
Abstract
Background
Tooth loss has been reportedly associated with shorter disability-free life expectancy (DFLE). However, no study has explored whether oral self-care offsets reduction in DFLE. The present study aimed to assess the association between oral self-care and DFLE in older individuals with tooth loss.
Methods
Data on the 13-year follow-up from a cohort study of 14,206 older Japanese adults aged ≥ 65 years in 2006 were analyzed. Information on the number of remaining teeth was collected using a questionnaire, and the participants were then categorized into three groups (0–9, 10–19, and ≥ 20 teeth). Additionally, “0–9” and “10–19” groups were divided into two subgroups based on whether they practiced oral self-care. DFLE was defined as the average number of years a person could expect to live without disability, and was calculated by the multistate life table method based on a Markov model.
Results
DFLE (95% confidence interval) was 19.0 years (18.7–19.4) for 0–9 teeth, 20.1 (19.7–20.5) for 10–19 teeth, and 21.6 (21.2–21.9) for ≥ 20 teeth for men. For women, DFLE was 22.6 (22.3–22.9), 23.5 (23.1–23.8), and 24.7 (24.3–25.1), respectively. Practicing oral self-care was associated with longer DFLE, by 1.6–1.9 years with brushing ≥ 2 times a day in people with 0–9 and 10–19 teeth, and by 3.0–3.1 years with the use of dentures in those with 0–9 teeth.
Conclusions
Practicing oral self-care is associated with an increase in DFLE in older people with tooth loss.
Similar content being viewed by others


Background
According to a United Nations forecast, the global population aged 60 years and over will triple, from 0.7 billion in 2009 to 2 billion in 2050 [1]. This rapid increase in the older population will lead to a higher prevalence of such chronic conditions as dependence in activities of daily living (ADL) and dementia, thus compromising people’s quality of life (QOL) and increasing the burden on social security. In this context, extending healthy life expectancy (HLE) has become the global public health goal. Previous studies have identified modifiable factors for extending HLE, including blood pressure control, weight control, non-smoking, physical activity, social participation, and so forth [2, 3].
Oral health is a leading candidate for extending HLE, because past studies agreed that there were inverse relations between the number of remaining teeth and mortality risk, incident risks of physical disability, and dementia [4,5,6]. These findings suggest that a smaller number of remaining teeth would be associated with shorter HLE. To the best of our knowledge, there has been only one study that investigated the association between the number of remaining teeth and HLE. Matsuyama et al. reported that having more remaining teeth was associated with longer HLE in a population of older people in Japan [7]. However, they did not examine the impact of oral self-care on HLE.
We previously reported that practicing oral health care was inversely associated with mortality and disability incidence in older people with tooth loss [8, 9]. In participants with 0–19 teeth, the mortality risk of those practicing oral care decreased by about 46% compared with participants who did not practice oral care [8], and participants with 0–19 teeth without regular dental care had a greater risk of functional disability by approximately 46% than those with ≥ 20 teeth [9].
Because practicing good oral self-care could offset the detrimental effect of shorter DFLE from tooth loss, we can see its benefit in extending HLE. To the best of our knowledge, no study has investigated this association. Clarifying how oral self-care affects HLE would provide an inexpensive method for healthy aging since oral self-care is categorized as primary prevention and can be promoted as population-based prevention.
Therefore, the present study aimed to investigate the association between the number of remaining teeth and the extension of HLE, using a 13-year follow-up of a community-based, large-scale (N = 14,206) cohort study of older Japanese adults. The impact of oral self-care on HLE in those with tooth loss was also examined. Of the various definitions of HLE, the present study focused on disability-free life expectancy (DFLE), which is defined as the average number of years that a person can expect to live without disability because data on the incidence of disability are available from long-term care insurance (LTCI) information.
Methods
Study cohort
The details of the Ohsaki Cohort 2006 Study have been introduced previously [10]. In brief, the source population for the baseline survey was all older residents (i.e., 31,694 men and women) living in Ohsaki City, Miyagi Prefecture, Japan aged ≥ 65 years in December 1, 2006 [10]. The questionnaire survey included items on the number of remaining teeth, body weight, height, smoking status, time spent walking, educational status, and history of hypertension, diabetes mellitus, stroke, myocardial infarction, and cancer.
The baseline survey was conducted between December 1 and 15, 2006, with questionnaires distributed by the heads of individual administrative districts and then collected by mail [10]. Follow-up started from December 16, 2006 until November 30, 2019. For the present analyses, the study cohort consisted of 23,091 participants who provided valid responses. Then 6,333 participants who had not provided written consent for a review of their LTCI information, 1,979 who had already been certified as having a disability by the LTCI (Support Level 1 or higher) before the beginning of follow-up, five who had died or moved before the beginning of follow-up, and 568 whose data about the number of remaining teeth were missing were excluded. The characteristics of those who did not provide written consent for a review of their LTCI information are shown (Supplementary Table 1). Eventually, 14,206 participants were included for the present analyses (Fig. 1).

Flowchart of study participants
Exposure (number of remaining teeth)
In the baseline questionnaire, respondents were asked to classify the number of their remaining teeth into six categories: none (0 teeth), few (1–9 teeth), about half (10–19 teeth), moderate (20–24 teeth), most (25–27 teeth), and all (28 teeth). The respondents were then divided into three groups: (1) 0–9 teeth, (2) 10–19 teeth, and (3) ≥ 20 teeth. Whether they used dentures and whether they visited a dental clinic for dental checkups at least once a year were also asked. The respondents were asked to mark ‘yes’ or ‘no’ in reply. How many times participants brushed their teeth daily was also included as a question.
Outcomes
The study outcomes were incident disability according to national standards (LTCI Care Level 2 or higher: limited in performing ADL) and death [10]. With these data, DFLE, which was defined as the average number of years that a person could expect to live without disability, was calculated.
LTCI in Japan is a mandatory social insurance system that is meant to help frail older individuals carry out ADL. Everyone aged ≥ 40 years pays a premium, and everyone aged ≥ 65 years is eligible for formal caregiving services depending on the level (Support Level 1–2, and Care Level 1–5). LTCI certification was found to be associated with the ability to perform ADL in a community-based study [11], and it has been used in epidemiologic studies as a measure of incident functional disability in older individuals [12, 13]. Data regarding incident functional disability, death, or emigration during follow-up were transferred from the Ohsaki City Government through an agreement about the secondary use of data. All data were transferred from the Ohsaki City Government yearly each December under the agreement on Epidemiologic Research and Privacy Protection.
The multistate life table (MSLT) method
The MSLT method was used to analyze HLE [14]. In the present analysis, a Markov transition model for disability and mortality had three states; two non-absorbing states (non-disabled and disabled) and one absorbing state (dead). In the model, four possible health transitions over time were shown as follows: (a) from non-disabled to disabled (the incidence of a disabled status); (b) from disabled to non-disabled (recovery from a disabled status); (c) from non-disabled to dead; and (d) from disabled to dead. In this model, retention status was allowed for the non-disabled and disabled states. (i.e., remaining in disabled status and in disability-free status are another two health transition pathways.) The emigrants after the beginning of the follow-up were included in the calculations.
Statistical analysis
The DFLE in both non-disabled and disabled states was computed using Interpolated Markov Chain (IMaCh) software (version 0.98r7), which was developed at the Institut national d’études démographiques by Brouard and Lièvre [15]. This well-known software package has been widely used in several recent studies to compute HLE [16,17,18]. The program has been described in detail in a previous paper [19], so only a brief description is provided here. In the present analysis, a Markov model was created to calculate DFLE. Four age- and group-specific transition probabilities of the Markov model were estimated using multinomial logistic regression. These probabilities were implemented in the MSLT, and the total life expectancy (TLE), DFLE, and disable life expectancy (DLE) were calculated for each subgroup. The participants were categorized into three groups according to the number of remaining teeth. Group-specific DFLEs were then calculated using IMaCh.
Moreover, in this analysis, whether DFLE differed among participants with a fewer number of remaining teeth was examined depending on whether they practiced oral self-care (‘tooth brushing ≥ 2 times per day’, ‘use of dentures’, and ‘taking dental checkups’ being defined as ‘practicing oral self-care’). For this, participants were divided into the following five categories based on three oral self-care measures: (1) ‘non-practicing and having 0–9 teeth’; (2) ‘practicing and having 0–9 teeth’; (3) ‘non-practicing and having 10–19 teeth’; (4) ‘practicing oral self-care and having 10–19 teeth’; and (5) ‘having ≥ 20 teeth’.
Instead of adjusting confounders in the IMaCh program, four stratified analyses were performed, by smoking status (never or former vs. current), body mass index (BMI) (18.5 ≤ BMI < 25.0 vs. BMI < 18.5 or BMI ≥ 25.0 kg/m2), time spent walking (≥ 0.5 vs. < 0.5 h/day), and educational status (junior high school or less vs. high school or higher) Furthermore, the effect of oral self-care on DFLE stratified by smoking status, BMI, time spent walking, and educational status were analyzed.
All MSLT methods were performed using the IMaCh software program, and the data preparation and description were made by SAS version 9.4 (SAS Inc., Cary, NC, USA).
Results
Participants’ characteristics
A total of 14,206 participants (men: 45.1%) were included in the present analysis, and their mean age (standard deviation) was 73.9 (6.0) years. Only 612 individuals were lost to follow-up because they emigrated from the study area, with a follow-up rate of 95.7%.
Table 1 shows the baseline characteristics according to the number of remaining teeth. Participants in the “0–9 teeth” group were older than other groups, and participants with more remaining teeth were less likely to be female, to be current smokers and to walk < 0.5 h/day, and more likely to practice oral self-care including daily brushing, use of dentures, and regular dental checkup.
At the end of follow-up in 2019, 47.7% were non-disabled, 9.9% were disabled, and 38.1% were dead. Table 2 also shows the sex-specific distribution of outcomes by the number of remaining teeth. Participants with more remaining teeth had a higher proportion of being non-disabled in both men and women.
Association between the number of remaining teeth and disability-free life expectancy (DFLE)
Table 3 shows DFLE, DLE, and TLE by the number of remaining teeth for men and women at age 65 years. The number of remaining teeth was associated with longer DFLE and TLE for both sexes. DFLE (95% confidence interval) was 19.0 years (18.7–19.4) for “0–9 teeth”, 20.1 (19.7–20.5) for “10–19 teeth”, and 21.6 (21.2–21.9) for “ ≥ 20 teeth” for men, and 22.6 (22.3–22.9), 23.5 (23.1–23.8), and 24.7 (24.3–25.1), respectively, for women. The difference in DFLE between the “0–9 teeth” group and the “ ≥ 20 teeth” group was about 2 years for both sexes (19.0 vs. 21.6 years for men and 22.6 vs. 24.7 years for women).
Table 4 shows DFLE, DLE, and TLE by the number of remaining teeth for men and women at age 65 years by frequency of brushing teeth a day. There was about a 2-year difference in DFLE between those who brushed < 2 times a day and those ≥ 2 times (men: 18.5 vs. 20.1 years; women: 21.7 vs. 23.3 in the “0–9 teeth”, men: 19.3 vs. 21.1 years; women: 22.3 vs. 24.2 in the “10–19 teeth”). In addition, we also compared those who brushed once a day and those ≥ 2 times, differences of DFLE were almost the same as seen in Table 4 (Supplementary Table 2).
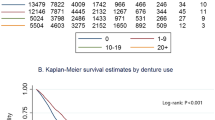
Table 5 shows DFLE, DLE, and TLE by the number of remaining teeth for men and women at age 65 years with or without the use of dentures. There was about a 3-year difference in DFLE between those without and with the use of dentures in the “0–9 teeth” group (men: 16.2 vs. 19.3 years; women: 19.8 vs. 22.8). In the “10–19 teeth” group, the difference in DFLE was small (men: 19.5 vs. 20.3 years; women: 22.8 vs. 23.6).
Table 6 shows that there was about 0.5-year difference in DFLE depending on dental checkups (men: 18.9 vs. 19.5 years; women: 22.5 vs. 22.9 in the “0–9 teeth”, men: 19.9 vs. 20.6 years; women: 23.3 vs. 24.0 in the “10–19 teeth”).
Stratified analysis
Lifestyle factors including smoking status, BMI and time spent walking, and educational status may affect the association between the number of remaining teeth and DFLE. Thus, several stratified analyses were performed by those factors. A consistent association between the number of remaining teeth and DFLE, and an extension of DFLE with daily brushing and use of dentures was also observed, when the participants were stratified by smoking status (Supplementary table 3–5), BMI (Supplementary table 6–8), time spent walking (Supplementary table 9–11), or educational status (Supplementary table 12–14).
Discussion
In the present study, we estimated DFLEs according to the number of remaining teeth using the data from a cohort study of 14,206 older Japanese men and women aged 65 years or older followed-up for 13 years. DFLE was longer by 2 years in participants with ≥ 20 teeth than those with 0–9 teeth in both men and women. The association between the number of remaining teeth and DFLE did not change greatly after the participants were stratified by smoking status, BMI, time spent walking, and educational status. To our knowledge, this is the first study to investigate the association of the number of remaining teeth and oral self-care with DFLE.
The present result is consistent with the previous study that showed that there was an association between the number of remaining teeth and DFLE [9]. It was further demonstrated that oral self-care may contribute to the extension of DFLE even among older people with tooth loss. Moreover, the difference in DFLE between those with oral self-care and those without it among people with relatively less teeth was also analyzed. When the impact of brushing was investigated, the difference in DFLE between < 2 times/day and ≥ 2 times/day was 1.6 years in the 0–9 teeth group and about 2 years in the 10–19 teeth group. As for the use of dentures, the difference in DFLE between with and without dentures was about 3 years in the 0–9 teeth group and about 1 year in the 10–19 teeth group. From the above, use of dentures seems to alleviate the adverse effect of worse dentition status on DFLE if severe, and it may be more effective for those having much fewer teeth. With respect to dental checkups, the difference in DFLE between with and without checkups was about 0.5 years in both the 0–9 teeth and the 10–19 teeth group. Therefore, promoting oral self-care may extend HLE even when the number of remaining teeth is reduced.
There are several possible pathways linking oral self-care to the extension of DFLE. In this study, use of dentures had a stronger effect on DFLE than those of daily brushing and dental checkups in “0–9” group. Denture can directly affect chewing and swallowing when eating, the support of which may be more fundamental especially in those with severe tooth loss. Tooth brushing would clean up the oral microbiota, which is associated with an increased risk of pneumonia in older people [20]. Possible mechanisms also include the possibility that chewing and swallowing are directly related to cognitive function [21,22,23]. In addition, denture use would improve chewing and swallowing, thus increasing the amount and kinds of food intake and improving nutritional status [24], eventually preventing sarcopenia [25]. Furthermore, tooth brushing would alleviate oral inflammation, thus decreasing the risk of such systemic diseases as cardiovascular events [26], Alzheimer's disease [27], and obesity [28].
Oral health is a neglected issue on the global health agenda, so it was an important advance when a resolution on oral health was adopted at WHO’s 2021 World Health Assembly [29]. The resolution demands nations to provide a basis for a healthy mouth, where no one is left behind, and to develop “best-buy” interventions for oral health [30]. In the context of this resolution, oral self-care is certainly the “best-buy” option because the present result suggests that it could increase DFLE by about 2 years, preventing the deterioration of QOL including functional disability or onset of disease, and saving tremendous costs of medication and welfare.
The present study had some strengths. First, it was a large population-based cohort study involving 14,206 persons. Second, few participants were lost during follow-up (4.3%).
Some limitations need to be mentioned. First, not all candidates had applied for LTCI certification, and provided consent for a review to their LTCI information. However, we compared baseline characteristics of study participants and those who did not agree to the review to their LTCI information (Supplementary Table 1). Those who agreed to the review to their LTCI information were more likely to be male, to have higher education, but to have medical history of hypertension, myocardial infarction, stroke, and cancer. These results were statistically significant, although the differences were not substantive. Thus, we cannot completely exclude the possibility of selection bias in the present study. Second, information on the number of remaining teeth and dental health behaviors were only assessed once at baseline in the present study, but these variables may change over time. It is also worthwhile to investigate the differences in DFLEs among people with different patterns of changes in oral care habits (e.g., unchanged, decreased, or increased frequency of teeth brushing or dental check-ups), obtained by multiple assessments of variables.
Conclusions
The results of this study suggest the substantial impact of the number of remaining teeth on longer DFLE among older people. A 2-year difference in DFLE was observed between those who had 0–9 teeth compared with those who had ≥ 20 teeth; this association was consistent for both men and women. In addition, oral self-care could have a great positive impact on the extension of DFLE of those with fewer teeth. Therefore, promoting oral self-care may extend HLE even when the number of remaining teeth is decreased. These findings suggest that maintaining the number of remaining teeth and promoting oral self-care at the population level could increase life-years lived in good health among community-dwelling older people.
Availability of data and materials
Data described in the manuscript, code book, and analytic code will not be made publicly available because private information of participants were included but are available from the corresponding author on reasonable request.
Abbreviations
- HLE:
-
Healthy life expectancy
- DFLE:
-
Disability-free life expectancy
- ADL:
-
Activities of daily living
- TLE:
-
Total life expectancy
- DLE:
-
Disabled life expectancy
- LTCI:
-
Long-term care insurance
- MSLT:
-
Multistate life table
- BMI:
-
Body mass index
- IMaCh:
-
Interpolated Markov Chain
- CI:
-
Confidence interval
- QOL:
-
Quality of life
References
the United Nations, Department of economic and social affairs. World population policies. 2009. https://www.un.org/en/development/desa/population/publications/pdf/policy/wpp.pdf. Accessed 24 Oct 2022.
Forouzanfar MH, Afshin A, Alexander LT, Anderson HR, Bhutta ZA, Biryukov S, Brauer M, Burnett R, Cercy K, Charlson FJ, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1659–724.
Matsuyama S, Murakami Y, Lu Y, Sone T, Sugawara Y, Tsuji I: Association between social participation and disability-free life expectancy in Japanese older people: the Ohsaki Cohort 2006 Study. J Epidemiol. 2021.
Peng J, Song J, Han J, Chen Z, Yin X, Zhu J. The relationship between tooth loss and mortality from all causes, cardiovascular diseases, and coronary heart disease in the general population: systematic review and dose-response meta-analysis of prospective cohort studies. Biosci Rep. 2019;39(1):BSR20181773.
Komiyama T, Ohi T, Miyoshi Y, Murakami T, Tsuboi A, Tomata Y, Tsuji I, Watanabe M, Hattori Y. Relationship between status of dentition and incident functional disability in an elderly Japanese population: prospective cohort study of the Tsurugaya project. J Prosthodont Res. 2018;62(4):443–8.
Chen J, Ren CJ, Wu L, Xia LY, Shao J, Leng WD, Zeng XT. Tooth Loss Is Associated With Increased Risk of Dementia and With a Dose-Response Relationship. Front Aging Neurosci. 2018;10:415.
Matsuyama Y, Aida J, Watt RG, Tsuboya T, Koyama S, Sato Y, Kondo K, Osaka K. Dental Status and Compression of Life Expectancy with Disability. J Dent Res. 2017;96(9):1006–13.
Hayasaka K, Tomata Y, Aida J, Watanabe T, Kakizaki M, Tsuji I. Tooth loss and mortality in elderly Japanese adults: effect of oral care. J Am Geriatr Soc. 2013;61(5):815–20.
Komiyama T, Ohi T, Miyoshi Y, Murakami T, Tsuboi A, Tomata Y, Tsuji I, Watanabe M, Hattori Y. Association Between Tooth Loss, Receipt of Dental Care, and Functional Disability in an Elderly Japanese Population: The Tsurugaya Project. J Am Geriatr Soc. 2016;64(12):2495–502.
Kuriyama S, Nakaya N, Ohmori-Matsuda K, Shimazu T, Kikuchi N, Kakizaki M, Sone T, Sato F, Nagai M, Sugawara Y, et al. The Ohsaki Cohort 2006 Study: design of study and profile of participants at baseline. J Epidemiol. 2010;20(3):253–8.
Arai Y, Zarit SH, Kumamoto K, Takeda A. Are there inequities in the assessment of dementia under Japan’s LTC insurance system? Int J Geriatr Psychiatry. 2003;18(4):346–52.
Hozawa A, Sugawara Y, Tomata Y, Kakizaki M, Ohmori-Matsuda K, Nakaya N, Kuriyama S, Fukao A, Tsuji I. Relationships between N-terminal pro B-type natriuretic peptide and incident disability and mortality in older community-dwelling adults: the Tsurugaya study. J Am Geriatr Soc. 2010;58(12):2439–41.
Matsuyama S, Zhang S, Tomata Y, Abe S, Tanji F, Sugawara Y, Tsuji I. Association between improved adherence to the Japanese diet and incident functional disability in older people: The Ohsaki Cohort 2006 Study. Clin Nutr. 2020;39(7):2238–45.
Rogers A, Rogers RG, Branch LG. A multistate analysis of active life expectancy. Public Health Rep. 1989;104(3):222–6.
Brouard N. Computing health expectancies using IMaCh (a maximum likelihood computer program using interpolation of Markov chains), Version 0.71a. Institut National d'Etudes Demographiques (INED, Paris) and EUROREVES; 2002. https://euroreves.ined.fr/imach/doc/imachold.htm. Accessed 24 Oct 2022.
Yong V, Saito Y. Are there education differentials in disability and mortality transitions and active life expectancy among Japanese older adults? Findings from a 10-year prospective cohort study. J Gerontol B Psychol Sci Soc Sci. 2012;67(3):343–53.
Crimmins EM, Hayward MD, Hagedorn A, Saito Y, Brouard N. Change in disability-free life expectancy for Americans 70-years-old and older. Demography. 2009;46(3):627–46.
Jagger C, Matthews R, Melzer D, Matthews F, Brayne C, Mrc C. Educational differences in the dynamics of disability incidence, recovery and mortality: findings from the MRC Cognitive Function and Ageing Study (MRC CFAS). Int J Epidemiol. 2007;36(2):358–65.
Lièvre A, Brouard N, Heathcote C. The estimation of health expectancies from cross-longitudinal surveys. Math Popul Stud. 2003;10(4):211–48.
Kageyama S, Takeshita T, Furuta M, Tomioka M, Asakawa M, Suma S, Takeuchi K, Shibata Y, Iwasa Y, Yamashita Y. Relationships of variations in the tongue microbiota and pneumonia mortality in nursing home residents. J Gerontol A Biol Sci Med Sci. 2018;73(8):1097–102.
Jo SY, Hwang JW, Pyun SB. Relationship between cognitive function and dysphagia after stroke. Ann Rehabil Med. 2017;41(4):564–72.
Muhle P, Claus I, Labeit B, Ogawa M, Dziewas R, Suntrup-Krueger S, Warnecke T. Effects of cognitive and motor dual-tasks on oropharyngeal swallowing assessed with FEES in healthy individuals. Sci Rep. 2020;10(1):20403.
Winchester J, Winchester Carol G. Cognitive dysphagia and effectively managing the five systems. Perspect Gerontol. 2015;20(3):116–32.
Kazemi S, Savabi G, Khazaei S, Savabi O, Esmaillzadeh A, Keshteli AH, Adibi P. Association between food intake and oral health in elderly: SEPAHAN systematic review no. 8. Dent Res J (Isfahan). 2011;8(Suppl 1):S15-20.
Azzolino D, Passarelli PC, De Angelis P, Piccirillo GB, D’Addona A, Cesari M. Poor oral health as a determinant of malnutrition and sarcopenia. Nutrients. 2019;11(12):2898.
Priyamvara A, Dey AK, Bandyopadhyay D, Katikineni V, Zaghlol R, Basyal B, Barssoum K, Amarin R, Bhatt DL, Lavie CJ. Periodontal inflammation and the risk of cardiovascular disease. Curr Atheroscler Rep. 2020;22(7):28.
Jiang Z, Shi Y, Zhao W, Zhou L, Zhang B, Xie Y, Zhang Y, Tan G, Wang Z. Association between chronic periodontitis and the risk of Alzheimer’s disease: combination of text mining and GEO dataset. BMC Oral Health. 2021;21(1):466.
Martinez-Herrera M, Silvestre-Rangil J, Silvestre FJ. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med Oral Patol Oral Cir Bucal. 2017;22(6):e708–15.
Benzian H, Guarnizo-Herreño CC, Kearns C, Muriithi MW, Watt RG. The WHO global strategy for oral health: an opportunity for bold action. Lancet. 2021;398(10296):192–4.
World Health Organization. Agenda item 6 of World Health Organization Executive Board 148th Session: Oral Health. 2021. https://apps.who.int/gb/ebwha/pdf_files/EB148/B148_R1-en.pdf. Accessed 24 Oct 2022.
Acknowledgements
The authors would like to thank Yoshiko Nakata for her technical assistance.
Funding
This work was supported by the Foundation for Health, Labour and Welfare Policy Research Grants from the Ministry of Health, Labour and Welfare of Japan (19FA2001, 21FA1013, 22FA2001).
Author information
Authors and Affiliations
Contributions
MY: Conceptualization, Formal analysis, Writing—original draft. SM: Conceptualization, Formal analysis, Writing – original draft. YM: Methodology, Writing—review & editing. JA: Writing—review & editing. YL: Writing—review & editing. YS: Writing—review & editing. IT: Conceptualization, Funding acquisition, Resources, Supervision, Writing – original draft. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The return of a completed questionnaire was considered to imply consent to participate in the study, including the baseline survey data and subsequent follow-up. Information regarding LTCI certification status was also confirmed after obtaining written consent. Informed consent was obtained from all subjects. The Ethics Committee of Tohoku University Graduate School of Medicine (Sendai, Japan) reviewed and approved the study protocol including the method to obtain informed consent (approval code: 2006–206). All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Baseline characteristics according to whether or not agreed to a review of their LTCI information. Supplementary Table 2. DFLE, DLE, and TLE at 65 years by the number of remaining teeth with brushing (once vs. twice or more per day). Supplementary Table 3. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by smoking status. Supplementary Table 4. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by daily brushing and smoking status. Supplementary Table 5. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by use of dentures and smoking status. Supplementary Table 6. DFLE, DLE, and TLE at 65 years according to the number of teeth stratified by BMI. Supplementary Table 7. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by daily brushing and BMI. Supplementary Table 8. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by use of dentures and BMI. Supplementary Table 9. DFLE, DLE, and TLE at 65 years according to the number of teeth stratified by time spent walking. Supplementary Table 10. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by daily brushing and walking. Supplementary Table 11. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by use of dentures and walking. Supplementary Table 12. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by educational status. Supplementary Table 13. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by daily brushing. Supplementary Table 14. DFLE, DLE, and TLE at 65 years according to the number of remaining teeth stratified by use of dentures and educational status.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yamato, M., Matsuyama, S., Murakami, Y. et al. Association between the number of remaining teeth and disability-free life expectancy, and the impact of oral self-care in older Japanese adults: a prospective cohort study. BMC Geriatr 22, 820 (2022). https://doi.org/10.1186/s12877-022-03541-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03541-2