
Abstract
Objective
Minor stroke or transient ischemic attack (TIA) usually have mild and nondisabling symptoms, and these functional deficits may recover fully e.g., TIA, however, part of them still suffer from cognitive impairment and poor outcomes. We conducted a study to determine the relationship between cognition evaluated by Montreal Cognitive Assessment (MoCA) and poor functional outcomes assessed by the Modified Rankin Scale (mRS) (mRS ≥ 2) and Stroke Impact Scale (SIS)-16(SIS-16<25%).
Methods
The data of this study come from the impairment of cognition and Sleep (ICONS) after acute ischemic stroke or transient ischemic attack in Chinese patients study. A total of 1675 minor stroke patients and TIA patients were finally recruited. Patients’ cognition were evaluated by Montreal Cognitive Assessment (MoCA) scale at 2-week (2w), 3 months (3 m) and 1 year(1y). Cognitive impairment (CI) was defined as MoCA score ≤ 22. According to MoCA score, patients were divided into 4 groups: no PSCI group: with MoCA-2w>22 and MoCA-3 m>22; improved PSCI group: with MoCA-2w ≤ 2 and MoCA-3 m>22;delayed PSCI group: MoCA-2w>22 and MoCA-3 m ≤ 22; persisting PSCI group: with MoCA-2w ≤ 22 and MoCA-3 m ≤ 22.
Results
A total of 1675 stroke patients were recruited in this study. There were 818 patients (48.84%) who had PSCI at baseline. Of these, 123 patients (15%) had mRS ≥2 at 3 months. The persisting PSCI group was a significant predictor of functional dependence at 3 months and 1 year after stroke and when adjusted for covariates such as gender, age, history of stroke, depression and intracranial atherosclerotic stenosis, stroke subtype and acute infarction type.
Conclusion
Persisting PSCI increased the risk of poor functional outcome after 3 months and 1 year follow-up. These high-risk individuals should be identified for targeted rehabilitation and counseling to improve longer-term post-stroke outcome.
Similar content being viewed by others


Introduction
Patients with minor stroke have mild symptoms and may go through a rapid physical recovery. However, they may struggle with more complex activities and experience cognitive impairment. Studies have reported rates of cognitive impairment ranging from 35 to 92% according to different evaluation time and scales [1]. Impairment has been reported to affect multiple cognitive domains [2], one recent study evaluating those with TIA and minor stroke found difficulty with executive function and psychomotor processing to be the most common cognitive deficits [3]. The widely used screening tool is Mini-Mental State Examination (MMSE) and MoCA. MoCA includes executive function and attention tests (among many different cognitive domains), which have been more suitable thus recommended for screening for cognitive impairment in patients with stroke or TIA [4]. Therefore, we used MoCA to evaluate cognitive status in the present study. The effects and outcomes of stroke can be devastating. The mRS score is commonly used to assess functional outcomes, but it has ceiling effect. The Stroke Impact Scale (SIS)-16 was designed to comprehensively assess stroke-related outcomes [5] and accurately assess recovery after stroke [6]. It contains 8 domains – strength, hand function, activities of daily living, mobility, communication, emotion, memory and thinking, participation [6]. It has been applied to evaluate the health-related quality of life in post-stroke patients [7], on discharge and at the first and the third-month post-stroke [6]. Previous studies investigated the relationship between cognitive decline and function outcomes after stroke [8,9,10]. Early screening through MoCA could predict long-term functional dependence [11]. Higher baseline scores and greater improvement of cognition were significantly associated with lower mortality at 1 year after stroke [12]. Cognitive tests could predict functional outcomes, including daily activities, return to work and driving. Neuropsychological assessment at acute stroke phase could predict functioning at work and fulfilling social roles at 1-year post-stroke [13, 14]. However, previous studies have primarily been cross-sectional, rather than longitudinal. The MoCA was administered within 7 days to > 1 year after stroke [9, 15] with just one timepoint. The studies also had a small sample size [9, 16]. Acute temporary cognitive deficits after minor stroke/TIA are common, and these cognitive deficits may recover to some extent (transient cognitive impairment [TCI]) over time, and are not in line with physical recovery [17]. About 57% patients with TIA/minor stroke have one or more impaired neuropsychological tests within 1 week [18] compared to only 19% of those seen after 7 days [17]. There are both transient and long-term cognitive impairment after TIA [19]. The changes of cognitive impairment after TIA/minor stroke may be improved, stable or declined. The executive dysfunction is a prominent feature after TIA [20]. No previous study has used serial assessment to examine the temporal profile of cognitive impairments at 2 week(2w), 3 month(3 m) and 1 year(1y) after TIA/minor stroke. Additionally, there is no study investigating the association between different cognitive change patterns and functional outcomes after stroke at 1-year follow-up.
A MoCA-Beijing ≤22 has been defined as cognitive impairment at 2 weeks after minor TIA/stroke [21]. In this study, we investigate the relationship between the different cognitive change patterns and 1-year functional outcomes.
Methods and materials
Subjects
The present cohort was from the Impairment of CognitiON and Sleep after acute ischemic stroke or transient ischemic attack in Chinese patients (ICONS) study. ICONS is one of the research subgroups of China National Stroke Registry-III (CNSR-III), which is a nationwide prospective registry for patients presented to hospitals with AIS or TIA between August 2015 and March 2018 from 201 hospitals that covers 22 provinces and four municipalities in China. The detailed design, rationale, and basic description of the CNSR-III have been published previously [22]. We recruited only minor stroke in this study. The minor stroke was defined as the National Institutes of Health Stroke Scale (NIHSS) [23] score ≤ 3. Cognitive function was evaluated by MoCA at 2-week (2w), 3-month (3 m), and 1 year(1y) after TIA/minor stroke in Chinese patients. Functional outcomes were evaluated by Modified Rankin Scale (MRS) and Stroke Impact Scale (SIS-16) at 3-month (3 m) and 1 year(1y).
We excluded the patients who have stroke mimics (ie, seizures, migraine), illiteracy, history of dementia, aphasia, hemispatial neglect, disturbance of consciousness or limb dyskinesia and any major mental conditions that may impede cognitive assessments. Total 2625 patients enrolled in ICONS subgroup with MoCA-2w. We excluded 700 patients with NIHSS>5, and 250 patients without MoCA-3 m score and mRS-3 m data. Finally, 1675 patients of TIA/minor stroke completed MoCA-2w and MoCA-3 m tests, as well as mRS-3 m (Fig. 1). And then, we excluded 621 patients without mRS-1y data. There were 1054 patients with TIA/minor stroke completed MoCA-2w and MoCA-3 m tests, as well as mRS-3 m and mRS-1y (Fig. 1).

Flowchart of patients participating in the study
Data collection
All study investigators were trained and certified to assess NIHSS scores before the beginning of the study. We collected baseline information including patient demographics, vascular risk factors, stroke severity (NIHSS score), stroke management discharge and drugs status. Vascular risk factors included hypertension, diabetes, lipid metabolism disorders, atrial fibrillation, previous stroke or TIA, current or previous smoking and body mass index (BMI) at admission. Etiologic subtypes of ischemic stroke were classified by the Stop Stroke Study Trial of Org 10,172 in Acute Stroke Treatment (SSS-TOAST) classification criteria. In ICONS study, MRI were recommended for all patients, including Diffusion-Weighted Imaging (DWI) with Apparent Diffusion Coefficient (ADC) maps, T1 weighted, T2 weighted, Fluid-attenuated Inversion Recovery (FLAIR), T2*/Susceptibility Weighted Imaging (SWI), and Magnetic Resonance Angiography (MRA). Acute infarction type including single infarction, multiple infarctions, simple watershed infarction and no infarction, and were completed by Imaging experts.
At 2-week or discharge, 3-month and 1-year, MoCA-Beijing [24],Pittsburgh Sleep Quality Index (PSQI) [25], Epworth Sleeping Scale(ESS) [26], Anxiety Disorder-7(GAD-7) [27], and Patient Health Questionnaire-9(PHQ-9) [28] were evaluated face to face [5]. The detailed design, rationale, and basic description of the ICONS have been published previously [29]. All tests above were administered by trained examiners. In the medication survey at each follow-up point, information about whether combined with dual antiplatelet therapy and intravenous thrombolysis after stroke onset was collected.
Outcome assessment
The follow-up was done by face-to-face interview. Patients were asked the standardized follow-up questions at 3 months and 1 year after stroke onset. Outcome data included the scores of mRS and SIS-16. The poor functional outcome was defined as a score of 2 to 6 on the mRS [30] . Poor physical and social functioning was defined as a percentage of SIS-16<25% [31].
Diagnosis of VCI
Patients in this study with MoCA-Beijing ≤22 defined as cognitive impairment after TIA/minor stroke according to the results of our previous study recruited 102 patients after TIA/minor stroke at 2 weeks in China with MoCA-Beijing test and a formal neuropsychological test battery [21]. Our previous data showed that the optimal cutoff point for MoCA-Beijing in discriminating patients with CI from those with no cognitive impairment (NCI) was 22/23 (sensitivity 85%, specificity 88%, PPV = 91%, NPV = 80%). According to the results of cognitive evaluation, we divided patients into 4 groups as mentioned above: A group (no PSCI group): with MoCA-2w >22 and MoCA-3 m>22; B group(improved PSCI group): with MoCA-2w ≤ 22 and MoCA-3 m>22; C group (delayed PSCI group): MoCA-2w >22 and MoCA-3 m ≤ 22; D group (persisting PSCI group): with MoCA-2w ≤ 22 and MoCA-3 m ≤ 22.
Statistical analyses
All statistical analyses were carried out with SAS 9.4 software (SAS Institute Inc., Cary, NC). The differences in baseline demographic and clinical features between NCI and CI were tested for continuous variables with normal distribution using Student-t test and with skewed distribution using nonparametric test. The χ2 or Fisher exact test was used for categorical variables. We analyzed the association between the clinical outcomes including early recurrent stroke, stroke disability and all-cause death and relevant covariates with logistic regression analysis adjusting age, gender, previous stroke, TOAST subtype, acute infarction type, and dual antiplatelet therapy after stroke onset. We have determined that two-tailed p values less than 0.05 was statistically significant.
Results
Baseline characteristics of TIA/minor stroke patients
Among the 2625 patients in the ICONS database, a total of 1675 had completed MoCA-2w, MoCA-3 m tests and mRS-3 m, the baseline and clinical features of the included 1675 patients are demonstrated in Table 1. Overall, the subjects with cognitive impairment (MoCA≤22) accounted for 48.84% of the total studied population at 2 weeks after stroke. Patients were divided into cognitive impairment (CI) group and non-cognitive impairment(NCI) group. The CI group were more likely to be elderly and female. They were also more likely to have a history of stroke, combination of sleep disorders(PSQI>5), depression(PHQ-9>9), and intracranial atherosclerotic stenosis. They have a higher percentage of receiving dual antiplatelet medications after onset. The acute infarction type and stroke etiology was imbalanced between the two groups. No significance was detected in the treatment for hypertension, diabetes mellitus, use of antiplatelet agents and statin.
Comparison of outcomes at 3 months between CI and NCI groups
Table 2 showed the comparison of outcomes at 3 months between CI and NCI groups. CI group have significantly worse stroke outcome (mRS ≥ 2) and SIS-16<25% than those in NCI group. After adjusted for the confounders, there were no statistic differences.
Association of different change patterns of PSCI with clinical outcome at 3 months
The association of different change patterns of PSCI with clinical outcomes after stroke at 3 months is presented in Table 3. In the univariate analysis, data showed that the persisting PSCI was associated with the adverse stroke outcomes at 3 months by higher percentage of mRS ≥ 2 and SIS-16<25% (P < 0.001). After adjusting for age, sex, history of stroke, combination of sleep disorders(PSQI>5), depression(PHQ-9>9), acute infarction type, stroke etiology and other potential confounding factors at baseline, patients with persisting PSCI had an increased risk of poor outcome [adjusted OR (aOR) =1.75; 95% CI, 1.21-2.51] and poor physical and social functioning[adjusted OR (aOR) =1.38; 95% CI, 1.04-1.83] at 3 months(Fig. 2). On the contrary, other 3 groups were not associated with 3-month poor outcome and physical and social functioning in this study.

Association of different change patterns of PSCI with clinical outcome at 3 months
Association of different change patterns of PSCI with clinical outcome at 1 year after adjusted for confounding factors at baseline
The association of different change patterns of PSCI with clinical outcomes after stroke at 1 year is presented in Table 4. About 1054 patients had completed MoCA-2w, MoCA-3 m tests, mRS-3 m and mRS-12 m, the baseline and clinical features of the included 1054 patients are demonstrated in Supplementary File 1. Similarly, in the univariate analysis, data showed that the persisting PSCI was associated with the adverse stroke outcomes at 1 year by higher percentage of mRS ≥ 2 and SIS-16<25% (P < 0.001). After adjusting for age, sex, history of stroke, combination of depression (PHQ-9>9), acute infarction type, stroke etiology and other potential confounding factors at baseline, patients with persisting PSCI had an increased risk of poor outcome [adjusted OR (aOR) =1.88; 95% CI, 1.16-3.05] and poor physical and social functioning [adjusted OR (aOR) =1.68; 95% CI, 1.16-2.43] at 1 year (Fig. 3). There was no significant association between other 3 groups and 1-year poor outcome and physical and social functioning in this study.

Association of different change patterns of PSCI with clinical outcome at 1 year after adjusted for confounding factors at baseline
Comparison of outcomes at 1 year between CI and NCI groups
There were 1054 patients with TIA/minor stroke completed MoCA-2w, MoCA-3 m tests, mRS-3 m and mRS-1y tests. According to the MoCA score, there were 368 patients had cognitive impairment (MoCA≤22) at 3 months. The CI patients have significantly worse stroke outcome (mRS ≥ 2) and SIS-16<25% than those in NCI group at 1 year (Table 5). After adjusted for the confounders at 3 months, the CI group still has dramatically higher percentage of SIS-16<25% than that in NCI group.
Association of different change patterns of PSCI with clinical outcome at 1 year after adjusted for confounding factors at 3 months
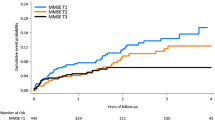
After adjusting for age, sex, history of stroke, combination of intracranial atherosclerotic stenosis, depression (PHQ-9>9), acute infarction type, stroke etiology and other potential confounding factors at 3 months, patients with persisting PSCI had an increased risk of poor outcome [adjusted OR (aOR) =1.77; 95% CI, 1.03-3.03] and poor physical and social functioning [adjusted OR (aOR) =1.69; 95% CI, 1.16-2.47] at 1 year (Table 6 and Fig. 4). There was no significant association between other 3 groups and 1-year poor outcome and physical and social functioning in this study.

Association of different change patterns of PSCI with clinical outcome at 1 year after adjusted for confounding factors at 3 months
Discussion
In the present study, early cognitive impairment was observed in 48.84% of patients with minor stroke/TIA. Previously study reported that the rate of cognitive impairment in stroke patients varied from 21 to 70% [32]. One recent observational study reported that cognitive impairment was detected at Day 7 in 54 of 100 patients (54%) with TIA and minor stroke [8]. Another study reported that cognitive impairment (MoCA < 24) was detected within 5 days in 63% of patients with minor stroke. In the present study, cognitive impairment (MoCA≤22) was observed at 2 weeks in 48.84% of patients with TIA/minor stroke, which is lower than in previous reports. It maybe that our cohort patients were younger than those in previous studies (60 years versus 63 and 70 years in the aforementioned studies). Another reason was that we excluded those patients with pre-stroke dementia. Similar to our study, one Japanese study investigated the cognitive impairment with MoCA in 69 ischemic stroke patients (average age: 73 years), and cognitive impairment defined as a MoCA cutoff score of less than 23 was observed in 39 of 69 patients (57%) within 14 days of onset [33]. The differences might be attributed to the stroke severity, MoCA cutoff scores, and pre-existing cognitive status. The CI group had significantly higher percentage of multiple infarctions than NCI group, consistent with previous studies [34, 35]. Having multiple infarctions, compared with having a single infarction, was significantly associated with post stroke dementia [34]. Multiple brain infarctions have also been suggested to be an important risk factor for dementia. There is also a significant distribution for TOAST classifications between CI and NCI groups. Higher proportions of large-artery atherosclerosis (LAA) and cardioembolism (CE) subtypes are found in patients with CI, consistent with a previous study reporting higher prevalence of cognitive impairments in LAA and CE subtype [36]. The LAA subtype, mostly caused by the occlusion of middle cerebral artery and anterior cerebral artery, and can lead to large infarction in cerebral lobes or strategic infarctions [36,37,38]. LAA subtype and total anterior circulation infarction were correlated with increased PSCI risk at 3 months [36]. These pathologies play a key role in the occurrence of PSCI by causing multifocal emboli involving either bilateral or multilevel structures.
Recent hospital-based cohort studies showed that the MoCA score predicted long-term functional outcome [9]. Previous studies showed that cognitive deficits at 3 months after stroke and incident poststroke dementia to associate with poor outcome [39]. Early MoCA testing could predict 5-year functional impairment (mRS score > 2) and mortality after stroke [9]. Specially, the 14-day visuospatial/executive functions could predict 3-month functional outcomes in stroke patients with endovascular treatment [40]. Early cognitive evaluation after stroke could be affected by many factors such as delirium, tiredness and mood. Thus, using serial assessments for cognitive changes is very important. Some patients might have deteriorated while others improved, or keeping stable, respectively. According to the results and progression of cognitive assessment from 2 weeks to 3 months, we divided patients into 4 groups, and firstly explore the association between PSCI changes and functional outcomes. The present study found that the persisting PSCI type was independently associated with poor functional outcome and physical and social functioning at 3 months and 1 year, even after adjusting for age, sex, history of stroke, combination of sleep disorders, depression, acute infarction type, stroke etiology and other potential confounding factors at baseline. Moreover, the significance of the persisting PSCI to poor function outcome and physical and social functioning remained when adjusted for variables at 3 months. Extending these observations, this founding has a great clinical significance, highlighting the effectiveness of cognitive assessment with the MoCA early, as well as follow-up evaluation later. Early usage of the MoCA in different cognitive regions could predict the PSCI and future functional outcomes, which is important for screening patients with high-risk of poor prognosis and conducting an early intervention [40]. Our findings promote routine cognitive screening test and follow-up assessment after acute stroke. It is possible that in the population with minor stroke (NIHSS<3 scores), the persisting PSCI is a more sensitive predictor of functional dependence in 3-12 months. In addition, it supports the logical assumption that persisting cognitive decline at follow-up is a significant predictor for long-term functional status [41]. These results reveal the significant relationship between persisting PSCI and functional status at 3 and 12 months, even after adjusting for multiple confounding factors, emphasizing the effect of persisting PSCI on one’s ability and physical functioning independent after stroke. The findings of this study could help to identify at risk patients for cognitive decline, who will benefit from early and customized rehabilitation. Such intervention includes therapeutic lifestyle change (e.g., physical exercises, diet and sleep), cognitive training, mood and stress management [42]. The MoCA should be implemented as a crucial part of the routine follow-up clinical assessment. Its early detection of at risk stroke patients will prompt the multidisciplinary rehabilitation team to follow up with comprehensive assessment to customize care, consequently better prognosis [43].
This study shows that early cognitive screening and follow-up assessment using MoCA after stroke adds to the prediction of functional outcome up to 1 years after the event. This may partly be associated with the influence of cognitive impairment on the performance of daily activities and complexity. Previous study considered that the poor functional performance might relate to poorer adherence to treatment guidelines for PSCI patients and to have limited access to rehabilitation programs. However, in this study, we put the drug adherence into the logistic regression, still we found that the persisting PSCI still have a poor outcome at 12 months after stroke onset. It implied that the persisting PSCI patients have special pathological mechanisms from others. Hence, the persisting MoCA score ≤ 22 from baseline to 3 months might identify patients requiring special attention.
In addition, our results support the feasibility and routine use of the MoCA early after stroke. It takes about 10 minutes to rate [44], and is appropriate for stroke patients’ cognitive screening [45]. It could better reflect the underlying vascular pathology than other cognitive screening tools [46]. Besides, there are strong arguments for serial MoCA tests for cognitive follow-ups after hospital admission.
The present study had some limitations. Firstly, our study might not be fully representative of stroke in general because this study excluded patients with history of dementia and recruited patients with mild stroke. Secondly, only 24% of patients were women in the current study. Though gender was pooled into the final model, caution was needed regarding generalizability. This finding may not be generalizable to major stroke patients. Thirdly, depressive mood disorders, anxiety and delirium may have affected early cognitive performance. This condition may have an impact on functional outcome. However, serial MoCA tests were conducted at 2 weeks and 3 months, which may reduce the bias. Fourthly, we did not find statistically significantly differences in intravenous thrombolysis between CI and NCI groups. A previous study showed that intravenous thrombolysis with alteplase could improve the MMSE score at acute phase significantly than the control group [47]. However, a longitudinal study in alteplase treatment was inconsistent because the load of CMBs had been associated with cognitive impairment [48]. Thus, further studies are needed to explore the relationship between intravenous thrombolysis and PSCI. Fifthly, only a minority of patients (n = 10, 0.71%) used drug-treatment to improve cognition, such as donepezil (n = 9) and memantine(n = 1), which might influence PSCI trajectory. Therefore, the evidence of cognitive treatment was insufficient to make statistical comparisons. Additionally, this study did not collect information on physiotherapy [49] or language therapy [50], which might have an impact on cognitive changes. Further studies on relationships between treatment or rehabilitation, as well as PSCI are needed.
In conclusion, this study shows that the persisting PSCI is a strong predictor of l-year functional outcome. Patients with persisting PSCI should be given special attention. Our findings promote the use of MoCA as a routine clinical tool to identify high-risk patients in the setting of acute stroke, particularly given its brevity of administration.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. We are unable to deposit the data in a publicly available source because there are ongoing studies using this data.
Change history
30 March 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12877-023-03763-y
References
MacKenzie G, Gould L, Ireland S, LeBlanc K, Sahlas D. Detecting cognitive impairment in clients with mild stroke or transient ischemic attack attending a stroke prevention clinic. Can J Neurosci Nurs. 2011;33:47–50.
Jokinen H, Melkas S, Ylikoski R, Pohjasvaara T, Kaste M, Erkinjuntti T, et al. Post-stroke cognitive impairment is common even after successful clinical recovery. Eur J Neurol. 2015;22:1288–94.
Lim KB, Kim J, Lee HJ, Yoo J, You EC, Kang J. Correlation between Montreal cognitive assessment and functional outcome in subacute stroke patients with cognitive dysfunction. Ann Rehabil Med. 2018;42:26–34.
Hachinski V, Iadecola C, Petersen RC, Breteler MM, Nyenhuis DL, Black SE, et al. National institute of neurological disorders and stroke-Canadian stroke network vascular cognitive impairment harmonization standards. Stroke. 2006;37:2220–41.
Duncan PW, Lai SM, Bode RK, Perera S, DeRosa J. Stroke impact scale-16: a brief assessment of physical function. Neurology. 2003;60:291–6.
Lai SM, Studenski S, Duncan PW, Perera S. Persisting consequences of stroke measured by the stroke impact scale. Stroke. 2002;33:1840–4.
Baba SS, Yarube IU. Raised high-sensitivity c-reactive protein and cognitive impairment among african stroke survivors within the first three months following stroke. J Clin Neurosci. 2021;88:191–6.
Sivakumar L, Kate M, Jeerakathil T, Camicioli R, Buck B, Butcher K. Serial Montreal cognitive assessments demonstrate reversible cognitive impairment in patients with acute transient ischemic attack and minor stroke. Stroke. 2014;45:1709–15.
Zietemann V, Georgakis MK, Dondaine T, Müller C, Mendyk AM, Kopczak A, et al. Early Moca predicts long-term cognitive and functional outcome and mortality after stroke. Neurology. 2018;91:e1838–50.
Kwon HS, Lee D, Lee MH, Yu S, Lim JS, Yu KH, et al. Post-stroke cognitive impairment as an independent predictor of ischemic stroke recurrence: Picasso sub-study. J Neurol. 2020;267:688–93.
Suda S, Nishimura T, Ishiwata A, Muraga K, Aoki J, Kanamaru T, et al. Early cognitive impairment after minor stroke: associated factors and functional outcome. J Stroke Cerebrovasc Dis. 2020;29:104749.
Weng SC, Hsu CY, Shen CC, Huang JA, Chen PL, Lin SY. Combined functional assessment for predicting clinical outcomes in stroke patients after post-acute care: a retrospective multi-center cohort in Central Taiwan. Front Aging Neurosci. 2022;14:834273.
Arsić S, Konstantinović L, Eminović F, Pavlović D. Correlation between demographic characteristics, cognitive functioning and functional independence in stroke patients. Srp Arh Celok Lek. 2016;144:31–7.
Slavin SJ, McCune-Richardson L, Moore J, Ecklund-Johnson E, Gronseth GS, Akinwuntan A. Cognitive testing during mild acute ischemic stroke predicts long-term return to work. J Stroke Cerebrovasc Dis. 2022;31:106132.
Dong Y, Slavin MJ, Chan BP, Venketasubramanian N, Sharma VK, Crawford JD, et al. Cognitive screening improves the predictive value of stroke severity scores for functional outcome 3-6 months after mild stroke and transient ischaemic attack: an observational study. BMJ Open. 2013;3:e003105.
Tveiten A, Ljøstad U, Mygland Å, Naess H. Functioning of long-term survivors of first-ever intracerebral hemorrhage. Acta Neurol Scand. 2014;129:269–75.
Pendlebury ST, Wadling S, Silver LE, Mehta Z, Rothwell PM. Transient cognitive impairment in tia and minor stroke. Stroke. 2011;42:3116–21.
Sörös P, Harnadek M, Blake T, Hachinski V, Chan R. Executive dysfunction in patients with transient ischemic attack and minor stroke. J Neurol Sci. 2015;354:17–20.
Ganesh A, Barber PA. The cognitive sequelae of transient ischemic attacks-recent insights and future directions. J Clin Med. 2022;11:2637.
O'Brien JT. Vascular cognitive impairment. Am J Geriatr Psychiatry. 2006;14:724–33.
Zuo L, Dong Y, Zhu R, Jin Z, Li Z, Wang Y, et al. Screening for cognitive impairment with the Montreal cognitive assessment in chinese patients with acute mild stroke and transient ischaemic attack: a validation study. BMJ Open. 2016;6:e011310.
Wang Y, Jing J, Meng X, Pan Y, Wang Y, Zhao X, et al. The third China national stroke registry (cnsr-iii) for patients with acute ischaemic stroke or transient ischaemic attack: design, rationale and baseline patient characteristics. Stroke Vasc Neurol. 2019;4:158–64.
Fischer U, Baumgartner A, Arnold M, Nedeltchev K, Gralla J, De Marchis GM, et al. What is a minor stroke? Stroke. 2010;41:661–6.
Wen HB, Zhang ZX, Niu FS, Li L. The application of Montreal cognitive assessment in urban chinese residents of Beijing. Zhonghua Nei Ke Za Zhi. 2008;47:36–9.
Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213.
Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14:540–5.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the gad-7. Arch Intern Med. 2006;166:1092–7.
Kroenke K, Spitzer RL, Williams JB. The phq-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Liao XL, Zuo LJ, Zhang N, Yang Y, Pan YS, Xiang XL, et al. The occurrence and longitudinal changes of cognitive impairment after acute ischemic stroke. Neuropsychiatr Dis Treat. 2020;16:807–14.
Weisscher N, Vermeulen M, Roos YB, de Haan RJ. What should be defined as good outcome in stroke trials; a modified Rankin score of 0-1 or 0-2? J Neurol. 2008;255:867–74.
Duncan PW, Bode RK, Min Lai S, Perera S. Rasch analysis of a new stroke-specific outcome scale: the stroke impact scale. Arch Phys Med Rehabil. 2003;84:950–63.
Moran GM, Fletcher B, Feltham MG, Calvert M, Sackley C, Marshall T. Fatigue, psychological and cognitive impairment following transient ischaemic attack and minor stroke: a systematic review. Eur J Neurol. 2014;21:1258–67.
Takahashi Y, Saito S, Yamamoto Y, Uehara T, Yokota C, Sakai G, et al. Visually-rated medial temporal lobe atrophy with lower educational history as a quick indicator of amnestic cognitive impairment after stroke. J Alzheimers Dis. 2019;67:621–9.
Kumral E, Bayam FE, Arslan H, Orman M. Associations between neuroanatomic patterns of cerebral infarctions and vascular dementia. J Neuropsychiatr Clin Neurosci. 2021;33:49–56.
Zhang L, Li Y, Bian L, Luo Q, Zhang X, Zhao B. Cognitive impairment of patient with neurological cerebrovascular disease using the artificial intelligence technology guided by mri. Front Public Health. 2021;9:813641.
Clery A, Bhalla A, Rudd AG, Wolfe CDA, Wang Y. Trends in prevalence of acute stroke impairments: a population-based cohort study using the South London stroke register. PLoS Med. 2020;17:e1003366.
Kalaria RN, Akinyemi R, Ihara M. Stroke injury, cognitive impairment and vascular dementia. Biochim Biophys Acta. 2016;1862:915–25.
He M, Wang J, Liu N, Xiao X, Geng S, Meng P, et al. Effects of blood pressure in the early phase of ischemic stroke and stroke subtype on poststroke cognitive impairment. Stroke. 2018;49:1610–7.
Desmond DW, Moroney JT, Sano M, Stern Y. Mortality in patients with dementia after ischemic stroke. Neurology. 2002;59:537–43.
Zhang M, Wang K, Xie L, Pan X. Short-term Montreal cognitive assessment predicts functional outcome after endovascular therapy. Front Aging Neurosci. 2022;14:808415.
Abzhandadze T, Rafsten L, Lundgren Nilsson Å, Palstam A, Sunnerhagen KS. Very early Moca can predict functional dependence at 3 months after stroke: a longitudinal, cohort study. Front Neurol. 2019;10:1051.
Reynolds CF 3rd, Jeste DV, Sachdev PS, Blazer DG. Mental health care for older adults: recent advances and new directions in clinical practice and research. World Psychiatry. 2022;21:336–63.
Kim CK, Sachdev PS, Braidy N. Recent neurotherapeutic strategies to promote healthy brain aging: are we there yet? Aging Dis. 2022;13:175–214.
Quinn TJ, Elliott E, Langhorne P. Cognitive and mood assessment tools for use in stroke. Stroke. 2018;49:483–90.
Burton L, Tyson SF. Screening for cognitive impairment after stroke: a systematic review of psychometric properties and clinical utility. J Rehabil Med. 2015;47:193–203.
Zamboni G, Griffanti L, Jenkinson M, Mazzucco S, Li L, Küker W, et al. White matter imaging correlates of early cognitive impairment detected by the Montreal cognitive assessment after transient ischemic attack and minor stroke. Stroke. 2017;48:1539–47.
Gao L, Zhang S, Wo X, Shen X, Tian Q, Wang G. Intravenous thrombolysis with alteplase in the treatment of acute cerebral infarction. Pak J Med Sci. 2022;38:498–504.
Jabłoński B, Gójska-Grymajło A, Ossowska D, Szurowska E, Wyszomirski A, Rojek B, et al. New remote cerebral microbleeds on t2(*)-weighted echo planar mri after intravenous thrombolysis for acute ischemic stroke. Front Neurol. 2021;12:744701.
Zou L, Sasaki JE, Zeng N, Wang C, Sun L. A systematic review with meta-analysis of mindful exercises on rehabilitative outcomes among poststroke patients. Arch Phys Med Rehabil. 2018;99:2355–64.
Park K, Moon S. Informative and semantic language features of people with dementia displayed during reminiscence therapy. Psychogeriatrics. 2022;22:843-850.
Acknowledgements
The authors would like to thank all participants for their involvement.
Funding
This work was supported by the following institutions: the National Key Research and Development Program of China (2020YFC2004800) and Beijing Excellent Talents Training Program (2018000021469G237).
This work was performed at Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
Author information
Authors and Affiliations
Contributions
LX and ZL: drafting/revising the manuscript, study concept or design, analysis or interpretation of data, accepts responsibility for conduct of research and will give final approval, acquisition of data, statistical analysis. DY, PY, YH, MX, LH, ZX and WY: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. SJ: assistance with early design, critical review of the analysis and manuscript. WY: study concept or design, analysis or interpretation of data, accepts responsibility for conduct of research and will give final approval, acquisition of data, statistical analysis, study supervision. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol of the ICONS study and consent forms were also approved by ethics committee at Beijing Tiantan Hospital and all participating centers. Separate written informed consent was also obtained. Studies were conducted in accordance with the Declaration of Helsinki. The ethics approval number was KY2015-001-01.
Consent for publication
Not applicable.
Competing interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: in the Funding section, the number belonging to the National Key Research and Development Program of China was incorrectly given as ‘2017YFC1308404' and should have read ‘2020YFC2004800’.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liao, X., Zuo, L., Dong, Y. et al. Persisting cognitive impairment predicts functional dependence at 1 year after stroke and transient ischemic attack: a longitudinal, cohort study. BMC Geriatr 22, 1009 (2022). https://doi.org/10.1186/s12877-022-03609-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03609-z