation relative to education, reading level, and occupational attainment, and at least 1.5 standard deviations below published norms on at least one test. These are similar to the criteria for a diagnosis of mild cognitive impairment (MCI), but MCI requires both measured declines in cognitive testing and reported problems with cognition or daily activities [18].
Apolipoprotein E4 (APOE4) genotyping
In ADAMS, APOE4 genotype was assessed via genotyping of a buccal swab DNA sample. The Oragene-250 protocol and saliva kits were used to collect the specimen. Staff at the Center for Inherited Disease Research genotyped the DNA using the Illumina HumanOmni2.5 array (8v1 and 4v1). Quality control was conducted by the Genetics Coordinating Center (University of Washington in Seattle, WA). Carrier status was dichotomized (0 vs 1 or 2 copies) since few participants carried 2 copies of the APOE4 gene.
Dementia risk factors
Participant characteristics were assessed by self-report (educational attainment [high school or less vs more than high school], hypertension, T2DM, elevated depressive symptoms [Center for Epidemiological Studies Depression score ≥ 4], [15] smoking [ever smoker vs never smoker], age, and gender) or objective measurement (hearing loss [unable to hear rubbing fingers or whispering in either ear], vision impairment [visual acuity < 20/40 in the better seeing eye], obesity [BMI ≥ 35]).
Statistical analysis
First, a Cox proportional hazard model was constructed with time to incident CIND as the dependent variable and death as a competing risk [19]. Independent variables included: APOE4 status, educational attainment, hypertension, T2DM, elevated depressive symptoms, hearing loss, vision impairment, smoking, obesity, age, and gender. In eight separate iterations of this model, an interaction term between APOE4 and a selected modifiable risk factor was used to test for modification by APOE status. All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA). Statistical tests were two-tailed and a significance threshold of α = 0.05 was used. The Holm’s Step-Down Procedure was used to adjust for multiple comparisons. Respondents with no event or death were censored at the last wave of the survey in which they participated. Respondents who transitioned from cognitively normal to dementia (without an intervening diagnosis of CIND) were assumed to have developed CIND at the midpoint between being cognitively normal and being diagnosed with dementia [20]. Death was modeled as a competing risk [19].
Results
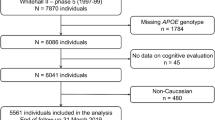
Of the 196 participants eligible participants, 181 who had complete data for each of the variables in the models were included in this analysis. Mean (standard deviation [SD]) age was 77.7 [5.1] years and 45.9% were male. Descriptive statistics for the analytic sample are presented in Table 1. Median (interquartile range) follow up duration was 5.0 (2.0-6.6) years.
The APOE4 genotype was independently associated with a greater hazard of CIND in each model (Hazard Ratios [HR] between 1.81–2.66, p < 0.05 in all models, Table 2) except the model evaluating educational attainment (HR 1.65, p = 0.40). In those with no copies of APOE4, the hazard of CIND was not associated with any of the eight selected modifiable risk factors (Fig. 1, Table 2).

Modifiable Risk Factors and their Joint Effects with Apolipoprotein E4 Genotype as Predictors of Incident Cognitive Impairment No Dementia (CIND)
APOE4: Apolipoprotein E4. BMI: Body Mass Index. Depressive symptoms were defined as Center for Epidemiological Studies Depression score ≥ 4. Smoking was defined as current or past tobacco smoking. Hazard ratios are from 8 separate Cox proportional hazard models with a main effect and a joint effect with APOE4 for the given predictor. Models were fitted with time to incident CIND as the dependent variable and death as a competing risk. Each model was additionally adjusted for age, sex, and each of the other 7 predictors. The bottom row shows the range for the hazard ratio for the main effect of APOE4 across the 7 models (confidence intervals are shown in Table 2).
Conversely, there was a statistically significant interaction between APOE4 and seven of the eight modifiable risk factors in predicting time to CIND (Fig. 1). The joint effects of APOE4 and high school or less educational attainment (HR 3.61, 95% CI: 1.51–8.61, p = 0.003), hypertension (HR = 2.46, 95% CI: 1.28–4.73, p = 0.007), elevated depressive symptoms (HR = 5.09, 95% CI: 2.59–10.02, p < 0.001), hearing loss (HR = 3.44, 95% CI: 1.87–6.33, p < 0.001), vision impairment (HR = 5.14, 95% CI: 2.31–11.43, p < 0.001), smoking (HR = 2.35, 95% CI: 1.24–4.47, p = 0.009), and obesity (HR = 3.80, 95% CI: 2.11–6.85, p < 0.001) were associated with incident CIND in separate models. The joint effect of APOE4 and T2DM was not associated with CIND (HR = 1.58, 95% CI: 0.67–2.48, p = 0.44).
Discussion
In this longitudinal study of 181 older adults, APOE4 genotype significantly modified the association between incident CIND and educational attainment, hypertension, elevated depressive symptoms, hearing loss, vision impairment, smoking, and obesity. Given the increasing number of older adults with dementia, detection of early risk factors for cognitive decline and identifying sub-groups for whom early risk factors are most relevant are important research priorities [1,2,3, 5]. Our results suggest that those with both genetic (e.g., APOE4) and modifiable risk factors may be at particularly high risk for cognitive decline. It is possible that such individuals could benefit from closer monitoring or earlier interventions to slow the progression of cognitive decline (e.g., more intensive cardiovascular risk factor control, exercise, cognitive training, etc.) [5].
Some prior studies have reported interactions between modifiable (e.g., smoking, [8] depression, [9] sleep disordered breathing [23]) and genetic risk for dementia or cognitive decline, while other studies have reported no interaction [10,11,12]. For example, the interaction between smoking and APOE4 status has been associated with incident dementia in the UK Biobank [8]. On the other hand, no significant interaction between polygenic risk score (excluding the APOE4 allele) and smoking was found in the UK Biobank cohort [8]. As such, it is possible that APOE4 genotype is a stronger modifier of the impact of modifiable risk factors on cognitive health as compared to other gene loci. Further research is needed to determine if there are significant interactions between modifiable dementia or cognitive impairment risk factors and other individual gene loci.
In the present study, there was so significant joint effect between T2DM and APOE4 status. Prior cohort study data have provided mixed epidemiologic evidence for an association between diabetes and cognitive impairment, with some reporting no association [3, 24] while others suggest a significant association [25,26,27]. As such, it is possible that the lack of a significant joint effect between diabetes and APOE4 status in the present study may be attributable to a lack of association between diabetes and CIND among this study population. Studies with longer follow-up, larger sample size, and assessment of duration of time lived with diabetes, will be important for elucidating the association of T2DM with CIND. Moreover, once one reaches CIND, risk factor interactions could become less important because the risk of progression from CIND to dementia may be high regardless of the presence of other risk factors [2, 3, 20].
The present study assesses risk factors from throughout the life course. For example, educational attainment is more readily modifiable in young adulthood and tends to remain unchanged as participants progress through mid-life and older adulthood, when cognitive impairment and dementia is more prevalent. The Lancet Commission’s 2020 Report on Dementia Prevention, Intervention, and Care recommends using a life course framework for understanding risk factors for cognitive decline and dementia [5]. In turn, studies assessing dementia risk factors have typically included risk factors from throughout participants’ life course [8,9,10,11,12]. While some risk factors may no longer be modifiable once individuals reach older-adulthood, early life interventions (e.g. education programs, smoking cessation, diabetes control, etc.) may result in later-life benefits for cognitive health, though considerable interventional research is needed to test this [5]. Further research is also needed to determine whether APOE4 genotype may modulate the effectiveness of early interventions to prevent cognitive decline [28].
The present study has several strengths compared to prior studies, including longitudinal follow up (median 5.0 years), consensus panel diagnoses of cognitive status, genotyping of all subjects, robust covariate adjustment, inclusion of 8 key CIND risk factors, and use of CIND as an outcome, which may have a stronger association with APOE4 than dementia [14]. Prior studies reporting no interaction differed from the present study based on lack of robust cognitive status assessment and/or assessment of polygenic risk rather than APOE4 status.
Limitations
Studies with a larger sample may be better suited for assessing interactions, subgroup analyses (e.g., by ancestry), and dose-response effects by number of APOE4 allele copies. Moreover, some null findings may have been due to large standard errors related to our relatively small sample size. Nevertheless, with a sample size of 181 participants, the present study detected significant interactions between APOE4 genotype and seven of the eight modifiable risk factors that we investigated, suggesting the sample was adequate to test the study’s hypothesis. Additionally, some participant characteristics were ascertained by self-report (educational attainment, hypertension, T2DM, elevated depressive symptoms, and smoking). Use of objective measures (e.g. blood pressure or hemoglobin A1c) could provide additional useful information about the relationship between chronic disease, APOE4 genotype, and cognitive impairment.
Conclusion
The combination of APOE4 genotype and modifiable risk factors conveys a stronger association with incident CIND than either type of risk factor alone. If these findings are confirmed, they may be useful for risk stratification, prognostication, and targeting of early interventions.
Availability of data and materials
The HRS collects a wide array of sociodemographic, health, and economic data that is made publicly available (hrsonline.isr.umich.edu).
Abbreviations
- APOE4:
-
Apolipoprotein E ε4
- T2DM:
-
Type 2 diabetes mellitus
- ADAMS:
-
Aging Demographic and Memory Study
- HRS:
-
Health and Retirement Study
- CIND:
-
Cognitive impairment, no dementia
- BMI:
-
Body mass index. HR: Hazard Ratio
References
Estimation of the global prevalence of dementia. in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7:e105–25.
Roberts RO, Knopman DS, Mielke MM, Cha RH, Pankratz VS, Christianson TJH, et al. Higher risk of progression to dementia in mild cognitive impairment cases who revert to normal. Neurology. 2014;82:317–25.
Plassman BL, Langa KM, McCammon RJ, Fisher GG, Potter GG, Burke JR, et al. Incidence of Dementia and Cognitive Impairment Not Dementia in the United States. Ann Neurol. 2011;70:418–26.
Langa KM, Levine DA. The Diagnosis and Management of Mild Cognitive Impairment: A Clinical Review. JAMA. 2014;312:2551–61.
Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396:413–46.
Ware EB, Faul JD, Mitchell CM, Bakulski KM. Considering the APOE locus in Alzheimer’s disease polygenic scores in the Health and Retirement Study: a longitudinal panel study. BMC Med Genomics. 2020;13:164.
Shang X, Zhu Z, Wang W, Ha J, He M. The Association between Vision Impairment and Incidence of Dementia and Cognitive Impairment: A Systematic Review and Meta-analysis. Ophthalmology. 2021;128:1135–49.
Zhang N, Ranson JM, Zheng Z-J, Hannon E, Zhou Z, Kong X, et al. Interaction between genetic predisposition, smoking, and dementia risk: a population-based cohort study. Sci Rep. 2021;11:12953.
Meng X, D’Arcy C. Apolipoprotein E. gene, environmental risk factors, and their interactions in dementia among seniors. Int J Geriatr Psychiatry. 2013;28:1005–14.
Lourida I, Hannon E, Littlejohns TJ, Langa KM, Hyppönen E, Kuzma E, et al. Association of Lifestyle and Genetic Risk With Incidence of Dementia. JAMA. 2019;322:430–7.
Folley S, Zhou A, Llewellyn DJ, Hyppönen E. Physical Activity. APOE Genotype, and Cognitive Decline: Exploring Gene-Environment Interactions in the UK Biobank. J Alzheimers Dis. 2019;71:741–50.
Neff RM, Jicha G, Hawk GS, Bush ML, McNulty B. Association of Subjective Hearing Loss and Apolipoprotein E ε4 Allele on Alzheimer’s Disease Neurodegeneration. Otol Neurotol. 2021;42:e15–21.
Rusanen M, Rovio S, Ngandu T, Nissinen A, Tuomilehto J, Soininen H, et al. Midlife Smoking, Apolipoprotein E and Risk of Dementia and Alzheimer’s Disease: A Population-Based Cardiovascular Risk Factors, Aging and Dementia Study. DEM. 2010;30:277–84.
Brainerd CJ, Reyna VF, Petersen RC, Smith GE, Kenney AE, Gross CJ, et al. The apolipoprotein E genotype predicts longitudinal transitions to mild cognitive impairment but not to Alzheimer’s dementia: findings from a nationally representative study. Neuropsychology. 2013;27:86–94.
Langa KM, Plassman BL, Wallace RB, Herzog AR, Heeringa SG, Ofstedal MB, et al. The Aging, Demographics, and Memory Study: study design and methods. Neuroepidemiology. 2005;25:181–91.
Sonnega A, Faul JD, Ofstedal MB, Langa KM, Phillips JW, Weir DR. Cohort Profile: the Health and Retirement Study (HRS). Int J Epidemiol. 2014;43:576–85.
Graham JE, Rockwood K, Beattie BL, Eastwood R, Gauthier S, Tuokko H, et al. Prevalence and severity of cognitive impairment with and without dementia in an elderly population. Lancet. 1997;349:1793–6.
Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund L-O, et al. Mild cognitive impairment–beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med. 2004;256:240–6.
Fine JP, Gray RJ. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J Am Stat Assoc. 1999;94:496–509.
Ehrlich JR, Swenor BK, Zhou Y, Langa KM. The Longitudinal Association of Vision Impairment With Transitions to Cognitive Impairment and Dementia: Findings From the Aging, Demographics and Memory Study. J Gerontol A Biol Sci Med Sci. 2021;76:2187–93.
Alzheimer’s disease facts and figures. Alzheimer’s & Dementia. 2020;16:391–460.
Ehrlich JR, Goldstein J, Swenor BK, Whitson H, Langa KM, Veliz P. Addition of Vision Impairment to a Life-Course Model of Potentially Modifiable Dementia Risk Factors in the US. JAMA Neurol. 2022;79:623–6.
Nikodemova M, Finn L, Mignot E, Salzieder N, Peppard PE. Association of Sleep Disordered Breathing and Cognitive Deficit in APOE ε4 Carriers. Sleep. 2013;36:873–80.
Tervo S, Kivipelto M, Hänninen T, Vanhanen M, Hallikainen M, Mannermaa A, et al. Incidence and Risk Factors for Mild Cognitive Impairment: A Population-Based Three-Year Follow-Up Study of Cognitively Healthy Elderly Subjects. DEM. 2004;17:196–203.
Launer LJ. Demonstrating the case that AD is a vascular disease: epidemiologic evidence. Ageing Res Rev. 2002;1:61–77.
Haan MN, Shemanski L, Jagust WJ, Manolio TA, Kuller L. The Role of APOE ∊4 in Modulating Effects of Other Risk Factors for Cognitive Decline in Elderly Persons. JAMA. 1999;282:40–6.
Lopez OL, Jagust WJ, Dulberg C, Becker JT, DeKosky ST, Fitzpatrick A, et al. Risk Factors for Mild Cognitive Impairment in the Cardiovascular Health Study Cognition Study: Part 2. Arch Neurol. 2003;60:1394–9.
Claxton A, Baker LD, Hanson A, Trittschuh EH, Cholerton B, Morgan A, et al. Long-Acting Intranasal Insulin Detemir Improves Cognition for Adults with Mild Cognitive Impairment or Early-Stage Alzheimer’s Disease Dementia. J Alzheimer’s Disease. 2015;44:897–906.
Acknowledgements
N/A
Sponsor’s Role
The funding source did not play any role in the design, execution, or writing of this investigation.
Funding
JRE is supported by a grant from the National Institutes of Health (K23EY027848). This work was supported by a grant from the Michigan Center on the Demography of Aging to JRE funded by the National Institute on Aging (P30AG012846). KML is supported by a grant from the National Institute on Aging (R01AG053972). EBW is supported by grants from the National Institute on Aging (R01AG055406, R01AG067592, R01AG055654). The Health and Retirement Study is funded by the National Institute on Aging (U01AG009741) and the Social Security Administration, and performed at the Institute for Social Research, University of Michigan. The funding sources did not have a role in the study design; the collection, analysis, interpretation of data; the writing of the report; or the decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
A.K. wrote the main manuscript text and prepared Fig. 1. Y.Z. and G.C. conducted data analyses, created Tables 1 and 2, and contributed to the editing and finalization of the manuscript. J.R.E., E.B.W. and K.M.L. contributed to the conceptualization of the work, the study design, and revision of the manuscript. Each author was involved in the conceptualization, design, determination of study methodology, and preparation of the paper. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Subjects have given their written informed consent and that the study protocol was approved by the University of Michigan’s Institutional Review Board.
Consent for publication
N/A
Competing interests
JRE has consulted for MetLife, unrelated to the topic of this study. No other authors have conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kolli, A., Zhou, Y., Chung, G. et al. Interactions between the apolipoprotein E4 gene and modifiable risk factors for cognitive impairment: a nationally representative panel study. BMC Geriatr 22, 938 (2022). https://doi.org/10.1186/s12877-022-03652-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03652-w