
Abstract
Background
The elderly face a greater burden of illnesses than other age groups and have a more frequent need of healthcare, including in-patient hospitalisations. Catastrophic expenditure on hospitalisation of the elderly poses a significant challenge to India’s aim of achieving Universal Health Coverage (UHC). India has implemented a policy of Publicly Funded Health Insurance (PFHI) to provide free inpatient care by empanelling private and public hospitals. The existing studies have examined the performance of PFHI in financial protection of the elderly.
Methods
This study utilised the Longitudinal Ageing Study in India (LASI) Wave 1, conducted in 2017–18. LASI is a large-scale nationally representative survey collecting data on elderly health including illness burden, healthcare use and out of pocket expenditure (OOPE). It covered a sample 72,250 individuals aged 45 or above. Financial Protection was measured in terms of Catastrophic Health Expenditure (CHE). Multivariate analysis was conducted to find effect of PFHI on OOPE—quantile and logistic models were applied for OOPE and CHE respectively. For robustness, Propensity Score Matching (PSM) model was applied.
Results
Of the hospitalisations, 35% had taken place in public hospitals. The mean OOPE for a hospitalisation in public sector was Indian Rupees (INR) 8276, whereas it was INR 49,700 in private facilities. Incidence of CHE was several times greater for using private hospitals as compared to public hospitals. Multi-variate analyses showed that enrolment under PFHI was not associated with lower OOPE or CHE. PSM model also confirmed that PFHI-enrolment had no effect on OOPE or CHE. Use of private facilities was a key determinant of OOPE, irrespective of enrolment under PFHI.
Conclusions
This was the first study in India to examine the performance of PFHI in the context of catastrophic hospitalisation expenditure faced by the elderly. It found that PFHI was not effective in financial protection of the elderly. The ongoing reliance on a poorly regulated private sector seems to be a key limitation of PFHI policy. Governments need to find more effective ways of protecting the elderly from catastrophic health expenditure if the goal of UHC has to be realized.
Similar content being viewed by others


Background
The share of the elderly in global population has been rising including in the Low and Low-to Middle-Income countries (LLMICs) [1,2,3]. The elderly face a greater burden of illnesses than other age groups and thereby have greater need for healthcare [4,5,6]. India has a large population of the elderly [7]. According to the last national census held in 2011, India had 104 million persons above the age of 60 years and they constituted 8.6% of its total population [3].
The recent studies in India show that a rapidly aging population is facing increasing burden of chronic health problems. While the non-communicable diseases have been rising everywhere, many parts of India continue to have a significant burden of communicable diseases also [8,9,10,11,12]. This situation means a more frequent need of healthcare for the elderly, including in-patient hospitalisations. The hospital care of the elderly is resulting in large out of pocket expenditure (OOPE) [8,9,10,11,12].
Nations across the world have adopted Universal Health Coverage (UHC) as the desired goal for health systems and ensuring protection from catastrophic health expenditures is central to it. Studies in India and other LLMICs have shown that hospitalisations of the elderly often lead to catastrophic expenditure for the elderly and their families [8, 13,14,15,16,17,18]. The occurrence of large OOPE on hospitalisations of the elderly poses a significant challenge to India’s aim of achieving UHC, [8, 11, 19].
Publicly Funded Health Insurance (PFHI) schemes are seen as important means to achieve UHC in LLMICs as a strategy for expanding access and ensuring financial protection for healthcare [20]. These demand-side financing mechanisms entitle poor and other vulnerable households to choose cashless healthcare from a pool of empanelled providers [21]. PFHI programmes have existed in India for more than a decade now [21]. PFHI in India has been aimed at providing free inpatient care by empanelling private and public hospitals [20, 21].
The elderly are an important group to be covered under PFHI so that they are protected from large out of pocket expenditure when they need to utilise healthcare. It is therefore crucial to know how PFHI has performed in achieving the above objective..Despite the important role of PFHI in financial protection, none of the existing studies in India have examined its performance in protecting the elderly from OOPE and catastrophic expenditure. The current study was therefore aimed at addressing the above gap in literature.
PFHI in India: PFHI schemes started in some states of India around 2006 and a national scheme got launched in 2008 [20, 21]. Thereafter most states in India have implemented PHI schemes to cover the poor households and other vulnerable populations. PFHI in India mainly covers inpatient care i.e. hospitalisation expenditure [20, 21]. Government carries out the enrolment of the eligible households and individuals. Some states engage insurance firms as intermediaries. Other state governments set up their own ‘Trusts’ to act as a purchaser organisations [20, 21]. The states or their purchaser organisations enter into contracts with private and public hospitals. Government announces a defined list of services covered under the scheme and the pre-defined prices at which hospitals will get reimbursed. Hospitals interested in joining the scheme apply for empanelment and those who pass the government's scrutiny for defined capacity and quality parameters enter into contracts [20, 21]. The contracted hospitals provide services to enrolled individuals and generate claims through an online process to get reimbursed at pre-defined prices. The services under PFHI are expected to be completely free for the enrolled persons and 'cash-less' at the point of care [20, 21]. The contracts with the hospitals prohibit them to charge any copayments from the patients. The contracts with hospitals are renewed annually [20, 21].
Methods and materials
Dataset
This study utilised the Longitudinal Ageing Study in India (LASI), Wave 1 that was conducted in 2017–18 [22]. LASI is planned to be conducted every 3 years for the next 25 years. LASI is a large-scale national survey collecting data on burden of disease, functional health, healthcare financing, utilisation, and the social and economic wellbeing of the elderly population.
LASI has a multi-stage sampling design with a nationally representative sample of rural and urban population of older adults (aged 45 and above). It covers all states of India. In its first wave, it covered a sample of 72,250 individuals [22]. The sample size was sufficient for the purpose of the current study.
It collected information on demographic details, household characteristics, food and non-food consumption expenditure; self reported morbidity, healthcare utilisation, household health expenditures (OOPE) and health insurance coverage.
Data analysis
LASI survey data was analysed using STATA V.14. Sampling weights were applied to account for both study design (stratification) and non-response [22]. Individual response rate was 87.3%. Descriptive statistics was used to calculate mean and median OOPE with 95% confidence intervals (CI). Out of pocket expenditure (OOPE) for each episode included all medical expenses and the expenses on transportation.
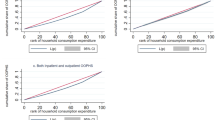
Financial Protection was measured in terms of Catastrophic Health Expenditure (CHE) as proposed by Wagstaff and Doorslaer [23]. The survey collected data on consumption expenditure of households on food and non-food purposes. This study used two types of measures for CHE:
-
a)
CHE as a proportion of annual non-food consumption expenditure: A threshold of 40% of concerned household’s annual non-food consumption expenditure were taken for CHE and named CHE40. This is a commonly used measure of calculating CHE [23].
-
b)
CHE as a proportion of annual consumption expenditure: A threshold of 25% of concerned household’s total annual consumption expenditure were taken for CHE and named CHE25. Recent studies in India have used such a measure for CHE [20, 21, 24].
The list of the variables included in this study is given in Table1.
Multivariate quantile regression analysis was carried out to examine the effect of PFHI on size of OOPE [25]. Quantile regression was used to address the possibility of any skew or extreme values in OOPE. For comparison of results, Ordinary Least Squares (OLS) regression was also carried out for OOPE and reported alongside. The independent variables included in the regression models were selected based on the existing studies of PFHI in India [20, 21, 24].
Multivariate logistic regression analysis was used to find out the association of enrolment under PFHI with CHE25 and CHE40.
For robustness, Propensity Score Matching (PSM) model was applied to examine the effect of enrolment under PFHI on OOPE, CHE25 and CHE40. PSM was meant to confirm whether OOPE differed significantly between episodes of the PFHI-enrolled individuals and the non-enrolled individuals while other relevant characteristics were matched. PSM has been recommended as a suitable method for making such comparisons because it can help in achieving a better balance in patient characteristics [26, 27]. The application of the PSM model includes computing the propensity scores and treatment effect. The average treatment effect on the treated (ATET) gets computed by taking the average of the difference between the observed and potential outcomes for each subject [28]. In the current analysis, the enrolment status of the individual (PFHI enrolled/non-enrolled) was used as the treatment variable while applying the PSM model in STATA. PSM has been used by many studies for evaluating PFHI schemes on financial protection [20, 21, 24, 29].
Results
The sample profile of individuals covered under LASI wave 1 is given in Table 2.
Around two-third of the elderly were residents of rural areas. Around a third of the elderly belonged to the vulnerable social groups of the scheduled castes and scheduled tribes. Less than 5% of the elderly were above 80 years old and 56% were younger than 60 years. Around half the elderly did not have any formal education.
Overall, 18.13% of the elderly were covered under PFHI. The proportion of those covered under other kinds of health insurance was relatively small, at 2.58%.
Hospitalisation rates among elderly under PFHI schemes
The overall hospitalisation rate was 7.1% (6.5%-7.6%) of the elderly (Table 3). Among the PFHI enrolled, the hospitalisation rate was 8.8% (8.2%-9.4%), whereas it was 6.8% (6.2%-7.5%) among those not enrolled under PFHI.
The overall share of public facilities in the hospitalisations of the elderly was 35.06% (31.8%-38.5%) and the rest was in private hospitals (Table 2). Public sector utilisation among the PFHI-enrolled individuals was greater than those not enrolled under PFHI (Table 2).
Out of pocket expenditure (OOPE)
Overall, the mean OOPE for utilising hospitalisation care in private sector was around six times greater than in public sector (Table 4). A similar ratio was seen in mean OOPE incurred in private and public facilities by the PFHI-enrolled individuals.
The mean OOPE for utilising private hospitals was lower for the PFHI-enrolled individuals than the non-enrolled individuals. However, the median OOPE for hospitalisation in private hospitals was almost equal for the PFHI-enrolled and the non-enrolled individuals.
Catastrophic health expenditure (CHE)
Overall, the incidence of CHE25 was around four times greater for utilising private hospitals in comparison to the public hospitals. Around 30% of the episodes in private facilities resulted in occurrence of CHE25 when the individuals involved were covered under PFHI. The incidence of CHE25 among those enrolled under PFHI was also about four times greater for hospitalisation in private facilities as compared to public facilities (Table 5). The pattern of CHE25 among those not enrolled under PFHI was also similar.
The incidence of CHE40 among the PFHI-enrolled was around three times greater for hospitalisations in private facilities as compared to public facilities (Table 5). More than half of the hospitalisations in private sector resulted in CHE40 irrespective of the PFHI-enrolment status of the individuals.
Effect of PFHI enrolment on size of OOPE
The quantile regression analysis for OOPE showed that there was no significant association between PFHI-enrolment and size of OOPE. Utilisation of private facilities was associated significantly with greater OOPE as compared to public facilities. Longer duration hospitalisations resulted in greater OOPE (Additional File S1). Hospitalisations of the elderly living in urban areas involved greater OOPE than those from rural areas. Hospitalisation OOPE was likely to be greater for the richer individuals. Hospitalisation OOPE was likely to be greater for the individuals with higher educational attainment. Hospitalisations of men involved greater OOPE than the women. OOPE also varied according to the type of disease and the state of residence. The OLS model also showed a similar pattern of results (Additional File S1).
The PSM model showed that the PFHI-enrolment did not have a significant effect on size of OOPE for hospitalisations of the elderly (Table 6).
Effect of PFHI enrolment on CHE25 and CHE40
The logistic regression model showed that CHE25 was not significantly associated with the PFHI-enrolment status of the hospitalised individuals (OR = 1.01, p = 0.92) (Additional File S2). Those using public facilities were significantly less likely to incur CHE25 (OR = 0.17, p < 0.01). Longer duration hospitalisations were more likely to result in CHE25. Hospitalisations of men involved greater incidence of CHE25 than women. Hospitalisations of those in the poorest quintile involved greater incidence of CHE25 than those in middle quintile. Incidence of CHE25 varied for different diseases and states (Additional File S2). The logistic regression for CHE40 showed a similar pattern (Additional file S2).
The PSM Model showed no effect of PFHI-enrolment on CHE25 (Table 6). The same finding was there for CHE40 (Table 6).
Discussion
The elderly are one of the most important parts of the population who need to be protected from large healthcare expenditure if countries are to make progress towards the goal of UHC. In India, PFHI is the key policy to achieve this end. The present study is the first study in India that has examined the effect of PFHI on financial protection of the elderly population. It utilised a large survey of elderly individuals known as the Longitudinal Aging Study (LASI) Wave 1 conducted in 2017–18. The survey provided the large and nationally representative sample required for such an evaluation on a national scale. The present study computed the out of pocket expenditure and catastrophic health expenditure as key measures of financial protection. Since PFHI in India is focused on inpatient care, the study examined the effect of PFHI on financial protection for inpatient care of the elderly.
The current study found that 7.1% of the elderly (aged 45 and above) got hospitalised over a year. According to another study of the same period (2017–18), the hospitalisation rate was 8.5% for the above 60 years age group. The difference may be due to the different age groups in the two studies.
The current study found that 35% of hospitalisations of the elderly (age 45 and above) took place in public facilities. Another study of the same period was based on the National Sample Survey (NSS) dataset and it reported the share of public sector as 40% for the above 60 age group [30].
The current study found that enrolment under PFHI increased the chances of using public facilities for hospitalisation. This is surprising, considering that one of the objectives of PFHI was to expand access to hospital care by making the private sector affordable to the poor. This phenomenon may be related to failure of PFHI in actually improving the affordability of private sector [20, 21, 29, 31, 32].
The key finding of the current study is that enrolment under PFHI was not effective in improving financial protection for the elderly. Though the existing studies in India have not examined effectiveness of PFHI for the elderly, most of them have reported that PFHI could not reduce OOPE or catastrophic expenditure for the overall population [8, 20, 21, 29, 31,32,33]. Many of the existing studies on PFHI have been based on analysis of National Sample Survey (NSS) dataset on healthcare utilisation. The current study is the first one to use the LASI dataset. This shows that the effectiveness of PFHI has been poor in India, whether examined through NSS or LASI datasets.
Studies from other LLMICs on OOPE incurred by the elderly have also shown a lack of evidence in favour of PFHI. In China, there was some improvement in access to healthcare with PFHI but such schemes could not protect the elderly from large OOPE [19, 34]. In Philippines, a study has shown that enrolment under PFHI resulted in increase in OOPE for the elderly [35]. In Mexico, studies have shown the ineffectiveness of PFHI in reducing OOPE [36, 37].
The current study found that utilisation of private facilities involved substantially greater financial risk as compared to public facilities, irrespective of the PFHI. A similar finding has been reported by a number of Indian studies, though not in the context of the elderly [20, 21, 24]. The private hospitals entered into contracts under PFHI that forbade them from charging anything from patients. However as the current study shows, they continued to charge from patients enrolled under PFHI. Private hospitals in India are poorly regulated [28,29,30]. Purchasing arrangements through contracts also seem to be ineffective in ensuring price regulation in India’s private sector [20, 21, 24, 31,32,33, 38, 39]. A question arises why adherence to the contracts could not be ensured. Some have pointed out the 'provider capture' as a possible explanation [40, 41]. The private hospitals in India wield significant economic and political clout to thwart the chances of any punitive action when they flout the contracts [41, 42]. A qualitative study has concluded that the normative and cultural context of private sector provisioning in India is a key constraint [33]. The failure of PFHI could be due to a combination of gaps—of poor government regulation, cultural acceptance of illegal payments and treating healthcare as a market transaction [33].
In the current study, the elderly utilising public facilities faced less incidence of catastrophic expenditure, irrespective of their enrolment under PFHI. A study from Mexico also found the use of public facilities by elderly to have a protective effect [43].
Further research is recommended to understand the governance gaps that lead to poor performance of PFHI in India.
Further research is also recommended on financial protection policies for the elderly in India, including by using the future waves of the LASI survey.
Limitations
The current study is cross-sectional whereas two rounds of measurement would be ideal for an evaluation. The current study did not have the option of using two rounds as only the first wave of LASI had been completed. The quality of care could not be included as a variable.
Conclusion
This is the first study in India that examines the performance of PFHI in providing financial protection to the elderly population from hospitalisation costs. Based on the analysis presented in the present study, we conclude that PFHI was not effective in financial protection of the elderly. The ongoing reliance of such policies on a poorly regulated private sector seems to be a big limitation. Further studies are recommended to find out the reasons of poor performance of PFHI for the elderly in LLMIC contexts such as India’s. The goal of UHC cannot be realized unless the elderly are protected from financial risk of healthcare costs. Governments need to find more effective ways of ensuring affordable healthcare for the elderly.
Availability of data and materials
The dataset used and analyzed during the current study is available in public domain. It is freely available for research and academic purposes.
It can be requested at https://www.iipsindia.ac.in/content/LASI-data using request form https://iipsindia.ac.in/sites/default/files/LASI_DataRequestForm_0.pdf
Abbreviations
- CHE:
-
Catastrophic Health Expenditure
- CHE40:
-
Catastrophic Health Expenditure at threshold of 40% of annual non-food expenditure of household
- CHE25:
-
Catastrophic Health Expenditure at threshold of 25% of annual expenditure of household
- CI:
-
Confidence Interval
- INR:
-
Indian Rupees
- LLMICs:
-
Low and Low- to Middle-Income Countries
- OOPE:
-
Out-of-pocket expenditure
- PFHI:
-
Publicly Funded Health Insurance
References
United Nations. World Population Ageing 2019: Highlights. Department of Economic and Social Affairs, Population Division. 2019. United Nations, New York. Available at: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf. Accessed 23 Dec 2021.
Sudharsanan N, Bloom DE. The demography of aging in low- and middle-income countries: chronological versus functional perspectives. In: Future directions for the demography of aging: proceedings of a workshop. Washington (DC): National Academies Press (US); 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513069/.
Bussolo M, Koettl J, Sinnott E. Golden aging: prospects for healthy, active, and prosperous aging in Europe and Central Asia. Washington (DC): The World Bank; 2015. http://hdl.handle.net/10986/22018.
Prince MJ, Wu F, Guo Y, Gutierrez Robledo LM, O’Donnell M, Sullivan R, Yusuf S. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–62. https://doi.org/10.1016/S0140-6736(14)61347-7 Epub 2014 Nov 6.
Dey S, Nambiar D, Lakshmi JK, et al. Health of the elderly in India: challenges of access and affordability. US: National Academies Press; 2012. Available from: https://www.ncbi.nlm.nih.gov/books/NBK109208/.
McGrath R, Al Snih S, Markides K, et al. The burden of health conditions for middle-aged and older adults in the United States: disability-adjusted life years. BMC Geriatr. 2019;19:100. https://doi.org/10.1186/s12877-019-1110-6.
United Nations. World Population Prospects, The 2017 Revision: Datasheet. United Nations. Department of Economic and Social Affairs Population Division. 2017.
Ranjan A, Muraleedharan VR. Equity and elderly health in India: reflections from 75th round national sample survey, 2017–18, amidst the COVID-19 pandemic. Global Health. 2020;16:93. https://doi.org/10.1186/s12992-020-00619-7.
Chatterjee C, Nayak NC, Mahakud J, Chatterjee SC. Factors affecting the choice of health care utilisation between private and public services among the elderly population in India. Int J Health Plann Manage. 2019;34(1):e736–51.
Sahoo H, Govil D, James KS, Prasad RD. Health issues, health care utilisation and health care expenditure among elderly in India: thematic review of literature, aging and health research. 2021;1(2):1-7. https://doi.org/10.1016/j.ahr.2021.100012.
Banerjee S. Determinants of rural-urban differential in healthcare utilisation among the elderly population in India. BMC Public Health. 2021;21:939. https://doi.org/10.1186/s12889-021-10773-1.
Singh SK, Pandey P. Morbidity profile, healthcare utilisation and associated out of pocket expenditure on health among elderly population of Lucknow district. Northern India Trop Med Surg. 2016;4:210. https://doi.org/10.4172/2329-9088.1000210.
Eozenou P-V, Neelsen S, Smitz M-F. Financial protection in health among the elderly – a global stocktake. Health Systems Reform. 2021;7(2).https://doi.org/10.1080/23288604.2021.1911067.
Baird K. High out-of-pocket medical spending among the poor and elderly in nine developed countries. Health Serv Res. 2016;51(4):1467–88. https://doi.org/10.1111/1475-6773.12444.
Piroozi B, Moradi G, Nouri B, Bolbanabad AM, Safari H. Catastrophic health expenditure after the implementation of health sector evolution plan: a case study in the west of Iran. Int J Health Policy Manage. 2016;5(7):417. https://doi.org/10.15171/ijhpm.2016.31.
Barros AJ, Bastos JL, Dâmaso AH. Catastrophic spending on health care in Brazil: private health insurance does not seem to be the solution. Cad Saude Publica. 2011;27:s254–62. https://doi.org/10.1590/S0102-311X2011001400012.
Pal R. Measuring incidence of catastrophic out-of pocket health expenditure: with application to India. Int J Health Care Finance Econ. 2012;12(1):63–85. https://doi.org/10.1007/s10754-012-9103-4.
Aregbeshola BS, Khan SM. Determinants of catastrophic health expenditure in Nigeria. European J Health Econ. 2018;19(4):521–32. https://doi.org/10.1007/s10198-017-0899-1.
Macinko J, Cristina Drumond Andrade F, Bof De Andrade F, Lima-Costa MF. Universal health coverage: are older adults being left behind? evidence from aging cohorts in twenty-three countries: study examines access to care, use, catastrophic expenditures, and other factors among several aging cohorts in twenty-three countries. Health Aff. 2020;39(11):1951–60. https://doi.org/10.1377/hlthaff.2019.01570.
Ranjan A, Dixit P, Mukhopadhyay I, et al. Effectiveness of government strategies for financial protection against costs of hospitalisation Care in India. BMC Public Health. 2018;18:501. https://doi.org/10.1186/s12889-018-5431-8.
Garg S, Chowdhury S, Sundararaman T. Utilisation and financial protection for hospital care under publicly funded health insurance in three states in Southern India. BMC Health Serv Res. 2019;19:1004. https://doi.org/10.1186/s12913-019-4849-8.
International Institute for Population Sciences (IIPS), National Programme for Healthcare of Elderly - Ministry of Health and Family Welfare, India; Harvard T. H. Chan School of Public Health (HSPH) and the University of Southern California (USC). Longitudinal Ageing Study in India (LASI) Wave 1, 2017-18, India Report, 2020. International Institute for Population Sciences, Mumbai. Available at: https://www.iipsindia.ac.in/sites/default/files/LASI_India_Report_2020_compressed.pdf. Accessed 23 Dec 2021.
Wagstaff A, Doorslaer E. Catastrophe and impoverishment in paying for healthcare: with applications to Vietnam 1993–98. Health Econ. 2003;12:921–34.
Garg S, Bebarta KK, Tripathi N. Performance of India’s national publicly funded health insurance scheme, Pradhan Mantri Jan Arogaya Yojana (PMJAY), in improving access and financial protection for hospital care: findings from household surveys in Chhattisgarh state. BMC Public Health. 2020;20:949. https://doi.org/10.1186/s12889-020-09107-4.
Anindya K, Ng N, Atun R, et al. Effect of multimorbidity on utilisation and out-of-pocket expenditure in Indonesia: quantile regression analysis. BMC Health Serv Res. 2021;21:427. https://doi.org/10.1186/s12913-021-06446-9.
Ali M S, Prieto-Alhambra D, Lopes LC, Ramos D, Bispo N, Ichihara M Y, Pescarini JM et al. Propensity score methods in health technology assessment: principles, extended applications, and recent advances. Frontiers in Pharmacology. 2019;10. https://doi.org/10.3389/fphar.2019.00973.
Littnerova S, Jarkovsky J, Parenica J, Pavlik T, Spinar J, Dusek L. Why to use propensity score in observational studies? case study based on data from the Czech clinical database AHEAD 2006–09, Cor et Vasa. 2013;55(4):E383-90.
STATA Corp LLC. STATA Treatment Effects Reference Manual: Potential Outcomes/Counterfactual outcomes. Texas: STATA Press; 2017. Available at: https://www.stata.com/manuals/te.pdf. Accessed 23 Dec 2021.
Ghosh S, Gupta N. Targeting and effects of Rashtriya Swasthya BimaYojana on access to care and financial protection. Econ Polit Wkly. 2017;52(4):61–70.
Government of India. NSS 75th round-key indicators of social consumption in India: Health. New Delhi; 2019. http://www.mospi.gov.in/unit-level-data-report-nss-75th-round-july-2017-june-2018-schedule-250social-consumption-health
Nandi S, Schneider H, Dixit P. Hospital utilisation and out of pocket expenditure in public and private sectors under the universal government health insurance scheme in Chhattisgarh State, India: lessons for universal health coverage. PLoS ONE. 2017;12(11):e0187904.https://doi.org/10.1371/journal.pone.0187904.
Reshmi B, Unnikrishnan B, Rajwar E, Parsekar SS, Vijayamma R, Venkatesh BT. Impact of public-funded health insurances in India on health care utilisation and financial risk protection: a systematic review. BMJ Open. 2021;11(12): e050077. https://doi.org/10.1136/bmjopen-2021-050077.
Nandi S, Schneider H. When state-funded health insurance schemes fail to provide financial protection: an in-depth exploration of the experiences of patients from urban slums of Chhattisgarh. India Glob Public Health. 2019. https://doi.org/10.1080/17441692.2019.1651369.
Zhao S-W, Zhang X-Y, Dai W, Ding Y-X, Chen J-Y, Fang P-Q. Effect of thecatastrophic medical insurance on household catastrophic health expenditure: evidence from China. Gac Sanit. 2020;34(4):370–6.
Abrigo Michael R.M., Halliday Timothy J., Molina Teresa. Expanding health insurance for the elderly of the Philippines. working papers 201907, University of Hawaii at Manoa, Department of Economics. 2019.
Doubova SV, Pérez-Cuevas R, Canning D, Reich MR. Access to healthcare and financial risk protection for older adults in Mexico: secondary data analysis of a national survey. BMJ Open. 2015;5(7):e007877.44
Pavón-León P, Reyes-Morales H, Martínez AJ, Méndez-Maín SM, Gogeascoechea-Trejo MDC, Blázquez-Morales MSL. Out-of-pocket expenditure by elderly adults enrolled in a public health insurance programme in Mexico. Gac Sanit. 2017;31(4):286–91. https://doi.org/10.1016/j.gaceta.2016.12.015.
Devadasan N, Seshadri T, Trivedi M, Criel B. Promoting universal financial protection: evidence from the Rashtriya Swasthya Bima Yojana (RSBY) in Gujarat, India. Heal Res Policy Syst. 2013;11(1):29. https://doi.org/10.1186/1478-4505-11-29.
Rent P, Ghosh S. Understanding the cash-less nature of government-sponsored health insurance schemes: evidence from Rajiv Gandhi Jeevandayee Aarogya Yojana in Mumbai. Sage Open. 2015; October–December: 1–10. https://doi.org/10.1177/2158244015614607.
Sanders D, Nandi S, Labonte R, Vance C, Damme WV. From primary health care to universal health coverage—one step forward and two steps back. Lancet. 2019;394(10199):619–21. https://doi.org/10.1016/S0140-6736(19)31831-8.
Nandi S, Schneider H. Using an equity-based framework for evaluating publicly funded health insurance programmes as an instrument of UHC in Chhattisgarh State, India. Health Res Policy Sys. 2020;18:50. https://doi.org/10.1186/s12961-020-00555-3.
Mackintosh M, Channon A, Karan A, Selvaraj S, Zhao H, Cavagnero E, et al. What is the private sector? understanding private provision in the health systems of low-income and middle-income. Lancet. 2016;6736(16):1–10.
Salinas-Escudero G, Carrillo-Vega MF, Pérez-Zepeda MU, et al. Out of pocket expenditure on health during the last year of life of Mexican elderly: analysis of the Enasem. Salud Publica Mex. 2019;61(4):504–13.
Acknowledgements
Not Applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
SG contributed to the study design; SG and NT contributed to writing of the manuscript. SG, KB, and NT analyzed the data; All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The secondary dataset analysed for this article are from the LASI Wave 1, which contain anonymised data in the public domain. The researchers had no access to personal identifiable data. The survey is undertaken by the International Institute of Population Sciences, Mumbai under the national Ministry of Health and Family Welfare, India. Data available in public domain are approved for use for research purpose by Government of India.
All methods were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Not Applicable.
Competing interests
The authors declare that there are no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Table: OLS and Quantile regression for OOPE.
Additional file 2.
Table: Logistic regression models for CHE25 and CHE40.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Garg, S., Bebarta, K.K. & Tripathi, N. Role of publicly funded health insurance in financial protection of the elderly from hospitalisation expenditure in India-findings from the longitudinal aging study. BMC Geriatr 22, 572 (2022). https://doi.org/10.1186/s12877-022-03266-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03266-2