
Abstract
Objectives
The present study aimed to identify the gender-specific trajectories of grip strength using group-based trajectories, explore the interaction between grip strength and physical activity on depression, and investigate the association of physical activity with the change in depression by different grip strength groups among middle-aged and older European adults.
Methods
A total of 14,098 participants aged 50 years or older from the Survey of Health, Ageing and Retirement in Europe 2007–2019 were included in this study. Group-based trajectory modeling was used to identify the low, middle and high group of grip strength by gender. Generalized estimated equations were fitted to analyze the interaction effect. The data of wave 2-wave 5 and wave 2-wave 7 were chosen to conduct sensitivity analyses.
Results
Significant interactions between grip strength group and physical inactivity were found (x2 interaction = 11.16, P = 0.004). Significant interactions between physical inactivity and time on depression were identified in low (x2 interaction = 27.83, P < 0.001) and moderate (x2 interaction = 23.67, P < 0.001) grip strength, but a similar result was not found in high grip strength (x2 interaction = 4.39, P = 0.495). Participants in the physical inactivity group had higher depression scores in the low and moderate grip strength groups. Sensitivity analyses yield almost similar results.
Conclusions
Grip strength and physical inactivity interact with depression. Lower grip strength and insufficient physical activity can increase depressive symptoms. People with lower grip strength and physical inactivity should pay special attention to the prevention of depression.
Similar content being viewed by others

Background
Depression is the leading cause of mental health disorders worldwide, affecting an estimated 300 million people [1]. Meanwhile, the increasing aging population and elongated life expectancy make it a great challenge for humans [2]. Late-life depression is highly prevalent in aging people, and is a difficult challenge. Moreover, late-life depression dramatically reduces the quality of life [3]. Long-term depression increases morbidity risk [4], mortality [5] and the frequency of healthcare service use [6]. Multiple factors, including dysfunctional cognitions, stressful life events, health status and interpersonal dysfunction, are significantly associated with depression [7, 8]. In addition, it has been reported that higher handgrip strength and sufficient physical activity are negatively related to depression, they could improve mental health [9, 10].
Handgrip strength is a well-established measure of physical performance/muscle strength and has been widely used in an observational cohort studies and clinical settings [11, 12]. Numerous studies have shown that handgrip strength is associated with depressive symptoms, and individuals with higher handgrip strength tend to have a lower risk of depression [9, 13]. In addition, evidence of sex-related differences in handgrip strength that decrease with age has been reported [14]. However, the definition of good grip strength remians controversial [15]. Most studies group handgrip strength use the percentage method based on data distribution [16]. The time effect on grip strength is ignored, although the above studies have considered the influence of sex and age on grip strength.
The relationship between physical activity and handgrip strength has been reported in previous studies. Both studies recommend physical activity during middle age to protect against sarcopenia and depression when the handgrip strength starts to decline [17, 18]. Furthermore, engagement in physical activity has a psychological benefit in later life [19]. However, to our knowledge, little information is currently available on the combined effects of grip strength and physical activity on depression in older people and whether the effect of physical and long-term changes on depression is differentiated by grip strength groups.
Hence, we conducted a prospective study with a large, multinational cohort derived from the Survey of Health, Ageing and Retirement in Europe (SHARE) 2005–2019 to (1) identify the gender-specific trajectories of grip strength using group-based trajectories (GBTM) [20]; (2) explore the joint effect of grip strength trajectory groups and physical inactivity, and (3) investigate the association of insufficient physical activity with a long-term change in depression according to grip strength.
Methods
Study population
Data were obtained from SHARE, which is biennial longitudinal study aimed at assessing the population aged ≥50 years across European countries using probability-based sampling. Details of the sampling methodology can be found in an official published article [21]. The information in this survey concerned health, socioeconomic status, and social and family networks. Seven waves (1, 2, 4, 5, 6, 7, and 8) and one retrospective life history wave (3) have been conducted since 2004. Based on the first wave, SHARE has successively incorporated more European countries since the second wave, including the Czech Republic, Poland, and Ireland. Thus, we analyzed data from six-panel waves of SHARE but excluded the first and third waves in the present study. SHARE was reviewed and approved by the ethics committee of the University of Mannheim and the Ethics Council of the Max Planck Society.
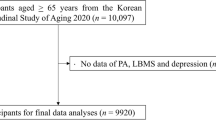
A total of 37,152 people participated in the second wave, which was conducted in 2006. The exclusion criteria were as follows: (1) participation in less than three waves during the following years (n = 16,793); (2) those with cancer, Parkinson’s disease, Alzheimer’s disease, and stroke in any survey that may affect handgrip strength measurement (n = 1370); (3) those with missing data on alcohol intake, smoking status, family economic level, European depression scale, grip strength and cognitive function (n = 1103) and (4) individuals with depression at baseline (wave 2) to avoid causing reverse causality (n = 3788). Ultimately, 14,098 individuals were included in this study. The selection process for the study population is shown in Fig. 1. Most baseline characteristics were well balanced between the original wave 2 (excluding subjects without studied variables and with baseline depression) and the final analyzed wave 2 participants, indicating that those enrolled participants represented the total participants (S-Table 1).

Flow chart of the analytic sample
Depression
Depression was evaluated using the European Depression Scale (EURO-D). The scale is a 12-item binary scale that includes the following symptoms: depression, pessimism, suicidality, guilt, sleep, irritability, fatigue, appetite, interests, enjoyment, concentration and tearfulness, and has been validated by the European Depression Concerted Action Project [22]. The total EURO-D scale ranged from 0 to 12, with a score above three representing depression [23].
Physical inactivity
Physical activity was assessed by asking two questions about how often they engage in moderate- and vigorous-intensity physical activities daily. The following response options were provided: more than once a week, once a week, one to three times a month, and hardly ever or never. Participants who reported ‘hardly ever or never’ for both moderate- and vigorous-intensity physical activity were defined as physical inactivity [24].
Grip strength
Grip strength was measured using a Smedley handheld dynamometer (100 kg) [25]. Participants were asked to sit or stand while keeping their upper arms tight against the trunk with their elbows at a 90° angle and then squeeze the handles as hard as possible for 5 s. Two alternate measures from their right and left hands were performed, the highest value of four measures in each survey wave was used in the present study. Due to the lack of a standard grouping method for grip strength, we used GBTM to explore a suitable group according to sex based on the panel data.
Covariates
Covariates in this study were acquired from the questionnaire, including age, gender (male/female), European region (central, northern, southern, and western Europe), marital status (married, living with a spouse, or other married status such as divorced, widowed), education (primary/secondary/tertiary education). Furthermore, employment status (employed/retired/unemployment), family economic level, smoking status (never, ever, and current smoker), and alcohol intake (drinking exceeds two glasses) were also acquired. In addition, heart attack (yes/no), hypertension (yes/no), hyperlipidemia (yes/no), diabetes (yes/no), mobility limitation (yes/no), body mass index (BMI), and cognitive function were acquired. Education was categorized according to the International Standard Classification of Education [26]. The family economic level was determined by one question: “Is your household able to make ends meet?” The answers included easy, fairly easy, with some difficulty, and with great difficulty. BMI was calculated as weight in kilograms divided by height in meters squared. Cognitive function was assessed in four domains: time orientation, memory, verbal fluency, and numeracy [27, 28]. The scores for each domain ranged from 0 to 5, 0–20, 0–100, and 0–5, respectively. To avoid the proportion of memory and fluency being too high, we standardized the four scores and the sum of the these scores were used to assess cognitive function.
Statistical analysis
All statistical analyses were conducted using STATA version 16.0 (Stata Corp, College Station, Texas, USA). A two-stage approach is used to select the optimal number of groups and trajectory shapes. First, we fitted all trajectory models in cubic form, initiated a model with one trajectory, and then fitted the models up to the optimal number of trajectories based on the Bayesian information criterion value (BIC). The minimum sample size for each trajectory was > 5%. The average posterior probability of assignments (APPA) values should be> 70%, and the odds of correct classification (OCC) should be> 5.0. We examined models based on all grip strength data and found three trajectory groups based on BIC values that appeared to provide the best balance between data fit and complexity. GBTM identified low-, moderate-, and high-grip strength groups of individuals following similar patterns of grip strength according to gender. Data are presented as mean and standard deviation (SDs) for continuous variables or as percentages for categorical variables. One-way analysis of variance (ANOVA) was used to examine the difference in means for continuous variables with normal distribution; otherwise, the Kruskal-Wallis test was used. Pearson’s χ2 test was performed to compare the distribution of categorical variables among the three grip strength groups. Multiplicative interaction was assessed using the grip strength-physical inactivity interaction term in the generalized estimated equation (GEE) model. After determining the joint effect of grip strength and exercise on depression, the time variable interacted with physical inactivity according to the grip strength group to identify the independent effect of exposure on the change in depression over time. Depression was treated as a continuous variable in all the GEE models. The independent working correlation structure was chosen for the GEE analysis.
Considering that the majority of participants were lost to follow-up due to the relatively long survey time of SHARE, we further performed sensitivity analyses with.
data from waves 2 to 5 and from waves 2 to 7 (all excluding wave 3) of SHARE to ensure the robustness of the results.
All GEE models were adjusted for potential confounders including age, gender, European region, marital status, education, employment status, family economic level, smoking status, alcohol intake, heart attack, hypertension, hyperlipidemia, diabetes, mobility limitation, BMI and cognitive function. A two-tailed P value≤0.05 was recognized as statistically significant.
Results
Baseline characteristics of participants
This study included 3123 participants in the low grip strength group, 7454 in the moderate grip strength group, and 3521 in the high grip strength group. The gender-specific grip strength groups explored using GBTM are presented in S-Fig. 1. Grip strength trajectories met the model evaluation criteria (S-Table 6). The mean follow-up time was 9.25 years. The baseline characteristics of the participants across the three grip strength groups are shown in Table 1. Individuals with high grip strength tended to be younger (mean age, 58.12 years old), male (48.08%), married (80.26%), had secondary education (56.43%), had a higher family economic level, had higher alcohol intake, have a higher BMI (average BMI, 26.91 kg/m2) and had cognitive function (average standardized score, 2.14). Participants with low grip strength were more likely to live in Southern Europe (35.34%), retired (67.92%), never smoked (41.63%), had a heart attack (12.74%), had hypertension (39.39%), had hyperlipidemia (24.78%), had diabetes (14.22%), had mobility limitation (58.70%), and were physically inactive (9.54%). The average depression scores increased over time, but this trend was more obvious in the low and moderate grip strength groups than in the high grip strength group.
The joint effect of grip strength and physical inactivity
The results of the multiplicative interaction analysis between grip strength and physical inactivity are presented in Table 2. We also conducted a joint test to assess the association between grip strength, physical inactivity, and depression. A significant interaction effect between grip strength and physical inactivity on depression was identified (joint test: x2 interaction = 11.16, df = 2, P = 0.004).
Impact of physical inactivity according to grip strength groups
Table 3 summarizes the results of physical inactivity interactions with time according to grip strength groups. Significant interactions between physical inactivity and time with depression were identified in both the low (joint test: x2 interaction = 27.83, df = 4, P < 0.001) and moderate (joint test: x2 interaction = 23.67, df = 4, P < 0.001) grip strength groups. As shown in Fig. 2A, B, the increasing rate of depression was faster in the physical inactivity group than in the physical activity group. Compared to the physical activity group, participants in the physical inactivity group were positively associated with depression scores at Waves 4 (β = 0.64, P = 0.002), 5 (β = 0.71, P = 0.001), 6 (β = 0.78, P < 0.001), 7 (β = 0.61, P = 0.009), and 8 (β = 0.57, P = 0.030) except at baseline (β = 0.08, P = 0.418) in the low grip strength group. For moderate grip strength, participants in the physical inactivity group had higher depression scores at Waves 6 (β = 0.55, P = 0.008), 7 (β = 0.80, P < 0.001), and 8 (β = 0.76, P = 0.001) but no significant differences were found at baseline (β = − 0.01, P = 0.913), wave 4 (β = 0.29, P = 0.124), and wave 5 (β = 0.26, P = 0.197). No significant interaction between physical inactivity and time with depression was identified in the high (joint test: x2 interaction = 4.39, df = 4, P = 0.495) grip strength group (Fig. 2C).

Physical inactivity on longitudinal change of depression symptoms according to grip strength groups
Sensitivity analyses
Both sensitivity analyses recognized low, moderate and high grip strength trajectories according to genders (S-Figs. 2 and 3). All trajectories of grip strength met the model evaluation criteria (S-Table 6).
The combined effect of grip strength and physical inactivity used wave 2-wave 5 data/ wave 2-wave 7 are shown in S-Tables 2 and 4, respectively. Significant interaction effects between grip strength and physical inactivity with depression were found in these two sensitivity analyses (joint test of wave 2–wave 5: x2 interaction = 17.95, df = 2, P < 0.001; joint test of wave 2–wave 7: x2 interaction = 16.52, df = 2, P < 0.001).
A significant interaction between physical inactivity and time with depression was identified in the low (joint test: x2 interaction = 19.97, df = 2, P < 0.001) grip strength group based on wave 2-wave 5 (S-Table 3). Significant interactions between physical inactivity and time with depression were identified in both the low (joint test: x2 interaction = 24.95, df = 5, P < 0.001) and moderate (joint test: x2 interaction = 23.14, df = 5, P < 0.001) grip strength groups based on wave 2-wave 7 (S-Table 5). The influence of physical inactivity on depression over the survey time in different grip strength groups is displayed in S-Figs. 4 and 5, respectively. Sensitivity analyses yielded similar results.
Discussion
This large longitudinal study has documented two major findings. First, a multiplicative interaction was found between grip strength, physical inactivity, and depressive symptoms. Second, a significant difference in the change in depressive symptoms between physical inactivity and activity was found in the low and moderate grip strength groups, but no significant difference was found in the high grip strength group.
The interaction effect indicated that individuals with physical inactivity and decreased grip strength had a higher risk of depression than those with sufficient physical activity and good grip strength. Previous cohort studies have reported the protective benefits of grip strength in incident depression [9, 29]. The relationship between physical activity and depression have also been well documented. Physical inactivity was related to sustained depression. Physical activity could confer protection against the emergence of depression [30, 31]. The results of the present study support those of the previous studies. Grip strength is commonly used as a measure of muscle strength. Lack of muscular strength may affect myokines released into the circulatory system, which could protect against the risk of depression [32]. In addition, muscular strength is related to sarcopenia [33], functional limitations and disabilities [34]. Individuals with lower grip strength may experience poorer health conditions. A decline in physical function may predict the risk of mental illness [35]. Continuous engagement in physical activity could make the elderly experience more positive leisure activities and sufficient social support, which results in higher psychological well-being and finally reduces depression [36]. However, the associations among grip strength, physical activity, and depression are complex and bidirectional. Depression symptoms are an important mechanism that can impact physical activity [37, 38]. Furthermore, higher physical activity is associated with greater skeletal muscle strength and muscle power [39]. In the present study, our prospective findings indicate that low grip strength and physical inactivity may have a combined effect on depression, both biologically and psychosocially, which is greater than each effect.
Physical inactivity was related to changes in depression in the low and moderate grip strength groups. However, this association was not observed in the high grip strength group. A s British birth cohort study revealed that increased physical activity levels could prevent a decline in grip strength [40]. Randomized controlled trials have shown that physical activity reduces depressive symptoms in older adults [41]. Physical activities can temporarily change central norepinephrine activity, decrease the hypothalamopituitary–adrenocortical axis, and increase the secretion of beta-endorphins, which positively affect mood [42]. In addition, physical activity may increase hippocampal volume and neurogenesis levels, and adjust the imbalance between anti- and pro-inflammatory and oxidant markers to play an antidepressant role [31]. Previous studies have shown that people with depression have lower levels of peripheral brain-derived neurotrophic factor (BDNF), which may contribute to the pathophysiology of depression [43]. Physical activity increases the concentration of several neurotrophic factors, including BDNF, thus possibly exerting a protective effect against depression [44]. Participation in physical activity could give a positive mood to the participant and improve their ability to cope with depression [45]. Compared to the high grip strength group, people in the low- and moderate-strength grip groups were older and more likely to develop chronic diseases. Handgrip strength was an indicator of an individual’s muscle mass, and lower handgrip strength represents poorer health status. Long-term physical inactivity may play an important role in depression in a low-health state. Sufficient physical activity may not prevent depression in participants with health conditions. However, in our present study, the sample size of people with physical inactivity was relatively small, which may have induced an estimated confidence interval that wa too wide resulting in a false negative conclusion.
A major strength of this study was a large number of participants from a prospective study, which provided sufficient power for our statistical analysis. Besides, the GBTM was used to identify grip strength groups by gender based on the study population, which was more suitable than the percentage method. Furthermore, we assessed the association between changes in physical inactivity across the lifespan and depression. However, this study has some limitations. First, self-reported evaluations of physical activity and other health-related statuses might lead to recall bias. Second, physical activity in SHARE did not differentiate between aerobic and strength training, which may have influenced our findings. Second, some participants were excluded due to study criteria. However, most baseline characteristics were well balanced between the included and excluded participants. Finally, despite controlling for many potential covariates, residual confounding may have influenced the observed associations between physical inactivity and grip strength on depression.
Conclusion
In summary, the results from European middle-aged and older adults indicate that grip strength and physical inactivity have a joint effect on depression. Lower grip strength and physical inactivity can worsen depressive symptoms. Physical inactivity is associated with a change in depression in low and moderate grip strength but not in high grip strength. Therefore, attention should be paid to those with lower grip strength and physical inactivity to prevent depression.
Availability of data and materials
The data that support the findings of this study are available in the Survey of Health, Ageing and Retirement in Europe at doi:https://doi.org/10.1093/ije/dyt088. These data were derived from the following resources available in the public domain: http://www.share-project.org/data-access.html.
Abbreviations
- SHARE:
-
Survey of Health, Ageing and Retirement in Europe
- GBTM:
-
Group-based trajectory modeling
- EURO-D:
-
European depression scale
- SD:
-
Standard deviation
- ANOVA:
-
One-way analysis of variance
- GEE:
-
Generalized estimated equation
- BDNF:
-
Brain-derived neurotrophic factor
References
Patel V, Chisholm D, Parikh R, Charlson FJ, Degenhardt L, Dua T, et al. Addressing the burden of mental, neurological, and substance use disorders: key messages from disease control priorities, 3rd edition. Lancet. 2016;387(10028):1672–85.
Partridge L, Deelen J, Slagboom PE. Facing up to the global challenges of ageing. Nature. 2018;561(7721):45–56.
Blazer DG. Depression in late life: review and commentary. J Gerontol A Biol Sci Med Sci. 2003;58(3):249–65.
Nuyen J, Volkers AC, Verhaak PFM, Schellevis FG, Groenewegen PP, Van den Bos GAM. Accuracy of diagnosing depression in primary care: the impact of chronic somatic and psychiatric co-morbidity. Psychol Med. 2005;35(8):1185–95.
Farrokhi F, Abedi N, Beyene J, Kurdyak P, Jassal SV. Association between depression and mortality in patients receiving long-term dialysis: a systematic review and meta-analysis. Am J Kidney Dis. 2014;63(4):623–35.
Andersson D, Magnusson H, Carstensen J, Borgquist L. Co-morbidity and health care utilisation five years prior to diagnosis for depression. A register-based study in a Swedish population. BMC Public Health. 2011;11:552.
Hammen C. Risk factors for depression: an autobiographical review. Annu Rev Clin Psychol. 2018;14:1–28.
Schaakxs R, Comijs HC, van der Mast RC, Schoevers RA, Beekman ATF, Penninx BWJH. Risk factors for depression: differential across age? Am J Geriatr Psychiatry. 2017;25(9):966–77.
McDowell CP, Gordon BR, Herring MP. Sex-related differences in the association between grip strength and depression: results from the Irish longitudinal study on ageing. Exp Gerontol. 2018;104:147–52.
Marques A, Gaspar de Matos M, Bordado J, Gouveia ÉR, Peralta M, Gomez-Baya D. Different levels of physical activity and depression symptoms among older adults from 18 countries: a population-based study from the survey of health, ageing and retirement in Europe (SHARE). Eur J Sport Sci. 2020:1–8.
Cooper R, Kuh D, Hardy R. Objectively measured physical capability levels and mortality: systematic review and meta-analysis. BMJ. 2010;341:c4467.
Rantanen T, Guralnik JM, Foley D, Masaki K, Leveille S, Curb JD, et al. Midlife hand grip strength as a predictor of old age disability. JAMA. 1999;281(6):558–60.
Firth J, Firth JA, Stubbs B, Vancampfort D, Schuch FB, Hallgren M, et al. Association between muscular strength and cognition in people with major depression or bipolar disorder and healthy controls. JAMA Psychiatry. 2018;75(7):740–6.
Sevene TG, Berning J, Harris C, Climstein M, Adams KJ, DeBeliso M. Hand grip strength and gender: Allometric normalization in older adults and implications for the NIOSH lifting equation. J Lifestyle Med. 2017;7(2):63–8.
Hahn P, Spies C, Unglaub F, Mühldorfer-Fodor M. Grip strength measurement : significance and boundaries. Orthopade. 2018;47(3):191–7.
Wang T, Wu Y, Li W, Li S, Sun Y, Li S, et al. Weak grip strength and cognition predict functional limitation in older Europeans. J Am Geriatr Soc. 2019;67(1):93–9.
Hansen AW, Beyer N, Flensborg-Madsen T, Grønbæk M, Helge JW. Muscle strength and physical activity are associated with self-rated health in an adult Danish population. Prev Med. 2013;57(6):792–8.
Ahn H, Choi HY, Ki M. Association between levels of physical activity and low handgrip strength: Korea National Health and nutrition examination survey 2014-2019. Epidemiol Health. 2022;44:e2022027.
Chang S-C, Pan A, Kawachi I, Okereke OI. Risk factors for late-life depression: a prospective cohort study among older women. Prev Med. 2016;91:144–51.
Nagin DS. Group-based trajectory modeling: an overview. Ann Nutr Metab. 2014;65(2–3):205–10.
Börsch-Supan A, Brandt M, Hunkler C, Kneip T, Korbmacher J, Malter F, et al. Data resource profile: the survey of health, ageing and retirement in Europe (SHARE). Int J Epidemiol. 2013;42(4):992–1001.
Kuiper JS, Zuidersma M, Zuidema SU, Burgerhof JG, Stolk RP, Oude Voshaar RC, et al. Social relationships and cognitive decline: a systematic review and meta-analysis of longitudinal cohort studies. Int J Epidemiol. 2016;45(4):1169–206.
Castro-Costa E, Dewey M, Stewart R, Banerjee S, Huppert F, Mendonca-Lima C, et al. Ascertaining late-life depressive symptoms in Europe: an evaluation of the survey version of the EURO-D scale in 10 nations. The SHARE project. Int J Methods Psychiatr Res. 2008;17(1):12–29.
de Souto BP, Delrieu J, Andrieu S, Vellas B, Rolland Y. Physical activity and cognitive function in middle-aged and older adults: an analysis of 104,909 people from 20 countries. Mayo Clin Proc. 2016;91(11):1515–24.
Andersen-Ranberg K, Petersen I, Frederiksen H, Mackenbach JP, Christensen K. Cross-national differences in grip strength among 50+ year-old Europeans: results from the SHARE study. Eur J Ageing. 2009;6(3):227–36.
International Standard Classification of Education-ISCED 1997 www.unesco.org/education/information/nfsunesco/doc/isced_1997.htm.
Tampubolon G. Cognitive ageing in Great Britain in the new century: cohort differences in episodic memory. PLoS One. 2015;10(12):e0144907.
Falk N, Cole A, Meredith TJ. Evaluation of suspected dementia. Am Fam Physician. 2018;97(6):398–405.
Fukumori N, Yamamoto Y, Takegami M, Yamazaki S, Onishi Y, Sekiguchi M, et al. Association between hand-grip strength and depressive symptoms: locomotive syndrome and health outcomes in Aizu cohort study (LOHAS). Age Ageing. 2015;44(4):592–8.
Carter JD, Assari S. Sustained obesity and depressive symptoms over 6 years: race by gender differences in the health and retirement study. Front Aging Neurosci. 2016;8:312.
Schuch FB, Vancampfort D, Firth J, Rosenbaum S, Ward PB, Silva ES, et al. Physical activity and incident depression: a Meta-analysis of prospective cohort studies. Am J Psychiatry. 2018;175(7):631–48.
Köhler CA, Freitas TH, Maes M, de Andrade NQ, Liu CS, Fernandes BS, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. 2017;135(5):373–87.
Manini TM, Clark BC. Dynapenia and aging: an update. J Gerontol A Biol Sci Med Sci. 2012;67(1):28–40.
McGrath R, Robinson-Lane SG, Peterson MD, Bailey RR, Vincent BM. Muscle strength and functional limitations: preserving function in older Mexican Americans. J Am Med Dir Assoc. 2018;19(5):391–8.
Yanagita M, Willcox BJ, Masaki KH, Chen R, He Q, Rodriguez BL, et al. Disability and depression: investigating a complex relation using physical performance measures. Am J Geriatr Psychiatry. 2006;14(12):1060–8.
Eyler AA, Brownson RC, Donatelle RJ, King AC, Brown D, Sallis JF. Physical activity social support and middle- and older-aged minority women: results from a US survey. Soc Sci Med (1982). 1999;49(6):781–9.
Deka P, Almenar L, Pathak D, Klompstra L, López-Vilella R, Marques-Sule E. Depression mediates physical activity readiness and physical activity in patients with heart failure. ESC Heart Fail. 2021;8(6):5259–65.
Wu IHC, Strong LL, Nguyen NT, Cho D, John J, McNeill LH. Psychosocial stressors, depression, and physical activity among African Americans. Am J Health Behav. 2019;43(4):717–28.
Ramsey KA, Rojer AGM, D'Andrea L, Otten RHJ, Heymans MW, Trappenburg MC, et al. The association of objectively measured physical activity and sedentary behavior with skeletal muscle strength and muscle power in older adults: a systematic review and meta-analysis. Ageing Res Rev. 2021;67:101266.
Dodds R, Kuh D, Aihie Sayer A, Cooper R. Physical activity levels across adult life and grip strength in early old age: updating findings from a British birth cohort. Age Ageing. 2013;42(6):794–8.
Ansai JH, Rebelatto JR. Effect of two physical exercise protocols on cognition and depressive symptoms in oldest-old people: a randomized controlled trial. Geriatr Gerontol Int. 2015;15(9):1127–34.
Bouchard C, Shepard RJ, Stephens T, Sutton JR, Mcpherson BDJM. Sports ei, exercise: exercise, fitness, and health: a consensus of current knowledge. 1991;23(5):643.
Molendijk ML, Spinhoven P, Polak M, Bus BA, Penninx BW, Elzinga BM. Serum BDNF concentrations as peripheral manifestations of depression: evidence from a systematic review and meta-analyses on 179 associations (N=9484). Mol Psychiatry. 2014;19(7):791–800.
Huang T, Larsen KT, Ried-Larsen M, Møller NC, Andersen LB. The effects of physical activity and exercise on brain-derived neurotrophic factor in healthy humans: a review. Scand J Med Sci Sports. 2014;24(1):1–10.
Morgan K, Dalleosso H, Bassey EJ, Ebrahim S. Aire THDJA, society: customary physical activity. Psychol Well-being Success Ageing. 1991;11(4):399–415.
Acknowledgements
We thank the Survey of Health, Ageing and Retirement in Europe (SHARE), which is funded by the European Commission, Horizon 2020, DG Employment, Social Affairs & Inclusion, German Ministry of Education and Research, the U.S. National Institute on Aging and other various national funding sources for providing the datasets to complete the entire study. We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Han Zheng provided the conception of the research design, performed a brief preliminary analysis, completed the remaining analyses and wrote the article; Qingwen He and Hongyan Xun collated data during the early-stage preparations; Xiaowei Zheng proposed sensitivity analyses and wrote the article; Yanfang Gu wrote and revised the article. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
SHARE was reviewed and approved by the ethics committee of the University of Mannheim and the ethics council of the Max Planck Society.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: S
-Fig. 1. Trajectory groups of grip strength according to genders from 2007 to 2019. S-Fig. 2. Trajectory groups of grip strength according to genders from 2007 to 2011. S-Fig. 3. Trajectory groups of grip strength according to genders from 2007 to 2017. S-Fig. 4. Physical inactivity on longitudinal change of depression symptoms according to grip strength groups (Wave 2- Wave 5). S-Fig. 5. Physical inactivity on longitudinal change of depression symptoms According to grip strength groups (Wave 2- Wave 7).
Additional file 2: S
-Table 1. Characteristics of participants according to analyzed samples. S-Table 2. Interactions between grip strength and physical activity (Wave 2-Wave 5). S-Table 3. Interactions between time and physical activity according to grip strength group. S-Table 4. Interactions between grip strength and physical activity (Wave 2-Wave 7). S-Table 5. Interactions between time and physical activity according to grip strength group (Wave 2-Wave 7). S-Table 6. Model evaluation indexes of grip strength trajectories in both genders according to different survey wave.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zheng, H., He, Q., Xu, H. et al. Lower grip strength and insufficient physical activity can increase depressive symptoms among middle-aged and older European adults: a longitudinal study. BMC Geriatr 22, 696 (2022). https://doi.org/10.1186/s12877-022-03392-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03392-x